Document 13233729
advertisement

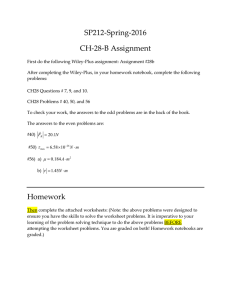
JACC: CARDIOVASCULAR INTERVENTIONS © 2009 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION PUBLISHED BY ELSEVIER INC. VOL. 2, NO. 8, 2009 ISSN 1936-8798/09/$36.00 DOI: 10.1016/j.jcin.2009.05.014 Magnetic Tagging Increases Delivery of Circulating Progenitors in Vascular Injury Panagiotis G. Kyrtatos, BMEDSCI,*†§ Pauliina Lehtolainen, PHD,* Manfred Junemann-Ramirez, MD,‡ Ana Garcia-Prieto, PHD,储 Anthony N. Price, PHD,* John F. Martin, MD,‡ David G. Gadian, DPHIL,† Quentin A. Pankhurst, PHD,§储 Mark F. Lythgoe, PHD*† London, United Kingdom Objectives We sought to magnetically tag endothelial progenitor cells (EPCs) with a clinical agent and target them to a site of arterial injury using a magnetic device positioned outside the body. Background Circulating EPCs are involved in physiological processes such as vascular re-endothelialization and post-ischemic neovascularization. However, the success of cell therapies depends on the ability to deliver the cells to the site of injury. Methods Human EPCs were labeled with iron oxide superparamagnetic nanoparticles. Cell viability and differentiation were tested using flow cytometry. Following finite element modeling computer simulations and flow testing in vitro, angioplasty was performed on rat common carotid arteries to denude the endothelium and EPCs were administered with and without the presence of an external magnetic device for 12 min. Results Computer simulations indicated successful external magnetic cell targeting from a vessel with flow rate similar to a rat common carotid artery; correspondingly there was a 6-fold increase in cell capture in an in vitro flow system. Targeting enhanced cell retention at the site of injury by 5-fold at 24 h after implantation in vivo. Conclusions Using an externally applied magnetic device, we have been able to enhance EPC localization at a site of common carotid artery injury. This technology could be more widely adapted to localize cells in other organs and may provide a useful tool for the systemic injection of cell therapies. (J Am Coll Cardiol Intv 2009;2:794 – 802) © 2009 by the American College of Cardiology Foundation From the *Centre for Advanced Biomedical Imaging, University College London (UCL) Department of Medicine and UCL Institute of Child Health, London, United Kingdom; †Radiology and Physics Unit, UCL Institute of Child Health, London, United Kingdom; ‡Centre for Cardiovascular Biology and Medicine, UCL Department of Medicine, London, United Kingdom; §Davy-Faraday Research Laboratories, The Royal Institution of Great Britain, London, United Kingdom; and 储London Centre for Nanotechnology, London, United Kingdom. Supported by the UCL Institute of Child Health (Child Health Research Appeal Trust), the British Heart Foundation, the Alexander S. Onassis Public Benefit Foundation, and the Biotechnology and Biological Sciences Research Council. Panagiotis G. Kyrtatos and Dr. Lehtolainen contributed equally to this manuscript. Manuscript received May 4, 2009, accepted May 20, 2009. Kyrtatos et al. Magnetic Tagging Increases Cell Delivery JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 2, NO. 8, 2009 AUGUST 2009:794 – 802 One of the current challenges in the biomedical sciences is the localization of stem cells to sites of interest for the repair of tissue damage. Cellular therapies are increasingly applied in clinical trials, and in recent years the use of hematopoietic progenitors as repairing modules in the compromised cardiovascular system has been the focus of considerable attention (1–3). In the context of ischemic heart disease, these efforts have led to modest success (4,5). However, delivery to specific targets within the body generally remains a difficult task, in part due to low uptake at the site of injury. As such, cell therapies would greatly benefit from methodologies aimed at targeting and monitoring cell trafficking. See page 803 Superparamagnetic iron oxide nanoparticles (SPIO) offer attractive possibilities in biomedicine as they can be incorporated into cells affording a controllable means of “tagging” (6). These particles lead to a marked decrease in the magnetic resonance imaging (MRI) parameter T2* and the possibility of visualizing their localization noninvasively on T2*-weighted MRI (7–9). Furthermore, the magnetic properties of SPIOs allow them to be manipulated mechanically by a magnetic field gradient. This “action at a distance,” combined with the intrinsic penetrability of magnetic fields into human tissue, opens up potential applications involving the transport of magnetically tagged biological entities. Such tagging has to date mainly been the focus of drug delivery systems (10 –12), including drug targeting in humans (13). Recent efforts on cell targeting in the arterial circulation have been limited to animal models; to achieve cell capture, these have necessitated the use of large nonbiodegradable micron-sized beads (14 –16) or nanoparticle composites fabricated in-house (17), and in most cases, the additional introduction of permanent intravascular metallic devices not currently approved for human use (15–17). It may also be possible to attract gene-carrying cells