Science Simulation of Clinic Electrophysiology in 3D e Human Atrium
advertisement

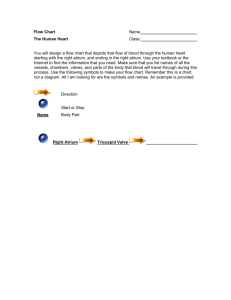
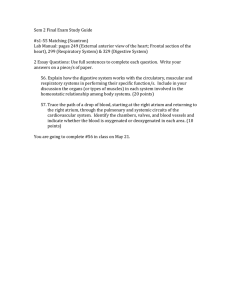
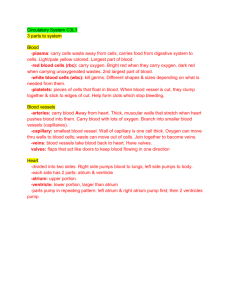
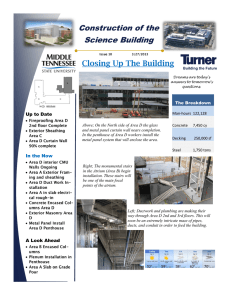
eScience Simulation of Clinic Electrophysiology in 3D Human Atrium Sanjay Kharche1, Gunnar Seemann2, Lee Margetts3, Joanna Leng3, Arun V Holden4, and Henggui Zhang1 1 School of Physics and Astronomy, University of Manchester, Manchester, M60 1QD, UK 2 Institute of Biomedical Engineering, University of Karlsruhe (TH), Karlsruhe, Germany 3 Directorate of Information Systems, University of Manchester, Manchester, M13 9PL, UK 4 Institute of Cell Membrane and Systems Biology, University of Leeds, Leeds, LS1 9JT, UK Abstract Atrial fibrillation (AF) is a common cardiac disease with high rates of morbidity, leading to major personal and NHS costs. Computer modeling of AF using a detailed cellular model with realistic 3D anatomical geometry allows investigation of the underlying ionic mechanisms in far more detail than in a physiology laboratory. We have developed a 3D virtual human atrium that combines detailed cellular electrophysiology, including ion channel kinetics and homeostasis of ionic concentrations, with anatomical detail. The segmented anatomical structure and multi-variable nature of the system makes the 3D simulations of AF large and computationally intensive. The computational demands are such that a full problem solving environment requires access to resources of High Performance Computing (HPC), High Performance Visualization (HPV), remote data repositories and a backend infrastructure. This is a classic example of eScience and Gridenabled computing. Initial work has been carried out using multiple processor machines with shared memory architectures. As spatial resolution of anatomical models increases, requirement of HPC resources is predicted to increase many-fold (~ 1 – 10 teraflops). Distributed computing is essential, both through massively parallel systems (a single supercomputer) and multiple parallel systems made accessible through the Grid. 1. Introduction AF is a condition in which the upper chambers of the heart contract at a very high rate and in a disorganized manner. As a result, the pulse of AF patients is highly irregular. AF affects about 4% of the population over the age of 60 years. Mortality rate associated with AF has increased over the past two decades. In the US, the age standardized death rate (per 100,000 US population) increased from 28 to 70 in 1998 [1]. In the UK alone, around 500,000 patients are affected by AF and the mortality rate has doubled since 1993. AF also increases the risk of stroke and heart failure among other complications. The electrophysiology of the atrium, as in other cardiac tissue, is extremely complex. The membrane potential is determined by the integrated actions of ionic channels, Na/Ca exchanger and Na/K pump currents. In addition, regulative mechanisms governing the homeostasis of intracellular calcium concentration also affects the membrane potential. Modeling such a system requires use of high order, stiff ordinary differential Figure 1. 3D anatomical model of human female atrium showing PM (blue), CT (red), RA (purple), LA (green). SAN and BB are embedded close to the CT and cannot be seen equations. For example, the Courtemanche et al. [2] (CRN) model for human atrial cells consists of 24 state-variables of ODE. Such a description is necessary for the simulation of the effects of drugs, age and genetic disorders on ionic channel kinetics and thus single cell and tissue electrical activities. Simple models, e.g. FitzHugh-Nagumo (FHN) excitation model, A 2. Heterogenities in human atrial AP and anatomy 20 mV 0 atrium pm CT appendage AV ring -20 -40 -60 -80 200 300 400 500 600 700 800 t (ms) B 1200 800 [Ca2+]i atrium pm ct appendage AV ring 400 0 200 220 240 260 t (ms) Figure 2. (A) AP heterogeneity in human atrium. LA, RA, PM and BB have