Implementation of the reservoir-wave hypothesis
advertisement

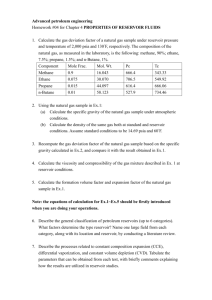
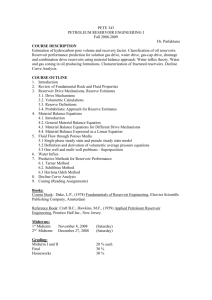
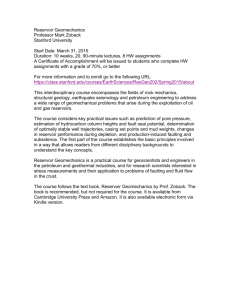
Implementation of the reservoir-wave hypothesis with CMR-derived aortic area and flow velocity Robert D. M. Gray CoMPLEX, University College London Supervisors: Dr. Giovanni Biglino and Prof. Andrew Taylor 4381 words 6th March 2015 Abstract The reservoir-wave hypothesis states that the blood pressure waveform can be usefully divided into a reservoir pressure that is related to the global compliance and resistance of the arterial system and an excess pressure that depends on local conditions. The formulation of the reservoir-wave hypothesis applied to the area waveform is shown, and the analysis is applied to area and velocity data from highresolution phase-contrast cardiovascular magnetic resonance. A feasibility study shows the success of the principle, with the method producing largely robust and physical parameters, and the linear relationship between flow and wave pressure seen in the pressure formulation is retained. A small proof of concept study suggests the potential of the technique by comparing patient and control data. Finally, the analysis is applied to the ascending and descending aorta and interestingly the invariant property of the reservoir pressure is shown to be lost in the area formulation. 1 Background As background to this project, I will give a brief overview of the anatomy and physiology of the heart and arteries. Experiments in cardiovascular magnetic resonance (CMR) provide the data for this project so an outline of this new and non-invasive method is also instructive. Finally I will present the basic theory behind the arterial models which underpins the reservoir-wave theory developed in the later sections. 1.1 Basic Cardiovascular Anatomy and Physiology The heart pumps blood around the circulatory system. It consists of four chambers. The right atrium collects blood from the systemic veins; blood flows from the right atrium into the right ventricle, which supplies the pulmonary arteries; the left atrium analogously collects blood from the pulmonary veins; finally the left ventricle receives blood from the left atrium and ejects it into the systemic arteries.1 1 (b) (a) Figure 1: A diagram of the heart and great arteries (a) from2 and an example arterial pressure waveform (b) from3 On exiting the left ventricle blood flows from the aortic root into the ascending aorta and up into the aortic arch. In the arch three major arteries branch off the aorta which supply the head and upper body. These are the brachiocephalic artery, the left common carotid artery and the left subclavian artery. Blood not flowing into any of these continues into the descending aorta which passes down into the body, becoming the thoracic aorta and branching to supply the rest of the body.1 Figure 1a shows the structure of this anatomy. The periodic sequence of events in which the heart executes its pumping function is the cardiac cycle. Systole is the period of contraction of the heart in which blood is ejected from the left ventricle into the arteries. The subsequent period of relaxation as the chambers refill with blood is known as diastole.1 During this cycle blood pressure rises as blood is forced from the left ventricle, then decays away during diastole. The arterial blood pressure waveform over the cardiac cycle is important for this project so an example is show in Figure 1b. 1.2 Cardiovascular Magnetic Resonance The method by which the data for this project is acquired is cardiovascular magnetic resonance imaging (CMR). Magnetic resonance imaging (MRI) is a general technique for medical imaging that works by exposing the body to a very strong magnetic field. The physics of the technique are not wholly relevant but broadly the responses of water molecules to small perturbations in the field, which depend on the local molecular environment, are measured using radio waves. This produces contrast between tissues which allows images of the body to be created. CMR operates on the same principles and is optimised for use in the cardiovascular system.4 It is further possible to extract velocity data with a technique known as phase contrast cardiovascular magnetic resonance imaging (PC-CMR). Again without any detailed physics, the phase of the response of the water molecules contains information about 2 (a) (b) Figure 2: Examples of magnitude (a) and phase (b) CMR images their velocity.4 The combination of the tissue differentiation and