Oscar Luaces , Jos´e R. Quevedo , Francisco Taboada ,
advertisement

Prediction of Probability of Survival in Critically Ill Patients
Optimizing the Area Under the ROC Curve∗
Oscar Luaces , José R. Quevedo , Francisco Taboada† ,
Guillermo M. Albaiceta† , Antonio Bahamonde
†
Artificial Intelligence Center
Hospital Univ. Central de Asturias (HUCA)
University of Oviedo at Gijón
University of Oviedo
Asturias - Spain
Asturias - Spain
Abstract
The paper presents a support vector method for estimating probabilities in a real world problem: the
prediction of probability of survival in critically ill
patients. The standard procedure with Support Vectors Machines uses Platt’s method to fit a sigmoid
that transforms continuous outputs into probabilities. The method proposed here exploits the difference between maximizing the AUC and minimizing the error rate in binary classification tasks. The
conclusion is that it is preferable to optimize the
AUC first (using a multivariate SVM) to then fit a
sigmoid. We provide experimental evidence in favor of our proposal. For this purpose, we used data
collected in general ICUs at 10 hospitals in Spain;
6 of these include coronary patients, while the other
4 do not treat coronary diseases. The total number
of patients considered in our study was 2501.
1
Introduction
The available models for predicting outcomes in intensive
care units (ICU) are usually scoring systems that estimate
the probability of hospital mortality of critically ill adults.
This is the case of APACHE (Acute Physiology And Chronic
Health Evaluation) [Knaus et al., 1991], SAPS (Simplified
Acute Physiology Score) [Le Gall et al., 1984], and MPM
(Mortality Probability Models) [Lemeshow et al., 1993]. The
score functions of these predictors were induced from data on
thousands of patients using logistic regression. The data required by these systems come from monitoring devices, clinical analysis, and demographic and diagnostic features of patients. So, APACHE III includes age, 16 acute physiologic
variables that use the worst value from the first 24 hours
in the ICU (temperature, heart rate, blood pressure, respiratory rate, oxygenation, acid-base status, serum sodium, serum
blood urea nitrogen, serum creatinine, serum albumin, serum
bilirrubin, serum glucose, white cell count, hematocrit, itemized Glasgow Coma Scale score, and urine output), preexist∗
The research reported here is supported in part under grant
TIN2005-08288 from the MEC (Ministerio de Educación y Ciencia
of Spain). The authors acknowledge the work of the Grecia Group
in the collection of data.
ing functional limitations, major comorbidities, and treatment
location immediately prior to ICU admission.
These prognostic models are mainly used to measure the
efficiency of ICU treatments. The risk stratification of patients allows comparison of the observed outcomes versus
accepted standards provided by score functions. ICU assessment is very important since it is estimated that end-of-life
care consumes 10% to 12% of all healthcare costs. Moreover, in 2001 the average daily cost per patient in ICUs was
about $3000 in the USA [Provonost and Angus, 2001]. On
the other hand, the literature also shows that prognoses have
constituted an important dimension of critical care, as patients
and their families seek predictions about the duration and outcome of illness [Lemeshow et al., 1993].
In this paper we propose a new method for learning probabilities that will be tested on the probabilities of survival in
ICU patients. The method makes intensive use of the socalled Support Vector Machines (SVM), a powerful family
of algorithms for learning classification and regression tasks.
When used for binary classification, SVM learn hypotheses
that return continuous numbers: positive values for cases of
one class, and negative for the other class.
On the other hand, to measure the performance of predictions in medicine, and in general when classes are very unbalanced, the misclassification rate (or accuracy) is usually
inadequate. Frequently, the Area Under a receiver operating characteristic (ROC) Curve (AUC for short) is used. This
amount can be interpreted as the degree of coherence between
a continuous output (such as the probability, or the continuous
output of an SVM) and a binary classification. It is important
to emphasize that that coherence is established in terms of orderings. For this purpose, continuous outputs or scores are
used to rank available cases, while classes in the ICU problem are codified by ‘+1’ when the patient has survived, and
‘−1’ otherwise.