to post-capillary venules of tumors (18). However, the targeted delivery of progenitor cells using external magnetic devices and clinically approved iron-bearing agents has not yet been accomplished. Early endothelial progenitor cells (EPCs) derived from CD34⫹/CD133⫹ cells (19,20) have been shown to be involved in post-ischemic neovascularization (21) and reendothelialization, reducing neointima formation following arterial injury (22). We chose to target EPCs to a site of rat common carotid artery (CCA) injury, as localization of such progenitors to sites of vascular catheterization may help prevent post-angioplasty restenosis (23,24). Although various SPIO formulations have been used in the past, their future use as clinical agents is not straightforward due to safety issues raised by cell labeling and the use of transfection agents. To obviate these concerns, we have chosen to label human EPCs with the U.S. Food and Drug Administration (FDA)- 795 approved nano-sized SPIO compound Endorem (Guerbet, Paris, France), the only agent to date that has been used to monitor cells in humans using MRI (8). Methods Cells. Human mononuclear cells (MNCs) were collected by leukapheresis from peripheral blood of donors stimulated with granulocyte colony-stimulating factor (25). We magnetically isolated the CD133⫹ progenitor cells using antihuman CD133 (epitope 1) microbeads (Miltenyi Biotec, Bergisch Gladbach, Germany). These beads are biodegradable and typically disintegrate after a few days in culture. Then, EPCs were derived by culturing CD133⫹ cells for up to 21 days on fibronectin-coated plates (BD, Franklin Lakes, New Jersey) in growth medium consisting of 20% fetal bovine serum/endothelial basal medium 2 (Lonza, Basel, Switzerland) and supplemented with fibroblast, insulinlike, and endothelial growth factors; ascorbic acid; heparin; and recombinant human vascular endothelial growth factor 165 (25 ng/ml) (R&D Systems, MinneAbbreviations apolis, Minnesota) (26). Growth and Acronyms media were supplemented with CCA ⴝ common carotid recombinant human stem cell facartery tor (100 ng/ml), rhFlt-3/Flk-2 liEPC ⴝ endothelial progenitor gand (50 ng/ml), and recombicell nant human interleukin 3 (10 ng/ FDA ⴝ Food and Drug ml) (R&D Systems) for the first Administration 72 h. MNCs were grown for 2 h MNC ⴝ mononuclear cell in serum-free Dulbecco’s modiMRI ⴝ magnetic resonance fied eagle medium (Gibco, Inimaging/images vitrogen, Carlsbad, California) SPIO ⴝ superparamagnetic followed by removal of nonadheriron oxide ent cells and culture of the adherent fraction in 10% fetal bovine serum/Dulbecco’s modified eagle medium. All blood samples were obtained with written consent and were approved by local ethics committees. Labeling of cells with SPIO. At day 9 of culturing, the CD133⫹ cells were labeled with the FDA-approved SPIO Endorem (also known as Feridex in the U.S.) (Guerbet) using 0.5 mg/ml SPIO in growth medium. Suspension CD133⫹ cells were labeled for 24 h and adherent cells for 1 h. Additionally, adherent cells were labeled for 2 or 24 h to increase the amount of iron in the cells. Mononuclear cells were labeled with SPIO by overnight incubation. Labeled cells were washed twice in 15 ml phosphatebuffered saline. Quantification of cellular SPIO uptake. We used a superconducting quantum interference device (27) to measure the amount of Fe3O4 in the cells. To separate SPIO signal from background signal coming from the cells and media, measurements were performed at –263oC. The samples were saturated in an applied field of 2-T, which was subsequently 796 Kyrtatos et al. Magnetic Tagging Increases Cell Delivery removed to leave the SPIO particles in a magnetized state. Comparison of this remnant signal with that of an undiluted SPIO sample of known Fe3O4 concentration allowed quantification of Fe3O4 per cell. Magnetic actuation. Neodymium iron boron permanent disk magnets (1.195-T, grade N35SH, Magnet Applications Ltd., Hertfordshire, United Kingdom) 22 mm in diameter and 16 mm in height were used to test cell viability and differentiation following magnetic attraction. The SPIO-labeled EPCs were placed 1 mm from the magnet surface (maximum: 19.8 T2/m). For the flow system and in vivo magnetic targeting, a magnetic actuator was constructed using 5 10 ⫻ 10 ⫻ 25-mm3 NdFeB grade N35 blocks, attached together inside a machined aluminum casing in a configuration of rotating magnetization (Halbach array), which concentrates the force on 1 side of the actuator (28). Viability assays. The CellTiter 96 AQueous One Solution Assay (Promega, Madison, Wisconsin) was performed after 24 h of magnetic attraction of labeled CD133⫹ cells. The tetrazolium compound in this assay undergoes reduction to a colored formazan product by viable cells, primarily mediated by reduced nicotinamide adenine dinucleotide phosphate (29). Colorimetric quantification of viability of samples of 3 ⫻ 104 CD133⫹ cells was performed using a spectrophotometric microplate reader (GENios, Tecan Group Ltd., Männedorf, Switzerland) (490 nm, at 4 h). Sample activity was normalized to the mean absorbance of control (no magnet). Cell apoptosis was analyzed using an annexin-V-fluorescein isothiocyanate/propidium iodide flow cytometric assay (ApoTarget, Invitrogen). Flow cytometry. Immunophenotypic characteristics of CD133⫹ cells labeled with SPIO at day 10 were analyzed with a fluorescence-activated cell sorter (FACSCalibur, BD) at day 21 of cultivation. Cells pre-treated with crystallizable fragment receptor blocking reagent (Miltenyi Biotec) were stained using the following antihuman antibodies: phycoerythrin (PE)-CD304 BDCA-4/neuropilin-1 (30), biotin-CD144/vascular endothelial cadherin (Bender MedSystems Inc., Burlingame, California) with streptavidinfluorescein isothiocyanate for endothelial differentiation; PE-CD14 and CD11b (BD Biosciences, San Jose, California) for monocytic differentiation. Fluorochrome- and dosematched isotypes were used as controls. Cells were suspended in 20 mmol/l N-2-hydroxyethylpiperazine-N-2ethanesulfonic acid/0.5% bovine serum albumin/phosphatebuffered saline containing 10 g/ml 7-aminoactinomycin D (Sigma Aldrich, St. Louis, Missouri). The 7-aminoactinomycin D–positive, nonviable cells were excluded and 1 ⫻ 104 viable cells were scored per analysis (CellQuestPro, BD). MRI. The SPIO-labeled CD133⫹ cells were embedded in low melting point agarose (0.5%, 37°C) at concentrations of 745, 165, 49.5, 16.5, and 0 ⫻ 103 cells/ml in 250-l Eppendorf tubes (Eppendorf North America, Westbury, JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 2, NO. 8, 2009 AUGUST 2009:794 – 802 New York) and were cooled to 4°C. Suspension in agarose allowed for homogeneous distribution of the cells. The tubes were imaged in a 9.4-T horizontal bore Varian MRI system (VNMRS, Varian Inc., Palo Alto, California) using a 39-mm radiofrequency coil (RAPID Biomedical GmbH, Rimpar, Germany). The T2*-weighted images were acquired using a spoiled gradient echo sequence (echo time [TE] ⫽ 25 ms, repetition time [TR] ⫽ 200 ms, flip angle [FA] ⫽ 30, 5122 matrix). The T2* maps were obtained from 20 echo times (TE ⫽ 2.5 to 30 ms, TR ⫽ 200 ms, FA ⫽ 30, 2562 matrix) and produced using the ImageJ MRI Analysis Calculator plug-in (K. Schmidt, ImageJ, U.S. National Institutes of Health, Bethesda, Maryland). Computer simulations and in vitro flow system. Magnet designs for acquiring optimal magnetic field strength to capture intravascular SPIO-labeled cells were modeled using Opera-2d and -3d (Cobham Technical Services, Aurora, Illinois) and COMSOL Multiphysics 3.1 (COMSOL Inc., Burlington, Massachusetts) software. Fluid flow rate, cell size and Fe3O4 content, and distance of magnet from the vessel were considered by solving for the Khan and Richardson hydrodynamic drag force and the attractive force from the magnet, in parabolic nonpulsatile laminar flow. Simulated cells were 10 m in diameter, 3.9 pg Fe3O4/cell, within a circulating blood volume of 20 ml. Cell capture was defined as approximation and contact with the vessel wall within the 50-mm length of the array. The Halbach magnet design described earlier was assessed in an in vitro flow system by placing 1 ⫻ 106/ml SPIO-labeled blood MNCs (3.5 pg Fe3O4/cell) in peristaltic pump-driven flow (10 ml/min, mean velocity: 0.4 m/s) using biocompatible (ISO 10993) Tygon S-54 elastic microtubing (SaintGobain Performance Plastics, Courbevoie, France). The magnet array was placed at distances of 1 and 5 mm from the tubing. The mean of 5 hemocytometer cell counts was calculated. Digital images were acquired using a standard dissection microscope and a digital camera. Vascular injury and in vivo magnetic targeting. Male Sprague-Dawley rats (n ⫽ 13, 380 to 420 g) (Charles River Laboratories International, Wilmington, Massachusetts) were anaesthetized using midazolam (625 g/100 g) and fentanyl (40 g/100 g) supported by halothane at 0.5% to 2% at 2 l/min oxygen. The left CCA was exposed at the bifurcation to the external and internal carotid artery and a 2-F embolectomy catheter (Edwards Lifesciences Corp., Irvine, California) was advanced proximally through an arteriotomy into the CCA. The catheter was inflated with 100 l of air and rotated as it was being retracted (31). The SPIO-labeled CD133⫹ cells were labeled with 5-mol/l CellTracker Green 5-chloromethylfluorescein diacetate (Invitrogen-Molecular Probes). This dye is activated by intracellular esterases and only stains viable cells. We administered 5 ⫻ 105 cells in the CCA, which was temporarily clamped for 10 min with the magnet array JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 2, NO. 8, 2009 AUGUST 2009:794 – 802 Kyrtatos et al. Magnetic Tagging Increases Cell Delivery 797 placed at a 5-mm distance. The circulation was restored and the magnet removed after a further 2 min of magnetic actuation (n ⫽ 5). Two types of controls were used: 1) CCA injury was performed and labeled cells were injected without magnetic actuation (n ⫽ 6); and 2) magnetic attraction of labeled cells was performed on uninjured vessels (n ⫽ 2). Tissues were retrieved 24 h later and fixed with 1% p-fluoro-phenylalanine/phosphate-buffered saline. All experimental procedures complied with the institutional guidelines for animal experiments. Confocal microscopy and quantitation of cell engraftment. Arteries were opened longitudinally and counterstained with 4=,6-diamidino-2-phenylindole (Vector Labs, Burlingame, California). Total arterial surface confocal microscope