velocity determination allows simultaneous measurement of the area of an artery and the velocity of the blood flowing through it. These measurements make the entire analysis involved in this project possible. Figure 2 shows examples of PC-CMR images. Shown are magnitude (a) and phase (b) images of a transverse plane of a person’s chest. In the magnitude image different shades of grey represent different responses and thus different types of tissue. In the phase image the velocity data are encoded into the grey scale such that grey is not moving, white is movement out of the plane and black is into the plane. The rounded regions in the centre and towards the bottom-right of the images are the ascending and descending aorta respectively. Images like these are acquired over the cardiac cycle; these frames are taken at peak systole, when you appreciate the maximum expansion of the aorta and the motion of blood. The data for my analysis is then produced from this raw PC-CMR data in image processing software called OsiriX (Pixmeo, Geneva, Switzerland). In this program the blood vessel to be measured, termed the region of interest (ROI), is manually selected from one frame. The ROIs can then be automatically propagated through the rest of the frames using nonrigid registration.5 The area and average velocity are then extracted from the images to produce the data to be analysed. 1.3 Arterial Blood Flow Models Wave intensity analysis is a method of modelling arterial blood flow that has arisen in the last 25 years. Having its roots in gas dynamics it differs from traditional Fourier and impedance methods in being a time domain analysis, allowing application to nonperiodic or transient flow.6 At the most basic level we are considering a 1D model of the arterial system as a deformable tube described by a position coordinate x filled with and inviscid, incompressible fluid. Immediately we are making several simplifying assumptions. In terms of the dimension reduction, according to Willemet and Alastruey “several comparisons against in 3 vivo, in vitro and 3D numerical models have shown the ability of the 1D formulation to capture the main features of pressure and flow waveforms in human systemic arteries”.7 The fluid mechanical assumptions can be relaxed to investigate more complex flow, but this is not in this case useful and I continue the analysis following Parker.8 We can write down the equation for conservation of mass in a differential element of the tube as ∂A ∂(AU ) + =0 (1.1) ∂t ∂x where A(x, t) is the cross-sectional area of the tube, U (x, t) is the flow velocity averaged over the cross-section and t is time. We also have the conservation of momentum in the differential element as ∂U ∂U 1 ∂P +U + =0 ∂t ∂x ρ ∂x (1.2) where ρ is the density of blood and P is the pressure in the tube averaged over the cross section. We also write down a “tube law” A(x, t) = A(P (x, t); x) (1.3) which just says that the area is some function of the local pressure and distance only. We can write down an explicit relationship for (1.3)9 or allow A to depend directly on t but for simplicity again following Parker I keep (1.3) as is. At this point we use the tube law to elimate the derivatives of one variable from (1.1) and (1.2), constructing a matrix equation in two variables which can be solved by Riemann’s method of characteristics. These variables are typically pressure and velocity but they should be chosen depending on the application so following Biglino et al.10 we use area and velocity which are our measured variables. As such we write the x-derivative of P as ∂P 1 ∂A = (1.4) ∂x t AP ∂x t ∂A where AP = ∂P so that (1.1) and (1.2) become x U ∂ + 1 ∂t ρAP A ∂ A = 0 U ∂x U 0 (1.5) These equations are hyperbolic, which means according to the method of characteristics we can solve along the “characteristic directions” which are the eigenvalues of the matrix of coefficients of the x-derivative 1 2 A λ± = U ± (1.6) ρAP 4 But we note that, as we define the distensibility, which is the fractional change in area with a change in pressure AP D= (1.7) A this is nothing more than the wave speed c as first defined by Bramwell and Hill11 where 1 c= √ = ρD A ρAP 1 2 (1.8) so that λ± = U ± c (1.9) Therefore, as Parker states: “any perturbations introduced into an artery will propagate as a wave with the speed U + c in the forward direction and speed U − c in the backward direction.” This analysis can be continued as it is by Parker to derive the wave intensity, which is a useful way of quantifying the pulse waves in arteries and preceded the reservoir-wave hypothesis but is not necessary for its development. Really the important point is that this model admits a rigorous but straightforward description of waves travelling at a single speed c which can be determined from measurements of two of the variables A, U and P . Also again note that pressure and area are related through the distensibility as dP 1 = d ln A D (1.10) and that, once c is measured, D can be determined from (1.8). This means that any differential relationship in terms of P can be recast in terms of ln A, which is central to the focus of this project. 