health watch Living Longer? Living Better? Estimates of Life Expectancy
advertisement
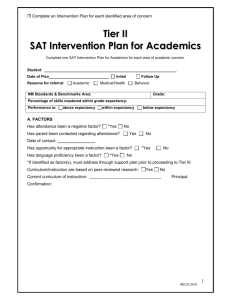
health C O L O R A DO DEP ART MENT OF PUBL I C HE AL TH AND E NVIR O N ME N T watch N IO UN AND January 2012 CO NS TI TU TI ON No. 82 Living Longer? Living Better? Estimates of Life Expectancy and Healthy Life Expectancy in Colorado Kirk Bol, MSPH, Health Statistics Section, Colorado Department of Public Health and Environment Health Statistics Section Alyson Shupe, Ph.D., Section Chief Monica Clancy Kieu Vu, M.S.P.H. Maternal and Child Health Surveillance Unit Rickey Tolliver, M.P.H., Director Janelle Mares Irene Pinela Public Health Informatics Unit Chris Wells, M.S., Director Geoff Bock Doug Duncan Gloria Mora Jeff Scott Bruce Straw Paul Turtle Survey Research Unit Becky Rosenblatt, M.A., Director Mark King Michael Poisson Ava Williams Vital Statistics Unit Mary Chase, Director Kirk Bol, M.S.P.H. Alison Grace Bui, M.P.H. Juanita Galvan Karl Herndon 4300 Cherry Creek Drive South Denver, Colorado 80246-1530 (303)692-2160 (800)886‑7689 health.statistics@state.co.us www.cdphe.state.co.us/hs/ Introduction Out of Colorado’s Public Health Improvement Plan of 2009 came the recommendation to “Ensure a comprehensive set of public health indicators.” Included in the indicators developed for this purpose are measures of health status, namely life expectancy and quality of life. Life expectancy is a measure used frequently to assess the health of a population, and represents the average number of years an individual in a given population could expect to live if experiencing the mortality (death) risk over a lifetime that the entire population experienced in that year. As a summary measure, life expectancy simultaneously includes and reflects the complete mortality experience in a population, from earliest infancy through the extreme elder years.1 Separate quality of life measures, typically measured through survey-based public health surveillance systems, assess in similar summary fashion the population’s self-perceived health status. Self-reported measures of health status, such as the proportion of the population in poor health, have been demonstrated to be reliable and independent predictors of morbidity (illness) and mortality.2 Daniel Sullivan noted in 1971 that while no one index can reflect all aspects of health, “there is considerable agreement that an index which measures some aspects of nonfatal illness as well as mortality would be desirable.”3 One such metric used to combine mortality and morbidity (i.e. quality of life) into a single measure is healthy life expectancy. This is interpreted as the average number of healthy years (i.e. years spent in ‘good or excellent’ health) an individual in a population under study could expect to live given the mortality and general health status of that population in some stated period of time. Unfortunately, due to concerns related to availability of data and their statistical validity and reliability, healthy life expectancy is rarely computed at the county or community level. Even at the statewide level, few estimates have been generated to date regarding healthy life expectancy for Colorado. It is the intent of this report to present estimates of life and healthy life expectancy for Colorado; and in response to notable disparities in both life expectancy and quality of life among selected subpopulations, present similar estimates by race and Hispanic origin and region of residence. Additionally, this report will address concerns regarding the scarcity of these measures at the county and community levels, as well as describe interpretive issues and limitations of these measures. Methods Utilizing birth and death data from the Vital Statistics Unit in the Health Statistics Section at the Colorado Department of Public Health and Environment (CDPHE), life expectancy estimates among Colorado residents, including its race/ethnic and regional subgroups, were computed. Methods employed followed the abridged life table techniques presented by Dr. Chin Long Chiang,4 and which are frequently used by the National Center for Health Statistics at the Centers for Disease Control and Prevention (CDC).5 Using these methods, life