Document 13309139
advertisement

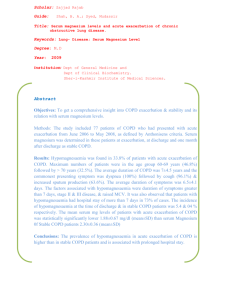
Int. J. Pharm. Sci. Rev. Res., 21(1), Jul – Aug 2013; n° 03, 10-14 ISSN 0976 – 044X Research Article Role of Eotaxin in Chronic Obstructive Pulmonary Disease (COPD) 1 1 1 Al-Midani Adnan , Al-Zain Ammar, Kwatly Khalil Faculty of Pharmacy, Damascus University, Damascus, Mezza Street, Syria. Accepted on: 09-04-2013; Finalized on: 30-06-2013. ABSTRACT Eotaxin is a chemokine which characterized by eosinophil chemotactic and activating effects. Eosinophil takes part in airway inflammation in chronic obstructive pulmonary disease (COPD). The aim was to determine eotaxin values as a biomarker in clinical evaluation of COPD patients, and to compare its levels with IL-8 and ECP levels. This study included 35 patients with exacerbation of COPD, 30 patients with stable COPD, and 23 healthy controls. Automated eosinophil count was done. Serum Eotaxin IL-8, and ECP were assessed by ELISA. Our results showed an increase in the serum levels of Eotaxin, IL-8, ECP, and Eosinophil percentage in exacerbation COPD patients [(479.484±231.331 pg/ml) (p<0.0001); (76.949±19.550 pg/ml) (p<0.0001); (48.185±17.476 ng/ml) (p<0.0001); (3.388%±2.002) (p<0.0001) respectively] compared to healthy controls. Serum levels of Eotaxin, IL-8, ECP and Eosinophil percentage in stable COPD patients increased – but less than their increase in exacerbation COPD patients – [(318.295 ± 144.882 pg/ml) (p<0.0001); (50.854 ± 11.217 pg/ml) (p<0.001); (30.675±12.688 ng/ml) (p<0.0001); (2.01%±1.506) (p>0.05) respectively] compared to healthy controls. This indicates the important role of eotaxin in the inflammatory process of the disease, and the association between eotaxin concentrations and COPD severity. Therefore eotaxin could might be used as a biomarker in the clinical evaluation of COPD. Keywords: Eotaxin, COPD, Exacerbation, Airway Inflammation, IL-8, Eosinophilic Cationic Protein. INTRODUCTION C hronic obstructive pulmonary disease (COPD) is the forth cause of morbidity and mortality in the world and represents a substantial economic and social burden. It is a preventable and treatable disease with some significant extra pulmonary effects that may contribute to the severity in individual patients. Its pulmonary component is characterized by airflow limitation that is not fully reversible. The airflow limitation is usually progressive and associated with an abnormal inflammatory response of the lung to noxious particles or gases.1 The pathological hallmarks of COPD are destruction of the lung parenchyma, which characterizes emphysema, inflammation of the peripheral airways, which characterizes bronchiolitis, and inflammation of the central airways which characterizes chronic bronchitis. Emphysema will contribute to the airflow limitation by reducing the elastic recoil of the lung through parenchymal destruction, as well as by reducing the elastic load applied to the airways through destruction of alveolar attachments. On the other hand, bronchiolitis will contribute to the airflow limitation by narrowing and obliterating the lumen and by actively constricting the airways. Interestingly, in peripheral airway epithelium of patients, goblet cell hyperplasia was associated with an increased 2 number of neutrophils. As neutrophil elastase is a remarkably potent secretagogue, the location of neutrophils within the epithelium may be crucial for the activation of the secretory function of goblet cells. Cigarette smoke, one of the causal factors of COPD, stimulates IL-8 release from bronchial epithelial cells and alveolar macrophages. IL-8 is a potent neutrophil activator, inducing neutrophil chemotaxis and increasing neutrophil adherence to endothelial and epithelial cells. The numerous functions of IL-8 in COPD have led to the proposal that the difference between patients with COPD and ‘healthy smokers’ could be related to the amount of IL-8 produced and released by airway epithelial cells. 3 In COPD airway wall eosinophilia has been observed at a level similar to that found in asthma, with an associated increase in eotaxin expression by airway sub-epithelial and epithelial cells.4 Increasing concentrations of CCL11/eotaxin were associated with increasing severity of airflow obstruction. Eotaxin is present in the serum of patients with COPD and the percentage fall in forced expiratory volume in one 5 second (FEV1) correlated with eotaxin levels. Eotaxin is a stimulus for eosinophils, inducing eosinophil migration in vitro and accumulation in vivo. It is a potent eosinophil chemoattractant which signals via CCR3, a chemokine receptor highly expressed on eosinophils. 