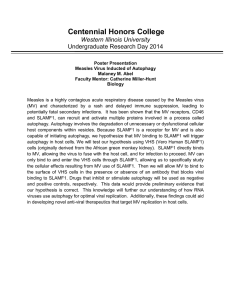
mTOR‑dependent abnormalities in autophagy characterize
advertisement

Acta Neuropathol (2013) 126:207–218 DOI 10.1007/s00401-013-1135-4 ORIGINAL PAPER mTOR‑dependent abnormalities in autophagy characterize human malformations of cortical development: evidence from focal cortical dysplasia and tuberous sclerosis Shireena A. Yasin · Abu M. Ali · Mathew Tata · Simon R. Picker · Glenn W. Anderson · Elizabeth Latimer‑Bowman · Sarah L. Nicholson · William Harkness · J. Helen Cross · Simon M. L. Paine · Thomas S. Jacques Received: 14 February 2013 / Revised: 23 May 2013 / Accepted: 24 May 2013 / Published online: 2 June 2013 © Springer-Verlag Berlin Heidelberg 2013 Abstract Focal cortical dysplasia (FCD) is a localized malformation of cortical development and is the commonest cause of severe childhood epilepsy in surgical practice. Children with FCD are severely disabled by their epilepsy, presenting with frequent seizures early in life. The commonest form of FCD in children is characterized by the presence of an abnormal population of cells, known as balloon cells. Similar pathological changes are seen in the cortical malformations that characterize patients with tuberous sclerosis complex (TSC). However, the cellular and molecular mechanisms that underlie the malformations of FCD and TSC are not well understood. We provide evidence for a defect in autophagy in FCD and TSC. We have found that balloon cells contain vacuoles that include components of the autophagy pathway. Specifically, we show that balloon cells contain prominent lysosomes by electron microscopy, immunohistochemistry for LAMP1 and LAMP2, Electronic supplementary material The online version of this article (doi:10.1007/s00401-013-1135-4) contains supplementary material, which is available to authorized users. S. A. Yasin · A. M. Ali · M. Tata · S. R. Picker · S. M. L. Paine · T. S. Jacques (*) Neural Development Unit, Birth Defects Research Centre, UCL Institute of Child Health, 30 Guilford Street, London WC1N 1EH, UK e-mail: t.jacques@ucl.ac.uk S. A. Yasin · S. R. Picker · G. W. Anderson · E. Latimer‑Bowman · S. L. Nicholson · S. M. L. Paine · T. S. Jacques Department of Histopathology, Great Ormond Street Hospital for Children NHS Foundation Trust, Great Ormond Street, London WC1N 3JH, UK S. R. Picker MRC National Institute for Medical Research, The Ridgeway, Mill Hill, London NW7 1AA, UK LysoTracker labelling and enzyme histochemistry for acid phosphatase. Furthermore, we found that balloon cells contain components of the ATG pathway and that there is cytoplasmic accumulation of the regulator of autophagy, DOR. Most importantly we found that there is abnormal accumulation of the autophagy cargo protein, p62. We show that this defect in autophagy can be, in part, reversed in vitro by inhibition of the mammalian target of rapamycin (mTOR) suggesting that abnormal activation of mTOR may contribute directly to a defect in autophagy in FCD and TSC. Keywords Autophagy · Epilepsy · Balloon cells · Focal cortical dysplasia · Tuberous sclerosis Introduction Epilepsy is the commonest severe neurological disease of children [18, 22]. Some children are severely disabled by their epilepsy, presenting with frequent seizures early in life. W. Harkness · J. H. Cross Neurosciences Unit, UCL Institute of Child Health, 30 Guilford Street, London WC1N 1EH, UK W. Harkness Department of Neurosurgery, Great Ormond Street Hospital for Children NHS Foundation Trust, Great Ormond Street, London WC1N 3JH, UK J. H. Cross Department of Neurology, Great Ormond Street Hospital for Children NHS Foundation Trust, Great Ormond Street, London WC1N 3JH, UK 13 208 In this group of children, structural abnormalities of the brain are frequent [5] and focal cortical dysplasia (FCD) is the most common [7]. FCD is a localized malformation of the cerebral cortex [7]. Children with FCD develop frequent seizures, for which treatment with standard anti-epileptic drugs in isolation or combination is usually ineffective, and they often require surgery. The cause of FCD is unknown. Therefore, there is a significant clinical need to understand the biology underlying this disease. Not only is FCD an important clinical problem, but also a disease characterized by fundamental, but poorly understood, abnormalities of human cortical development including regulation of cell size [7]. A frequent pathological feature of FCD is the presence of a population of cells with enlarged ballooned cytoplasm, known as balloon cells (BC) [7]. A similar cell type is seen in the cortex of patients with tuberous sclerosis complex (TSC) [12, 36]. FCD with BCs (FCD type IIb) is one of the commonest forms of FCD in children. Importantly, several studies have suggested that BCs are related to neural precursors or stem cells [10, 23, 37, 39, 40]. This suggests that an understanding of BCs will indicate how FCD arises. For example, one possibility is that BCs are abnormal stem cells that contribute directly to the disease. Alternatively, they may be derived from abnormal stem cells and will provide an insight into the primary abnormality affecting those stem cells [39]. Despite its clinical importance, the signalling