an APD90 of 325 ms (solid blue), PM (dash dot-doted black), CT is 330 ms (dashed green). In the atrial appendage the APD90 is known to be 310 ms (dotted red), in the AV ring is 300 ms (dash dotted cyan). (B) Intracellular calcium concentrations associated with APs in A. Color coding and dash styles are as in A. allow fast prototyping and (relatively) computationally inexpensive alternative for simulating electrical propagation in 3D geometries. Such models can be used as a starting point for the insertion of biophysically detailed cell models into anatomically detailed tissue models. The human atrium consists of left atrium (LA), right atrium (RA), pectinate muscles (PM), cristae terminalis (CT), the Bachmann’s bundles (BB), and sino-atrial node (SAN). Figure 1 shows a composite of all these components. The SAN is the pacemaker of the heart that initiates electrical action potential (AP). PM, CT and BB assist in conduction of electrical excitation waves. The human atrium is a heterogeneous tissue with cells in different regions having different action potential characteristics, preferential conduction pathways and varied fibre orientations. The CRN model is able to simulate AP in generic human atrial myocyte. However, the electrical activity in atrium is heterogeneous. The human atrium consists of several distinctively different regions with cells in each of the regions having different AP characteristics. The LA, RA, PM and BB have similar APs with an action potential duration (APD90) of approximately 325 ms. However, in the CT the APD90 is 330 ms, in the atrial appendage the APD90 is known to be 310 ms, in the atrioventricular (AV) ring is 300 ms. The CRN model can be adapted by adjusting maximal conductances of the transient outward current (Ito), the L-type calcium current (ICaL), and the rapidly activated potassium current (IKr) to simulate these heterogeneous APs [3] based on experimental data [4]. The results are shown in Figure 2, along with the corresponding heterogeneous calcium transients. Although there is heterogeneity in AP and calcium transients, the resting potential remains almost the same (-81.5 mV), as do the upstroke velocity (220 mV/ms) and the peak potentials (25 mV). The SAN is a pacemaker, and is autorhythmic, with a period of approximately 70 per minute pacing the atrium at the base of the PM close to the CT. We have modified the CRN model by including a hyperpolarising-activated current (If) as given in Zhang et al. [5] to simulate the auto-rhythmic AP in SAN as shown in Figure 3. Details of modifications to the CRN model to simulate SAN AP are given in [3]. The 3D anatomical model for an adult female human atrium [6] was obtained from the National Library of Medicine of the National Institute of Health in Bethesda, Maryland, USA [7, 8]. This spatial resolution of the data set is much higher than that of clinical MRI. The voxel size is 0.33 mm x 0.33 mm x 0.33 mm. The data were segmented as described in [6]. In the atrium, fibre orientation is not as structured as in the ventricle. The fibre orientation of the atrial working myocardium has a complex and nearly random fashion [9]. Only the conduction pathways, i.e. CT, BB and PM and the tissue near the mitral and tricuspidal ostia, near the superior and inferior vena cavae and near the pulmonary veins have a consistent orientation. The macroscopic anisotropy of the electrical excitation conduction pattern, as well as mechanical contraction, is strongly influenced by the spatial layout of the cardio- 20 mV 0 -20 -40 -60 -80 0 500 1000 1500 2000 2500 t (ms) Figure 3. Pacemaking AP in the SAN simulated using modifications to the CRN model as given in [3]. myocytes, i.e., the orientation of the muscle fibres and layers inside the myocardium. A nearly random fibre orientation is reported inside the human SAN [10]. These fibre orientations have been incorporated in our model. Normal electrical excitation in the atrium has been reconstructed previously [5, 11]. Normal