images were acquired using a Leica TCS SP2 confocal microscope. Reflectance scanning (32) was used to detect intracellular SPIO. Image processing was performed using the Volocity imaging software (Improvision, Waltham, Massachusetts). Background correction was performed using the “rolling ball” algorithm implemented in ImageJ software. Signal outliers were removed by application of a despeckle median filter (W.S. Rasband, ImageJ, U.S. National Institutes of Health). To analyze cell engraftment, x-y-z scans were rendered into a 3-dimensional vector graphic format; this enabled quantification the total volume of CellTracker-labeled cells per artery. Cell counts were calculated from the total volume based on a 10-m cell diameter and are presented per square millimeter of arterial surface area. Statistical analyses. We used SPSS version 11.5.1 (SPSS Inc., Chicago, Illinois) and Prism version 4.02 (Graphpad Software Inc., San Diego, California). Data were inspected visually and with the Shapiro-Wilk test for small samples to assess normality. The homogeneity of variance assumption was evaluated with the Levene test. Mean values are quoted with the standard error of the mean, medians are quoted with the interquartile range (IQR). The p values reported are 2-tailed and were considered statistically significant at the 5% level (p ⬍ 0.05). In the apoptosis assays, equivalence testing was considered appropriate because the null hypothesis was nondifference; 2 1-sided t tests were used with a 3% equivalence limit at the 0.05 level (Schuirmann test). A maximum acceptable difference of 3% was set a priori based on 24-h serum-deprived positive control cells (3% mean increase in early apoptosis, 16% increase in late apoptosis). Other statistical tests are specified in context. Results Cell labeling and biological assays. To demonstrate that the magnetic force following Endorem labeling was large enough to attract cells to the vessel wall through a liquid, we recorded the motion of labeled MNCs in real time as a Figure 1. Magnetic Attraction Causes Translocation of SPIO-Labeled MNC The estimated force is 19 pN per cell. (A) Video frames for t ⫽ 0 (application of magnet), 5, 10, and 15 s after exposure to the magnet. Relative position of the magnet is displayed. (B) Count of cells in field of view (20⫻ objective). The cells transiently acquire a magnetic dipole moment and experience intercell attraction, entering the field of view in aggregates (increase in count rate between 5 and 10 s). The cell count rate subsequently decreases as the suspension volume closest to the magnet is depleted of cells. MNC ⫽ mononuclear cell; SPIO ⫽ superparamagnetic iron oxide. magnetic force was applied (Fig. 1). Rapid movement toward the magnet was observed as the cells responded to the applied force. The CD133⫹-derived EPC viability was normal following labeling and magnetic attraction (Fig. 2A) and no increase in apoptosis was observed (Fig. 2B) when the amount of SPIO in the cells was controlled. Increased labeling resulted in a decrease in viability following magnetic attraction (Fig. 2A). This may be explained by force-induced mechanical damage of intracellular structures containing the iron nanoparticles (33). As shown in Figure 2C, there was normal expression of endothelial (vascular endothelial cadherin, CD304/NP-1) and monocytic (CD14, CD11b) markers of differentiation, 10 days after labeling. Using in vitro MRI, cells were visible on T2*weighted images at dilutions as low as 25 cells/mm2 and caused a marked reduction in T2* values from 8 cells/mm2 (Fig. 2D). Using a superconducting quantum interference device, we calculated that labeled cells contained on average 3.9 pg Fe3O4 per cell. Given the magnetic field applied in these experiments and the iron content of the cells, it is possible to estimate a “cell-safe” magnetic force for EPCs above which there is a risk of compromising viability; this was 9.3 pN per cell. External magnet design. An important consideration in our experimental model is that the rat CCA is a nonsuperficial structure approximately 5-mm from the skin in which there are large hydrodynamic forces acting on the cells, with peak systolic blood flow rate up to 10 ml/min (34,35). However, 798 Kyrtatos et al. Magnetic Tagging Increases Cell Delivery JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 2, NO. 8, 2009 AUGUST 2009:794 – 802 Figure 2. Labeling of CD133ⴙ Cells With SPIO (A) Viability assay following 24 h of magnetic attraction (n ⫽ 4 per group, analysis of variance with Tamhane T2 post hoc test). There was no notable effect on viability when the standard labeling method was used (adherent cells labeled for 1 h) when compared with the viability of the nonmagnet control group. Increased adherent cell labeling for 2 and 24 h resulted in a 20% and 75% decrease in viability after magnetic attraction, respectively. (B) Mean difference in apoptosis rates compared with apoptosis rates in the control group, at specified times after labeling and magnetic attraction. All groups passed equivalence testing with a 3% apoptosis limit. (C) Surface marker expression (percentage of live cells) at 10 days after labeling. No differences were observed on the expression of differentiation