expectancy at birth can be estimated, as can remaining years of life at various ages. Additionally, utilizing the Colorado Behavioral Risk Factor Surveillance System (BRFSS) and Child Health Survey (CHS) data from the Health Statistics Section at CDPHE, statewide, race/ethnic and region-stratified estimates of general health status were computed. The Colorado BRFSS is a telephone survey conducted by random-digit dialing of adults 18 years and older living in a household with a landline telephone. The survey is an important tool for surveillance and evaluation of health behaviors and chronic health conditions among the adult population. It is conducted annually by CDPHE in collaboration with the CDC. During the BRFSS interview, the interviewer inquires if a child between the ages of 1 and 14 years lives in the household, and about their willingness to complete the Child Health Survey. If agreed, the parent is called a few days later to complete a survey on a variety of topics including his or her child’s physical activity, nutrition, access to health and dental care, behavioral health, sun safety, injury and many others. Data for both surveys are collected over the calendar year; and at the end of the year, data are weighted to reflect the general population of adults at 18 and older and children ages 1 to 14, respectively. General health status is most often assessed using the following question: “Would you say your health in general is... ‘excellent, good, fair or poor?’” In this report, “unhealthy” status was measured as the proportion of adults who responded for themselves, or on behalf of the children selected, that their general 2 Colorado Department of Public Health and Environment health status was either ‘fair’ or ‘poor’. Proportions of fair or poor health were utilized for the following age groups: Under 1 year, 5-year age groups through age 84, and 85 years and older. As Colorado’s surveillance activities do not presently capture general health status for infants, an estimate of 5 percent was used for the proportion of infants in fair or poor health. This is reasonable when considering the prevalence of birth complications and health conditions among infants based on birth certificate data, as well as estimates of major congenital anomalies as generated by birth defect surveillance programs. Also, given the dearth of general health status by subpopulation among adolescents, the estimates for fair or poor health from the BRFSS for the age group 18 to 24 were applied to both the 15-19 and 20-24 years age groups. Following the work of Dr. Michael T. Molla, et al.,6 these general health status proportions for Colorado and its race/ ethnic and regional subpopulations were incorporated into the abridged life tables in order to compute estimates of healthy life expectancy. Ninety-five percent (95%) confidence intervals for both life expectancy and healthy life expectancy were also computed in a manner consistent with the methods presented by Dr. Chiang and Dr. Molla, et al. Results Life Expectancy Since 1990, life expectancy among Colorado residents has increased from 77.2 years to 80.4 years. While there have been increases in both male and female life expectancy over this time period, females continue to have higher life expectancy than males. This gap between males and females, however, has been shrinking over time (1990: females-80.3 years, males-74.1; 2010: females-82.4, males-78.3) (Figure 1). Figure 1. Life expectancy in years by sex: Colorado residents, 1990-2010. 85 84 83 82 Life expectancy in years 81 80 81.5 80.3 79 80.7 80.1 80 80.6 80.4 80.2 80.6 80.4 76 77.2 77.6 77.0 77.3 77.6 77.6 77.7 80.6 74 74.1 73.9 74.4 74.4 78.1 78.0 78.2 78.6 78.4 78.3 74.4 74.8 75.1 75.5 75.6 75.9 76.3 76.3 76 81.2 81.8 79.6 79.8 79.7 77.6 77.6 77.5 80.5 79.1 82.2 80.0 78.5 77 75 73 80.5 79.3 78 77 80.4 80.7 82 81.6 76.4 77.9 82.4 80.4 78.3 76.9 72 71 70 Total Male Female Error bars represent the 95% confidence interval of the life expectancy estimate. SOURCE: Health Statistics Section, Colorado Department of Public Health and Environment. Similarly, there have been increases in life expectancy across Colorado’s various race/ethnic populations. On the other hand, disparities persist, particularly