Electronic Transmission of Prescriptions and Integrated Care
advertisement

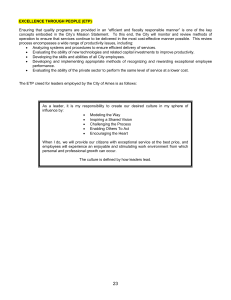
Electronic Transmission of Prescriptions and Integrated Care Records –Experience of the Evaluation of ETP Pilots Bob Sugden1 Rob Wilson2 1 Centre for Software Reliability, School of Computing Science, University of Newcastle 11th Floor, Claremont Tower, Newcastle upon Tyne, NE1 7RU, UK, +44 191 222 8007 Bob.Sugden@ncl.ac.uk 2 Centre for Social and Business Informatics, Institute of Policy and Practice, University of Newcastle, Claremont Tower, Newcastle upon Tyne NE1 7RU, UK, +44 191 222 5502 Rob.Wilson@ncl.ac.uk Keywords: Evaluation, Integrated Care Record Service (ICRS), Electronic Transmission of Prescriptions (ETP), Electronic Health Record (EHR). Abstract The proposed Integrated Care Record Service (ICRS), will in Phase 2 (2006-8) support Electronic Transmission of Prescriptions (ETP) as well as other services including the Electronic Health Record (EHR) spine. This paper reflects on the experience of evaluating three pilot implementations of ETP in England in 2002, and concludes that some findings may be relevant not only to ETP but to EHR systems and the wider implications of implementing ICRS. Introduction The DH Electronic Transmission of Prescriptions (ETP) programme is closely related to several key strands of Government policy in the NHS: • The development of prescribing, dispensing and reimbursement processes, and setting drug prices. The policy document Pharmacy in the Future set out the intentions and plans across a wide range of policy areas, affecting all the organisations that currently provide these services, with the aim being to improve the service to patients. • Wider developments in primary care, including the development of an Integrated Care Record Service (ICRS), primary care trusts, developments in contractual and employment arrangements for GPs, developing roles and responsibilities across the primary healthcare team, and developments in clinical governance. • The Information and Communications Technology (ICT) strategy for the NHS, as expressed in Delivering 21st Century IT Support for the NHS. To progress the ETP Programme the Department of Health (DH) commissioned the implementation and operation of three ETP pilots in different areas of England. These were undertaken and financed by private sector consortia and involved systems suppliers, pharmacies, NHS organisations, and patients. The consortia running the pilots were Flexiscript, Pharmacy2U, and TransScript. The scope of the pilots included acute and repeat prescribing, but did not encompass repeat dispensing, nurse prescribing, dispensing doctors, community dentist prescribing, or the prescribing of controlled drugs. The learning from the ETP pilots at the time of commissioning was intended to inform the establishment of a proposed National Prescription Service, supported by the implementation of an Integrated Care Record Service (ICRS). The intention was to explore the socio-technical context of ETP, to assess the change management issues inherent in introducing ETP to general practices, pharmacies and patients, and to develop technical standards, especially for electronic messages. To this end, a formative evaluation exercise was commissioned to run in tandem with the pilots. The key findings of the evaluation of the ETP Pilots are summarised in a report available from the DH [1]. This paper draws on that report and more detailed reports produced by the evaluation team which are not publicly available. The purpose of this paper is to draw attention to the socio-technical issues which emerged as key factors in the ETP pilots, and their relevance to implementation of ICRS; other themes of the evaluation are not reported here. Literature review The literature review for Electronic Transmission of Prescriptions (ETP) was carried out by School of Pharmacy and Pharmaceutical Sciences at Manchester University (MSP) and the Sowerby Centre for Health Informatics at Newcastle University (SCHIN). The aims of the literature review were: to acquire an understanding of electronic prescribing; to learn from what had already been researched; how it had been researched; and what are considered to be the key issues, especially incentives and barriers to ETP. The findings of the review were used to inform the evaluation criteria selected for the ETP pilots. At the point of the review there had been little published research worldwide on either the impact of electronic transfer of prescriptions (ETP) or the attitudes of stakeholders (GPs, pharmacists, patients and carers). The review therefore broadened the search to include work on prescription collection services and pharmacist-managed repeat prescribing services in the UK, to see if these studies could also provide useful insights. Although there was a considerable body of literature on electronic prescribing and in excess of 90 articles were identified, few of these actually refer to the process by which prescriptions are transmitted electronically from GP to pharmacy, and none to any subsequent transmission to an equivalent body to the NHS Prescription Pricing Authority (PPA). Those studies which did deal with the subject of ETP were generally considered to be of poor methodological quality with small, non-representative samples. Indeed, the majority of UK literature on this topic has not been published in peer-reviewed journals but has been undertaken by market research companies for an organisation contracted to deliver one of the three ETP pilots. The findings of these studies must therefore be approached with a degree of caution, but nonetheless do