markers (CS vs. LS and CA vs. LA) for vascular endothelial cadherin (VE-Cad, n ⫽ 6), CD304 (NP1, n ⫽ 6), CD14 (n ⫽ 6), or CD11b (n ⫽ 3). (D) In vitro MRI; T2*-weighted images (i) and T2* maps (ii) with equivalent average T2* values plotted against cell concentration (iii). CA ⫽ control nonlabeled adherent fraction; CI ⫽ confidence intervals; CS ⫽ control nonlabeled suspension fraction; EA ⫽ early apoptosis; LA ⫽ late apoptosis (B) or SPIO-labeled adherent fraction (C); LS ⫽ SPIO-labeled suspension fraction; MRI ⫽ magnetic resonance imaging; N ⫽ necrosis; SEM ⫽ standard error of the mean; T2* ⫽ MRI parameter, sensitive to SPIO presence; other abbreviations as in Figure 1. there is a rapid decline of magnetic force at increased target tissue distances, which poses a challenge to magnetic targeting using external devices in vivo (6,11). To overcome this issue, we chose a permanent magnetic actuator design that increases the force magnitude at large distances (Halbach array). With this actuator placed at a 5-mm vertical distance from the target tissue, a computed maximum 8.7 pN force was applied on each cell, which is below the 9.3 pN limit. Computer simulations. We proceeded by modeling the distribution of magnetic forces at distances of 1 and 5 mm from the magnetic actuator (Fig. 3A) and simulated the hydrodynamic and magnetic forces on intraluminal CD133⫹ cells using finite element modeling. With the vessel placed 1 mm away from the actuator, 11% of flowing cells made contact with the endothelial surface at each pass through the vessel. With the actuator at 5 mm, 2.3% of cells made contact. If the cells adhered at the contact site, approximately 50% of cells would be extracted from the circulation within 15 min at 1 mm, or 60 min at 5 mm. In vitro flow system. We investigated the targeting ability of the actuator in vitro at the 2 distances using a 10-ml/min flow system. At 1 mm, cells accumulated above the points of predicted maximum force within 1 min after initiation of flow (Fig. 3B). These cell aggregates dissociated a few seconds after removal of the actuator. Targeting for 15 min at 1 mm resulted in 252-fold increase in capture (mean ⫽ 41 ⫻ 103 ⫾ 6 ⫻ 103 cells) versus control (mean ⫽ 163 ⫾ 41 cells) specimens. At 5 mm, there was a 6-fold increase in capture (mean ⫽ 1,630 ⫾ 276 cells) versus nontargeted Kyrtatos et al. Magnetic Tagging Increases Cell Delivery JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 2, NO. 8, 2009 AUGUST 2009:794 – 802 799 Figure 3. Computer Models and In Vitro Flow System (A) Magnet array in aluminum casing; 5 bar magnets with rotating magnetization (top, digital image) and corresponding computer model (bottom), with color-coding of magnetic force magnitude, magnetic field lines displaying 1-sided flux, and 1 or 5 mm distance used in experiments (dotted lines). (B) In vitro cell capture (top, digital images) at 1 min of 10 ml/min flow and corresponding force distribution along horizontal line 1 mm away from array (red plot), showing predicted peaks of force magnitude at magnet junctions and cell aggregates within the vessel at these points (arrows and close up). Graph (right) displays 252-fold increase in cell capture after 15 min of magnetic targeting at 1 mm; n ⫽ 3, p ⫽ 0.003 (2-sample t test). (C) Force along the 5 mm horizontal line (left, orange plot) and in vitro magnetic cell capture at 5 mm after 1 h of 10 ml/min flow (right); n ⫽ 4, p ⫽ 0.017 (2-sample t test with Welch correction). control (mean ⫽ 281 ⫾ 21 cells) specimens after 1 h of flow (Fig. 3C). External targeting in a small animal model. To investigate the in vivo feasibility of magnetic targeting using external magnets, we attempted to increase SPIO-CD133 cell engraftment to a site of rat CCA injury by placing the actuator adjacent to the ventral aspect of the animal’s neck. Images in Figures 4A and 4B display representative (median) confocal scans of the arterial surface 24 h after cell delivery; there is a notable increase in cell retention following magnetic targeting. High power magnification (Fig. 4D) confirmed the presence of nucleated cells (using 4=,6-diamidino-2phenylindole) and the presence of intracellular clusters of SPIO nanoparticles in CD133⫹ cells was confirmed using reflectance confocal microscopy (Fig. 4E). Application of an external magnetic force using the actuator during and after cell delivery increased CD133⫹ cell engraftment to the injured vascular surface by a factor of 5.4 (median ⫽ 134, IQR: 47 to 362 cells/mm2) compared with cell delivery without the magnet (median ⫽ 25, IQR: 17 to 42 cells/ mm2). In the absence of vascular injury (control studies), no cells engrafted to the endothelial surface when the magnetic force was applied (cell count ⫽ 0). Discussion The concept of magnetic tagging and targeting could play an important role for future advances in delivery and noninvasive monitoring of cell-based therapeutic interventions. This is the first attempt to use a clinically approved agent to externally target EPCs in a high-flow system such as the arterial vasculature. We chose to use EPCs for this study as these may hold high therapeutic value for the future. Endothelial damage is an initiating event in many cardiovascular disorders. Transplantation