To Tap or Not To Tap: When Ascites is Not...
advertisement

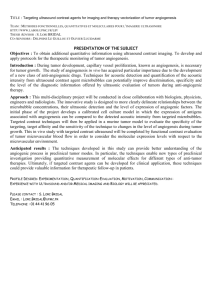
To Tap or Not To Tap: When Ascites is Not Ascites Ben Tomlinson MD (1), Heather Vierra MD (1), Rajendra Ramsamooj, MD () 1. Department of Internal Medicine. 2. Department of Patholgy. University of California, Davis Medical Center; Sacramento, CA PATIENT’S COURSE Z INTRODUCTION While ultrasound is the most sensitive and specific method of identifying ascities, most texts and guidelines consider it optional prior to therapeutic paracentesis. We present a case of desmoplastic small round blue cell tumor, a rare tumor most commonly seen in young men and adolescents, feigning large volume ascites in a patient with shortness of breath. Patient’s CT scans with contrast from initial presentation and after three cycles of chemotherapy. Bulky intrabdominal lymphadenopathy and liver metastases are the primary findings. Arrows highlight the displacement of the inferior vena cava – highlighting the improvement with therapy and the intrabdominal masses. LEARNING OBJECTIVES 1. Discuss the use of ultrasound in therapeutic paracentesis with malignant ascites. 2. Review the presentation, epidemiology, and pathological characteristics of desmoplastic small round blue cell tumor (DSCT). THE CASE: A 21 year old man Background: Patient was diagnosed with DSCT during a previous admission 5 months prior to presentation. Chief complaint at the time was abdominal distension and weight loss occurring over several weeks to months. Initial workup revealed diffuse large abdominal lymphadenopathy, and a 10x15cm pelvic mass. Core needle biopsy of mass identified DSCT. Patient was offered chemotherapy at time of diagnosis but chose to forgo therapy against medical advice and was discharged home. There was no further interaction with the health system until second presentation. Chief Complaint: Shortness of breath, leg edema and abdominal distension History of Present Illness: Patient reported that since his prior discharge, he returned to his daily routine as best as possible. Prior to this presentation, patient reported that his abdominal distension had become significantly worse over the few weeks preceding also with progressive leg swelling. His feet became swollen to the point where ambulating without assistance was very difficult. Moreover, over the final 2-3 days he reported increasing dyspnea on exertion that had reached the point where he had the sensation at rest. Additional review of systems was otherwise negative Past Medical History: Only significant for his previous admission and cancer diagnosis. There was no significant family or surgical history. Physical Exam: Vitals Signs – P: 145 RR: 28 T: 38.5 BP: 132/92 SpO2: 95% on RA General Appearance: thin, cachetic young man in moderate distress.. Mouth: moist mucous membranes, normal dentition, no throat erythema. Neck: Thin Lymphadenopathy: no cervical, supraclavicular, submandibular, submental, periauricular, occipital lymphadenopathy, or axillary lymphadenopathy Heart: tachycardic, but normal s1,s2 no murmurs, gallops, or rubs . Lungs: Very short lung fields, but no obvious wheezes, crackles, or rhonchi Abdomen: no audible bowel sounds, very distended, taught, dull to percussion diffusely. No obvious fluid wave, and tests for shifting dullness were equivocal. Genitourinary: scrotal edema Extremities: +2 radial and dorsalis pedis pulses, +3 pitting lower extremity edema, equal bilaterally. Patient’s CT scan identified large pleural effusion that contributed to patient’s compressive atelectasis. He received thoracentesis with immediate relief of his shortness of breath. Patient remained an inpatient to start a modified course of chemotherapy generally used for Ewing’s sarcoma. He received a pleural catheter to control his malignant pleural effusion. Patient was ultimately discharged. Five months later, he has completed three cycles of chemotherapy with significant improvement in his weight, abdominal distension, and functional status, as well as control of his pleural catheter. Initial Presentation DISCUSSION Ultrasound for paracentesis After 3 cycles of chemotherapy Second Presentation Non-contrast CT scan from second presentation. Patient’s abdominal girth is primarily from solid growth of tumor (arrows) with only very small areas of ascites. Scout image from CT scan – highlight’s the patient’s profile at his second presentation Ultrasound of