UND U N I V E R S I T Y ... N O R T H D A K...

U N I V E R S I T Y O F
UND
N O R T H D A K O T A
PSYCHOLOGICAL SERVICES CENTER
210 MONTGOMERY HALL
290 CENTENNIAL DRIVE STOP 7108
GRAND FORKS, NORTH DAKOTA 58202-7108
701.777.3691
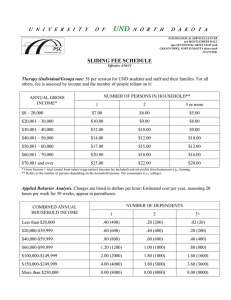
SLIDING FEE SCHEDULE
Effective 8/29/11
Therapy (Individual/Group) rate: 5$ per session for UND students and staff and their families. For all others, fee is assessed by income and the number of people reliant on it:
ANNUAL GROSS
INCOME*
1
NUMBER OF PERSONS IN HOUSEHOLD**
2 3 or more
$0 – 20,000 $5.00 $4.00 $3.00
$20,001 – 30,000
$30,001 – 40,000
$40,001 – 50,000
$50,001 – 60,000
$6.00
$8.00
$10.00
$12.00
$5.00
$7.00
$8.00
$10.00
$4.00
$5.00
$7.00
$8.00
$60,001 – 70,000 $15.00 $12.00 $10.00
$70,001 and over $18.00 $15.00 $12.00
* Gross Income = total earned from salary/wage earners (income tax included) and net profits from businesses e.g., farming.
** Refers to the number of persons depending on the household income. Not roommates (i.e., college).
Applied Behavior Analysis. Charges are listed in dollars per hour; Estimated cost per year, assuming 20 hours per week for 50 weeks, appear in parentheses.
COMBINED ANNUAL
HOUSEHOLD INCOME
1
NUMBER OF DEPENDENTS
2 3+
Less than $20,000
$20,000-$39,999
$40,000-$59,999
$60,000-$99,999
.20 (200)
.30 (300)
.40 (400)
.60 (600)
.10 (100)
.20 (200)
.30 (300)
.50 (500)
.01 (10)
.10 (100)
.20 (200)
.40 (400)
$100,000-$149,999
$150,000-$249,999
More than $250,000
1.00 (1000)
2.00 (2000)
4.00 (4000)
.90 (900)
1.90 (1900)
4.00 (4000)
.80 (800)
1.80 (1800)
4.00 (4000)
Assessment rate: Assessment (includes Interviewing, Test Administration, Scoring, Report Writing &
Feedback); Billed at a rate of $10/hour.
Type / Examples
Estimated Time*
Test-
Taking
Scoring/
Analysis
Cost
A.
Cognitive Abilities (Intellectual, attn/con, memory, exec function, etc.) 3 hrs 2 hrs $50
B.
Academic Achievement (Standard tests of achievement)
C.
Personality/Behavioral (e.g., MMPI-2 + Interview/MSE)
3 hrs
3 hrs
2 hrs
2 hrs
$50
$50
Example: ADHD/LD or Academic Disability Evaluation ( A + B + C ) 9 hrs 6 hrs $150
PAYMENT EXPECTATIONS: Fees for services are required at the time of the appointment. Clients will receive receipts for their paid fees. For assessments, at least 1/2 of the total fee must be paid before testing can begin. We do not bill insurance companies, however, these statements can be used to submit to your insurance claims department.
Should the situation arise that a client is financially unable to afford the fee (e.g., loss of job), this concern should be raised with your therapist who will inform the Clinic Director.
CLIENT AGREEMENT: Based on the above schedule, I understand that I will be expected to pay:
$_______ for individual/group therapy at the time of service, or $_______ per hour for ABA
$_______ for assessment services prior to the first assessment session
I acknowledge that these fees have been explained to me by the clinic associate, and that I agree to pay for the services as outlined in this document. If in the future my ability to pay for services changes, I will inform my therapist.
If I show up for services and am unable to pay for services based upon this agreement, I services will not be refused, but this will need to be discussed with my therapist, and directed to the Clinic Associate or Clinic
Director for further review. In this circumstance, referral to other resources may be warranted, if minimal payments are not possible.
DATE: _________ CLIENT NAME: ___________________________ CLIENT#: _________
Signature of Client Signature of Assessor/GSC
Date Reason For Review $ Approved PSC Director Signature Signature of Client