2 Reservoir Wave Hypothesis 2.1 Overview The concept of the reservoir in haemodynamics is an old one. In 1899 Frank12 presented his Windkessel model of arterial mechanics. The terms “Windkessel” and “reservoir” are in this context interchangeable. The model represents the arteries as a single compliant compartment also with a single resistance. This is a very elegant model showing the importance of compliance in the arteries: with a periodic influx of blood a rigid arterial system would exhibit periodic outflow. Sufficient compliance allows constant outflow, as the compliant compartment (the reservoir) fills with blood during systole and relaxes during diastole, releasing its contents. The model predicts exponentially falling pressure and this is indeed seen in diastole, as in Figure 1b. However, the model does not account for the sharp rise in pressure seen in systole. For this reason a more popular approach of late has been one which separates the pressure waveform into a combination of forward and backward travelling waves.13 This 5 Figure 3: The separation of velocity and pressure waveforms with and without the reservoir. The measured waveforms are in black, separated forward and backward waves in blue and red, and the reservoir pressure is in green. From Parker.8 is done through a continuation of the above mathematics which I will not present here. This analysis provides a good description during systole, where the separation produces an initial forward compression wave followed by backward reflected waves. However in diastole this approach predicts large cancelling forward and backward waves as “this is the only way that the wave theory can explain a falling pressure and a zero velocity”.8 The reservoir-wave hypothesis is an attempt to combine these two methods and benefit from the good predictions of the wave theory in systole and the Windkessel, or reservoir, theory in diastole. The reservoir-wave approach is itself rather young, beginning with Wang14 in 2003. Figure 3 from Parker8 demonstrates this synthesis. On the left is the separation of pressure and velocity waveforms into forward and backward waves. On the right is the inclusion of the reservoir which is subtracted from the measured waveform. Note that the reservoir pressure, in green, approximates the measured pressure well in diastole but not in systole, and that it resolves the problem of unphysical large cancelling velocity waves in diastole. 6 Figure 4: From Wang et al.,14 presented in Tyberg et al.15 The data are from anaesthetised dogs. The top panel shows the aortic, reservoir and left ventricular pressures.The bottom shows the wave pressure and the in- and outflows. Pwave and Qin are scaled to their peak values to show the proportinality. 7 The “wave” or “excess” (again interchangeable) refers to the remaining part of the pressure waveform when the reservoir is subtracted. It is found to have the interesting property of being proportional to the flow into the arterial system as shown in the bottom part of Figure 4. According to Tyberg this is “indicating that the nearly identical, superimposed Pwave and Qin waveforms result only from the forward-traveling compression and decompression waves generated by the LV [left ventricle]”.15 The reservoir pressure is derived from its definitive properties below, but from the nature of the reservoir as a single compartment we also have the the property that Pres = P (t); Pwave = P (x, t) (2.1) The reservoir pressure is the same at all points in space and only the wave pressure changes, hence its identification as a wave. 2.2 Mathematical Formulation We can now derive an analytical expression for the reservoir pressure. Following Tyberg15 we say that, as the reservoir is a single compliant compartment, the rate of change of the reservoir pressure must be equal to the rate of change of volume multiplied by a proportionality constant which is the inverse of the compliance C = dV dP . Secondly, the rate of change of volume is just the instantaneous