conduction starts at the SAN, which is the primary pacemaker of the heart with autorhythmic activity. Then the fast right atrial conduction pathways i.e. CT and PM transmit the excitation. During that phase, the right atrial working myocardium gets depolarised. At the same time, BBs transmit the activation towards the LA and the whole atrium is activated. All conduction pathways are characterized by a large electrical conductivity along the fibre direction. The excitation reaches the AV node, which is the only electrical path between atria and ventricles in the physiologically normal case. After a short delay, the excitation is then conducted into the ventricles. The simulated conduction pattern of atrial excitation is shown in Figure 4, using simple FHN cell model. 3. Computational resouces The simulations were performed using a number of different computing facilities. These included systems hosted by the Computational Biology Laboratories (CBL) at Leeds, the University of Manchester and the National HPC Service, CSAR [12]. At CBL Leeds a 24 processor SunFire-880 with UltraSPARC chip and a memory of 24 GB is available. The principal author’s laboratory has a 4 processor Sun-Fire-880 with UltraSPARC chip with 16 GB of memory. A local university wide (University of Manchester) SGI machine with 32 SGI R14k processors and a memory of 16 GB is also available [13]. All these are shared memory systems (SMP). A distributed memory system with 16 dual processor Sun-Blade-1000 nodes is also available at CBL, Leeds. CSAR provides, amongst other facilities, a 512 processor SGI Origin 3800 machine with 512 GB memory. Access to this system was granted through a Class 3 project, available for new users to gain access to the system for evaluation purposes. The Sun-Fire machines have suitable up to date C/C++ compilers for parallelisation using OpenMP. MPI codes are compiled with MPICH (freely downloadable from the web) on the Sun machines. CSAR has MIPSPro 7 series and Intel v series of compilers. 4. Computing aspects of the 3D model – necessisity of HPC The 3D anatomical atrial model, as described in the previous section, consists of 325 x 269 x 298 nodes. This amounts to more than 26 x 106 nodes. The following description of computing resource is based on implementation of the CRN 24 variable cell model, within human virtual atria. During a 3D simulation, the following arrays are required to be held in memory. A tissue information array (~108 integer values), the state array (109 consisting of double-precision floating-point data type), the diffusion matrix (109 double-precision floatingpoint data type), spatial derivatives are required to compute the heterogeneous conduction (108 double-precision floating-point data type). We can see that a minimum of 17.2 GB of memory is necessary. Instead of the CRN model, if a simple FHN model is used, the memory requirement is reduced to 10 GB due to a large reduction in number of independent variables associated with each node. In either case, large amounts of contiguous memory is required. The serial code for 3D models with FHN as cell model was ran to estimate scalability. Simulating 1000 time units of activity took 5 hours of computer time on a standard Sun-Fire 880 workstation. Upon parallelization, the same run for FHN case was reduced to elapsed time of 1.5 hours using 4 processors, showing good scalability. Further optimization was implemented by use of binary output. This further improved performance by 7 % for the 1000 time unit simulation. Results of this simulation are shown in Figure 4. Any pathology motivated case study requires many repeated simulations with different stimulus protocols or parameters in the model. This increases enormously the compute demand. AF due to re-entrant atrial excitation in A B C D E F Figure 4. Simulation of normal conduction pattern in human female atrium. Translucent blue denoted the atrial geometry and solid yellow represents the excitation. Propagation is from the SAN to the LA. Model is stimulated at SAN (A, t = 0) and conduction spreads in the RA and along the BB and PM into the LA (B, C, D, E, F). Simulation of 1000 time units of activity (frame F) takes 95 minutes on a standard 4 processor Sun Sparc. 