I’m Not Compacted! Left Ventricular Dysfunction in a Young Man
advertisement

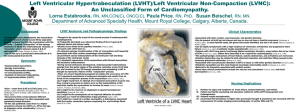
I’m Not Compacted! Left Ventricular Dysfunction in a Young Man Stephany Sanchez, MD (Associate); Jason H. Rogers, MD University of California, Davis Medical Center, Sacramento, CA LEARNING OBJECTIVES INVESTIGATIVE STUDIES HOSPITAL COURSE Isolated ventricular noncompaction (IVNC) is a rare genetic cardiomyopathy Medical management for heart failure Diuresed 8 liters and symptomatically improved Familial occurrence requires screening of first degree relatives Multiple runs of non-sustained ventricular tachycardia AICD placed Prognosis is poor given limited treatment options Close clinical follow up arranged/cardiac transplant assessment CASE INFORMATION HISTORY OF PRESENT ILLNESS: A 20 year-old Mexican man presented with dyspnea on exertion for one month. He denied any chest pain, orthopnea, PND, or lower extremity edema. He was experiencing progressively worsening palpitations over that last month. He had a 21 year-old brother who died of sudden cardiac death last year with autopsy-proven dilated cardiomyopathy. PHYSICAL EXAM: T 37 BP 103/65 P 73 R18 SaO2 98% Thin man in no acute distress Regular rate, rhythm, 3/6 holosytolic murmer at apex radiates to axilla. Laterally displaced PMI, no S3, JVD Soft, abdomen with diffuse discomfort, no hepatomegaly No lower extremity edema Siblings in Mexico contacted and screening ECHOs arranged Figure 1 Figure 2 Figure 3 Cardiovascular MRI. Enlarged left ventricle with deep trabeculations from noncompaction (arrow) Left Ventricular angiogram. Marked trabeculations (arrow) with severe mitral regurgitation Autopsy example. Compacted epicardial layer and noncompacted endocardial layer PATHOGENESIS: A Normal embryonic development C (B) Trabeculae alternate with recesses that communicate with the ventricular cavity (C) During weeks 5-8 ventricular myocardium is compacted and recesses turn into capillaries Figure 4 Normal embryonic development with compaction DIAGNOSIS: Jenni Criteria (by ECHO) Absence of coexisting cardiac problems 2 layer left ventricle wall structure: thin/compacted outer layer and thick/noncompacted internal layer LV Cardiac MRI hyper-trabeculated LV with multiple endocardial recesses and noncompacted myocardium LA Figure 5 Transthoracic Echo. Trabeculations of apical and lateral walls of LV (Inset) Blood flow in recesses Isolated ventricular noncompaction is a rare genetic cardiomyopathy. Male predominance (56-82%) Familial and sporadic cases Autosomal dominant and x-linked inheritance Pathogenesis Embryonic arrest of compaction. (Fig. 4) (A) Myocardium initially a meshwork of loosely interwoven muscle fibers ECHO ejection fraction 10%, 4 chamber dilated cardiomyopathy, 4+ mitral & tricuspid regurgitation, multiple trabeculae in left ventricle (LV) Cardiac Catheterization normal coronaries, cardiac output 3.8L/min, pulmonary capillary wedge pressure 18mmHg, elevated pulmonary artery pressures B Arrest of normal endomyocardial morphogenesis in embryonic development PERTINENT LAB/IMAGING FINDINGS: BNP 1726 AST 94 and ALT 100 Troponin 0.150.130.17 DISCUSSION Apical and mid-ventricle segments of inferior and lateral wall are affected Blood flow from LV cavity into trabecular recesses by Doppler DiagnosisECHO gold standard (Jenni Criteria) (Fig. 5) Clinical manifestations Heart failure (systolic) from subendocardial hypoperfusion Arterial thromboembolism from thrombi in trabecular recesses Arrhythmias Treatment Heart failure management, +/-ICD, +/- anticoagulation Cardiac transplantation Prognosis Sudden cardiac death 13-18%, thromboembolic events 24%, ventricular tachycardia 41%, heart failure >75% Limited treatment options result in poor prognosis REFERENCES Botto, LD. “Left Ventricular Noncompaction.” Orphanet Encyclopedia, Sept 2004. Chrissoheris MP, Ali R, Vivas Y, et al. “Isolated noncompaction of the ventricular myocardium: contemporary diagnosis and management.” Clin Cardiol. 2007 Apr;30(4):156-60. Freedom RM, Yoo SJ, Perrin D, et al. “The morphological spectrum of ventricular noncompaction.” Cardiol Young. 2005 Aug;15(4):345-64. Howedemakers, Y, et al. “Cardiac b-myosin heavy chain defects in two families with noncompaction cardiomyopathy: linking non-compaction to hypertrophic, restrictive, and dilated cardiomyopathies.” Eur Heart Journal 2007; 28: 2732-2737. Jenni R, Oeschslin, EN, Van der Loo B. “Isolated ventricular non-compaction of the myocardium in adults.” Heart 2007; 93: 11-15. Moreira FC, Miglioransa MH, Mautone MP, et al. “Noncompaction of the left ventricle: a new cardiomyopathy is presented to the clinician.” Sao Paulo Med J. 2006 Jan 5;124(1):31-5. Moric-Janiszewska, E, et al. “Genetic Heterogeneity of Left Ventricular Noncompaction Cardiomyopathy.” Clin Cardiology 2008; 31 (5):201-204. Pantazis, A, Elliot P. “Left Ventricular noncompaction.” Curr Opin Cardiol 2009; 24: 209-213.