provide an insight into the topic. The studies suggested that community pharmacists hold an ambiguous set of attitudes towards ETP. Although there is some evidence to suggest that they are generally positive about the concept of ETP, there is also indication that some pharmacists have serious concerns, particularly relating to the potential for ‘direction’ of prescriptions to particular pharmacies, to issues of security and to restrictions of customer freedom of choice. Both UK and US literature indicates that community pharmacists prefer the ‘push’ model, in which prescriptions are sent directly from the surgery to a patient’s nominated pharmacy. The ‘pull’ model, in which prescriptions can be retrieved by third party administrators, was viewed with concern, with the integrity of the prescription regarded as a key issue. Where the impact of ETP implementation has been assessed, positive findings have been reported. Studies from the USA and Denmark suggest that ETP confers benefits for GPs, pharmacists, and patients [2]. For example: pharmacists were able to provide an increased level of counselling without increasing the time taken to process prescriptions; and ETP appears to make the whole dispensing process less time-consuming. The emphasis in the literature has been on professional perspectives and the patient perspective is largely overlooked. There is some evidence to suggest that patients do benefit from ETP as they no longer have to wait for prescriptions to be filled. However, a Danish study [3] found that expected benefits to patients in terms of less time waiting did not materialise. The authors suggested that it might not be in the interests of pharmacies for patients to spend less time waiting in the pharmacy as this could lead to a loss of business. However, UK evidence suggests that as little as 30% of customers actually purchase something while they are waiting for their prescription to be dispensed. Overall, there appeared to be support for the concept of ETP from professionals and patients, although concern remained about how prescriptions will be transmitted. Research on patient views suggested a general acceptance of the concept of ETP, albeit with some reservations relating to confidentiality and security. Although one of the issues which concerned pharmacists was the potential restriction of freedom of choice if patients had to send their prescriptions to only one pharmacy, evidence suggests that the majority of patients are in fact loyal to one pharmacy and would be happy with this situation. Many patients already nominate pharmacies to collect and deliver their prescriptions and evidence suggests high levels of satisfaction with such services. The literature review carried out as part of the ETP evaluation informed: the focus and breadth of the evaluation topics; the data collection processes in research sites; and the design of the data collection tools. Aspects not covered by the literature but included in this evaluation included technical usability, and other key areas often overlooked in evaluation of information systems, namely: policy; training; ethical; professional; and legal issues. Informatics evaluations of message transfer systems have rarely been rigorous or reported, and thus there is a lack of proven data collection approaches and tools in this area. The social aspects of the evaluation have been addressed either by the use of a tool which has been applied to a related area (e.g. work sampling approach), or by incorporating the findings from previous studies within a tool such as a questionnaire (e.g. attitudes to ETP). In the evaluation of technical aspects, it was accepted that to some extent the pilot systems would have to be regarded as ‘black boxes’, since they were owned by third parties who were under no obligation to modify their systems to provide metrics for this evaluation. Evaluation methodology and context To successfully evaluate such a large scale healthcare technology the pre-post intervention approach was determined to be appropriate. The evaluation team collected post-intervention data from operational pilots in the period June 2002 to December 2003, and compared it with pre-intervention data collected earlier in 2002. The ETP pilots themselves commenced operation in mid-2002 and were closed in June 2003. It is often difficult to identify quantitative benefits from the introduction of new information systems in their initial phase of implementation. Therefore the study design required a strong qualitative element, aimed at identifying the specific circumstances where ETP could provide benefits, as well as exploring incentives and barriers to use. The collection of structured information before, during and after a defined observation period for each pilot enabled the evaluation team to attempt to predict the pace and eventual level of user acceptance and uptake that could be expected. The aim was to identify major influential factors and/or data collection problems that could be identified early on, and be corrected or taken account of in the later stages. It was clearly recognised that the evaluation focus would be formative, due to the evolving nature of the pilots during the evaluation period, and this put the onus on the evaluation team and pilot consortia to work closely together. The evaluation team needed to present interim findings where these could be useful in making the pilots more efficient and realistic, or make the evaluation more effective, and the pilot consortia were for their part obliged to make information freely available to the evaluation team and facilitate access to participants. Attempts were made to establish