pathways that underlie the development of FCD or BCs are unknown. The best described candidate mechanism in FCD is activation of the serine/threonine kinase, mammalian target of rapamycin (mTOR) [11]. Several lines of evidence indicate a role for mTOR in FCD. First, there is increased phosphorylation of downstream targets of mTOR in FCD and TSC when compared to control brain tissue [3, 24, 31, 32, 39]. Second, in TSC patients, mutations are found in the TSC1 and TSC2 genes that encode for hamartin and tuberin, inhibitors of mTOR [19]. Furthermore, in some patients with sporadic FCD, there are allelic variants in TSC1 that change the cellular localization of hamartin and its interaction with tuberin [4, 25]. Indeed, some studies have found reduced expression of tuberin or hamartin in FCD [14] or TSC [14, 32, 33]. Finally recent data raises the possibility that mTOR may be activated in FCD by congenital infection by human papilloma virus (HPV) [8]. However, the specific contribution of mTOR to the pathogenesis of FCD is unclear. The published studies have been descriptive reports of mTOR activity and a functional role for mTOR activity has not been proven. In addition, several of the studies have suggested differences in the activation of downstream targets between sporadic FCD and TSC [3, 31, 35, 39]. There is a suggestion in one report that mTOR activation is a feature of TSC but not FCD [3]. Given these potential differences between FCD and TSC, it is possible that a number of mechanisms may act 13 Acta Neuropathol (2013) 126:207–218 on a common final cellular process that is responsible for the pathogenesis of disease. However, the downstream consequences of mTOR activation in FCD and TSC are poorly understood. To elucidate these processes, we have focused on autophagy. Autophagy is a process for destroying organelles and proteins through the lysosomal system [13]. mTOR signalling has an important role in regulating autophagy [15, 16, 20, 21, 41]. We have found previously that BCs contain abundant mitochondria, intermediate filament proteins and vesicles [39]. We hypothesized that these observations were in keeping with an abnormality of autophagy; for example by reducing mitochondrial degradation (mitophagy) and the accumulation of vesicle components of the autophagy pathway. This would be supported by recent studies suggesting a defect in autophagy in TSC [29, 30]. In this study, we demonstrate that there is an abnormality in autophagy in BCs and that activation of mTOR is, at least in part, responsible for this defect. Materials and methods Tissue samples Tissue was obtained from the archives of the department of histopathology at Great Ormond Street Hospital for Children NHS Foundation Trust from patients who had been treated at the supra-regional epilepsy service as described previously [39]. All samples were from surgical cases. All cases were reviewed by a senior paediatric neuropathologist (TJ) and classified according to the ILAE classification of FCD [7]. Clinical details of the samples are included in Supplementary Table 1. Control samples were from the temporal neocortex of children undergoing temporal lobectomy for hippocampal pathology. Controls were included if the neocortex was normally formed but were excluded if there was tumour, encephalitis or cortical dysplasia (including FCD type III). Immunohistochemistry Paraffin-embedded sections were cut at 4–7 μm, dewaxed in xylene (10 min), rehydrated through a graded alcohol series, blocked in hydrogen peroxide (10 % hydrogen peroxide in PBS) and then rinsed in dH20. Antigen retrieval was performed by pressure-cooking sections in EDTA-Citrate buffer pH 6.2 for the following antigens: DOR, p62, ATG5, LC3/ATG8, ATG12 and Beclin-1/ATG6. Sections were then washed in PBS (2 × 3 min) and once in 0.1 % Tween/PBS (3 min). Primary antibodies [p62 (1:1000, BD Biosciences), DOR (1:400 a gift from Prof. Zorzano, Barcelona [2]) ATG5 (1:125, Abgent), 209 Acta Neuropathol (2013) 126:207–218 LC3/ATG8 (1:125, Abgent), ATG12 (1:100, Abgent) and Beclin-1 (1:100, Abgent)] were applied to sections, which were then incubated at room temperature for 60 min in a humid slide chamber. Sections were rinsed with dH2O, washed in PBS (2 × 3 min) and once in 0.1 % Tween/PBS (3 min). After washing with PBS, biotinylated secondary antibodies were subsequently applied to sections and incubated for 30 min at room temperature in a humid slide chamber. Sections were rinsed with dH2O, washed in PBS (2 × 3 min) and once in 0.1 % Tween/PBS (3 min). Detection was performed with Vectorstain ABC kit (Vector) and 0.5 % 3,3′ diaminobenzidine tetrahydrochloride (DAB) for 5 min. Sections were then rinsed with dH2O. Sections were counterstained with Mayer’s Haematoxylin for 1 min then washed in warm tap water for 1 min. Sections were dehydrated through a graded alcohol series (1 min in 70 % alcohol, 2 min in absolute alcohol and 2 min in xylene) before being mounted with DPX (BDH). The ATG antibodies were also stained on an intelliPATH FLX staining system (A. Menarini Diagnostics), which produced similar results. Additional immunohistochemistry was performed on a DAKO Bond-Max automated stainer: LAMP1 (Abcam) 1:200 