among the Black population, for which life expectancy in 2010 was 76.9 years, compared to 80.5 among White, non-Hispanic residents and 80.3 among White, Hispanic residents (Figure 2). Life expectancy estimates for Colorado’s Asian American/ Pacific Islander and American Indian/Native Alaskan populations are unstable and likely unreliable, and are shown here for illustrative purposes only. Because of the relatively small populations as well as the small numbers of deaths in each of these groups, life expectancies tend to be overestimated, and fluctuate greatly over time. This overestimation is the natural result of attempting to use life table methods when there are few or no deaths in the various abridged age groups used in the life table, and made worse when there are few or no deaths in the oldest age groups. As a result, the best and most stable estimates for these populations will need to be based on more robust multistate or national data. For the remainder of this report, and for these reasons, race/ethnic-specific estimates will be limited to White, non-Hispanic; White, Hispanic; and Black populations in Colorado. 3 Health Statistics Section Figure 2. Life expectancy in years by race/ethnicity: Colorado residents, 1990-2010. 110 108 106 104 102 100 Life expectancy in years 98 96 94 92 90 88 86 84 82 80 78 76 74 72 77.5 77.9 76.3 77.0 73.4 72.9 70 White, non-Hispanic 78.8 79.4 77.3 78.0 80.5 80.3 76.9 75.4 White, Hispanic 73.7 Black/African American Asian American/Pacific Islande American Indian/Native Alaskan Error bars represent the 95% confidence interval of the life expectancy estimate. SOURCE: Health Statistics Section, Colorado Department of Public Health and Environment. General Health Status Healthy Life Expectancy Based on Colorado BRFSS estimates, the proportion of Colorado adults reporting in 2009-2010 that they were in fair or poor health was 11.3 percent, a proportion consistent with the 2003-2004 reporting period (11.7%). Persistent over this time period was a significant disparity among Colorado Hispanic residents, among whom the proportion reporting fair or poor health in 2009-2010 was 22.7 percent, compared to White, non-Hispanics at 9.0 percent. Additionally, emerging in 20052006, and growing since, is a higher proportion of the Black population reporting fair or poor health, which in 2009-2010 was 16.6 percent. According to data from Colorado’s 2010 Child Health Survey, 2.2 percent of children ages 1-14 were reported as being in fair or poor health. This has been consistent since 2007 and is similar across the different race/ethnic populations. When looking at life and healthy life expectancies, a couple questions should be asked: “What are the life and healthy life expectancies, both overall/at birth and at various ages throughout life?” and “What is the difference between life and healthy life expectancy, that is, the proportion of life expected to be spent in fair or poor health?” The following estimates of healthy life expectancy and their relationship to life expectancy are examined with the above questions in mind. 4 Colorado Department of Public Health and Environment In addition to having a higher life expectancy than males for the combined time period 2008-2010 (female: 82.1 years; males: 77.9), females have a higher healthy life expectancy as well (female: 72.7, male: 69.4). These differences exist for life and healthy life expectancy at birth, as well as when looking at remaining years of life or remaining years of healthy life at various ages, for which the gap between male and female narrows, but never closes completely (Figure 3). Regardless of gender, approximately 11 percent of one’s life is expected to be spent in fair or poor health. Life- and healthy life expectancy in years Figure 3. Life expectancy and healthy life expectancy in years by sex: Colorado residents, 2008-2010. 