formal organisational arrangements and communications processes to facilitate this. Evaluations of healthcare IT applications are by necessity multi-perspective and multidisciplinary. In order to understand the mechanisms which cause new systems and procedures to succeed or fail, it is necessary to take account of the social and work environment within which they are being introduced. The advantages of this holistic (or multi-method) approach to evaluating interventions and the social systems, or context, within which the intervention exists, have been described and demonstrated by others [4,5,6]. Figure 1: Evaluation Context: Solid lines show formal reporting or working relationships Dotted lines indicate membership of groups Not all links or relationships are shown Figure 1 demonstrates the complicated organisational context of the evaluation project, distinguishing between the ultimate customers, influencers and advisors, other organisations with an interest in the conduct of the evaluation and its outcome, and specific organisations and types of user directly involved as pilot participants. It was this latter group within which the information gathering for the evaluation took place. One of the evaluation approaches thought to be useful to the programme was approach developed by Pawson and Tilley called ‘Realistic Evaluation’ [7]. In the context of this evaluation it was used to make the case that it was crucial to distinguish between social factors and processes (individual, group, organisational) and technical processes (business activities, professional issues, computer systems) and the complex interactions between them. The approach purports to help focus on the mechanisms of change and the drivers or influencers that bring change about, and how different mechanism and agents influence the outcomes. One example of the realistic evaluation approach in this study was the perceived socio-technical interactions in consultations between GPs and patients. In ‘Realistic Evaluation’ terms this was seen to be the ‘whens’ and ‘whys’ of how GPs use the ETP facilities in their clinical record systems during patient consultations. Using this framework for the ETP Evaluation highlighted the fact that there were social and technical issues in the spread of types of participating organisation; only assessment of the design and content of the electronic messages that flow between them could be considered to be purely technical. General Pharmacy Patients Practice PPA ETP Messaging and Carers Social X X X X X X X X Factors Technical X Factors Table 1: Socio-technical issues and evaluation participants The developmental and exploratory nature of the pilots meant that qualitative research methodologies had a significant part to play in the evaluation process. This study designers understood that a range of qualitative approaches were crucial given the lack of research on the effects of electronically transferred prescriptions on the stakeholders involved. Qualitative methods allow researchers to observe work practices and explore issues raised by the subjects by reacting to and following up comments made during interviews, focus groups, and observations which will lead to in-depth understanding of the micro impacts of and attitudes to ETP [8]. Within the ‘before and after’ approach this allowed the team to observe the impacts of ETP within similar organisations with different cultures and working practices. The use of qualitative research has been strongly endorsed by a NHS Health Technology Assessment Methodological Review [9]. The review recommends the use of qualitative approaches “particularly in exploratory research to study the range of and complexity of ideas and definitions employed by individuals and groups involved in the implementation of health technologies” and concludes that this “approach can provide valuable information on the implementation and impact of health technologies on both health professionals and patients” [10]. Table 2 outlines the topics and issues that were addressed, where relevant and possible. For the purposes of the programme these were grouped under general headings. 1 Dependability of Reliability, availability, speed, security and safety of ETP architecture, messages and systems communication 2 Content of Clarity and persistence of information passing between systems. information Errors, irregularities and changes to risks of fraud 3 Changes in GP practice procedures for ordering, checking, authorising, producing, and collecting prescriptions processes of Pharmacy receiving, checking, dispensing and endorsing prescriptions communication Potential change in PPA procedures for assessing and paying dispensing claims for prescriptions Ways that patients and carers order and collect their prescriptions Changes in advice given to patients and carers Changes in communications between stakeholders 4 Service and Patient satisfaction with ETP service including convenience and willingness to participate quality of care Pharmacy and GP practice assessment of ETP service and quality 5 Workload and Potential change to PPA workload and work practices work practices of Change to pharmacy workload and work practices stakeholders Change to GP practice workload and work practices 6 Stakeholders Attitudes and beliefs of GPs, GP practice managers, and administrators attitudes to ETP and Attitudes and beliefs of pharmacy staff beliefs about ETP Attitudes and beliefs of patients and carers 7 Use of ETP Barriers and drivers for use of ETP Usability and functionality of the pilot ETP systems System ‘work around’ strategies employed by users Training and education issues 8 Implications for