HIER 10 ER2 Bond-Max protocol F, LAMP2 (Abcam) 1:100 HIER 20 ER2 Bond-Max protocol F, Ubiquitin (Dako) 1:1200 HIER 20 ER1 Bond-Max protocol F and p62 (BD Biosciences) 1:1000 HIER 20 ER1 Bond-Max protocol F. The numbers of cases stained are indicated in the “Results” section. For each antibody, similar staining was seen in all stained cases of a given diagnosis unless specified in the text. For immunofluorescence, sections were dewaxed and washed in 0.1 % Tween/PBS (2 × 3 min). Sections were then blocked using 10 % heat-inactivated sheep serum/PBS for at least 10 min and rinsed with dH2O. Sections were again washed in 0.1 % Tween/PBS (2 × 3 min) before being incubated with primary antibody (anti-DOR 1:400 in 0.1 % BSA/PBS) at 4 °C overnight in a sealed, humid slide chamber. Sections were rinsed with dH2O, washed in 0.1 % Tween/PBS (2 × 3 min) and then incubated with Alexa Fluor 488 secondary antibody (1:240, Molecular Probes) in 1 % BSA/PBS in the dark for 90 min at room temperature. Slides were washed in PBS (3 × 3 min) and mounted in Vectashield aqueous mounting medium containing 4′, 6-diamidino-2-phenylindole/DAPI (Vector). 10 μm cryostat sections were allowed to thaw and 0.5 ml of incubation medium was applied to each slide. The slides were incubated at 37 °C for 2 h. The sections were washed, counterstained with Carazzi’s haematoxylin and dehydrated through a graded alcohol series before being mounted with DPX. Acid phosphatase staining Thawed BCs were allowed to settle overnight, the following day they were plated onto 5 μg/ml PDL coated 1 N HCL treated 13 mm glass coverslips and allowed to adhere for 2.5 h. The cells were then treated with 100 or 500 nM rapamycin diluted in dimethyl sulphoxide (DMSO) for either 6 or 24 h prior to being fixed and stained. Control BCs were treated with vehicle alone (DMSO) diluted in media for the same lengths of time prior to fixation in 4 % PFA. Rapamycin was diluted in sterile DMSO to a final To make the incubation solution, 5 mg Naphthol AS-BI phosphate was dissolved in 2–3 drops of dimethylformaldehyde, 2.5 ml of 0.1 M Acetate buffer, 6 ml of distilled water and 0.4 ml of hexazotized pararosaniline (HPR). The HPR solution was prepared by mixing equal volumes of 40 mg of basic fuchsin dissolved in 1 ml 2 M HCl with 40 mg of sodium nitrate dissolved in 1 ml distilled water. Electron microscopy All samples were fixed in 2.5 % glutaraldehyde in 0.1 M cacodylate buffer followed by secondary fixation in 1.0 % osmium tetroxide. Tissues were dehydrated in graded ethanol, transferred to propylene oxide and then infiltrated and embedded in Agar 100 epoxy resin. Polymerization was at 60 °C for 48 h. 90 nm ultrathin sections were then cut using a Diatome diamond knife on a Leica Ultracut UCT ultramicrotome. Sections were picked up on copper grids and stained with alcoholic uranyl acetate and Reynold’s lead citrate. The samples were examined in a JEOL transmission electron microscope. Cell culture immunocytochemistry BCs were cultured as previously described [39]. Dissociated cells from the TS tuber were plated onto 5 μg/ml PDL coated 1 N HCL treated 13 mm glass coverslips 1 day after dissociation and allowed to adhere for 2.5 h before fixation in 4 % PFA. Frozen cells from the FCDIIb case were allowed to settle in culture media overnight at 37 °C following thawing and were then plated onto PDL-coated coverslips and fixed as above. Some BCs could still be seen in culture 21 days after dissociation of the FCDIIb tissue. These cells were plated onto coverslips, allowed to adhere and fixed as above. Fixed cells were stained as described in [39] with antibodies to Beclin-1/ATG6 (1:50, Abgent), LC3/ATG8 (1:400, Abgent), ATG12 (1:50, Abgent), DOR (1:500 a gift from Prof. Zorzano, Barcelona), LAMP1 (1:200, Abcam), LAMP2 (1:100, Abcam), p62 (1:50, BD Biosciences), phospho-S6 (Ser235/236 1:100, Cell Signalling) and phospho-4EBP1 (Thr37/46 1:100, Cell Signalling). Cell treatments 13 210 concentration of 100 μM. For final concentrations this stock was then diluted to 1 μl/ml media for a final concentration of 100 nM and 5 μl/ml media for a final concentration of 500 nM. Control conditions were 5 μl DMSO only/ ml media (0.5 % DMSO). Acta Neuropathol (2013) 126:207–218 Results Lysosomes accumulate in balloon cells The lysosomes of cultured BCs (n = 3 cultures) were labelled by incubating them in LysoTracker dye (1 μM in media, Molecular Probes) for 5–10 min at 37 °C. Cells were washed with media and re-suspended in fresh media and the fluorescence observed under a time-lapse microscope using Volocity software (Improvision, UK). In order to explore the role of autophagy in FCD, we tested the hypothesis that BCs accumulate cellular structures normally consumed during autophagy. If autophagy were defective in BCs, one would anticipate an accumulation of these components. First, we explored the lysosomal component of BCs. Histochemical staining for the lysosomal enzyme, acid phosphatase, showed strong positive reactivity within BCs (n = 6 cases, FCDIIb) (Fig. 1a). There was weaker staining of some neurons and glia in FCDIIb. Staining of normally formed cortex from temporal lobectomy samples (n = 5 cases) showed relatively weak