3D atrium is primarily propagating scroll waves. Scroll waves can be initiated in the atrium using several protocols. Simple S1-S2 or cut wave, or the following possible protocols to initiate re-entrant scroll waves are [14]: 1. S1 would be a stimulus at SAN. Then an ectopic excitation S2 located within the RA near the superior vena cavae, 15 mm away from the SAN. 2. Another protocol is the S1-S2-S3 protocol. The S1-S2 is as the same as described above, but after a time delay, a S3 stimulus is applied to the same location of the S2. 3. This protocol rapidly paces the SAN at high frequency. This results in re-entry on the RA surface after sufficient number of stimuli. Initiation of re-entry at the required location in the 3D geometry using the S1-S2, S1-cut wave, or protocols 1 and 2 has to be done by trial and error, involving several trial simulations. Other possible stimulation protocols to induce normal and scroll waves have been described in [15, 16]. Upon using the cut wave protocol, we initiated re-entry and the results are shown in Figure 5. Such a simulation of 1 s takes about 44 hours on 16 processors using an improvement as described below. Full geometrical model demands very large amounts of contiguous memory. We have, however, exploited problem specific features in our simulations and reduced these overheads considerably. Atrial tissue geometry occupies about 8% geometry of the total data set, due to atrium being thin walled, large holes of atrial chambers and vena caves. We re-structure (or renumber) the arrays mentioned in section 4 such that the real atrial nodes (leaving out the empty nodes) of the data set, i.e. only 8% of the total 26 million nodes and related information are stored. This improved efficacy of memory usage. By re-numbering the real atrial nodes we are not storing any data points that are not atrium. This reduced the memory required by FHN model to less than 3 GB. The memory required by CRN is reduced to less than 10 GB. As a first step toward biophysically detailed modeling of human atrium, we have simulated electrical propagation using shared memory systems. A shared memory system is not necessary and the same results can be obtained using distributed memory systems. Distributed memory parallelism may give better scalability. 5. 2D Atrial and other small sized simulations Often, 2D tissue simulations offer useful insights into the mechanisms underlying the A B D E C F Fig 5. Initiation and propagation of scroll wave in human female atrium considering the healthy, or control case. Translucent blue shows atrial geometry, and solid yellow denotes propagating electrical activity. The SAN was stimulated to induce a solitary propagation. After an appropriate duration of time, the upper half of the geometry was reset to resting conditions simulating the cutexamples wave protocol (A, Following are two where t = 210 ms). Propagation of scroll wave can be seen in distributed B (t = 230 ms), C (t = 250 ms), D (t = 270 ms) memory computing can assist in and E (t = 290 ms). In control case, re-entrant scroll waves self terminate (F,and t = 1D 335tissue ms). behaviors. investigation of cell genesis of AF, without dealing with complex 3D simulations. 