90 85 80 75 70 65 60 55 50 45 40 35 30 25 20 15 10 5 0 82.1 77.9 72.7 69.4 Age group in years Life expectancy- female Healthy life expectancy- female Life expectancy- male Healthy life expectancy- male SOURCE: Health Statistics Section, Colorado Department of Public Health and Environment. As overall life expectancy varies across Colorado’s race/ethnic populations, so does healthy life expectancy. White, nonHispanic residents have both the highest life and healthy life expectancies (80.2 and 73.0 years, respectively). While White, Hispanic residents have only a slightly lower life expectancy (79.2 years), their healthy life expectancy is lowest among the race/ethnic groups described here (61.1 years). Black residents have the lowest life expectancy (76.8 years), which is more than three years lower than White, non-Hispanic residents; but healthy life expectancy among Black residents (64.0 years) is higher than that for White, Hispanic residents. That said, there remains a noteworthy gap between life and healthy life expectancy. Among White, non-Hispanic residents, approximately 9 percent of one’s life is expected to be spent in fair or poor health; while for Black residents, this proportion increases to 17 percent; and among White, Hispanic residents, 23 percent of one’s life is expected to be in fair or poor health (Figure 4). 5 Health Statistics Section Life-and healthy life expectancy in years Figure 4. Life expectancy and healthy life expectancy in years at selected ages by race/ethniciy: Colorado residents, 2008-2010. 85 80 75 70 65 60 55 50 45 40 35 30 25 20 15 10 5 0 80 80.2 79.2 76.8 56.1 56.2 55.4 71.0 73.0 61.1 64.0 48.2 49.7 38.8 Total White, White, nonHispanic Hispanic Infancy 53.6 Black Total White, nonHispanic White, Hispanic 37.2 37.3 30.9 31.8 36.5 35.1 24.0 25.3 42.0 Black Total 25-29 years Healthy life expectancy White, nonHispanic White, Hispanic 45-49 years Black 20 20 19.8 19.1 15.8 16.1 12.4 13.5 Total White, nonHispanic White, Hispanic Black 65-69 years Life expectancy Error bars represent the 95% confidence interval of the life expectancy estimate. SOURCE: Health Statistics Section, Colorado Department of Public Health and Environment. Noteworthy, too, is the persistence of differences in life- and healthy life expectancy by race and ethnicity over a lifetime. As seen in Figure 4, the smallest number of years of life remaining at various periods in life, namely at 25-29, 45-49, and 65-69 years of age, is found among Black residents (53.6, 35.1, and 19.1 years, respectively, compared to White, non-Hispanic residents with 56.2, 37.3, and 20.0 years). Additionally, the difference between remaining years and healthy years of life is largest among White, Hispanic residents at these three ages (16.6, 12.5, 7.4 years, respectively, compared to White, nonHispanic residents with 6.5, 5.5, and 3.9 years). The nature of these disparities hint that risk factors, behaviors, and causes of morbidity and mortality that affect life and healthy life expectancy likely affect disproportionately Black and White, Hispanic residents at any and all ages compared to White, non-Hispanic residents. Both life expectancy and healthy life expectancy vary by geographic region of residence. Across Colorado’s Health Statistics 6 Colorado Department of Public Health and Environment Regions, which are often used to examine regional differences within Colorado, life expectancy ranged from 76.3 years to 83.7 in the 2008-2010 time period. The difference between the minimum and maximum healthy life expectancy was a bit larger, with estimates ranging from 64.5 years to 77.1. Across regions, the difference between life and healthy life expectancy ranged from 5.8 to 13.3 years. Regions in the state in which life expectancy and/or healthy life expectancy were lower than the statewide estimate include those in southern (region 8) and southeast Colorado (region 6), the south-central mountains (region 13), as well as Adams, Denver, and Mesa Counties. Areas in which life and healthy life expectancy were higher include the mountain resort/west I-70 area (region 12) and Boulder, Douglas, and Larimer Counties (Figures 5 and 6). Figure 5. Life expectancy and healthy life expectancy by region of residence: Colorado residents, 2008-2010. 90 85 80 75 82.9 81.6 83.7 79.6 76.3 70 Life- and healthy life expectancy in years 80.4 80.2 79.6 77 79.9 80.6 78.5 77.9 80.4 81.7 80.4 78.1 80.2 80.2 78.8 78.2 67.6 67.0 Colorado life expectancy: 80.0 years Colorado healthy life expectancy: 71.0 years 65 60 55 50 45 40 35 30 73.1 66.3 77.1 71.7 72.7 71.4 64.5 65.8 65.6 70.4 72.6 75.8 70.3 72.6 67.1 75.7 73.3 69.6 72.8 25 20 15 10 5 0 Life expectancy Healthy life expectancy Error bars represent the 95% confidence interval of the life expectancy estimate. SOURCE: Health Statistics Section, Colorado Department of Public Health and Environment. 