staining of neurons and glia (Fig. 1d). This lysosomal accumulation was confirmed by immunohistochemistry for the two major lysosomal glycoproteins, LAMP1 and LAMP2. BCs in FCDIIb and TSC showed prominent and consistent expression of LAMP1 and LAMP2 (FCDIIb n = 3 cases, TSC n = 4 cases) (Fig. 1b, c). Some BCs showed paranuclear or central staining for LAMP. In contrast, there was notably less expression of LAMP1 in normally formed cortex and white matter (n = 5 cases) than in cortical dysplasia (Fig. 1e). LAMP2 showed variable labelling of glia and neurons in normally formed cortex (Fig. 1f) and in cortical dysplasia (Fig. 1c). Fig. 1 Balloon cells accumulate lysosomes. Acid phosphatase staining of balloon cells in FCDIIb (a) compared with normally formed cortex (d). LAMP1 staining of balloon cells in FCDIIb (b) com- pared with normally formed cortex (e). LAMP2 staining of balloon cells in FCDIIb (c) compared with normally formed cortex (f). Scale bar = 50 μm Confocal microscopy Confocal images of immunostained BCs were acquired with a Zeiss LSM710 microscope (Zen2009, Zeiss) using oil immersion (63×, N.A. 1.4) and water immersion (25×, N.A 0.8). Z-projections of confocal stacks were created in ImageJ. Images of single BCs in immunopanels show a Z-projection of all channels around the nucleus/ nuclei of cells. For the quantitative analysis fluorescence was measured per cell using an entire tile scan (10 × 10 grids at 20×) over 3 coverslips from 2 temporally separate experiments. LysoTracker labelling of cultured BC 13 211 Acta Neuropathol (2013) 126:207–218 Fig. 2 The prominent lysosomal component of balloon cells is maintained in culture. Confocal projection of balloon cells at low power (a, c) and at high power (b, d) stained with antibodies against LAMP1 (a, b) and LAMP2 (c, d). Scale bars in a, c = 25 μm, scale bars in b, d = 10 μm BCs isolated in vitro also showed extensive immunoreactivity for LAMP1 and LAMP2. LAMP1 and LAMP2 were strongly expressed in a punctate pattern, which in some cases was found within the centre of the cells (n = 3, 1 FCDIIb after 1DIV, 1 FCDIIb 21DIV and 1TSC after 1 DIV) (Fig. 2). Furthermore, live cell staining with the lysosomal stain, LysoTracker showed frequent mobile punctate structures with a central accumulation (n = 3) (Supplementary Video 1). These data suggest that there is a significant accumulation of lysosomes in BCs. To confirm this, we undertook electron microscopy on BCs in vivo (n = 3 FCDIIb, n = 2 TSC). BCs in vivo could be identified by their enlarged cytoplasm, eccentric nuclei with prominent nucleoli and lack of features of neuronal or astrocytic differentiation. Similar to our previous in vitro findings, BCs in vivo contained prominent mitochondria, intermediate filaments and vesicles, many of which were lysosomes (Fig. 3). Taken together, these data support the hypothesis that BCs showed a significant accumulation of lysosomes. Components of the autophagy cascade accumulate in balloon cells Next, we tested the hypothesis that components of the mechanisms that mediate autophagy also accumulate in BCs. A protein cascade that directs the formation of autophagosomes initiates autophagy. We examined the expression of four components of this pathway, ATG5, LC3/ATG8, ATG12 and Beclin-1/ATG6 in FCD with (IIb, n = 5) and without BCs (IIa, n = 4), TSC (n = 5) and normally formed cortex (n = 5). These components were chosen, not only because they are critical parts of the machinery of autophagy, but also because previous studies had indicated there was low or absent immunoreactivity in normal cortex and their accumulation had been taken to indicate an abnormality of autophagy [26]. All four proteins showed prominent accumulation in a proportion of BCs from FCDIIb or TSC and this was readily distinguished from the comparatively low levels of expression seen in normally formed cortex (Fig. 4) or in FCD lacking BCs (FCDIIa). In these control cases, there 13 212 Acta Neuropathol (2013) 126:207–218 Fig. 3 Ultrastructural examination by electron microscopy shows that the balloon cells contain abundant mitochondria, intermediate filament and vesicles that included prominent dense cored lysosomes (arrows). The images show electron micrographs taken at low power (showing the entire balloon cell) (a, b) and at high power (showing the organelles) (c, d). Cells from both TSC (a, c) and FCDIIb (b, d) are shown. Scale bars in a, b = 2 μm and in c, d = 500 nm Fig. 4 Balloon cells accumulate components of the autophagy pathway. a–d FCDIIb, e–h TS and i–l control tissue (normally formed cortex from temporal lobectomies). Balloon cells in FCDIIb and TS tissue sections express the autophagy markers ATG5 (a, e), BECN- 13 1/ATG6 (b, f), LC3/ATG8 (c, g) and ATG12 (d, h). Normally formed cortex and white matter showed low levels or negative expression of these proteins (i–l). Scale bar = 100 μm 213 Acta Neuropathol (2013) 126:207–218 was some expression of ATG proteins (mostly of ATG5 and ATG8) that was predominantly in neurons. This was quite distinct from the strong reactivity of BCs. Immunoreactivity for Beclin-1/ATG6, ATG12 and LC3/ATG8 was confirmed within cultured BCs (Fig. 5). Notably, the strongest reactivity