of these early progenitor cells, which resemble hemangioblasts in their properties of marker expression, proliferation, migration, and differentiation, may expand the therapeutic arsenal to repair vessels or endothelium and improve perfusion of ischemic tissues by providing new progenitor cells capable of responding to angiogenic stimuli, and have recently been used for cardiac neovascularization in clinical trials (36 – 40). In the majority of these and other studies on cardiac regeneration, cells were administered via intracoronary injection with “flow-stop” periods of several minutes to increase engraftment; yet it has been shown that despite this 800 Kyrtatos et al. Magnetic Tagging Increases Cell Delivery JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 2, NO. 8, 2009 AUGUST 2009:794 – 802 Figure 4. Magnetic Targeting Following Balloon Angioplasty (A) Sample 2-dimensional tile, total surface area scanning of the luminal side of a rat common carotid artery following injury and cell delivery without magnetic targeting; 18 cells/mm2. (B) Cell delivery with targeting; 142 cells/mm2. Square box included for orientation. (C) A 3-dimensional reconstruction used for quantitation. Objects meeting signal intensity and volume threshold criteria are shown in pink. (D) High power magnification of specimen showing CellTracker-labeled cells (green) adhering to the injured vascular intima. Cell nuclei are labeled with 4,6-diamino-2-phenylindole (blue). (E) Reflectance confocal image of a CD133⫹ cell showing SPIO-nanoparticles (yellow). (F) Magnetic targeting increased adhesion of SPIO-labeled, CD133⫹-derived to the injured vascular intima (n ⫽ 5) versus to the nontargeted control group (n ⫽ 6); p ⫽ 0.017 (Wilcoxon-Mann-Whitney exact test). Medians are highlighted in red. Boxes represent the quartiles and whiskers extend to the last value within 1.5 interquartile range from the quartiles. Cross (ⴙ) represents a value at 581 cells/mm2. Abbreviation as in Figure 1. maneuver, only 1% to 3% of the cells remain on site (1,41), and there is a pressing need for targeting strategies (42). We have based our cell targeting technique on a biodegradable iron oxide nanoparticle preparation, which should facilitate transition to human studies, in contrast to other nonbiodegradable agents used in cell tracking (43,44) and targeting applications (14 –16). Previous investigations have indicated that application of a magnetic force on labeled cells can distort intracellular membranes (33). We noted that the application of a magnetic force for 24 h had the potential to compromise cell viability, an effect that was dependent on the extent of iron loading. Although we did not evaluate this in the current study, we anticipate that higher magnetic forces will be tolerable if applied for shorter lengths of time. By controlling iron uptake and the specific design of magnetic devices, we have been able to safely attract cells without affecting cell viability, apoptosis, or differentiation in culture. Most importantly, our data suggest that by tagging human EPCs with an FDA-approved agent, it is possible to safely target them in static and flowing conditions in vitro and in vivo. We have assembled and tested a specialized external magnetic actuator using an in vitro flow system. Using this actuator, we have also been able to enhance cell localization following common carotid artery injury in an animal model; the increase in engraftment was 5-fold higher than in control (nontargeted) cells. In this study, a flow interruption period was implemented, which is similar to those employed in clinical trials and is a favorable condition for cell enrichment. Our computer simulations and in vitro data suggest that in the presence of high flow rates at the target area, very few cells are captured under nontargeted conditions, which allows up to 252-fold enhancement in vitro using magnetic attraction, depending on the distance of the target tissue. This highlights the potential for extensive targeting in the cardiovascular system, even in areas of high blood velocity. Nevertheless, further in vivo studies are warranted to assess EPC engraftment in a variety of flowing conditions following peripheral intravenous injection. Our results also emphasize a key issue regarding external targeting in vivo; invariably, cells flowing in vessels closer to the magnetic source than the target tissue will also be targeted (6). However, such cells should be released following removal of the magnetic JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 2, NO. 8, 2009 AUGUST 2009:794 – 802 source in the absence of an underlying biological mechanism to keep them engrafted, as observed both in our in vitro flow experiments and our noninjured control subjects in vivo. In the injured arteries, we were not able to provide a circumferential external magnetic force; previously this problem has been partially circumvented by axial rotation of the animal (14). Despite this fact, we did not observe any consistent preferential targeting of the cells in the arterial specimens. This may be due to a combination of factors. The broad distribution of magnetic targeting forces due to the large size of the magnetic actuator compared with the size of the