difference between the flow of blood in Qin (t) and out Qout (t) of the system. So dPres 1 = (Qin − Qout ) dt C (2.2) Next we make the assumption that the outflow can be described by a simple resistive relationship so that 1 Qout = (Pres − P∞ ) (2.3) R where P∞ is the asymptotic pressure at which flow from the arteries ceases. Substituting (2.3) into (2.2) we get dPres Pres − P∞ Qin (t) + = (2.4) dt RC C which we can solve to Z e−t/τ t 0 −t/τ Pres = P∞ + (P0 − P∞ )e + Qin (t0 )et /τ dt0 (2.5) C 0 with P0 the pressure at t = 0 and τ = RC. To evaluate the reservoir pressure for all time we need the parameters τ , C and P∞ . To do this we say that after a certain time T in diastole Qin = 0. This is largely a good assumption as the aortic valve is closed after systole. Under these conditions (2.5) becomes a simple exponential Pres = P∞ + PT e−t/τ 8 (2.6) By fitting this expression to the data the parameters τ and P∞ can be found. Secondly, the resistance R can be calculated from the mean of the measured pressure and flow rate over the cardiac cycle. C is then determined from τ and R allowing Pres to be calculated for all time from (2.5). There are a number of methods for fitting the exponential to find the parameters but Wang and others use a Nelder-Mead simplex method to minimise the least squares error over the last two thirds of diastole.14 2.3 Applications and Reception The entire validity of the reservoir-wave approach comes down to its use in clinical applications, which have turned out to be many. Differences in the reservoir or excess pressure can be markers of cardiovascular problems and by the separation information can be gained about the effects of pharmacological interventions. For instance Davies et al., trying to gain understanding on the results of large-scale drug trials, assessed the augmentation index which is a metric of cardiovascular health. They found that “the augmentation index is principally determined by aortic reservoir function and other elastic arteries and only to a minor extent by reflected waves.”16 They therefore concluded that “modifying the behavior of the arterial reservoir rather than changing wave reflection may be a useful target for future therapy.” In another study it was found that “[excess pressure] integral was a significant predictor of cardiovascular events after adjustment for age and sex” and therefore “measurement [of it] offers a potentially new tool for selection of pharmacological therapies on a patient-specific basis.”17 Certainly this is an active area and there are a number of ongoing attempts to apply the approach in a clinically useful way.1819 Tyberg stated in 2014 that “Clinical studies employing the Reservoir-Wave Approach should be undertaken to verify experimental observations and, perhaps, to gain new diagnostic and therapeutic insights.”20 These potential applications are in large part the motivation for this project. The concept of the reservoir-wave is certainly interesting and has many proponents. It also however has its detractors. Mynard and Smolich21 claim the formulation “contains internal inconsistencies and does not provide incremental clinical value compared with conventional wave separation.” The criticism is focussed on the fact that the reservoir pressure can appear to have wave-like properties, thus violating its spatial invariance (2.1). Consideration of this disagreement is outside the scope of this project, but it is important to know that this approach is not beyond controversy and has not reached its full development. 3 Implementation with Area Data: Results and Discussion The main focus of the original work in this project is to implement the reservoir-wave hypothesis using area and velocity data which can be derived from non-invasive CMR as described in section 1.2. From CMR we essentially have the area A and velocity U as functions of time, although sampled with a certain time resolution which was is 9 typically around 10ms, and from this also the flow as Qin = U A. I have incorporated all the analysis into a Python script. General wave intensity analysis and separation into forward and backward components has been applied using this sort of data10 with promising results so we expect something similar from separation into reservoir and wave. 3.1 Formulation Mathematically, we can recast (2.4) in terms of area using the distensibility relationship (1.10) as d ln Ares ln Ares − ln A∞ D + = Qin (t) (3.1) dt RC C and solve analogously to Z D −t/τ t 0 −t/τ ln Ares = ln A∞ + (ln A0 − ln A∞ )e + e Qin (t0 )et /τ dt0 (3.2) C 0 Again if we say