was demonstrated for ATG12. The staining of the ATG proteins was punctate and predominantly distributed throughout the cytoplasm, raising the possibility of autophagosome formation. Balloon cells show cytoplasmic expression of the diabetes and obesity‑related gene (DOR) We examined the localization of the product of the diabetes and obesity-related gene (DOR) in BCs. DOR is a nuclear cofactor that is involved in the initiation of autophagy. Stimulation of autophagy is thought to cause DOR to shuttle from the nucleus to the cytoplasm where it binds to autophagosomes and facilitates the initiation of autophagy [27]. We hypothesized that the localization of DOR may be interpreted as an indication of the state of autophagy in BCs. Staining of FCDIIb cases (n = 4) with an antibody against DOR showed prominent cytoplasmic expression and variable nuclear expression in dysplastic cells that included BCs and dysmorphic neurons (Fig. 6c). The principal normal cell type expressing DOR were small glial cells, which in contrast, predominantly showed nuclear staining (Fig. 6a, b). Morphologically normal neurons showed a more variable, often weak, pattern of staining. Confocal microscopy confirmed that the predominant pattern of DOR expression in BCs in vivo and in vitro was as cytoplasmic puncta (Fig. 6d, e). These observations suggest that there is an accumulation of autophagosomes in BCs. Balloon cells accumulate p62 To test the hypothesis that autophagy is inhibited in BCs, we examined the expression of the adaptor protein, p62. p62 marks proteins for degradation via autophagy and is itself destroyed in the process. The turnover of p62 is rapid in normal cells (e.g. pulse chase experiments in culture suggest a half life of 6 h with complete loss in 24 h [6]) and expression is not detectable in the normal brain by immunohistochemistry on paraffin-embedded tissue. Furthermore, p62 levels rise following inhibition of autophagy [17]. Therefore, we hypothesized that BCs would show an accumulation of p62 compared to normally formed brain. Immunohistochemistry for p62 revealed strong staining of BCs in FCDIIb (n = 5) and TSC (n = 5), indicating an accumulation of p62. Staining was present in the cytoplasm and the nucleus of cells and occasional surrounding processes (Fig. 6g, h). Weaker staining was seen in occasional dysmorphic neurons but this was not a consistent finding. The dysplastic cortex of FCDIIa showed very little p62 expression, with most cases either entirely negative or with weak neuronal staining (n = 4). Normally formed cortex was negative for p62 (n = 4) (Fig. 6f) (the association between p62 reactivity in BC-cases vs. normally formed cortex is significant, p = 0.001 Fisher’s exact test). These data show that p62 accumulation occurs in BCs supporting the view that autophagy is defective in these cells. Staining of balloon cells in culture showed prominent punctate staining for p62 in the cytoplasm and nucleus. To exclude the alternative possibility that p62 accumulation reflects a defect in the ubiquitin–proteasome system, we undertook immunohistochemistry for ubiquitin. While occasional cells showed weak staining similar to the controls, there was no reproducible specific staining of BCs (n = 5) (data not shown). mTOR activity is required for defective autophagy in balloon cells A major regulator of autophagy is the mTOR pathway and a number of reports have suggested that mTOR activation characterizes BCs in FCD [16, 20, 21, 35, 39, 41]. We wished to determine whether this activation of mTOR in BCs contributes to the defect in autophagy or if other mechanisms are responsible. First, to test the hypothesis that mTOR is activated in BCs from FCDIIb, we measured immunoreactivity for phosphorylation of S6, a downstream target of mTOR, in BCs after treatment with the mTOR inhibitor, rapamycin. Six hours after treatment with rapamycin, there was no detectable staining for phosphorylated S6 in the cultured BCs confirming that phosphorylation of S6 in BCs is driven by mTOR (p < 0.001 ANOVA with Dunnet’s post hoc testing) (Fig. 7, Supplementary Figure 1 and Figure 8). In order to determine if the defect in autophagy in BCs is dependent on mTOR, we stained BCs for p62 with or without treatment with rapamycin. In the absence of rapamycin, p62 was expressed in strong punctate structures scattered throughout the cell (Fig. 6i, j). The intensity of staining, density of puncta and distribution of p62 varied considerably between cells. p62 aggregates were seen throughout the cytoplasm but in addition, in shortterm cultures we often found large aggregates of p62 in the nucleus. Rapamycin treatment lead to a significant decrease in p62 immunoreactivity within 24 h indicating that the defect in autophagy is at least in part dependent on mTOR activity (p < 0.001 ANOVA with Dunnet’s post hoc testing) (Fig. 7, Supplementary Figure 1 and Fig. 8). 