NHS strategy and policy issues roll-out Analysis of the costs involved with aspects of ETP Legal and regulatory issues Ethical and professional practice issues Patient confidentiality and recruitment issues Most appropriate technical and infrastructure (including network and security analysis) Most appropriate message design (including standard and solution-specific/proprietary messages) Most appropriate public key and digital signature infrastructure (including analysis of potential future technical developments) Barriers and drivers for national implementation Table 2: Evaluation topics addressed The evaluation was evolutionary in nature, and on commencement there was a significant period of negotiation between the parties involved. One of the key outcomes of the negotiations was to emphasise that the evaluation project was not designed to make commercial judgements about the ability of an individual pilot consortium to deliver one or other of the possible ETP systems. Further aims of the evaluation were to assess how the pilots performed in relation to the DH ETP Pilot Criteria and Key Professional Principles listed in the original invitation to tender issued to pilot consortia. Many of these criteria were specifically included within the evaluation elements described above; the challenges in adhering to the principles and criteria were subsequently discussed with consortia. In circumstances of non-adherence to the criteria each consortium was afforded an opportunity to discuss the constraints under which their pilot system was developed or operated, and how they might subsequently implement a revised solution. The ETP Model Commercial Context Three different architectures for ETP were chosen by the DoH for piloting. The three delivery consortia (Flexiscript, Pharmacy2U, and TransScript) were chosen on a number of criteria, a key one being the differing ETP business process models offered. All three consortia initially relied on the same GP clinical system supplier, although due to difficulties in servicing three different ETP architectures, this supplier withdrew from one pilot at the beginning of the evaluation, enforcing a switch to an alternative supplier which caused considerable delay in implementation. Technical Overview Figure 2 shows the potential flows of information in prescribing, between GP practice, patient, pharmacy and the Prescription Pricing Authority (PPA). Two of the pilots used a point-to-point connection between GP practice and pharmacy (directed prescriptions), whilst the third used a centralised messaging service (call-down relay). The minimum flows include GP to community pharmacist and pharmacist to PPA (data flow Y), mirroring the flow of the current paper-based system. In addition there are three other possible flows between GP and community pharmacist: query resolution between the pharmacist and the GP (data flow ‘β’), confirmation of dispensing to the GP (data flow Z), and notification of prescription issue by the GP to the PPA. A copy of all prescribing messages (known as the ‘gold script’) was forwarded to the PPA directly from the GP practice. All pilots facilitated electronic claims for payment by sending ‘endorsed’ prescription messages from the pharmacy to the PPA. Messages could also be sent from the PPA to the pharmacy if any claims were rejected. The Three ETP Architectures Piloted Whilst there were many differences in the technical approaches adopted by the three consortia, the issues discussed here are those properties of each business process model which have a direct impact on the users of the system. It should also be recognised that the architectures adopted in the pilots are not the only ones possible. A paper form signed by the patient was required for initial registration for any of the ETP services. pe Pa Patient or Carer r eT ok en A B pe r eT ok en W1 X1 Paper pickup by pharmacy GP Pa α Telephone β eCommuncation W2 Pharmacy W3 Rx Relay? C I ED I I ED Pa pe r Z X4 4 ED ED W I Y KEY PPA Current ETP Figure 2: Current and ETP Prescribing and Dispensing Process Messaging Flow Description A Paper FP10 prescription form (GP to patient) B Paper FP10 prescription form (patient to pharmacy) C Paper FP10 prescription form with pharmacy endorsements and exemption status information (pharmacy to PPA: used as claim for payment) 2 Prescription collection service (GP to pharmacy) 1 Information flow analogous to ‘A’ with prescription information or method of accessing prescription information using a W W token (e.g. bar-coded FP10) (GP to patient) 1 X Information flown analogous to ‘B’ with prescription information or method of accessing prescription information using a α Telephone communication (between GP and pharmacy) token (e.g. bar-coded FP10) (Patient to pharmacy) Electronic communication (between GP and pharmacy) β 3 W Electronic prescription (GP to nominated pharmacy) 4 W Electronic prescription (GP to relay) 4 X Electronic prescription (forwarded by relay to nominated pharmacy or called down by pharmacy) Y Information flow analogous to ‘C’ or paired with ‘C‘ (prescription with pharmacy endorsements and exemption status information (pharmacy to PPA: used as claim for payment) Z Confirmation of dispensing (primary compliance feedback) from PPA to GP ‘Rx’ is a common abbreviation used to indicate a prescription, hence the term ‘Rx Relay’ used in Fig. 2 Data flows not depicted: ‘gold script’ copy of prescription sent directly to PPA; ‘Call down’ of prescription from CMS/Relay by pharmacy; prescribing analysis provided to GP by PPA (ePACT) Table 3: Explanation of data flows depicted in Figure 2 Similarly, in accordance with current legislation, the