that during late diastole after some time t = Tld the inflow Qin = 0 then (3.2) becomes ln Ares = ln A∞ + (ln A0 − ln A∞ + ln AT )e−t/τ where D ln AT = C . Z Tld 0 Qin (t0 )et /τ dt0 (3.3) (3.4) 0 At this point the analysis differs from the pressure formulation. Due to the differential relationship between A and P we do not have access to the mean pressure, and so not to the resistance. This means the fitting is not quite as simple as in section 2.2 as if we just fit to find τ and ln A∞ we would not be able to find C and so could not calculate ln Ares for all time. Instead we can use the data to estimate C. After Tld , ln Ares is a function of the three reservoir parameters. ln Ares (ln A∞ , τ, C) = ln A∞ + (ln A0 − ln A∞ + ln AT (τ, C))e−t/τ (3.5) To determine the parameters I first set the cutoff time Tld as the time when the inflow Qin first goes to 0. Then I define a sum of squares function which measures the total squared difference between this function and the data as X S(ln A∞ , τ, C) = (lnAdata − lnAres (ln A∞ , τ, C, ti ))2 (3.6) i i where the sum is over all points i for which t > Tld S is then minimised using a Nelder-Mead simplex algorithm in Scipy to produce the three parameters ln A∞ , τ and C. Note that this is equivalent to fitting a simple exponential to find the two parameters ln A∞ and τ and then inverse solving (3.5) to find C but this method allowed more flexibility when I later attempted to use bounded optimisation. 10 3.2 Feasibility To test the feasibility of this approach I applied the analysis to 10 sets of data taken from healthy volunteers. This was area and velocity data from the ascending aorta as well as distensibility calculated from the wave speed. The time resolution was 9.56ms. I ran the exponential fitting in each case and the parameters which resulted are shown in Table 1. The results were largely positive: for 8 out of the 10 cases the fitting algorithm converged onto parameters than are physically realistic and with a reasonably tight distribution. For all cases the fitting was robust in that changing the initial parameter values did not make a difference to the result: the optimisation algorithm appears to find a global minimum. Four examples are shown in Figure 5. These show the reservoir which is fitted to the raw log-area data, and the flow and excess log-area, in analogy to the pressure graphs in Figure 4. The good fitting of the reservoir to the data can be seen along with the noisiness of the data which made the fitting problematic. Most importantly, there is largely a well-approximated linear proportionality between the flow and the excess, which shows the method works as expected. In 2 out of the 10 cases (#s 3 and 8) the fitting algorithm settles on values which are not physically realistic. Some of the area data takes on a shape significantly different from the expected increase in systole and decay in diastole exhibited by the pressure graphs in Figure 4 and the log-area graphs in Figure 5. Because the data’s resemblance to a decaying exponential is reduced the “best fit” exponential turns out to be something unphysical and essentially the fitting fails. I attempted to overcome this by fitting with a different method, Sequential Least SQuares Programming (SLSQP), which allows the parameter space to be bounded. In this way I was able to force the convergence to a physical range, but this method turned out to be highly sensitive to the initial parameter values that are put into the search. It was therefore unsuitable. There exist methods such as the Levenberg–Marquardt Volunteer # 1 2 3 4 5 6 7 8 9 10 ln A∞ 0.97 1.49 -1.54×108 1.30 1.61 1.77 1.37 -3.42×104 1.32 1.58 τ 2069.01 490.65 4.18×1010 1164.17 963.58 635.16 340.35 4.79×107 599.32 413.24 C 0.51 0.24 0.56 0.92 1.72 0.55 0.24 0.42 0.44 0.63 Table 1: Fitted parameters for the 10 volunteer data sets for the feasibility study. 11 Figure 5: Graphs for 4 sets of volunteer data. In each case the first graph is the log-area data (blue) and the reservoir fitted to the exponential part (green) plotted against time. The second graph is the excess (black), which is the data minus the reservoir, and the flow (red) against time. These are scaled to have their maxima both at 1. 