In this context, Hanley and McNeil [1982] showed that the
AUC is the probability of a correct ranking; in other words,
it is the probability that a randomly chosen subject of class
‘+1’ is (correctly) ranked with greater output than a randomly
chosen subject of class ‘−1’. Therefore, AUC coincides with
the value of the Wilcoxon-Mann-Whitney statistic.
Additionally, there are other measures of the goodness of
probability estimations; for instance, the Brier score is the average of quadratic deviations of true and predicted probabili-
IJCAI-07
956
ties. The relation between AUC and Brier scores was studied
in [Ikeda et al., 2002]. However, the relationship found is
guaranteed only under very restrictive conditions that are difficult to check in real world cases. Moreover, the relationship
is not always direct even in the case study reported in the experimental section of this paper.
To learn a probability distribution using SVM, it is crucial
to transform their scores or continuous outputs into probabilities. But this is what a method presented by Platt [2000]
does. The core idea is to fit a sigmoid, using a maximum
likelihood procedure. The novelty of the proposal reported
in this paper is that we postulate that to compute Platt’s sigmoid it is better to look for an optimum AUC first than to
minimize the error rate with a classification SVM. For this
reason, in Section 2.3 we shall discuss how to optimize the
AUC with a Support Vector method [Herbrich et al., 2000;
Joachims, 2005].
The rationale behind our proposal is that the quality of the
sigmoid fit depends on the quality of the ranking of the scores.
If most of the cases with a higher score than a given one of
class y have a class greater than y, then the task of the sigmoid
can be easily accomplished, and the performance of the final
probability is nearly optimal.
At the end of the paper we provide experimental evidence
in favor of our proposal, comparing it with other alternative
approaches. For this purpose, we used data collected in general ICUs at 10 hospitals in Spain, 6 of which include coronary patients, while the other 4 do not treat coronary diseases. The total number of patients considered in our study
was 2501, 19.83% of whom did not survive.
2
Predicting probabilities
In this section we shall start off by reviewing a standard
method for learning probabilities based on Support Vector
Machines to then present our proposal. But first of all we
must realize that the performance of classification learners is
not satisfactory in the ICU problem; otherwise, nobody would
turn to probabilities. This is a general situation in medicine,
as well as in other fields; accurate crisp predictions are difficult to make, but some useful knowledge can be drawn from
data.
The section will end with the description of a straightforward approach for learning probabilities using regression.
This method will be used as a baseline for measuring the merits of the other options.
2.1
Therefore, we shall assume that the true class probability,
P rtrue (y = +1|x), is 1 when the class of x, y, is +1 and
0 otherwise.
In general, when predictions are discrete probability distributions, there is basically one standard loss function: the average quadratic deviation. If there are two possible outputs,
the probability loss is given by
1 (h(xi ) − pi )2
(1)
ΔPr (h, S ) = |S | xi ∈S
where the hypothesis h returns the estimation of the probability h(x) = P r(y = +1|x), and pi stands for the observed
probability of the i-th case, pi = P rtrue (y = +1|xi ).
The measurement in Equation (1) is frequently used in
medicine and meteorology, and is known as the Brier [1950]
index or score. If the number of possible outputs is greater
than two, the estimated probabilities can be seen as a vector,
and the Mean Square of the Euclidean (MSE) distance from
predicted and observed probabilities is then used; see, for instance [Melville et al., 2005]. It can be seen that, in the ICU
problem, MSE is 2 times the Brier score.
2.2
Optimizing accuracy plus a sigmoidal
transformation
The straightforward approach to the ICU problem is a binary
classification SVM followed by a sigmoid estimated using
Platt’s method [2000]. Thus, given the training set S, we can
use a transformation φ defined from input entries in X into a
feature space H, where classes should be mostly separable by
means of a linear function. As is well known, H must have
an inner product , , and
K(xi , xj ) = φ(xi ), φ(xj )
is called the kernel function of the transformation. We shall
use the rbf kernel that is defined by
K(xi , xj ) = e−
xi −xj 2
2σ 2
(3)
The work of the SVM consists in solving the following
convex optimization problem:
n
min
w,ξ
s.t.