13 214 Fig. 5 Cultured balloon cells expressed markers of the autophagy cascade. Confocal images a–i = FCDIIb and j–r = TS. Cells expressed BECN-1/ATG6 (a–c and j–l), LC3/ATG8 (d–f and m–o) and ATG12 (g–i and p–r). These markers were expressed in a punctate pattern at high density in the cytoplasm of cells from FCDIIb and TS. Scale bar = 10 μm 13 Acta Neuropathol (2013) 126:207–218 Acta Neuropathol (2013) 126:207–218 Fig. 6 Balloon cells show cytoplasmic accumulation of DOR (a–e) and nuclear and cytoplasmic accumulation of p62 (f–j). Immunohistochemistry for DOR in tissue sections shows frequent strong nuclear staining in small glial cells (arrows), variable staining in neurons (arrow heads) (a and b adjacent non-dysplastic regions of an FCDIIb case) and strong cytoplasmic staining in balloon cells (c). Confocal microscopy of tissue sections shows that this staining has a punctate 215 cytoplasmic pattern (d). Similar punctate cytoplasmic staining was seen in balloon cells in culture (e). p62 was strongly expressed in the cytoplasm and nucleus of balloon cells from FCDIIb (g) and TSC (h), but was not expressed in control cortex (f). There are aggregates of p62, in the nucleus and cytoplasm of cultured balloon cells. (i FCDIIb) and (j TSC). Scale bars a–c and f–h = 50 μm; d, e, i, j = 10 μm Fig. 7 Balloon cells show down-regulation of pS6 and p62 in response to rapamycin. Immunofluorescence for pS6 (a, c) and p62 (b, d) in control media (upper row) and rapamycin (500 nM) (lower row). The images are counterstained with DAPI. See Fig. 8 for quantification and supplementary figure 1 for a high power image. Scale bar = 100 μm 13 216 Fig. 8 Balloon cells show down-regulation of pS6 and p62 in response to rapamycin. Fluorescence intensity of pS6 (a) and p62 (b), in balloon cells grown in control conditions (DMSO, blue bars) and in 2 concentrations of rapamycin (100 nM green bars and 500 nM rapamycin brown bars) at 6 and 24 h post-treatment. pS6 is almost completely switched off in both concentrations of rapamycin at both time points (p < 0.001 ANOVA with Dunnett’s post hoc testing). p62 shows significant down-regulation by 24 h at both concentrations (p < 0.001 ANOVA with Dunnett’s post hoc testing). The images shown are the average fluorescence signal per cell and have been normalized to the control sample Discussion We have provided evidence that FCD with BCs shows an abnormality in autophagy. We have also confirmed for the first time functionally that mTOR is over-activated in BCs and that the abnormality in autophagy is at least in part dependent on this mTOR activity. This raises the possibility that FCD arises due to a defect in autophagy during 13 Acta Neuropathol (2013) 126:207–218 development that is at least in part driven by dysregulation of the mTOR pathway. Several lines of evidence support the view that autophagy is dysregulated in FCD. The most direct evidence is that the protein, p62 accumulates in BCs. p62 is normally turned over rapidly by autophagy and inhibition of autophagy (e.g. by knocking out components of the autophagy pathway) leads to p62 accumulation [17]. p62 is a ubiquitin-binding protein and a defect in the ubiquitin– proteasome system may also lead to accumulation of p62. However, we do not favour this explanation in view of the lack of accumulation of ubiquitinated proteins in FCD. We cannot exclude entirely the possibility that p62 has additional roles acting through other mechanisms in FCD or TSC or that there are more subtle effects on ubiquitinated proteins that we have not been able to detect. A number of additional observations also support the view that autophagy is abnormal in these cells. First, we have shown that lysosomes, an essential precursor organelle for autophagy, are a prominent cytoplasmic component of BCs. This would be in keeping with an accumulation of the precursor organelle following a block in autophagy. Similarly, there is a prominent punctate expression of autophagy cascade proteins in the cytoplasm of BCs. This expression was mirrored by the cytoplasmic expression of DOR. Several studies have shown that DOR shuttles between the cytoplasm and the nucleus and that one of its cytoplasmic functions is to regulate autophagosome formation [27, 28]. It is not possible to compare the expression of these components directly with a ‘normal comparison’ cell as we do not know the cell of origin for BCs but the accumulation of these components, compared to normally formed cortex, supports the hypothesis that autophagy is inhibited in FCD. However, the punctate cytoplasmic staining suggests that autophagy has been initiated as autophagosomes are accumulating. Our data supports the hypothesis that activation of mTOR is a key pathway in the pathogenesis of FCD. Several previous publications have implicated over-activation of mTOR in FCD. Previously, this has been supported by the histological and biological similarity of FCD with BCs to the cortical pathology seen in TSC, which is due to mutations in the genes encoding for the inhibitors of mTOR, hamartin (TSC1) and tuberin (TSC2) [36]. Furthermore, polymorphisms in the TSC1 gene have been described in FCD [4]. Finally, there is phosphorylation of targets of mTOR in BCs in FCD [3, 24, 31, 34, 39]. However, the pattern of target phosphorylation differs in some studies between FCD and TSC [3, 31, 34, 39]. For example activation of pS6 kinase and pS6, which are not entirely specific to mTOR, are common to both diseases but activation of the more specific target of mTOR, 