6 Thus it is involved in both the mobilization of eosinophils and their progenitors from the bone marrow into the blood and in their subsequent recruitment into lung tissue. Furthermore this chemokine combined with the elevated levels of MCP-1 found in COPD to cause increased monocyte migration into the airways thus resulting in the increased macrophages in the tissues associated with COPD. 7 International Journal of Pharmaceutical Sciences Review and Research Available online at www.globalresearchonline.net 10 Int. J. Pharm. Sci. Rev. Res., 21(1), Jul – Aug 2013; n° 03, 10-14 MATERIALS AND METHODS ISSN 0976 – 044X 600 479.5±231.3 Eotaxin concentration pg/ml Study Subjects 500 88 individuals (74 men and 14 women) took part in this study, and they were divided into three groups: Group A : 35 patients (mean age 65.37) with chronic obstructive pulmonary disease during exacerbation, from Assad University hospital and Al-Mowasa University Hospital. Group B : 30 patients (mean age 63.36) with stable chronic obstructive pulmonary disease who had not been hospitalized for the exacerbation of the illness for the past tow month at least. Group C : 23 healthy subjects (mean age 62.78) as a control group. All of them were lifelong nonsmokers, with normal spirometry and with no history of atopy. 400 318.3±144.9 300 166.5±104.9 p<0.01 200 p<0.0001 100 0 ECOPD SCOPD Control Figure 1: levels of eotaxin in the study groups Table 1: Eotaxin sensitivity and specificity for patient’s evaluation between exacerbation and stable COPD at some cut-offs values. Serology Cut-off 220.7 303.3 390 425.5 577.8 Sera from patient with COPD and healthy individual were stored at -80° C until the assay. Sensitivity 85.30% 73.50% 67.60% 55.90% 38.20% specificity Assays The levels of CCL11/Eotaxin in sera were determined by sandwich Elisa kit (RayBio®, USA). This assay employs an antibody specific for human eotaxin coated on a 96-well plate. The concentration of eotaxin in the sera is presented as relative value compared to OD of the stander serum. Also the levels of IL-8 and ECP in sera were determined by Elisa, and Automated eosinophil count was done. Statistical Analysis 32.30% 48.40% 61.30% 77.40% 96.80% PPV 60% 62.5% 68.57% 73.10% 92.80% NPV 66.7% 60% 63.33% 58.97% 56.86% At the cut-off value 577.8 pg/ml we got a very good specificity (96.80%) which gave us a good differentiation between exacerbation and stable COPD patients (high specificity helps in the differentiation between the two patient groups). In our study this eotaxin concentration was the best value that represent the threshold between exacerbated and stable COPD patients. The area under ROC curve was 0.703. Data were analyzed using Excel (2007), SPSS version 19. Results were expressed as mean ± SD. Test was used to evaluate the relation between the variants, correlation between two variable was performed using Spearman correlation, P-value less than 0.05 was regarded as significant. The area under ROC curve were concluded to determine the diagnostic value for eotaxin. RESULTS Serum titer of Eotaxin for COPD patients and control group The average level of eotaxin were significantly higher in patient with COPD during exacerbation (X±SD: 479.5 ±231.3 pg/ml) than stable COPD patients (X±SD=318.3±144.9 pg/ml) and control group (X±SD=166.5±104.9 pg/ml), (P<0.01 and P<0.0001 respectively), Figure (1). Serum Eotaxin sensitivity and specificity for patient’s evaluation between exacerbation and stable COPD Serum eotaxin sensitivity and specificity for some cut-offs values and the results were as shown in table 1. Figure 2: Serum Eotaxin sensitivity and specificity for patient evaluation between exacerbation and stable COPD Serum Eotaxin sensitivity and specificity for differentiation between COPD patients and healthy controls Serum eotaxin sensitivity and specificity for some cut-offs values and the results were as shown in table 2. At the cut-off value 235.3 pg/ml we got a good sensitivity (73.80 %) which gave us a good Differentiation between COPD patients and healthy individuals (high sensitivity helps in the detection of the largest proportion of International Journal of Pharmaceutical Sciences Review and Research Available online at www.globalresearchonline.net 11 Int. J. Pharm. Sci. Rev. Res., 21(1), Jul – Aug 2013; n° 03, 10-14 patients). In our study this eotaxin concentration was the best value that represent the threshold between COPD patients and healthy controls. The area under ROC curve was 0.872. Table 2: Eotaxin sensitivity and specificity of differentiation