7 Health Statistics Section Figure 6. Map of life expectancy (LE) and healthy life expectancy (HLE) in years (with 95% confidence intervals) by geographic region of residence: Colorado residents, 2008-2010. BOULDER BROOMFIELD GILPIN ADAMS DENVER 21 LE: 78.2 (78.0-78.4) HLE: 67.0 (65.8-68.2) PARK LE: 80.4 (79.6-81.2) GARFIELD 1 6LE: 81.7 (81.4-82.0) SUMMIT EAGLE MESA PITKIN LE: 78.8 (78.4-79.2) HLE: 67.6 (65.7-69.5) SAN MIGUEL DOLORES LAKE CHAFFEE 9 OURAY SAN JUAN LE: 80.4 (79.8-81.0) HLE: 72.7 (71.0-74.4) LA PLATA MONTEZUMA 17 8 LE: 77.9 (77.1-78.7) HINSDALE HLE: 65.6 (63.4-67.8) MINERAL ALAMOSA RIO GRANDE ARCHULETA CONEJOS Colorado Department of Public Health and Environment 5 ELBERT LE: 79.6 (79.4-79.8) HLE: 71.7 (70.8-72.6) EL PASO LE: 80.2 (79.3-81.1) HLE: 71.4 (69.5-73.3) LINCOLN CHEYENNE KIOWA 7 CROWLEY LE: 77.0 (76.6-77.4) HLE: 65.8 (64.3-67.4) PUEBLO OTERO 6 BENT PROWERS LE: 76.3 (75.6-77.0) HLE: 64.5 (62.4-66.6) HUERFANO COSTILLA SOURCE: Health Statistics Section, Colorado Department of Public Health and Environment. 8 YUMA WASHINGTON 4 13 CUSTER LE: 79.6 (79.0-80.2) HLE: 66.3 (64.1-68.5) KIT CARSON DOUGLAS LE: 80.4 (79.6-81.2) HLE: 73.3 (71.5-75.1) TELLER FREMONT SAGUACHE MORGAN 14 DENVER 15 3 LE: 78.5 (77.9-79.1) HLE: 70.3 (68.9-71.7) LE: 79.9 (79.3-80.5) HLE: 70.4 (68.9-71.9) MONTROSE 22 00 PARK GUNNISON 10 21 PHILLIPS 1 HLE: 75.7 (74.7-76.7) BOULDER CLEAR CREEK GILPIN 12 LOGAN 18 WELD LE: 83.7 (83.2-84.2) HLE: 75.8 (74.2-77.4) DELTA SEDGWICK LARIMER GRAND EL PASO LE: 80.2 (79.8-80.6) HLE: 69.6 (68.2-71.0) 2 RIO BLANCO 19 TELLER LE: 81.6 (81.3-81.9) HLE: 73.1 (71.8-74.4) ROUTT 5 ELBERT LE: 82.9 (82.5-83.3) HLE: 77.1 (75.7-78.5) LE: 80.4 (79.6-81.2) JACKSON 3 DOUGLAS HLE: 73.3 (71.5-75.1) ARAPAHOE LE: 80.4 (80.2-80.6) HLE: 72.6 (71.6-73.6) 15 LE: 80.2 (80.0-80.4) HLE: 72.8 (72.0-73.6) 11 14 22 00 JEFFERSON MOFFAT LE: 80.6 (79.7-81.5) HLE: 72.6 (70.8-74.4) LE: 78.1 (77.8-78.4) HLE: 67.1 (65.8-68.4) LAS ANIMAS BACA 14 Discussion Measures of life- and healthy life expectancy are summary measures: They represent the combined morbidity and mortality experience within a population, and distill that information into an average number of years of life or healthy life remaining for the members of that population. These types of summary measures are most commonly computed at the national level and for other countries around the world, and are useful in estimating overall population health and the global burden of disease.7 Summary measures are necessary to facilitate discussions about the ability of countries to provide for and maintain the health of their respective populations, particularly in light of increasing life expectancies, aging populations, and increased chronic disease maintenance and care. These measures are also important in identifying and exploring health and outcome disparities among different race/ethnic and geographic populations. How to combat these disparities poses a challenge to today’s health care and public health care systems in the U.S.. This is particularly true given the variation in disparities, and the uncertain roles that lacking health insurance, health-related behaviors, risk factors, and social risks play in both the presence and magnitude of disparities.8 Life- and healthy life expectancy are also found among the foundation health measures for Healthy People 2020 under measures of general status, which are used for monitoring progress toward the goals of increasing life expectancy and eliminating disparities set forth by this initiative.9 The estimates of life expectancy found in this report are among the most current presented for Colorado, while those for healthy life expectancy are among the first of their kind generated for Colorado and its race/ethnic and geographic subpopulations. These measures provide the unique opportunity to compare Colorado’s experience with the country as a whole, as well as discuss differences in these measures among Colorado’s residents and the disparities found. Life