12 algorithm which may be able to overcome this issue and be both robust and bounded, but I was unable to investigate these within the timeframe of this project. It would be a useful extension to the project to do so. This highlights a problem with this method of fitting the exponential. In essence, the parameter space is relatively flat, meaning the sum of squares function (3.6) will not drastically increase if the parameters are changed slightly from their optimised values. The SLSQP method hops between local minima depending on the initial parameter values because the parameter space does not converge straightforwardly to a minimum. This is a problem with the method but also a sign that we may need to be careful assigning too much importance to the optimised parameters as they are affected by noise in the data. Another issue is that there is often non-negligible flow in diastole. This breakdown of one the assumptions of the model will cause the fitted parameters to deviate from their true values. It may be possible to include diastolic flow in the analysis, for instance by fitting a general form of equation (3.2) to the data, which would take into account the Qin integral over all time. Then all of a reasonable region of the parameter space could be searched to find the best fit. This would not be computationally trivial but it would be possible and would resolve the issue of non-negligible diastolic flow. 3.3 Proof of Concept As a further proof of concept study, I applied the analysis to data from two differing groups. These were a further 5 healthy, young volunteers (4 males, age range 25-37) and 5 older patients with confirmed coronary artery disease referred for clinical CMR (4 males, age range 53-74). Again the data was from the ascending aortic position and the time resolution was 9.56ms. The parameters which resulted from the exponential fitting are shown in Table 2. I did not have access to the distensibility in each case. This means I could not determine the value of the compliance C but in terms of τ and ln A∞ the fitting is unchanged, so I just present these. This time 3 out of the 10 examples did not converge satisfactorily. Again this issue may be able to be resolved but for now I had to just exclude these cases. The mean values of the parameters excluding those which did not converge to physical values are also shown. There appears to be some difference between the two groups in terms of the parameters ln A∞ and τ . This is what we would expect if the analysis is sound. The groups would have greatly different arterial systems due to the age and pathological differences so if the parameters have any physical meaning they should certainly differ. However the sample size is far too small to enable any statistics. Having discussed the feasibility of the method and considering these encouraging albeit preliminary results, the next step would be to apply this technique to larger samples of data and assess what differences could be detected between different patients groups, or between patients and controls. CMR imaging based wave intensity has shown some interesting results,1022 particularly in congenital heart disease where ventriculo-arterial coupling is compromised, and there may be similar scenarios where the complexity of the 13 Healthy volunteers Volunteer # ln A∞ τ 1 1.40 121.05 2 1.08 468.41 3 -4.45×106 5.77×109 4 0.60 201.99 9 5 -4.17×10 8.60×109 Mean 1.03 263.82 Older patients Volunteer # ln A∞ τ 1 1.33 879.33 2 1.55 1665.04 3 1.90 540.30 4 -1.21×107 2.64×1010 5 1.61 124.00 Mean 1.60 802.16 Table 2: Fitted parameters for the 5 volunteer and 5 patient proof of concept study. physiology could be further unravelled by gathering additional insight using the reservoir method. Indeed, as described in section 2.3, the reservoir-wave separation of the pressure waveform has found numerous promising clinical applications, and given the parallels between the pressure and area formulations that I have demonstrated there is every reason to expect similar applications could be found with the reservoir-wave separation of the area waveform. For instance, Tyberg et al. have related diastolic hypertension to alterations in the asymptotic reservoir pressure P∞ , saying “Diastolic hypertension would seem to be related most directly to alterations in reservoir pressure, particularly P∞ and reservoir resistance.”18 A similar study could look at the affect of hypertension on the asymptotic area A∞ . It is probably inadvisable to attach too much physical significance to A∞ but in the model it represents the asymptotic area at which flow from the arteries ceases. This does not seem too abstracted and it would be very interesting to investigate how it correlates with certain conditions and pharmacological interventions, particularly as area data can be gathered non-invasively unlike pressure. Furthermore, the parameter τ can give insight into ventricular relaxation. Nagueh et al. state that “τ is a widely accepted invasive measure of the rate of LV relaxation”.23 A non-invasive measurement of τ may be very useful, for example in children with diastolic dysfunction. According to Dragulescu “Assessment of DD [diastolic dysfunction] in childhood CM [cardiomyopathy] seems inadequate using current guidelines. The large range of normal pediatric reference values allows diagnosis of DD in only a small proportion of patients”24 when using echocardiography. Therefore getting information on τ from CMR could be desirable in children with presumed diastolic dysfunction. 