The goodness of probability predictions
Let S = {(x1 , y1 ), . . . , (xn , yn )} be a training set for a learning task in which a function (or hypothesis) is sought that is
able to return outputs yi from entries xi of an input space
X . An important issue when we are learning is to fix the
way in which we are going to measure the quality of the result. In fact, given S formally, the aim of learning is to find a
hypothesis h (from a given hypothesis space) that minimizes
the average loss extended over the set of independently identically distributed (i.i.d.) test sets S , usually represented by
Δ(h, S ).
In the ICU problem, training and test examples have
no probability attached, they are labeled with +1 or −1.
(2)
1
ξi ,
w, w + C
2
i=1
(4)
yi (w, φ(xi ) + b) ≥ 1 − ξi ,
i = 1, . . . , n
ξi ≥ 0,
Then, the classification is accomplished by the hypothesis
sign(w, φ(xi ) + b)
(5)
It can be seen that the kernel and the vector α = (αi :
i = 1, . . . , n) of Lagrange multipliers define the implementation of Function (5) computed from input space entries x as
follows:
n
αi yi K(xi , x) + b (6)
sign(w, φ(x) + b) = sign
IJCAI-07
957
i=1
According to (4), the aim of this function is to maximize the margin (between classes) and to minimize the training
n loss. In fact, the sum of the so-called slack variables,
i=1 ξi , is an upper bound of misclassifications of (6) on
the training set. It is acknowledged that the Function (6) so
achieved has good classification accuracy on unseen cases.
In order to compute the probabilistic outputs, we get rid of
the sign function, and we only consider the continuous outputs
n
αi yi K(xi , x) + b
(7)
fac (x) = w, φ(x) + b =
For each x of the input space, the hypothesis so found returns
f (x) = w, φ(x) =
αi,j (K(xi , x)−K(xj , x)) (12)
yi >yj
where αi,j are again the Lagrange multipliers computed by
the optimizer.
Unfortunately, this approach leads to dealing with one constraint for each element of the dataset
S̄ = {(xi , xj ; +1) : yi = +1 > yj = −1}
i=1
Platt’s method then fits a sigmoid to estimate probabilities:
1
hac (x) = P r(y = +1|x) =
(8)
1 + eAac ·fac (x)+Bac
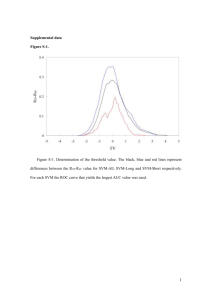
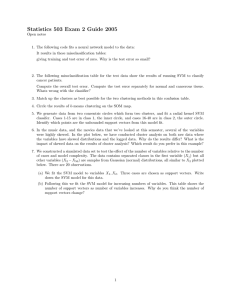
Figure 1 depicts the fit of this sigmoid to the dataset of
all patients (2501) at all the available hospitals. Notice that
the fac values follow a bell-shape distribution with most individuals having positive values, which means that they have
a survival prediction.
2.3
Optimizing the AUC first
When classification predictions are made comparing the values returned from patients’ descriptions x by a rating function
with a threshold, as in classification SVM (see Equation (5)),
then the performance of these predictions can be assessed using the AUC. According to its probabilistic interpretation, the
complementary of this amount (1-AUC) can be used as a loss
function. Thus, if g is a hypothesis, its loss evaluated on a test
set S is
ΔAU C (g, S )
f (φ(xi )) > f (φ(xj )) ⇔ f (φ(xi ) − φ(xj )) > 0.
(10)
Notice that this statement converts ordering constraints into
classification constraints (with one class), but now the input
space is X × X and each pair (xi , xj ) is represented by the
difference φ(xi ) − φ(xj ). According to this approach, the
aim is to find a hypothesis f (x) = w, φ(x) such that w
solves the following convex optimization problem:
1
ξi,j
(11)
w, w + C
min
w,ξ
2
i,j:y >y
i
s.t.
whose size is the number of positive (class +1) examples
times the number of negatives, #pos×#neg, i.e. O(n2 ) when
the size of S is only n. This means that some applications
become intractable, although the approach (or a simplified
version of it) has been successfully used on other occasions
[Joachims, 2002; Bahamonde et al., 2004].