4E-BP1 is either variable or absent in FCD depending on the study [3, 39]. This has led some authors Acta Neuropathol (2013) 126:207–218 to suggest that TSC but not FCD is characterized by mTOR activation [3]. Therefore, our cell culture data is important as we have found that phosphorylation of S6 is rapidly ablated by the addition of the specific mTOR inhibitor, rapamycin. This strongly supports the view that S6 is phosphorylated in FCD by activation of mTOR and supports the view that mTOR activation characterizes FCD. Interestingly, as with the in vivo studies, we have not found that phosphorylation of 4E-BP1 is a reliable marker of BCs (in vitro) (data not shown). The reason for the difference between S6 and 4E-BP1 is not clear but data in other cell types suggest that phosphorylation by mTOR of the pS6 kinase/pS6 system can be unlinked to phosphorylation of 4E-BP1 [9]. As several mechanisms, including mTOR, regulate autophagy, it was important to determine if the abnormalities in autophagy in FCD are dependent on the activation of mTOR seen in FCD or if other pathways are responsible. We found that a significant reduction in p62 accumulation was seen following mTOR inhibition. This result indicates that reversing the activation of mTOR, at least in part, can reverse the defect in autophagy. This raises the possibility that over-activation of mTOR in the developing cortex leads to defective autophagy and may be an important mechanism in the pathogenesis of FCD. We cannot exclude the possibility that other pathways contribute to the inhibition of autophagy in BCs, as we were unable to eliminate p62 accumulation entirely in these experiments. Taken together, these data raise two possible mechanisms linking autophagy and the pathogenesis of FCD. In the first, over-activation of mTOR during cortical development leads to a defect in autophagy that directly impairs normal development. The role of autophagy in normal cortical development is unclear but several studies have suggested that autophagy regulates normal progenitor cell function [1, 38]. The second possibility is that the defect in autophagy and mTOR is responsible for specific aspects of the phenotype, for example, abnormalities in this pathway would easily explain the abnormalities of cell size that characterize several forms of FCD and that are not restricted to BCs. Acknowledgments TSJ was in receipt of funding from the Great Ormond Street Hospital Children’s Charity and holds a HEFCE Clinical Senior Lecturer Award. This report is independent research supported by the National Institute for Health Research Great Ormond Street Hospital Biomedical Research Centre. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health. We are grateful to Prof. Zorzano, Institute of Research in Biomedicine, Barcelona for the DOR antibody. References 1. Baek S-H, Kim E-K, Goudreau JL, Lookingland KJ, Kim SW, Yu S-W (2009) Insulin withdrawal-induced cell death in adult 217 hippocampal neural stem cells as a model of autophagic cell death. Autophagy 5(2):277–279 2. Baumgartner BG, Orpinell M, Duran J et al (2007) Identification of a novel modulator of thyroid hormone receptor-mediated action. PLoS ONE 2(11):e1183 3. Baybis M, Yu J, Lee A, Golden JA, Weiner H, Mckhann G, Aronica E, Crino PB (2004) mTOR cascade activation distinguishes tubers from focal cortical dysplasia. Ann Neurol 56(4):478–487 4. Becker AJ, Urbach H, Scheffler B et al (2002) Focal cortical dysplasia of Taylor’s balloon cell type: mutational analysis of the TSC1 gene indicates a pathogenic relationship to tuberous sclerosis. Ann Neurol 52(1):29–37 5.Berg AT, Mathern GW, Bronen RA, Fulbright RK, DiMario F, Testa FM, Levy SR (2009) Frequency, prognosis and surgical treatment of structural abnormalities seen with magnetic resonance imaging in childhood epilepsy. Brain 132(Pt 10):2785–2797 6.Bjorkoy G (2005) p62/SQSTM1 forms protein aggregates degraded by autophagy and has a protective effect on huntingtininduced cell death. J Cell Biol 171(4):603–614 7. Blümcke I, Thom M, Aronica E et al (2011) The clinicopathologic spectrum of focal cortical dysplasias: a consensus classification proposed by an ad hoc Task Force of the ILAE Diagnostic Methods Commission. Epilepsia 52(1):158–174 8. Chen J, Tsai V, Parker WE, Aronica E, Baybis M, Crino PB (2012) Detection of human papillomavirus in human focal cortical dysplasia type IIB. Ann Neurol 72(6):881–892 9. Choo AY, Yoon S-O, Kim SG, Roux PP, Blenis J (2008) Rapamycin differentially inhibits S6Ks and 4E-BP1 to mediate celltype-specific repression of mRNA translation. Proc Natl Acad Sci USA 105(45):17414–17419 10.Crino PB, Trojanowski JQ, Eberwine J (1997) Internexin, MAP1B, and nestin in cortical dysplasia as markers of developmental maturity. Acta Neuropathol 93(6):619–627 11.Crino PB (2011) mTOR: a pathogenic signaling pathway in developmental brain malformations. Trends Mol Med 17(12):734–742 12.Crino PB (2013) Evolving neurobiology of tuberous sclerosis complex. Acta Neuropathol 125(3):317–332 13. Glick D, Barth S, Macleod KF (2010) Autophagy: cellular and molecular mechanisms. J Pathol 221(1):3–12 14.Grajkowska W, Kotulska K, Matyja E, Larysz-Brysz M, Mandera M, Roszkowski M, Domańska-Pakieła