between COPD patients and healthy controls at some cut-offs values. Cut-off 161.9 235.3 292.2 381.2 Sensitivity 87.70% 73.80% 64.60% 56.90% specificity 65.20% 78.30% 87.00% 95.70% PPV 87.69% 90.56% 93.33% 97.36% NPV 65.21% 51.42% 46.51% 44.00% Figure 3: Serum Eotaxin sensitivity and specificity for differentiation between COPD patients and healthy controls The diagnostic value of serum eotaxin when shared with other parameters to assess the patient's condition between stable and exacerbated disease ISSN 0976 – 044X Table 4: The diagnostic value of eotaxin when shared with other parameters for the differentiation between COPD patients and healthy controls sensitivity specificity PPV NPV Eotaxin+IL-8 92.3% Eotaxin+ECP 98.5% 60.9% 87% 73.7% 65.2% 88.9% 93.7% Correlations between serum eotaxin and the rest of the studied parameters in patients with Chronic Obstructive Pulmonary Disease A strong and statistically significant correlation was observed between serum levels of eotaxin and the eosinophil percentage in the exacerbation group (P-value <0.0001, R = 0.779). Figure 4: linear regression between serum eotaxin and eosinophil percentage in group A. A statistically significant correlation was observed between serum levels of eotaxin and the Eosinophil percentage in the stable group (P-value <0.0001, R = 0.681) The diagnostic value of serum eotaxin in the patient evaluation is between exacerbation and stable COPD at the 577.8 pg/ml cut-off, when shared with IL-8 at its 64 pg/ml cut-off or with ECP at its 47.1 ng/ml cut-off. We had got results shown in table 3. Table 3: The diagnostic value of eotaxin when shared with other parameters to assess the patient's condition between stable and exacerbated disease sensitivity specificity PPV NPV Eotaxin+IL-8 77.1% 90% 90% 77.1% Eotaxin+ECP 65.7% 83.3% 82.1% 67.7% The diagnostic value of serum eotaxin when shared with other parameters for the differentiation between COPD patients and healthy controls The diagnostic value of serum eotaxin in the differentiation is between COPD patients and healthy individuals at the 235.3 pg/ml cut-off, when shared with IL-8 at its 44.3 pg/ml cut-off or with ECP at its 16.7 ng/ml cut-off. We had got results shown in table 4. Figure 5: linear regression between serum eotaxin and eosinophil percentage in group B. A statistically significant correlation was found between serum levels of eotaxin and ECP in exacerbation group (Pvalue <0.05, R = 0.393). We did not find a statistically significant correlation between serum levels of eotaxin and IL-8 neither in exacerbation group (P-value = 0.743>0.05, R = 0.058), nor in the stable group (P-value = 0.651 >0.05, R = 0.086). International Journal of Pharmaceutical Sciences Review and Research Available online at www.globalresearchonline.net 12 Int. J. Pharm. Sci. Rev. Res., 21(1), Jul – Aug 2013; n° 03, 10-14 ISSN 0976 – 044X eosinophils and subsequently the increase in its concentration in serum during exacerbation phase, ECP in his turn has a destructive effects on the airways thus contribute to the inflammatory process. R=0.393 P=0.02 y=269.36+4.361x CONCLUSION Figure 6: linear regression between serum eotaxin and ECP in group A. Also we did not find a statistically significant correlation between serum levels of eotaxin and ECP in the stable group (P= 0.408>0.05, R= 0.157). DISCUSSION Our results showed a clear rise in the serum eotaxin levels of exacerbation group compared to stable and control groups (P<0.01, P<0.0001 respectively). And the levels of stable group were higher than control group (P<0.0001). This changes in eotaxin concentrations demonstrated that the changing in eosinophils accumulation in the lungs may be an important factor in influencing the stability of the disease. Eotaxin -signals via CCR3 which is highly expressed on eosinophils- contributes to eosinophils recruitment into inflammated lung tissue during exacerbation8 and stable COPD9. These results were similar to D'Armiento JM et al., 200910 that found significantly high levels of eotaxin in severe stages and exacerbations than the level in stable disease and controls, but they found no significantly difference between stable patients and healthy subjects. Conversely our result was similar to Jahnz-Rozyk K et al., 200011 which included 15 stable COPD patients (X±SD=286.0±101.4 pg/ml), and 15 healthy controls (X±SD=109.6±56.1 pg/ml), and the difference was 12 statistically significant (P<0.0001). Zhu J et al., 2001 also found a significant eotaxin increase in smoking patients with stable COPD than healthy non-smokers. There were a significant correlations