To alleviate the difficulties caused by the size of data sets, it
is not straightforward to reformulate Herbrich’s approach as
an optimization problem with a small number of constraints.
The main problem is that the loss function (1-AUC) (see
Equation (9)) cannot be expressed as a sum of disagreements
or errors produced by each input xi .
Following a different procedure, Joachims [2005] recently
proposed a multivariate approach to solve this problem with a
convex optimization problem that converges using only a few
constraints.
The optimization problem is:
min
= P r(g(xi ) ≤ g(xj )|yi > yj ) =
i,j:yi >yj 1g(xi )≤g(xj )
=
(9)
i,j 1yi >yj
Let us stress that the explicit objective of SVM presented in
the preceding section is not to minimize Equation (9). [Cortes
and Mohri, 2004] provide a detailed statistical analysis of the
difference between maximizing the AUC and minimizing the
error rate in binary classification tasks.
Herbrich et al. [2000] presented a direct implementation
that solves a general ranking problem that is applicable to
maximizing the AUC. The core idea is that if a hypothesis
f : φ(X ) → R is linear and has to fulfill that f (φ(xi )) >
f (φ(xj )), since yi > yj , then
j
w, φ(xi ) − w, φ(xj ) ≥ 1 − ξi,j ,
ξi,j ≥ 0, ∀i, j : yi > yj
(13)
w,ξ
s.t.
1
w, w + Cξ
2
(1 − yi,j
)(φ(xi ) − φ(xj )) ≥
w,
(14)
yi >yj
≥ ΔAU C ((1, . . . , 1)(yi,j
)) − ξ
∀yi,j
∈ {+1, −1}#pos·#neg − {(1, . . . , 1)}
Despite the enormous potential number of constraints, the
algorithm proposed in [Joachims, 2005] converges in polynomial time. Moreover, it only requires a small set of constraints. However, the most interesting result is that the solution w of problem (14) is also the same as that of the optimization problem (11). Additionally, the slack variables in
both cases are related by
ξi,j
(15)
ξ=2
yi >yj
Finally, the multivariate SVM returns a function fAU C of
the form
(16)
fAU C (x) = w, φ(x).
Then Platt’s method can fit a sigmoid to transform the output of fAU C into a probability.
hAUC (x) = P r(y = +1|x) =
IJCAI-07
958
1
1+
eAAUC ·fAUC (x)+BAUC
(17)
1
18.0 %
0.9
16.2 %
0.8
14.4 %
0.7
12.6 %
0.6
10.8 %
0.5
9.0 %
0.4
7.2 %
0.3
5.4 %
0.2
3.6 %
0.1
1.8 %
0
3
2
1
0
1
2
3
0.0 %
Figure 1: The fit of the sigmoid to the dataset of all patients (2501). The horizontal axis represents the outputs of an SVM.
Each ‘*’ mark is the average posterior probability for all examples falling into a bin of width 0.2. The sigmoidal function is
the estimation computed by Platt’s method [2000] (the output values are labeled on the left vertical side), while the bell-shaped
function is the histogram for P r(f (x)) for all the examples (frequencies are labeled on the right).
2.4
3
Regression is a baseline approach
Considering that probabilities are real numbers, regression algorithms must be a first attempt to learn them. For this purpose, all training examples of class −1 are labeled as 0.
In order to maintain the uniformity of approach with preceding subsections, we considered the regression based on
support vectors, therefore we used the so-called Support Vector Regression (SVR). Although there are least squares SVR,
we used the standard version; i.e. a learner of a function
fRe (x) =
n
(αi− − αi+ )K(xi , x) + b∗
(18)
i=1
where K is once again the rbf (3) kernel, and αi are the Lagrange multipliers of the solution to the convex optimization
problem:
n
min
w,ξ
s.t.