D, Lewik-Kowalik J, Jozwiak S (2008) Expression of tuberin and hamartin in tuberous sclerosis complex-associated and sporadic cortical dysplasia of Taylor’s balloon cell type. Folia Neuropathol 46(1):43–48 15.Hall MN (2008) mTOR-what does it do? TPS 40(10 Suppl):S5–S8 16. Hosokawa N, Hara T, Kaizuka T et al (2009) Nutrient-dependent mTORC1 association with the ULK1-Atg13-FIP200 complex required for autophagy. Mol Biol Cell 20(7):1981–1991 17. Ichimura Y, Komatsu M (2010) Selective degradation of p62 by autophagy. Semin Immunopathol 32(4):431–436 18. Joint Epilepsy Council (2011) Epilepsy prevalence, incidence and other statistics. Available via http://www.jointepilepsycouncil. org.uk/resources/publications.html 19. Jozwiak J, Jozwiak S, Wlodarski P (2008) Possible mechanisms of disease development in tuberous sclerosis. Lancet Oncol 9(1):73–79 20. Jung CH, Jun CB, Ro S-H, Kim Y-M, Otto NM, Cao J, Kundu M, Kim D-H (2009) ULK-Atg13-FIP200 complexes mediate mTOR signaling to the autophagy machinery. Mol Biol Cell 20(7):1992–2003 21. Kim J, Kundu M, Viollet B, Guan K-L (2011) AMPK and mTOR regulate autophagy through direct phosphorylation of Ulk1. Nat Cell Biol 13(2):132–141 13 218 22.Kurtz Z, Tookey P, Ross E (1998) Epilepsy in young people: 23 year follow up of the British national child development study. BMJ 316(7128):339–342 23. Lamparello P, Baybis M, Pollard J, Hol EM, Eisenstat DD, Aronica E, Crino PB (2007) Developmental lineage of cell types in cortical dysplasia with balloon cells. Brain 130(Pt 9):2267–2276 24. Ljungberg MC, Bhattacharjee MB, Lu Y, Armstrong DL, Yoshor D, Swann JW, Sheldon M, D’arcangelo G (2006) Activation of mammalian target of rapamycin in cytomegalic neurons of human cortical dysplasia. Ann Neurol 60(4):420–429 25. Lugnier C, Majores M, Fassunke J, Pernhorst K, Niehusmann P, Simon M, Nellist M, Schoch S, Becker A (2009) Hamartin variants that are frequent in focal dysplasias and cortical tubers have reduced tuberin binding and aberrant subcellular distribution in vitro. J Neuropathol Exp Neurol 68(10):1136–1146 26. Ma J-F, Huang Y, Chen S-D, Halliday G (2010) Immunohistochemical evidence for macroautophagy in neurones and endothelial cells in Alzheimer’s disease. Neuropathol Appl Neurobiol 36(4):312–319 27. Mauvezin C, Orpinell M, Francis VA, Mansilla F, Duran J, Ribas V, Palacín M, Boya P, Teleman AA, Zorzano A (2010) The nuclear cofactor DOR regulates autophagy in mammalian and Drosophila cells. EMBO Rep 11(1):37–44 28. Mauvezin C, Sancho A, Ivanova S, Palacín M, Zorzano A (2012) DOR undergoes nucleo-cytoplasmic shuttling, which involves passage through the nucleolus. FEBS Lett 586(19):3179–3186 29. McMahon J, Huang X, Yang J, Komatsu M, Yue Z, Qian J, Zhu X, Huang Y (2012) Impaired autophagy in neurons after disinhibition of mammalian target of rapamycin and its contribution to epileptogenesis. J Neurosci 32(45):15704–15714 30.Miyahara H, Natsumeda M, Shiga A et al (2013) Suppressed expression of autophagosomal protein LC3 in cortical tubers of tuberous sclerosis complex. Brain Pathol 23(3):254–262 31.Miyata H, Chiang ACY, Vinters HV (2004) Insulin signaling pathways in cortical dysplasia and TSC-tubers: tissue microarray analysis. Ann Neurol 56(4):510–519 13 Acta Neuropathol (2013) 126:207–218 32. Mizuguchi M, Ikeda K, Takashima S (2000) Simultaneous loss of hamartin and tuberin from the cerebrum, kidney and heart with tuberous sclerosis. Acta Neuropathol 99(5):503–510 33.Mizuguchi M, Kato M, Yamanouchi H, Ikeda K, Takashima S (1996) Loss of tuberin from cerebral tissues with tuberous sclerosis and astrocytoma. Ann Neurol 40(6):941–944 34. Schick V, Majores M, Engels G, Hartmann W, Elger CE, Schramm J, Schoch S, Becker AJ (2007) Differential Pi3K-pathway activation in cortical tubers and focal cortical dysplasias with balloon cells. Brain Pathol 17(2):165–173 35. Schick V, Majores M, Koch A, Elger CE, Schramm J, Urbach H, Becker AJ (2007) Alterations of phosphatidylinositol 3-kinase pathway components in epilepsy-associated glioneuronal lesions. Epilepsia 48(Suppl 5):65–73 36. Sebire N, Malone M, Ashworth M, Jacques TS (2010) Diagnostic Pediatric Surgical Pathology. Elsevier, London 37.Urbach H, Scheffler B, Heinrichsmeier T, von Oertzen J, Kral T, Wellmer J, Schramm J, Wiestler OD, Blümcke I (2002) Focal cortical dysplasia of Taylor’s balloon cell type: a clinicopathological entity with characteristic neuroimaging and histopathological features, and favorable postsurgical outcome. Epilepsia 43(1):33–40 38. Vázquez P, Arroba AI, Cecconi F, de la Rosa EJ, Boya P, de Pablo F (2012) Atg5 and Ambra1 differentially modulate neurogenesis in neural stem cells. Autophagy 8((2):187–199 39.Yasin SA, Latak K, Becherini F et al (2010) Balloon cells in human cortical dysplasia and tuberous sclerosis: isolation of a pathological progenitor-like cell. Acta Neuropathol 120(1):85–96 40.Ying Z, Gonzalez-Martinez J, Tilelli C, Bingaman W, Najm I (2005) Expression of neural stem cell surface marker CD133 in balloon cells of human focal cortical dysplasia. Epilepsia 46(11):1716–1723 41.Yu L, Mcphee CK, Zheng L et al (2010) Termination of autophagy and reformation of lysosomes regulated by mTOR. Nature 465(7300):942–946