Abdomen. Demonstrates solid appearance of abdominal metastases. Desmosplastic Small Round Blue Cell Tumor (DSCT) DSCTs are a rare neuroendocrine tumor with sarcoma-like features. Initially described in the 1980s as a distinct tumor, they are primarily a disease of young persons with male predominance (5:1). The tumor’s course is aggressive and prognosis is typically poor. Patients will typically respond to chemotherapy for several months before the disease relapses. This patient’s presentation is classic for this tumor type. He initially presented with abdominal distension and cachexia. Moreover, on his later presentations, despite the high intraabdominal tumor burden, this patient displayed no symptoms of bowel or bladder obstruction, which prior case series have also noted as a feature. Knowledge of this tumor type can be important, even for the general internist, as cases can be confused with other malignancies. Indeed, the initial working diagnosis for this patient was lymphoma prior to biopsy. Confusion regarding the diagnosis can persist if an institution’s pathology department is unfamiliar with this rare tumor . DSCT should be included in the differential diagnosis of any young person, especially men, with new, large intrabdominal mass. Histology of patient’s tumor demonstrates the classic description of DSRBC tumor cells. On the left, small round cells are found along with desmoplastic stroma (arrows). Laboratory: On the right, a high power view demonstrates the high nucleus-tocytoplasmic ratio in a group of cells surrounded by desmoplastic stroma. Imaging: REFERENCES 1. 2. Excluding the surrounding stroma, these cells are morphologically similar to other small round cell tumors, such as Ewing’s sarcoma, or neuroectodermal tumors. Chest X-Ray: Noted to be compatible with ascites with compressive atelectasis and marked volume loss in the lungs CT Scans and ultrasound are displayed in figures 1 and 2. For many practicing physicians, the use of ultrasound to identify ascites prior to large volume paracentesis has become almost routine. Yet clinical guidelines, including suggested guidelines for cancer patients in palliative settings, generally advocate that ultrasound continues to be optional. This patient’s personal history of two-to-three weeks of worsening distension with history of malignancy, development of shortness of breath and the presence of the most sensitive physical exam findings of distension and lower extremity edema were highly suggestive of new onset large volume ascites. However, the use of ultrasound only identified small pockets of ascites. An attempted paracentesis may have placed the patient at risk of complication, and delayed the diagnosis of his pleural effusion as a significant contributor to his shortness of breath. Most guidelines cite a case series of ultrasound for paracentesis published in JAMA in the 1980s by Bard et al. Yet, this article’s purpose was to advocate for more frequent use as ultrasound was found to identity small bowel or other hazards near the site of paracentesis in many patients. Admittedly, published case series of paracentesis generally find rates of complications less than 1%, even without ultrasound, and no studies have directly compared paracentesis with or without it. However, studies on numerous other procedures suggest improved complication rates with ultrasound visualization. Given the already wide clinical practice, it may be time for guidelines to be updated. 3. 4. 5. Histology Figure 1 – Low Power Histology Figure 2 – High Power Bard C, Lafortune M, Breton G. Ascites: ultrasound guidance or blind paracentesis? CMAJ. Aug 1 1986;135(3):209-210. Chang F. Desmoplastic small round cell tumors: cytologic, histologic, and immunohistochemical features. Arch Pathol Lab Med. May 2006;130(5):728-732. Gerald WL, Miller HK, Battifora H, Miettinen M, Silva EG, Rosai J. Intra-abdominal desmoplastic small round-cell tumor. Report of 19 cases of a distinctive type of high-grade polyphenotypic malignancy affecting young individuals. Am J Surg Pathol. Jun 1991;15(6):499-513. Kushner B, LaQuaglia M, Wollner N, et al. Desmoplastic small round-cell tumor: prolonged progression-free survival with aggressive multimodality therapy. Journal of Clinical Oncology. May 1, 1996 1996;14(5):1526-1531. McGibbon A, Chen GI, Peltekian KM, van Zanten SV. An evidence-based manual for abdominal paracentesis. Dig Dis Sci. Dec 2007;52(12):3307-3315.