1
(ξi+ + ξi− ),
w, w + C
2
i=1
(19)
(w, φ(xi ) + b) − yi ≤ + ξi+ ,
yi − (w, φ(xi ) + b) ≤ + ξi− ,
ξi+ , ξi− ≥ 0,
i = 1, . . . , n
However, given that nothing forces fRe (18) outputs to be
in [0, 1], we set the hypothesis output to 1 whenever fRe returns values above 1, and 0 for fRe values below 0. In symbols, finally we have the hypothesis
hRe (x) = max{0, min{1, fRe (x)}}
(20)
Experimental results
Using a collection of data sets of survival probabilities in critically ill patients, we carried out an experimental comparison of four different learning approaches. SVM followed
by Platt’s fit of a sigmoid: the accuracy optimizer described
in subsection 2.2, which will be represented by SVM(Accu);
the multivariate version, aimed at optimizing the AUC (subsection 2.3), for short SVM(AUC); and finally the regression
approach, SVR (subsection 2.4). The fourth predictor used
was the commercial system APACHE III; we used the customization described in [Rivera-Fernández et al., 1998] that
was developed to improve its performance in Spain.
First of all, we have to point out that this is an unfair
comparison, since APACHE III was trained with a cohort
of 17440 patients from 40 different hospitals in the USA
[Knaus et al., 1991]; the Spanish version used records of
10929 patients from 86 ICUs; while the available data sets in
our experiments only included 2501 patients. Nevertheless,
this comparison is useful to test whether or not the scores
achieved by SVM methods are good enough to be considered
for future learning tasks.
To estimate the performance of the algorithms described in
the preceding section, we used data collected from ICUs at
10 different Spanish hospitals, 6 of which include coronary
patients. It is acknowledged among the medical community
that coronary diseases generally have a lower mortality risk
than other critical illnesses. So from a learning perspective, it
makes sense to differentiate between ICUs with and without
coronary patients.
The data were organized in 13 different training sets, one
IJCAI-07
959
# patients
Hospitals
108
189
194
194
195
239
269
297
337
479
1
2
3
4
5
6
7
8
9
10
Averages
919
1582
2501
{2,3,6,8}
{1,4,5,7,9,10}
all
SVM(AUC)
Bs
AUC (%)
SVM(Accu.)
Bs
AUC (%)
Bs
SVR
AUC (%)
APACHE III
Bs
AUC (%)
0.1712
0.1887
0.1735
0.1089
0.1102
0.1569
0.0993
0.1205
0.1096
0.1071
75.82
73.51
75.32
77.20
84.44
74.87
81.09
84.86
81.35
79.32
0.1860
0.1998
0.1897
0.1142
0.1094
0.1637
0.1096
0.1277
0.1128
0.1120
70.60
69.23
65.88
74.93
82.41
69.12
75.75
81.44
77.91
71.74
0.2019
0.2444
0.1976
0.1260
0.1078
0.1666
0.1044
0.1301
0.1099
0.1198
69.86
63.79
70.64
74.35
85.33
71.91
80.47
80.98
79.87
72.74
0.1473
0.1710
0.1592
0.0961
0.1079
0.1459
0.0852
0.1127
0.1071
0.1218
81.76
77.80
78.20
86.17
88.78
77.62
88.02
87.37
81.30
78.22
0.1346
78.78
0.1425
73.90
0.1509
74.99
0.1254
82.52
0.1494
0.1086
0.1234
79.75
81.79
81.51
0.1500
0.1108
0.1229
78.46
80.37
81.22
0.1546
0.1082
0.1234
76.72
80.08
80.85
0.1432
0.1094
0.1218
80.86
82.63
82.27
Table 1: Brier scores (Bs) and AUC estimated by a 10-fold cross-validation for the three learners described in the text, and
for the commercial system APACHE III. All differences from SVM(AUC) are significant according to a one tail t-test with
threshold p < 0.01, considering the results on the 10 hospitals. For ease of reading, AUC scores are represented as percentages.
for each single hospital, two collecting the data from not coronary/coronary ICUs respectively, and the last one containing
all the data. Each patient in these data sets was described
by the same set of variables used by APACHE III. However,
given that some of these variables have discrete values, we
had to transform them to be handled by SVM-based systems.
Thus, we codified each discrete variable using as many new
binary variables (with values 0 and 1) as the number of possible values of the original variable, setting only the variable
corresponding to the discrete value actually taken by the original variable to ‘1’.