3.4 Comparing Ascending and Descending Aorta Finally, we thought it may be interesting to compare the form of the reservoir area in two parts of the arterial network in the same volunteer. Data was recorded for healthy volunteers in two instances, one for the ascending aorta just above the aortic root and a separate acquisition in the descending aorta at the level of the diaphragm. The time resolution was again 9.56ms. 14 Figure 6: Comparison of the log of the reservoir area for the ascending (magenta) and descending (cyan) aorta. The motivation for this was to investigate how the property (2.1), that the reservoir pressure is theortically invariant in space, transferred into the area formulation. Immediately it was evident that it did not, as for all cases the reservoir log-area from the two aortic sections did not relate to one another. An example is shown in Figure 6. Fitting to the descending data was overall quite problematic because the data was extremely noisy. However the conclusion that the reservoir area does change over the aorta is probably not surprising. This can be considered a statement that the distensibility varies with x, which is completely expected as the elastic properties of arteries have been shown to vary along the aortic tree.25 4 Conclusion I have demonstrated the validity of the reservoir-wave hypothesis when applied to area data rather than the tradiational formulation in terms of pressure. Application of the analysis to volunteer cardiovascular magnetic resonance data largely produced the expected functional forms of the reservoir and wave areas, analogous to those seen in pressure data. The optimisation method failed for 2 out of 10 cases but I have suggested variant methods which may circumvent this problem. As a proof of concept I applied the analysis to patient and control groups which 15 should have varying reservoir-wave parameters. The mean values of these parameters show a difference, but the sample sizes are too small to assess significance. With reference to uses found for the pressure reservoir-wave I have suggested that the parameters of the area reservoir-wave may have similar application that could enhance understanding of cardivascular function under pathological or pharmacological influence. I investigated the variation of the form of the area reservoir in different sections of the aorta. It was found that unlike the pressure reservoir, the area reservoir does not retain its form across the arterial system. This work was largely a proof of principle, and there are a number of potentially fruitful directions to take it in, some of which I have outlined in Sections 3.2 and 3.3. In addition, it would be desirable to integrate the analysis of the reservoir-wave into the existing framework of image analysis and wave intensity analysis in OsiriX. This would allow immediate evaluation of the reservoir parameters and make any large-scale analysis greatly more straightforward. References 1 J. Betts, Anatomy and Physiology. 2013. 2 “http://antranik.org/blood-vessels/,” March 2015. 3 “http://people.ece.cornell.edu/land/,” March 2015. 4 J. Lotz, C. Meier, A. Leppert, and M. Galanski, “Cardiovascular flow measurement with phase-contrast mr imaging: Basic facts and implementation 1,” Radiographics, vol. 22, no. 3, pp. 651–671, 2002. 5 F. Odille, J. A. Steeden, V. Muthurangu, and D. Atkinson, “Automatic segmentation propagation of the aorta in real-time phase contrast mri using nonrigid registration,” Journal of Magnetic Resonance Imaging, vol. 33, no. 1, pp. 232–238, 2011. 6 K. H. Parker and C. Jones, “Forward and backward running waves in the arteries: analysis using the method of characteristics,” Journal of biomechanical engineering, vol. 112, no. 3, pp. 322–326, 1990. 7 M. Willemet and J. Alastruey, “Arterial pressure and flow wave analysis using timedomain 1-d hemodynamics,” Annals of biomedical engineering, pp. 1–17, 2015. 8 K. H. Parker, “An introduction to wave intensity analysis,” Medical & biological engineering & computing, vol. 47, no. 2, pp. 175–188, 2009. 