MECKLENBURG COUNTY Park and Recreation Department
advertisement

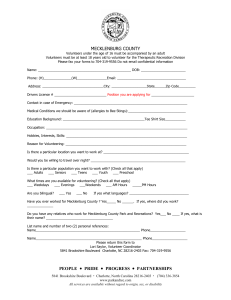
Submit by Email MECKLENBURG COUNTY Park and Recreation Department Therapeutic Recreation Division Program Accommodation Request Date: ______/______/______ Participants Name: ______________________________________________________________ Disability(s): ___________________________________________________________________ Date of Birth: ______/______/______ Program You Are Requesting Accommodates For: ____________________________________ Please note: The accommodations are based on the needs of the participant and the purposes of the program. Type of Accommodation Being Requested (check all that apply): _____ Braille or Large Print Documents _____ Change in rules and policies _____ Behavior Support Plan _____ Architectural Accessibility _____ Increased Supervision _____ Hand Over Hand Instruction _____ Adaptive Equipment/ Adaptation of Activities _____ Sign language interpreter or other alternative communication devices _____ Unsure / Other (please describe): _____________________________________________ Contact Name: ___________________________________ Phone Number: (____) _____-_____ Email Address: _________________________________________________________________ Preferred Means of Contact: _____ Phone _____ Email -------------------------------------------------------------------------------------------------------------------For Staff Use Date Received: _____/_____/_____ Meeting Date: _____/_____/_____ Staff Recommendations: _________________________________________________________ _____________________________________________________________________________ ______________________________________________________________________________ Staff Member Reviewing: ________________________________ Date: 10/22/07 PEOPLE y PRIDE y PROGRESS y PARTNERSHIPS 5841 Brookshire Boulevard x Charlotte, North Carolina 28216-2403 x (704) 336-3854 x Fax (704) 336-5472 www.parkandrec.com All services are available without regard to origin, sex, or disability Print Form