expectancy for the United States was 77.9 years (based on 2007 data, the latest available), compared to 79.8 years in Colorado for 2007. Over time, Colorado’s life expectancy has mirrored the general increase in life expectancy observed in the U.S., although Colorado life expectancy is generally about two years greater than the U.S. estimate in any year. Colorado and the U.S. share similar trends in life expectancy by race/ethnicity as well: Overall, life expectancies increased, though disparities persist. Most notable among these were consistently lower life expectancies within the Black population.1,10 A few concerns regarding interpretation, methodology, and statistical limitations warrant discussion. As previously described, life expectancy represents the combined, lifetime mortality experienced by the population from which the mortality data utilized arise. As such, life expectancy is influenced by such myriad events as infant mortality, injury and suicide deaths among teens and young adults, and deaths due to cancer, cardiovascular disease, diabetes, and respiratory diseases among adults and seniors (as well as all other causes of death across all ages). It is therefore impossible to point to any one cause as the reason why life expectancy would be higher in one group than another. Healthy life experience adds to the summary mortality experience a second dimension of general health status in the population, as derived from self-assessed and reported testaments of general health. One’s health status can be affected by a great number of factors, including presence of acute or chronic conditions, nutrition, physical activity, mental health, as well as differences in interpretation of what “fair” or “poor”’ health status is in comparison to “excellent” or “good.” Consequently, as with life expectancy, one cannot identify any single component affecting health as the root cause of differences in healthy life expectancy. There are also some statistical limitations associated with measures of life- and healthy life expectancy. Most of the estimates presented in this report are accompanied by 95 percent confidence intervals, which account for and reflect the uncertainty in these measures. Such uncertainties arise from possible errors in collection or estimation of the death, population, or health status components used in computing life and healthy life expectancy. Uncertainty is also introduced by the relatively small populations, numbers of deaths, or limited populations surveyed for general health status. The abridged life table technique applied here utilizes 19 age groups; for all of these 9 Health Statistics Section groups, mortality rates and estimates of general health status are required. There are several recommendations concerning the minimum population, number of deaths, or sample size required in order to compute reliable life and healthy life expectancy estimates. Examples include a required total population of 5,000 or more; a total of 700 deaths or more across all age groups; and/or a minimum of 50 respondents, within any single age group. For the combined three-year time period used in this report (2008-2010), and through the regionalization of less-populous counties in Colorado, requisite population sizes and death counts are generally met for the race/ethnic and geographic groups presented. Such, however, is not always the case for the Child Health Survey or BRFSS estimates of general health status. It would be possible to utilize additional years of data, or to incorporate larger age ranges/fewer age groups in the abridged life tables; however, the results would be even more difficult to interpret. When broader time periods are used, estimates of mortality or health status are less timely as they are lumped with earlier years of data, making it more difficult to measure changes over time. Similarly, if resolution of age groups is sacrificed, the ability to explore remaining life- and healthy years of life at specific ages is lost. This is therefore a case of using the best and most appropriate data available to achieve the most meaningful results. Even though ideal conditions were not always met when generating the estimates presented in this report, it is evident based