POST-BARIATRIC SURGERY PATIENTS VERSUS CONTROLS IN SUBSTANCE ABUSE TREATMENT
advertisement

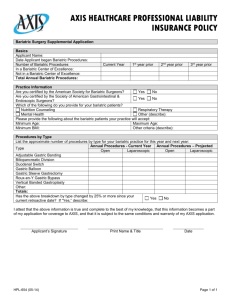
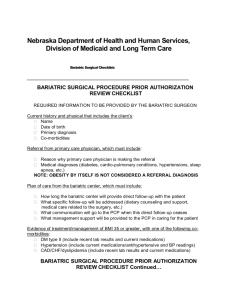
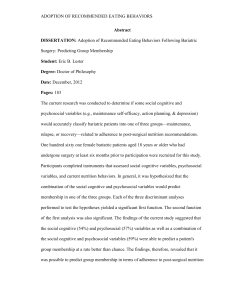
POST-BARIATRIC SURGERY PATIENTS VERSUS CONTROLS IN SUBSTANCE ABUSE TREATMENT 3 Hopper , 4 Foster-Hartsfield , Daniel John A. Joyce Ashley Valentina 1 1 1 1 1 Summar Reslan , Alisha Serras , Daniel Wood , Randi Nguyen , & Lorrianne Kukendall 1Eastern Michigan University, Ypsilanti, MI 3St. Joseph Mercy Hospital, Ypsilanti, MI of Michigan, Ann Arbor, MI 4Brighton Hospital, Brighton, MI Results Bariatric surgery candidates tend to report very low rates (1.7%) of substance use disorders at the time of pre-surgical assessment (Kalarchian et al., 2007). Evidence from our laboratory, however, demonstrates high rates of substance abuse treatment admissions among individuals who have had bariatric surgery. Specifically, we estimate that between 26% of substance abuse treatment admissions have had bariatric surgery (Saules et al., in press). Preliminary evidence suggests that for a considerable number of such individuals, onset of heavy substance use and associated problems began at some point after bariatric surgery (see Wiedemann et al., 2010). Understanding how post-bariatric patients are presenting to substance abuse treatment and how they may differ from their non-bariatric counterparts may yield important implications for prevention and treatment. Comparison of Bariatric versus Non-Bariatric Cases in the Full Sample: Relative to non-bariatric substance abuse treatment patients, those with bariatric surgery histories were significantly more likely to be female, Χ2 (1, N = 7,196) = 28.9, p < .001. With respect to admission diagnoses, bariatric and non-bariatric cases were equally likely to have been diagnosed with alcohol dependence, but bariatric patients were significantly more likely to also carry a diagnosis of alcohol withdrawal, Χ2 (1, N = 7,199) = 8.2, p < .01. Rates of diagnoses for other drug dependence categories, anxiety, and depression did not differ as a function of bariatric surgery history. Male Method Alcohol-related Diagnoses by Bariatric History Status Alcohol Dependence Female PARTICIPANTS: Chart review data from 54 post-bariatric substance abuse treatment admissions were compared with that from their matched 54 controls. Each group included 38 females and 16 males, with a mean age of 44.6 (± 9.1) years. 50 75 70.4 64.7 35.3 29.6 75 Percentage Percentage PROCEDURES: De-identified demographic and diagnostic information was exported from the electronic medical records of all patients admitted to Brighton Hospital’s rehabilitation, detoxification, and partial hospitalization programs between April 16, 2006 through May 31, 2009. The sample of post-bariatric cases was identified through a database search for the terms “intestinal bypass” or “bariatric bypass.” Matched control cases were randomly selected from the master database of 7,199 cases, matched on age (within two years), gender, and time of admission (often on the same day, but at most, within two months, to control for seasonal or cohort effects). 75 Alcohol Withdrawal 100 100 25 0 0 Bariatric Hx Bariatric Hx Neg Pos Χ 2(1, N = 7,196) = 28.9, p <.001 60.3 61.1 50.8 50 25 1 Ivezaj , 2University Introduction Gender by Bariatric History Status 1 Wiedemann , Bariatric Hx Neg Bariatric Hx Pos Χ 2(1, N = 7,199) = 8.2, p <.01 Comparison of Bariatric versus Non-Bariatric Matched Controls: Self-reported alcohol consumption per day was typically reported by patients as a range, e.g., “a pint to a fifth of vodka a day.” Therefore, the low and high end of each patient’s daily range was converted to minimum and maximum number of standard drinks per drinking day. On average, bariatric patients reported a higher minimum number of drinks per drinking day (13.1 ± 9.9 vs. 9.3 ± 6.7 drinks, t (97) = 2.2, p < .05), and, as shown, this effect was more pronounced among patients diagnosed with alcohol dependence. Presented at the 2010 Annual Meeting of the Society of Behavioral Medicine Control cases were more likely to be seeking treatment for opiate and polydrug abuse, while bariatric cases were more likely to be seeking treatment for problems related to alcohol, alcohol-plus-drug, and benzodiazepine abuse. Alcohol Consumption per Drinking Day for Alcohol Dependent Patients Min Drinks/Day Bariatric Hx Neg Bariatric Hx Pos 100 Max Drinks/Day 19.1 20 15 Reason for Treatment by Bariatric History Status 15 75 16.3 Percentage 2 Schwarz , Drinks per day Karen K. 1 Saules , 11 10 57.4 61.1 50 24.1 25 5 9.3 0 0 0 Bariatric Hx Bariatric Hx Neg Pos t (78) = 3.3, p <.01 for minimum drinks per day; t (78) = 2.4, p<.05 for maximum drinks per day. 14.8 7.4 1.9 13 0 1.9 3.7 0 5.6 Χ 2(6, N = 108) = 12.65, p<.05 Discussion Of most direct relevance to substance abuse treatment considerations, bariatric patients were more likely to carry a diagnosis of alcohol withdrawal and were consuming greater quantities of alcohol per drinking day. This finding takes on additional significance in light of evidence that bariatric patients reach higher peak BALs than controls, reach this level faster, and take longer to return to baseline (Hagedorn et al. 2007; Klockhoff et al., 2002). Faster absorption of ethanol and higher peak concentration in post-bypass patients would suggest that alcohol may serve as a stronger reinforcer among the bariatric population, thereby contributing to higher levels of alcohol intake and, by extension, putting bariatric patients at greater risk of developing alcohol problems. This heightened abuse liability could complicate the efforts of bariatric patients to achieve and maintain sobriety. Therefore, more in depth assessment of pre-surgical alcohol use and patient education regarding potential post-surgical risks is warranted. Contact: ksaules@emich.edu