artery (at least 100o arc) is likely to disperse the targeted cells. Small within-vessel variations in the extent of damage, unrelated of the direction of the magnetic force, could further facilitate nondirectional engraftment. In addition, the flow during the 24-h recirculation period may enable cells to migrate away from the targeted regions to areas of more pronounced damage. Indeed, in a recent study, despite the presence of an intravascular permanently magnetized device for 24 h, iron-labeled cells were present in the damaged areas adjacent to the device, as well as on it (15). The magnetic control of cells inside the vasculature is a fascinating and promising concept. In this preliminary report, we have outlined the feasibility of external targeting in the arterial circulation using a clinical-grade agent, bringing this technology a step closer to intervention in humans. Long-term studies will be necessary to investigate the retention of the cells at the site of engraftment, confirming a functionally beneficial increase in healing following magnetic targeting. Ultimately, we envisage concurrent MR imaging and MR-based magnetic guidance of labeled cells in the body, possibly in a manner similar to magnetic guidance of intravascular catheters (45) and magnetic beads (46). This approach could augment localization and simultaneous monitoring of cells in other organ systems such as the heart or the brain and may prove complementary to the systemic injection of cell therapies, thus expanding the horizon of cardiovascular interventions and the future of stem cell therapeutic strategies. Reprint requests and correspondence: Dr. Mark Lythgoe, Centre for Advanced Biomedical Imaging, University College London, 72 Huntley Street, WC1E 6DD London, United Kingdom. E-mail: mlythgoe@ich.ucl.ac.uk. REFERENCES 1. Hristov M, Weber C. The therapeutic potential of progenitor cells in ischemic heart disease—past, present and future. Basic Res Cardiol 2006;101:1–7. 2. Laflamme MA, Murry CE. Regenerating the heart. Nat Biotechnol 2005;23:845–56. Kyrtatos et al. Magnetic Tagging Increases Cell Delivery 801 3. Segers VF, Lee RT. Stem-cell therapy for cardiac disease. Nature 2008;451:937– 42. 4. Abdel-Latif A, Bolli R, Tleyjeh IM, et al. Adult bone marrow-derived cells for cardiac repair: a systematic review and meta-analysis. Arch Intern Med 2007;167:989 –97. 5. Bartunek J, Dimmeler S, Drexler H, et al., on behalf of Task Force of the European Society of Cardiology. The consensus of the task force of the European Society of Cardiology concerning the clinical investigation of the use of autologous adult stem cells for repair of the heart. Eur Heart J 2006;27:1338 – 40. 6. Pankhurst Q, Connoly J, Jones S, Dobson J. Applications of magnetic particles in biomedicine. J Phys D Appl Phys 2003;36:167– 81. 7. Bulte JW, Kraitchman DL. Iron oxide MR contrast agents for molecular and cellular imaging. NMR Biomed 2004;17:484 –99. 8. de Vries I, Lesterhuis WJ, Barentsz JO, et al. Magnetic resonance tracking of dendritic cells in melanoma patients for monitoring of cellular therapy. Nat Biotechnol 2005;23:1407–13. 9. Panizzo RA, Kyrtatos PG, Price AN, Gadian DG, Ferretti P, Lythgoe MF. In vivo magnetic resonance imaging of endogenous neuroblasts labelled with a ferumoxide-polycation complex. Neuroimage 2009;44: 1239 – 46. 10. Chertok B, Moffat BA, David AE, et al. Iron oxide nanoparticles as a drug delivery vehicle for MRI monitored magnetic targeting of brain tumors. Biomaterials 2008;29:487–96. 11. Dobson J. Magnetic nanoparticles for drug delivery. Drug Dev Res 2006;67:55– 60. 12. Hafeli UO. Magnetically modulated therapeutic systems. Int J Pharm 2004;277:19 –24. 13. Wilson MW, Kerlan RK Jr., Fidelman NA, et al. Hepatocellular carcinoma: regional therapy with a magnetic targeted carrier bound to doxorubicin in a dual MR imaging/conventional angiography suite— initial experience with four patients. Radiology 2004;230:287–93. 14. Consigny PM, Silverberg DA, Vitali NJ. Use of endothelial cells containing superparamagnetic microspheres to improve endothelial cell delivery to arterial surfaces after angioplasty. J Vasc Interv Radiol 1999;10:155– 63. 15. Pislaru SV, Harbuzariu A, Gulati R, et al. Magnetically targeted endothelial cell localization in stented vessels. J Am Coll Cardiol 2006;48:1839 – 45. 16. Pislaru SV, Harbuzariu A, Agarwal G, et al. Magnetic forces enable rapid endothelialization of synthetic vascular grafts. Circulation 2006; 114:I314 – 8. 17. Polyak B, Fishbein I, Chorny M, et al. High field gradient targeting of magnetic nanoparticle-loaded endothelial cells to the surfaces of steel stents. Proc Natl Acad Sci U S A 2008;105:698 –703. 18. Muthana M, Scott SD, Farrow N, et al. A novel magnetic approach to enhance the efficacy of cell-based gene therapies. Gene Ther 2008;15: 902–10. 19. Duda DG, Cohen KS, Scadden DT, Jain RK. A protocol for phenotypic detection and enumeration of circulating endothelial cells and circulating progenitor cells in human blood. Nat Protoc 2007;2: 805–10. 20. Peichev M, Naiyer AJ, Pereira D, et al. Expression of VEGFR-2 and AC133 by circulating human CD34(⫹) cells identifies a population of functional endothelial precursors. Blood 2000;95:952– 8. 