9 L. Formaggia, D. Lamponi, and A. Quarteroni, “One-dimensional models for blood flow in arteries,” Journal of Engineering Mathematics, vol. 47, no. 3-4, pp. 251–276, 2003. 16 10 G. Biglino, J. A. Steeden, C. Baker, S. Schievano, A. M. Taylor, K. H. Parker, and V. Muthurangu, “A non-invasive clinical application of wave intensity analysis based on ultrahigh temporal resolution phase-contrast cardiovascular magnetic resonance,” J Cardiovasc Magn Reson, vol. 14, no. 57.10, p. 1186, 2012. 11 J. C. Bramwell and A. Hill, “Velocity of transmission of the pulse-wave: and elasticity of arteries,” The Lancet, vol. 199, no. 5149, pp. 891–892, 1922. 12 K. Sagawa, R. K. Lie, and J. Schaefer, “Translation of otto frank’s paper “die grundform des arteriellen pulses” zeitschrift für biologie 37: 483–526 (1899),” Journal of Molecular and Cellular Cardiology, vol. 22, no. 3, pp. 253 – 254, 1990. 13 F. Pythoud, N. Stergiopulos, and J.-J. Meister, “Separation of arterial pressure waves into their forward and backward running components,” Journal of biomechanical engineering, vol. 118, no. 3, pp. 295–301, 1996. 14 J.-J. Wang, A. B. O’Brien, N. G. Shrive, K. H. Parker, and J. V. Tyberg, “Timedomain representation of ventricular-arterial coupling as a windkessel and wave system,” American Journal of Physiology-Heart and Circulatory Physiology, vol. 284, no. 4, pp. H1358–H1368, 2003. 15 J. V. Tyberg, J. E. Davies, Z. Wang, W. A. Whitelaw, J. A. Flewitt, N. G. Shrive, D. P. Francis, A. D. Hughes, K. H. Parker, and J.-J. Wang, “Wave intensity analysis and the development of the reservoir–wave approach,” Medical & biological engineering & computing, vol. 47, no. 2, pp. 221–232, 2009. 16 J. E. Davies, J. Baksi, D. P. Francis, N. Hadjiloizou, Z. I. Whinnett, C. H. Manisty, J. Aguado-Sierra, R. A. Foale, I. S. Malik, J. V. Tyberg, et al., “The arterial reservoir pressure increases with aging and is the major determinant of the aortic augmentation index,” American Journal of Physiology-Heart and Circulatory Physiology, vol. 298, no. 2, pp. H580–H586, 2010. 17 J. E. Davies, P. Lacy, T. Tillin, D. Collier, J. K. Cruickshank, D. P. Francis, A. Malaweera, J. Mayet, A. Stanton, B. Williams, et al., “Excess pressure integral predicts cardiovascular events independent of other risk factors in the conduit artery functional evaluation substudy of anglo-scandinavian cardiac outcomes trial,” Hypertension, vol. 64, no. 1, pp. 60–68, 2014. 18 J. V. Tyberg, N. G. Shrive, J. C. Bouwmeester, K. H. Parker, and J. Wang Jr, “The reservoir-wave paradigm: potential implications for hypertension,” Current Hypertension Reviews, vol. 4, no. 3, pp. 203–213, 2008. 19 S. S. Sridharan, L. M. Burrowes, J. C. Bouwmeester, J.-J. Wang, N. G. Shrive, and J. V. Tyberg, “Classical electrical and hydraulic windkessel models validate physiological calculations of windkessel (reservoir) pressure,” Canadian journal of physiology and pharmacology, vol. 90, no. 5, pp. 579–585, 2012. 17 20 J. V. Tyberg, J. C. Bouwmeester, K. H. Parker, N. G. Shrive, and J.-J. Wang, “The case for the reservoir-wave approach,” International journal of cardiology, vol. 172, no. 2, pp. 299–306, 2014. 21 J. P. Mynard and J. J. Smolich, “The case against the reservoir-wave approach,” International Journal of Cardiology, vol. 176, no. 3, pp. 1009 – 1012, 2014. 22 G. Biglino, S. Schievano, J. A. Steeden, H. Ntsinjana, C. Baker, S. Khambadkone, M. R. de Leval, T.-Y. Hsia, A. M. Taylor, A. Giardini, et al., “Reduced ascending aorta distensibility relates to adverse ventricular mechanics in patients with hypoplastic left heart syndrome: noninvasive study using wave intensity analysis,” The Journal of thoracic and cardiovascular surgery, vol. 144, no. 6, pp. 1307–1314, 2012. 23 S. F. Nagueh, C. P. Appleton, T. C. Gillebert, P. N. Marino, J. K. Oh, O. A. Smiseth, A. D. Waggoner, F. A. Flachskampf, P. A. Pellikka, and A. Evangelista, “Recommendations for the evaluation of left ventricular diastolic function by echocardiography,” Journal of the American Society of Echocardiography, vol. 22, no. 2, pp. 107–133, 2009. 24 A. Dragulescu, L. Mertens, and M. K. Friedberg, “Interpretation of left ventricular diastolic dysfunction in children with cardiomyopathy by echocardiography problems and limitations,” Circulation: Cardiovascular Imaging, vol. 6, no. 2, pp. 254–261, 2013. 25 T. T. Tanaka and Y.-C. Fung, “Elastic and inelastic properties of the canine aorta and their variation along the aortic tree,” Journal of Biomechanics, vol. 7, no. 4, pp. 357–370, 1974. 18