2D tissue simulations were performed to investigate the link between AF genesis and gain-of-function in IK1 due to Kir2.1 gene mutation [17]. In this simulation, tissue size was taken to be 37.5 mm x 37.5 mm, in accordance with normal size of atrial appendage. Spiral re-entry was initiated with a standard cross-field stimulation protocol [18]. To characterize the stability of reentry, a 10 s long run of simulations were performed for 3 cases, consisting of control, for heterozygous and homozygous Kir2.1 gene mutation. Surface potentials was taken, to allow reconstruction of animation of activity from t = 0 to t = 10 s. In addition, pseudo-ECG and spiral wave tip positions were computed at run time. Sample frames from the 2D simulation results are shown in Figure 6. Parallelization helps to reduce computing time and allows for a more intensive investigation. The program was parallelized using OpenMP and was ran on a dual processor Sun workstation. The time taken was 29 hours. We then ran it on 4 processor Sun-Fire and the elapsed time reduced to 16 hours. Our 2D code shows good scalability with near ideal speedup. The small fraction of code that has to be necessarily serial is while doing essential file output. Cell models need to be investigated for various behaviors [19]. In cell models, a generic investigation is that of pacing based behavior of AP. Detailed of biophysical cell models in themselves are not overly demanding on memory, requiring storage of several tens or few hundreds of variables (e.g. models incorporating Markov chain formulations of cellular processes). Pacing based investigations are however, long by the nature of the problem. A ventricular cell model developed by PriebeBeckmann (PB) [20] for non-failing and failing heart was pacing at various pacing rates from basic cycle length (BCL) = 100 ms, to BCL = 1200 ms in increments of 5 ms with trains of 100 stimuli. AP behavior for the final 10 stimuli were noted and plotted against BCL as a bifurcation diagram, to investigate the existence of AP alternans or 2:2 responses. Figure 7 shows the results from such a simulation. Simulation carried out on single processor as a serial run involved running this model for 60 hours. Inter-process communication in such a simulation is minimal, with the only synchronization required being in accumulation of the results. The pacing at a given BCL is independent of pacing result at another BCL. This being a cell model, the simulation is not demanding for memory of each node in the distributed memory system. Shared memory systems with large amount of memory are not required. If the code is parallelized for a I II III Figure 6. Representative frames from 2D simulations while investigating the effects of gain-offunction in IK1 on AF. Top panel shows frames for control, middle panel for heterozygous, and bottom panel for homozygous mutant type. 2D simulations at t = 400 ms in column I, t = 1300 ms in column II, and t = 2650 ms in column III. A total of 10 s of activity was simulated. 6.Conclusions and Discussions In this study, we have developed a 3D computer model of human atrium with detailed anatomical structures and cellular electrophysiology. This model provides an alternative to experimental methods to investigate the cellular ionic and molecular mechanisms underlying the genesis and control of AF in humans. Due to large size of geometry and multi-variable nature of the system, the model demands extensive computing resources 600 500 APD90 (ms) distributed memory system, then run time can be reduced drastically, depending on the number of nodes. Another example where low cost distributed memory systems can be utilized is shown in Figure 8. Here we have a 1D transmural strand of human ventricle of length 15 mm with a spatial resolution of 0.1 mm with 150 cells, of which 40 are endo-, 50 are mid-, and 60 are epi-. Computing vulnerability window (VW) at a ventricular cell location requires running the 1D serial program on 1 processor for 1.3 hours. Again, as in the cell model case, computation of VW at a cell location is independent of computation of VW at another cell location. The memory requirement by the 1D model is moderate and can be well managed by nodes of any reasonable distributed memory system. Since VW computations at each of the cell locations are independent of each other, synchronization is not required. This problem also lends itself distributed memory parallelism. heart failure Control 400 300 200 2:2 100 200 400 600 800 1000 1200 BCL (ms) Figure 7. APD90 alternans (2:2 response) in PB model. Blue denotes control, red denotes heart failure. PB model is paced at BCLs from 100 ms to 1200 ms in increments of 5 ms. Dynamic response of last 10 APs from a train of 100 was noted. Alternans occur at low BCL. and is an ideal test bed for HPC algorithms. Simulations with low memory demands, but require long computations due to nature of problem are ideal for distributed computing. 