Performance estimations were made using a 10-fold stratified cross-validation on each of the data sets, for all the algorithms except for APACHE III; since it was already trained
with a different data set, we used the available data to test its
predictions. Additionally, the data was standardized according to the mean and deviation observed on each training fold.
It is important to recall that the AUC achieved by the
Spanish version of APACHE III in our experiments, 82.27%
(in percentage) is similar to the amount reported by RiveraFernández et al. [1998]: 81.82%. This fact supports the representativeness of the sample of critically ill patients considered in the experiments described here.
As usual, when dealing with SVM, the parameter setting
stage is very important. To set the regularization parameter
C (see optimization problems in Section 2) and the rbf kernel
parameter σ (see Eq. (3)) in the three support vector based
algorithms, we performed a grid search on a validation set
formed by the patients at 3 hospitals: one hospital without
coronary patients (8), and 2 with coronary patients (1 and 9);
see Table 1. The ranges searched were the following: for C
we tested values from 10−4 to 102 varying the exponent in
steps of 1; for σ we tested values from 10−2 to 101 varying
the exponent in steps of 0.5. We found that the most promising values were C = 101 and σ = 10−2 for SVM(Accu)
and SVR; and C = 10−1 and σ = 10−2 for multivariate
SVM(AUC). It is worth noting that for SVM and SVR the
parameter search was aimed at minimizing the Brier score,
while for multivariate SVM it was aimed at maximizing the
AUC.
Table 1 shows the results obtained (Brier score and AUC)
in the experimental setting described above. Focusing on the
results obtained by the three support vector algorithms, we
can observe that, in general, the best performance (lowest Bs
and highest AUC) is achieved by multivariate SVM(AUC).
The differences are statistically significant according to a one
tail t-test with threshold p < 0.01. This should not be surprising for the AUC measure, since this algorithm was specially
devised to optimize such a measure. But it also outperforms
SVM and SVR in terms of the Brier score, whose parameters
were set to optimize this score.
Let us stress that, although the optimization problem posed
to SVR is precisely the minimization of the distance between
true and predicted probabilities, a large amount of data is required to tie the scores of SVM(AUC) in the Brier score. The
underlying reason explaining this behavior may be that the
hypothesis space used by SVR is not adequate so as to induce
probability distributions from a reduced set of training data,
even with an rbf kernel.
As regards the data sets used in the experiments, support
vector machines yielded the worst performance on the first
three data sets, i.e. the smallest. SVR performance was particularly poor on these data sets. Considering that the rows of
Table 1 are in ascending order of size of the data set, the trend
indicates that performance could be improved if more training cases were available. In fact, when the data set included
all available patients’ records, the results obtained were similar to those yielded by APACHE III (recall that it was trained
with data sets that were several times bigger). On the other
hand, we also observe that survival predictions seem to be
IJCAI-07
960
slightly harder for ICUs without coronary patients (Hospitals
2, 3, 6 and 8) than for ICUs including coronary patients.
4
Conclusions
We have presented a learning method for estimating probabilities in a real world problem: the prediction of survival in critically ill patients. However, the approach is general enough
to be applied to other learning tasks. The method is an alternative to the standard procedure when the learning machine
is based on Support Vectors and uses Platt’s method [Platt,
2000] to fit a sigmoid. Instead of using an SVM devised to optimize classification accuracy, we propose to use a learner that
optimizes the Area Under the ROC Curve (AUC). This can
be done using a multivariate SVM described in [Joachims,
2005].
We experimentally compared the results obtained by this
method with other approaches, and with a commercial scoring system trained with thousands of cases, APACHE III
[Knaus et al., 1991; Rivera-Fernández et al., 1998]. In the
reported experiments, we used real data from 10 ICUs at hospitals in Spain that contain records from 2501 patients. The
medical description of each patient includes monitoring variables, clinical analysis, and demographic and diagnostic features.
The method proposed here outperforms the standard SVM
approach, especially when the available data is scarce, which
is the usual situation. On the other hand, increasing the
number of training examples reduces differences in performance; even between probability predictions of APACHE III
and those made by the baseline method, a simple regression
with the output trimmed to the interval [0, 1].
References
[Bahamonde et al., 2004] Antonio Bahamonde, Gustavo F.