on the confidence intervals for life and healthy life expectancy that these estimates are sufficiently reliable to be explored and to serve as the basis for continued discussion and use in assessing population health. In response to the interpretive and statistical limitations concerning life- and healthy life expectancy, it is imperative that these measures not be used in isolation in an attempt to describe in comprehensive fashion the health status of a population. Rather, it is in conjunction with additional measures of morbidity and mortality, risk factors and health behaviors, and social and economic factors—such as those in Colorado’s Health Indicator Set11 and other data products—that the sum10 Colorado Department of Public Health and Environment mary measures such as those presented here are most meaningful. While respectful of the summary nature of life and healthy life expectancy estimates and their limitations, it is expected that these measures will supplement discussions concerning health status and health disparities in Colorado, assist in ongoing public health assessment and planning activities, and aid in the continued protection and improvement of the health of the people of Colorado. Acknowledgements The author would like to acknowledge Kieu Vu, MSPH, Colorado Behavioral Risk Factor Surveillance System Coordinator, and Rickey Tolliver, MPH, Colorado Maternal and Child Health Surveillance Coordinator, both in the Health Statistics Section at CDPHE, for their assistance with this report, and specifically for providing the child and adult general health status statistics needed to compute healthy life expectancy. 11 Health Statistics Section References 1. Health, United States, 2010: With Special Feature on Death and Dying. National Center for Health Statistics, 2010. 2. Race/ethnic Disparities in Self-Rated Health Status among Adults With and Without Disabilities: United States, 20042006. Centers for Disease Control and Prevention. Morbidity and Mortality Weekly Report: 47(39); 1069-1073, 2008. 3. Sullivan, Daniel. A Single Index of Mortality and Morbidity. Health Services and Mental Health Administration. Vol. 86, No. 4, April 1971. 4. Chiang, Chin Long. Introduction to Stochastic Processes in Biostatistics. Wiley Publications in Applied Statistics. John Wiley & Sons, Inc, 1968. 5. Anderson, Robert N. Method for Constructing Complete Annual U.S. Life Tables. National Center for Health Statistics. Vital Health Statistics: 2(129), 1999. 6. Molla, Michael T; Wagener, Diane K; Madans, Jennifer H. Summary Measures of Population Health: Methods for Calculating Health Life Expectancy. National Center for Health Statistics. Healthy People Statistical Notes: No. 21, 2001. 7. Masseria, Christina, et al. What are the methodological issues related to measuring health and drawing comparisons across countries. Research Note. European Commission, 2007. 8. Kulkarni, Sandeep, et al. Falling behind: life expectancy in U.S. counties from 2000-2007 in an international context. Population Health Metrics: 9(16), 2011. 9. U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Healthy People 2020. Washington, D.C. 10. Arias, Elizabeth. United States Life Tables, 2007. National Center for Health Statistics. National Vital Statistics Report: Vol. 59, No. 9, 2011. 11. Colorado Health and Environmental Data. http://www.chd.dphe.state.co.us Additional State Reports 1. New Jersey Department of Health and Senior Services. Martin, Rose Marie. Estimates of Healthy Life Expectancy in New Jersey for Selected Race/Sex Subpopulations, 1996-1998. Topics in Health Statistics, August 2002. 2. Rhode Island Department of Health. Jiang, Yongwen and Hesser, Jan. Healthy Life Expectancy in Rhode Island. Health by Numbers, Vol. 7, No. 8, August 2005. 3. North Carolina Public Health. Healthy Life Expectancy in North Carolina, 1996-2000. Special Report Series by the State Center for Health Statistics, No. 129, January 2002. 4. Utah Department of Health. Years of Healthy Life in Utah. Utah BRFSS Brief, July 2002. 5. Washington State Department of Health. Years of Healthy Life Expectancy, Washington State. Office of Epidemiology, August 2007.
 0
0
advertisement

Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users