patient (or patient’s representative) was required to sign a paper form to verify prescription charge exemption status if appropriate (either a paper copy of the prescription, or a special-purpose ‘exemption declaration form, depending on the pilot). The term ‘acute prescription’ is used here to describe those for which it is not anticipated there will be a repeat request, and also those that initiate medication for which a repeat prescription is possible. Requests for repeat prescriptions are usually requested by patients using the practice reception staff as an intermediary, but can also be made via a pharmacy ‘prescription collection service’, or direct to the GP in a face-to-face consultation [11]. Pharmacy2U - patient registration for ETP Patient registration for the ETP service is initiated at the pharmacy, which then sends a registration message to the GP practice. The practice system returns an acknowledgement. Pharmacy2U - patient de-registration from ETP Patient de-registration from the service is initiated at the GP practice, which then sends a message to the pharmacy. Pharmacy2U - acute prescribing via GP A prescription message is sent from the GP practice direct to the pharmacy. Pharmacy2U - repeat prescription request via pharmacy The pharmacy sends a request message to the GP practice. The GP can then generate a prescription message to the pharmacy in response, or a message to communicate any reason for rejecting the request. Pharmacy2U - repeat prescription request via GP The GP (on request from the patient) sends a prescription message to the pharmacy. Pharmacy2U - repeat request via GP practice reception staff The reception staff generate a repeat prescription which is sent to the GP for approval, who then either applies a digital signature for authorisation and forwards the message to the pharmacy, or rejects the request. Pharmacy2U - Observations The Pharmacy2U model accurately replicates the existing processes for acute and repeat prescribing. Feedback from this and the TransScript pilot is that patients liked the ability to deregister with a different healthcare professional from the one with whom they registered. As the prescribe message is received in the absence of the patient, the pharmacy can predispense medication before the patient arrives to collect it. In this pilot, ‘current medication’ information is sent with every prescription message, and also with the initial registration confirmation message. This facilitates intervention by the pharmacist, e.g. drug interaction checking; reminders to the patient of repeat medication they may need. In dispensing acute and repeat prescriptions (except at the mail order pharmacy), the patient is identified verbally, in line with current practice where prescription collection services are used. A unique service operated by one of the pharmacies involved in this pilot (confusingly named ‘Pharmacy2U Ltd’, operating a mail-order service) was to telephone patients (with their prior permission) to remind them to request repeat prescriptions. This feature was well-liked by those patients who took advantage of the mail order service. In the case of the mail order pharmacy, the form used to declare exemption status is a DH approved, amended prescription form, which the Pharmacy2U Ltd pharmacist signs on behalf of the patient. Table 4: Pharmacy2U Process Model (point-to-point messaging) TransScript - patient registration for ETP Patient registration for the ETP service is initiated at the pharmacy, which then sends a registration message to the GP practice. The practice system returns an acknowledgement. TransScript - patient de-registration from ETP Patient de-registration from the service is initiated either at the GP practice or pharmacy, initiating a message to the other party informing them of de-registration. TransScript - acute prescribing initiated via GP A bar-coded paper prescription form is used to carry the prescribing information from the GP to the pharmacy, rather than an electronic message. TransScript - repeat prescription request via pharmacy The pharmacy sends a request message to the GP practice. The GP can then generate a prescription message to the pharmacy in response, or a message to communicate any reason for rejecting the request. TransScript - repeat prescription request via GP The GP (on request from the patient) sends a prescription message to the pharmacy. TransScript - repeat request via GP practice reception staff The reception staff generate a repeat prescription which is sent to the GP for approval, who then either applies a digital signature for authorisation and forwards the message to the pharmacy, or rejects the request. TransScript - Observations The TransScript model accurately replicates the existing processes for acute and repeat prescribing. The use of a bar-coded (acute) prescription allows the patient flexibility in choice of pharmacy. The information is also in printed form, so a non-ETP pharmacy can be used. As the (repeat) prescribe message is received in the absence of the patient, the pharmacy can pre-dispense medication before the patient arrives to collect it. In dispensing repeat prescriptions, the patient is identified verbally, in line with current practice where prescription collection services are used. Table 5: TransScript Process Model (point-to-point messaging) Flexiscript - patient registration for ETP Patient registration for the ETP service is initiated at the pharmacy, which then sends a registration message to the relay, for which an acknowledgment is returned. When a GP practice connects to the service, a list of all current ETP-registered patients for that practice