Bayón, Jorge Dı́ez, José Ramón Quevedo, Oscar Luaces, Juan José del Coz, Jaime Alonso, and Félix Goyache. Feature subset selection for learning preferences: A
case study. In Russ Greiner and Dale Schuurmans, editors, Proceedings of the International Conference on Machine Learning (ICML ’04), pages 49–56, Banff, Alberta
(Canada), July 2004.
[Brier, 1950] G.W. Brier. Verification of forecasts expressed
in terms of probability. Monthly Weather Rev, 78:1–3,
1950.
[Cortes and Mohri, 2004] Corinna Cortes and Mehryar
Mohri. AUC optimization vs. error rate minimization.
In Sebastian Thrun, Lawrence Saul, and Bernhard
Schölkopf, editors, Advances in Neural Information
Processing Systems 16. MIT Press, Cambridge, MA,
2004.
[Hanley and McNeil, 1982] J.A. Hanley and B.J. McNeil.
The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology, 143(1):29–36,
1982.
[Herbrich et al., 2000] R. Herbrich, T. Graepel, and K. Obermayer. Large margin rank boundaries for ordinal regression. In A.J. Smola, P.L. Bartlett, B. Scholkopf, and
D. Schuurmans, editors, Advances in Large Margin Classifiers, pages 115–132. MIT Press, Cambridge, MA, 2000.
[Ikeda et al., 2002] Mitsuru Ikeda, Takeo Ishigaki, and
Kazunobu Yamauchi. Relationship between brier score
and area under the binormal roc curve. Computer Methods and Programs in Biomedicine, 67(3):187–194, 2002.
[Joachims, 2002] T. Joachims. Optimizing search engines
using clickthrough data. In Proceedings of the ACM Conference on Knowledge Discovery and Data Mining (KDD),
2002.
[Joachims, 2005] Thorsten Joachims. A support vector
method for multivariate performance measures. In Proceedings of the ICML ’05, 2005.
[Knaus et al., 1991] W.A. Knaus, E.A. Draper, D.P. Wagner,
J.E. Zimmerman, M. Bergner, P.G. Bastos, C.A. Sirio,
D.J. Murphy, T. Lotring, and A. Damiano. The APACHE
III prognostic system. Risk prediction of hospital mortality for critically ill hospitalized adults. Chest, 100:1619–
1636, 1991.
[Le Gall et al., 1984] J.R. Le Gall, P. Loirat, A. Alperovitch,
P. Glaser, C. Granthil, D. Mathieu, P. Mercier, R. Thomas,
and D. Villers. A simplified acute physiology score for
ICU patients. Crit Care Med., 12:975–977, 1984.
[Lemeshow et al., 1993] S. Lemeshow, D. Teres, J. Klar,
J. S. Avrunin, S. H. Gehlbach, and J. Rapoport. Mortality probability models (MPM II) based on an international
cohort of intensive care unit patients. Journal of the American Medical Association, 270(20):2478–2486, November
1993.
[Melville et al., 2005] Prem Melville, Stewart M. Yang,
Maytal Saar-Tsechansky, and Raymond J. Mooney. Active
learning for probability estimation using jensen-shannon
divergence. In Proceedings of The 16th European Conference on Machine Learning (ECML ’05), pages 268–279,
Porto, Portugal, October 2005.
[Platt, 2000] John Platt. Probabilistic outputs for support
vector machines and comparisons to regularized likelihood
methods. In A.J. Smola, P.L. Bartlett, B. Scholkopf, and
D. Schuurmans, editors, Advances in Large Margin Classifiers, pages 61–74. MIT Press, 2000.
[Provonost and Angus, 2001] P. Provonost and D.C. Angus.
Economics of end-life-care in the intensive care unit. Critical Care Med, 29(Suppl):46–51, 2001.
[Rivera-Fernández et al., 1998] R.
Rivera-Fernández,
G. Vázquez-Mata, M. Bravo, E. Aguayo-Hoyos, J. Zimmerman, D. Wagner, and W. Knaus. The APACHE III
prognostic system: customized mortality predictions
for Spanish ICU patients. Intensive Care Medicine,
24(6):574–581, June 1998.
IJCAI-07
961