21. Rafii S, Lyden D. Therapeutic stem and progenitor cell transplantation for organ vascularization and regeneration. Nat Med 2003;9:702–12. 22. Hristov M, Weber C. Endothelial progenitor cells in vascular repair and remodeling. Pharmacol Res 2008;58:148 –51. 23. Ward MR, Stewart DJ, Kutryk MJ. Endothelial progenitor cell therapy for the treatment of coronary disease, acute MI, and pulmonary arterial hypertension: current perspectives. Catheter Cardiovasc Interv 2007; 70:983–98. 24. Gulati R, Jevremovic D, Peterson TE, et al. Autologous culturemodified mononuclear cells confer vascular protection after arterial injury. Circulation 2003;108:1520 – 6. 25. Korbling M, Reuben JM, Gao H, et al. Recombinant human granulocyte-colony-stimulating factor-mobilized and apheresiscollected endothelial progenitor cells: a novel blood cell component for therapeutic vasculogenesis. Transfusion 2006;46:1795– 802. 802 Kyrtatos et al. Magnetic Tagging Increases Cell Delivery 26. Quirici N, Soligo D, Caneva L, Servida F, Bossolasco P, Deliliers GL. Differentiation and expansion of endothelial cells from human bone marrow CD133(⫹) cells. Br J Haematol 2001;115:186 –94. 27. Hautot D, Pankhurst QA, Dobson J. Superconducting quantum interference device measurements of dilute magnetic materials in biological samples. Rev Sci Instrum 2005;76:045101. 28. Mallinson J. One-sided fluxes—a magnetic curiosity? IEEE Trans Magn 1973;9:678 – 82. 29. Berridge MV, Tan AS. Characterization of the cellular reduction of 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT): subcellular localization, substrate dependence, and involvement of mitochondrial electron transport in MTT reduction. Arch Biochem Biophys 1993;303:474 – 82. 30. Fons P, Herault JP, Delesque N, Tuyaret J, Bono F, Herbert JM. VEGF-R2 and neuropilin-1 are involved in VEGF-A-induced differentiation of human bone marrow progenitor cells. J Cell Physiol 2004;200:351–9. 31. Santiago FS, Ishii H, Shafi S, et al. Yin Yang-1 inhibits vascular smooth muscle cell growth and intimal thickening by repressing p21WAF1/Cip1 transcription and p21WAF1/Cip1-Cdk4-cyclin D1 assembly. Circ Res 2007;101:146 –55. 32. Green CR, Holloway H, Walker MM. Detection of submicroscopic magnetite particles using reflectance mode confocal laser scanning microscopy. Cell Biol Int 2001;25:985–90. 33. Wilhelm C, Cebers A, Bacri JC, Gazeau F. Deformation of intracellular endosomes under a magnetic field. Eur Biophys J 2003;32: 655– 60. 34. Garcia-Villalon AL, Roda JM, Alvarez F, Gomez B, Dieguez G. Carotid blood flow in anesthetized rats: effects of carotid ligation and anastomosis. Microsurgery 1992;13:258 – 61. 35. Miyashiro JK, Poppa V, Berk BC. Flow-induced vascular remodeling in the rat carotid artery diminishes with age. Circ Res 1997;81:311–9. 36. Bartunek J, Vanderheyden M, Vandekerckhove B, et al. Intracoronary injection of CD133-positive enriched bone marrow progenitor cells promotes cardiac recovery after recent myocardial infarction: feasibility and safety. Circulation 2005;112:I178 – 83. 37. Stamm C, Kleine HD, Choi YH, et al. Intramyocardial delivery of CD133⫹ bone marrow cells and coronary artery bypass grafting for chronic ischemic heart disease: safety and efficacy studies. J Thorac Cardiovasc Surg 2007;133:717–25. JACC: CARDIOVASCULAR INTERVENTIONS, VOL. 2, NO. 8, 2009 AUGUST 2009:794 – 802 38. Losordo DW, Schatz RA, White CJ, et al. Intramyocardial transplantation of autologous CD34⫹ stem cells for intractable angina: a phase I/IIa double-blind, randomized controlled trial. Circulation 2007;115: 3165–72. 39. Erbs S, Linke A, Adams V, et al. Transplantation of blood-derived progenitor cells after recanalization of chronic coronary artery occlusion: first randomized and placebo-controlled study. Circ Res 2005;97: 756 – 62. 40. Schachinger V, Assmus B, Britten MB, et al. Transplantation of progenitor cells and regeneration enhancement in acute myocardial infarction: final one-year results of the TOPCARE-AMI trial. J Am Coll Cardiol 2004;44:1690 –9. 41. Charwat S, Gyongyosi M, Lang I, et al. Role of adult bone marrow stem cells in the repair of ischemic myocardium: current state of the art. Exp Hematol 2008;36:672– 80. 42. Roncalli JG, Tongers J, Renault MA, Losordo DW. Endothelial progenitor cells in regenerative medicine and cancer: a decade of research. Trends Biotechnol 2008;26:276 – 83. 43. Hill JM, Dick AJ, Raman VK, et al. Serial cardiac magnetic resonance imaging of injected mesenchymal stem cells. Circulation 2003;108: 1009 –14. 44. Hinds KA, Hill JM, Shapiro EM, et al. Highly efficient endosomal labeling of progenitor and stem cells with large magnetic particles allows magnetic resonance imaging of single cells. Blood 2003;102: 867–72. 45. Faddis MN, Blume W, Finney J, et al. Novel, magnetically guided catheter for endocardial mapping and radiofrequency catheter ablation. Circulation 2002;106:2980 –5. 46. Tamaz S, Gourdeau R, Chanu A, Mathieu JB, Martel S. Real-time MRI-based control of a ferromagnetic core for endovascular navigation. IEEE Trans Biomed Eng 2008;55:1854 – 63. Key Words: endothelial cells 䡲 local delivery 䡲 magnet 䡲 targeting 䡲 angioplasty. APPENDIX For more details regarding the methods and calculations used in this study, please see the online version of this article.