between serum levels of eotaxin and the eosinophil percentage in the stable (P-value<0.0001, R = 0.681) and exacerbation (Pvalue <0.0001, R = 0.779) groups. These correlations explain eosinophilic inflammatory process accruing in COPD patients by eotaxin recruitment and its specific chemotactic for these cells from circulation into lung 13 tissue. Our result was similar to Fujimoto K et al., 2005 which found that eotaxin as a eosinophil chemoattractant may contributes to eosinophilic inflammation during stable phase of COPD, and may plays a role in the increase in airway eosinophilic inflammation during an acute exacerbation. There was a statistically significant correlation between serum levels of eotaxin and ECP in the exacerbation phase (P-value <0.05, R = 0.393). This correlation refers to the potential role of eotaxin in ECP release from Serum Eotxin Levels were increased in COPD patients compared with healthy people, and it had a good diagnostic value in the differentiations between exacerbated COPD patients, stable COPD patients and controls. Combination between serological measure of eotaxin with IL-8 or ECP can increase the diagnostic value in the evaluation of the patient's condition and in differentiating between patients and healthy. REFERENCES 1. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. www.goldcopd.com. Date last accessed: June 30, 2007. Date last updated: 2006. 2. Saetta M, Turato G, Baraldo S, Zanin A, Braccioni F, Mapp Ce, Maestrelli P, Cavallesco G, Papi A, Fabbri LM: Goblet cell hyperplasia and epithelial inflammation in peripheral airways of smokers with both symptoms of chronic bronchitis and airflow limitation. Am J Respir Crit Care Med, 161, 2000, 1016–1021. 3. Schulz C, Wolf K, Harth M, Kratzel K, Kunz-Schughart L, Pfeifer M. Expression and release of interleukin-8 by human bronchial epithelial cells from patients with chronic obstructive pulmonary disease, smokers, and neversmokers. Respiration, 70, 2003, 254-261. 4. Saha S, Brightling CE: Eosinophilic airway inflammation in COPD. International Journal of COPD, 1(1), 2006, 39–47. 5. Lee JS, Rosengart MR, Kondragunta V, Zhang Y, McMurray J, Branch RA, Choi AM, Sciurba FC. Inverse association of plasma IL-13 and inflammatory chemokines with lung function impairment in stable COPD: a cross-sectional cohort study. Respir Res, 14, 2007, 8-64. 6. Griffiths-Johnson, D. A., and P. D. Collins. The chemokine, eotaxin, activates guinea pig eosinophils in vitro and causes accumulation into the lungs in vivo. Biochem Biophys Res Commun, 197, 1993, 1167. 7. Traves SL, Donnelly LE. Chemokines and their Receptors as Targets for the Treatment of COPD. Curr Respir Med Rev, 1, 2005, 15–32. 8. Bocchino V, Bertorelli G, Bertrand CP, Ponath PD, Newman W, Franco C, Marruchella A, Merlini S, Del Donno M, Zhuo X, Olivieri D: Eotaxin and CCR3 are up-regulated in exacerbations of chronic bronchitis. Allergy, 57(1), 2002, 17-22. 9. Brightling CE, Monteiro W, Ward R, Parker D, Morgan MD, Wardlaw AJ, Pavord ID: Sputum eosinophilia and shortterm response to prednisolone in chronic obstructive pulmonary disease: a randomised controlled trial. Lancet, 356(9240), 2000, 1480-1485. 10. D'Armiento JM, Scharf SM, Roth MD, Connett JE, Ghio A, Sternberg D, Goldin JG, Louis TA, Mao JT, O'Connor GT, Ramsdell JW, Ries AL, Schluger NW, Sciurba FC, Skeans MA, International Journal of Pharmaceutical Sciences Review and Research Available online at www.globalresearchonline.net 13 Int. J. Pharm. Sci. Rev. Res., 21(1), Jul – Aug 2013; n° 03, 10-14 Voelker H, Walter RE, Wendt CH, Weinmann GG, Wise RA, Foronjy RF. Eosinophil and T cell markers predict functional decline in COPD patients. Respir Res, 10, 2009, 113. 11. Jahnz-Royzk K, Plusa T, Mierzejewska J. Eotaxin in serum of patients with asthma or chronic obstructive pulmonary disease: relationship with eosinophil cationic protein and lung function. Mediators Inflamm, 9, 2000, 175-179. 12. Zhu J, Qiu YS, Majumdar S, Gamble E, Matin D, Turato G, Fabbri LM, Barnes N, Saetta M, Jeffery PK. Exacerbations of ISSN 0976 – 044X Bronchitis: bronchial eosinophilia and gene expression for interleukin-4, interleukin-5, and eosinophil chemoattractants. Am J Respir Crit Care Med, 164, 2001, 109-116. 13. Fujimoto K, Yasuo M, Urushibata K, Hanaoka M, Koizumi T, Kubo K. Airway inflammation during stable and acutely exacerbated chronic obstructive pulmonary disease. Eur Respir J, 25, 2005, 640–646. Source of Support: Nil, Conflict of Interest: None. International Journal of Pharmaceutical Sciences Review and Research Available online at www.globalresearchonline.net 14