is downloaded to the practice system. Flexiscript - patient de-registration from ETP Patient de-registration from the service is initiated at the pharmacy, which then sends a message to the relay, for which an acknowledgment is returned. Flexiscript - acute prescribing via GP A prescription message is sent from the GP practice to the relay. A paper prescription with a bar-code and Unique Prescription Identifier (UPN) is also printed and handed to the patient. The patient takes the printed prescription (as a token of identification) to the pharmacy, which then connects to the relay and requests the prescription details electronically using the UPN. Flexiscript - repeat prescription request via pharmacy The pharmacy sends a request message to the GP practice, via the relay. The GP can then generate a prescription message to the relay in response, or a message to communicate any reason for rejecting the request. A paper prescription with a bar-code and Unique Prescription Identifier (UPN) is also printed and collected by the patient or collected on their behalf by the pharmacy. If the patient collects the paper prescription, this is taken to the pharmacy, which then connects to the relay and requests the prescription details electronically using the UPN. If the pharmacy collects the prescription, it can then contact the relay and dispense the medication prior to collection by the patient. Flexiscript - repeat prescription request via GP The GP (on request from the patient) sends a prescription message to the relay. A paper prescription with a bar-code and Unique Prescription Identifier (UPN) is also printed and handed to the patient. The patient takes the printed prescription (as a token of identification) to the pharmacy, which then connects to the relay and requests the prescription details electronically using the UPN. Flexiscript - repeat request via GP practice reception staff The reception staff generate a repeat prescription which is sent to the GP for approval, who then either applies a digital signature for authorisation and forwards the message to the relay, or rejects the request. A paper prescription with a bar-code and Unique Prescription Identifier (UPN) is also printed and collected by the patient or passed on their behalf to a pharmacy of their choice. If the patient collects the paper prescription, this is taken to the pharmacy, which then connects to the relay and requests the prescription details electronically using the UPN. If the prescription is passed directly to the pharmacy, it can then contact the relay and dispense the medication prior to collection by the patient. Flexiscript - Observations The Flexiscript model accurately replicates the existing processes for acute and repeat prescribing. The use of a relay allows the patient flexibility in choice of pharmacy. The bar-coded prescription information is also in printed form, so a non-ETP pharmacy can be used. The prescribe message is received only when the patient contacts the pharmacy, so the pharmacy can only access the prescription information and pre-dispense medication if the patient has contacted them and quoted their UPN. In dispensing repeat prescription, the patient is identified verbally, in line with current practice where prescription collection services are used. In this pilot, ‘current medication’ information is sent to the relay. Although this could be retained on the relay to form the basis of an electronic health record, for the purposes of this pilot this feature was not operated. Table 6: Flexiscript Process Modell (centralised messaging service or ‘relay’) Evaluation findings When the evaluation was designed it was assumed that observation and data collection would take place over a period of six months of live processing in the three pilots, and that during this time there would be at least 100,000 electronic prescribe/dispense messages. Commissioning of the pilots was delayed by the necessity to undergo a rigorous programme of technical testing for each site connected (imposed by the PPA), which added considerably to the consortia effort. Specific constraints on functionality were imposed by the DH, which required some reengineering of the consortia models, and this also had to be taken into account when evaluating aspects of the pilots. Initial methods used to recruit patients resulted in a very slow take up of ETP, and additional recruitment methods were eventually employed to increase the numbers of patients using ETP. The take-up of ETP was slower than anticipated, and the volume of messages much smaller than expected, although in the last two months of 2002 it reached significant volumes (an aggregate of nearly 15,000 dispensed prescriptions from 34 GP practices and 23 pharmacies) and in the early part of 2003 (after evaluation ceased) was continuing an upward trend. This obviously constrained the effectiveness of the evaluation exercise. From experience with the pilots, it was clear that ETP could not feasibly be rolled out nationally on the basis of the pilot implementations, and a discussion forum was established with the objective of agreeing a single implementation approach or ‘common architecture’ for a potential ETP national roll out. This forum was coordinated by the Prescription Pricing Authority (PPA) and included representatives of the pilot consortia, service users from the primary care trusts involved in the pilots, and members of the evaluation team. Although the forum failed to reach a consensus on a common architecture, the PPA was able to make recommendations on a specification for inclusion in the proposed ICRS. The ETP pilots were closed in June 2003. At that time, the