500 VW (ms) heart failure 475 450 ENDO- MID- EPI- 425 Control 400 0 2 4 6 8 10 12 14 x (mm) Fig 8. Computation of VW at each cell location of a 15 mm human virtual ventricular 1D strand with endo-, mid-, and epi- regions. A serial run of the program takes 200 hours. A single determination of VW takes 1.33 hours. Acknowledgements This work was supported by British Heart Foundation (PG/03/140) and BBSRC (BBS/B/1678X) UK. References [1] Wattingney WA, Mensah GA, Croft JB. Increased Atrial Fibrillation mortality: United States, 1980 – 1998. Am J Epidemiol. 2002; 155: 819 – 826. [2] Courtemanche M, Ramirez RJ, Nattel S. Ionic mechanisms underlying human atrial action potential properties: insights from a mathematical model. Am J Physiol. 1998 Jul; 275 (1 Pt 2): H301-21. [3] Seemann G. Modeling of Electrophysiology and Tension Development in the Human Heart. 2005; Ph.D. Thesis. University of Karlsruhe. [4] Feng J, Yue L, Wang Z, and Nattel S. Ionic mechanisms of regional action potential heerogeniety in the canine right atrium. Circ. Res. 1998; 83: 541-551. [5] Zhang H, Holden AV, Kodama I, Honjo H, Lei M, Vagues T, and Boyett MR. Mathematical models of action potentials in the periphery and centre of the rabbit sinoatrial node. J. Am. Physiol. 2000; 279 (1): H397H421. [6] Seemann G, Hoper C, Sachse FB, Dossel O, Holden AV, Zhang H. 3D anatomical and electrophysiological model of human sinoatrial node and atria. Phil. Trans. Roy. Soc., 2006. In press. [7] Ackerman MJ. “Viewpoint: The Visible Human Project”. J. Biocommunications. 18 (2): 14 1991. [8] “Visible Human Project, National Library of Medicine, Bethsda, USA”. [9] Boineau JP, Canavan TE, Schuessler RB, Cain ME , Corr PB, Cox JL. Demonstration of a widely distributed atrial pacemaker complex in the human heart. Circ. 1988; 77: 1221-1237. [10] Anderson RH, Ho SY. The architecture of the sinus node, the atrioventricular conduction axis, and the internodal atrial myocardium. J. Cardiovasc. Electrophysiol. 1998; 9: 12331248. [11] Harrild DM, Henriquez CS. A computer model of normal conduction in the human atria. 2000; Circ. Res. 87 (7): e25-e36. [12] http://www.csar.cfs.ac.uk/ [13] http://www.mc.manchester.ac.uk/services [14] Virag N, Jacquemet V, Henriquez CS, Zozor S, Blanc O, Vesin J-M, Pruvot E, Kappenberger L. Study of atrial arrhythmias in a computer model based on magnetic resonance images of human atria. 2000; Chaos 12 (3): 754 – 763. [15] Vigmond EJ, Ruckdeschel R, Trayanova N. Re-entry in a morphologically realistic atrial model. 2001; J. Cardiovas. Electrophysiol. 12 (9): 1046 – 1054 [16] Haissaguerre M, Jais P, Shah DC, Takahashi A, Hocini M, Quiniou G, Garrigue S, Le Mouroux A, Le Metayer P, Clementy J. Spontaneous Initiation of Atrial Fibrillation by Ectopic Beats Originating in the Pulmonary Veins. N Engl J Med. 1998; 339 (10): 659-666 [17] Kharche S, Moore H, Garratt CJ, Hancox JC, Zhang H. Gain-of-Function in Kir2.1 and its Effects on Atrial Fibrillation in Homogeneous Virtual Human Atrial Tissue: A Computer Simulation Study. Poster at the ISCE 31st Meeting, Niagara-on-the-Lake, Canada. April 2006. [18] Biktasheva IV, Biktashev VN, and Holden AV. Wave-breaks and self-termination of spiral waves in a model of human atrial tissue. LNCS 2005; 3504: 293-303. [19] Kharche S, Zhang H, Holden AV. Vulnerability in a One-Dimensional Transmural Model of Human Ventricular Tissue in Heart Failure. Computers in Cardiology Conference, Lyon, 2005; 32: 563-566 [20] Priebe L and Beuckelmann DJ. Simulation Study of Cellular Electric Properties in Heart Failure, Circ Res. 1998; 82 (11): 1206-1223.