consortia were unwilling to develop implementations of a common architecture, for commercial reasons, principally the uncertainty of their future role in continuing to provide a service. Business Process Issues Several changes in business processes were observed as a consequence of the ETP pilot intervention, affecting all participants in the process. It was immediately apparent that the point of contact between pharmacy and GP practice had shifted from practice administrative staff (via prescription collection services and telephone calls) to the GP (via electronic requests for repeat prescriptions and electronic messaging to resolve queries on prescriptions). This was partly responsible for a shift in workload from administrative staff to GPs, and also caused problems when the GP was unavailable for any reason. It may therefore be more appropriate to route communication via GP practice administration staff. In two of the pilots, the GP had to sign paper prescriptions as well as electronically signing each prescription message. The electronic signing of repeat prescriptions was facilitated by a ‘bulk signing’ option. This may save time, but raised questions about attention to individual patient circumstance, and the majority of users avoided using this facility. A system design which more closely mirrored existing collaborative workflow for repeat prescribing in GP practices would probably be more acceptable. ETP did not appear to provide pharmacy staff with extra time to spend interacting with customers and providing health care advice. The amount of time patients spend in pharmacies waiting for their medication to be dispensed should in theory be reduced where the ETP solution facilitates direction of the prescription to a pharmacy in advance of the patient’s arrival in the pharmacy. In general, the incomplete development state of the pilots and unfamiliarity of the users seemed to result in an overall increase of time that patients spent waiting in pharmacies. Due to the nature of the service, patients who registered with the mail order pharmacy Pharmacy2U Ltd experienced significant changes in the way they received their medication, as they no longer had to make regular trips to the GP practice or visit the pharmacy. The latter is not essentially a consequence of ETP, but due to the ‘mail order’ business model offered by Pharmacy2U Ltd. Change Management Issues The way in which repeat prescriptions were processed pre-ETP varied considerably across GP practices and pharmacies, and this variation suggests that the impact of ETP on GP practices and pharmacies was not uniform even within any one of the pilots. In particular, the way in which ETP functions were implemented within each GP practice and pharmacy system varied, as did the operational procedures adopted by each practice and pharmacy. It was not possible to say if the majority of those patients who opted for ETP were satisfied overall, although many seemed to be unaware that anything had changed. It is important to acknowledge that some patients may want to maintain the current levels of contact with their GP practice, and this may be a potential barrier to high levels of take up of ETP, if patients continue to be offered a choice. This was a significant factor to emerge from questionnaires completed by those patients in pilot areas who chose not to take part in ETP. Findings also suggested that patient involvement in the ETP pilots was not a direct consequence of dissatisfaction with their current choice of system for ordering repeat medication. Additionally, it may be that there are different groups of patients who will be satisfied by different solutions. GPs and practice managers expect ETP to be one element leading towards the paperless practice. The attitudes of GPs and practice managers seemed to depend mainly on factors relating to their particular practice, and the difficulties encountered with new software and business processes. These problems could potentially be overcome with additional development, training, and familiarity. Practice managers and GPs were concerned about the increased need for competence with computers and technology. Practice administration staff attitudes towards ETP appeared to be influenced by concern that their role in repeat prescribing was minimal with the ETP pilots, as the workload shifted to the GP, and they would welcome an implementation which increased their involvement. Pharmacists were unsure if ETP will benefit them, although those that spend most time on operating prescription collection services seemed to feel most strongly that ETP will save them time. Issues were raised about the problems of operating dual processes for ETP and paper prescriptions, exacerbated by the necessity during the pilots to send paper copies of the prescriptions to the PPA as well as the electronic messages. Pharmacies also experienced difficulty with new software. Most GPs expressed concern that ETP could be a factor in the loss of community pharmacies. Current legislation requires a handwritten signature from the prescriber and also from the patient or the patient’s representative (when prescription charge exemption status is declared). A number of alternative methods were used in the pilots to replace this: digital signature of electronic messages by GPs, and the printing of exemption forms at pharmacies for handwritten patient signature. It is clear that the elimination of paper requires legislative change and alternative means of checking patient exemption status, such as centralised databases linked to pharmacy ETP systems. Gaining signed permission from each patient who was to use ETP also proved to be a time consuming exercise, and it was evident that pharmacy staff did not have time to recruit patients in this way. Technical Issues The pilots demonstrated that ETP is technically viable, and all three consortia successfully implemented ETP based on three different architectures and using three different message sets, all of which eventually operated as expected. Many of the performance and usability shortcomings identified appeared to be caused by system design which conflicted with existing business processes, or faulty implementation. The consortia identified and overcame a number of these problems before closure of the pilots. For the majority of GP and pharmacy systems ETP was implemented on existing hardware. Where a bar-code solution was adopted, appropriate bar-code readers were required at pharmacies, with upgraded printers at GP practices. Of the three architectures implemented, the ‘relay server’ architecture was considered the most technically complex, although it offered a more flexible service to patients. There were no major concerns with the security provided by the pilots, although potentially security compromises could occur, depending on the physical security of the installation and networks, correct software behaviour, and the behaviour of ETP users. Security analysis suggested that improved methods are needed for the secure identification of patients when collecting medication from pharmacies, to replace presentation of the paper prescription. However, current practice, for example on collecting repeat medication using a pharmacy collection service, commonly uses only verbal identification. Identification token methods based on paper prescriptions, bar-coded paper prescriptions, and ‘unique prescription numbers’ were successfully used in the pilots. Other possible solutions, such as patient entitlement or ‘smart’ cards, were not used in the pilots. It was estimated that by 2007 NHSNet could need an additional annual capacity of up to 193TB (Terabytes) to carry sufficient message traffic to support 100% of all prescriptions issued. Between 26TB & 61TB could be required in 2005 to support transmission of 50% of prescriptions, depending on the architecture employed. Although there may be advantages in adopting a ‘relay server’ approach to message forwarding, this could as a consequence generate more message traffic. Discussion of issues relevant to ICRS From their experience of evaluating the ETP pilots, their knowledge of the electronic health records pilots (ERDIP programme), and their understanding of the specification of the proposed ICRS, the authors conclude that the technical barriers to implementation may be the lesser of the problems confronting successful adoption of such systems. Specific socio-technical issues emerging included the apparent lack of understanding by suppliers of current end user business processes (resulting in clumsy work-around solutions and shifts in workloads between different classes of user); the unwillingness of suppliers to collaborate and conform to a standardised architecture and application program interfaces (API’s); pharmacy concerns over the direction of prescriptions by GPs (possibly affecting their commercial interests); and the difficulties of recruiting patients to use the service (both in terms of the resources required and the lack of perceived benefit by patients). Other issues in the process of being addressed include the adoption of a common drug dictionary (NHS Primary Care Drug Dictionary) and use of common clinical terminology (coding and classification via SNOMED-CT), to ensure that messages between system are not misinterpreted by a recipient system using a different coding scheme. It will clearly take some considerable time to migrate all systems and users to these new standards. Acknowledgements The evaluation of the ETP pilots was a collaborative project between the Sowerby Centre for Health Informatics at Newcastle; the School of Pharmacy and Pharmaceutical Sciences (University of Manchester); the Industrial Statistics Research Unit (University of Newcastle) and QinetiQ. The Principal Investigator was Professor I.N. Purves. Thanks are due also to the pilot consortia, GP practice and pharmacy staff, and not least to the patients for their assistance in providing information to assist with the evaluation. References 1. Summary Report on the Evaluation of Pilots for Electronic Transmission of Prescriptions http://www.doh.gov.uk/pharmacy/etp.htm 2. Moorman PW, Bernstein K (eds). The CoCo project report. 1999. Odense, Danish Centre for Health Telematics. Accessed through the CoCo website October 2002. 3. W.J. van der Kam, P.W. Moorman, M.J. Koppejan-Mulder. Effects of electronic communications in general practice. International Journal of Medical Informatics 2000; 60: 59-70. 4. Heathfield, H.A. (2001) Evaluating clinical systems: the social programme perspective. Health Informatics Journal 7, 8-12. 5. Heathfield, H., Pitty, D., and Hanka, R. (1998) Evaluating information technology in health care: barriers and challenges. British Medical Journal 316, 1959-1961. 6. Anderson, J.G., Aydin, C.E., and Jay, S.J. (1994) Evaluating health care information systems: methods and applications. London: Sage Publications. 7. Pawson, R. and Tilley, N. (1997) Realistic evaluation, London: Sage Publications. 8. Kaplan, B., "Evaluating Informatics Applications—Social Interactionism and Call for Methodological Pluralism," International Journal of Medical Informatics, 64(1): 39-56, 2001. 9. Murphy et al. Qualitative Research Methods in Health Technology Assessment: a review of the literature. Health Technology Assessment 1998;2 (16).