Annals of Internal Medicine Transmission of Tuberculosis in a Jail
advertisement

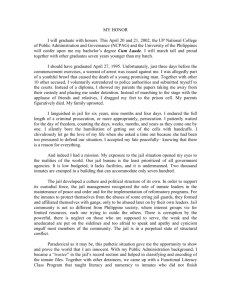
19 October 1999 Volume 131 Number 8 Annals of Internal Medicine Transmission of Tuberculosis in a Jail Timothy F. Jones, MD; Allen S. Craig, MD; Sarah E. Valway, DMD, MPH; Charles L. Woodley, PhD; and William Schaffner, MD Background: Outbreaks of tuberculosis are uncommonly recognized in jails. In 1996, an increase in active tuberculosis cases was noted among inmates of a large urban jail. Objectives: To determine the source and extent of a tuberculosis outbreak in an urban jail and to recommend control measures. Design: Retrospective cohort study. Setting: Urban jail. Patients: Inmates and guards with tuberculosis. Intervention: Outbreak evaluation and control. Measurements: Medical records of inmates and guards with tuberculosis were reviewed, and inmates were interviewed. DNA fingerprinting was performed on Mycobacterium tuberculosis isolates. Results: From 1 January 1995 through 31 December 1997, active tuberculosis was diagnosed in 38 inmates and 5 guards from the jail. Nineteen (79%) of the 24 culturepositive inmates had isolates with DNA fingerprints matching those of other inmates. Isolates from both culturepositive guards matched the predominant inmate strain; only 6 (14%) of 43 isolates from infected persons in the community had this pattern. The median length of incarceration of all inmates in the jail was 1 day; the median length of continuous incarceration before diagnosis of tuberculosis in inmates was 138 days. Inmates with tuberculosis had been incarcerated a median of 15 times. Fortythree percent of persons in this city with tuberculosis diagnosed from January 1995 through July 1997 had been incarcerated in the jail at some time before diagnosis. Conclusions: Traditional and molecular epidemiologic investigations suggest that tuberculosis was transmitted among inmates and guards in an urban jail. Aggressive measures to screen for active tuberculosis upon incarceration are important for preventing spread of disease in jails and to the surrounding community. Ann Intern Med. 1999;131:557-563. T uberculosis is a problem in correctional facilities throughout the United States. In 1996, 3.7% of all cases of tuberculosis nationwide occurred among residents of correctional facilities (1). Although in 1996 the incidence of new cases of active tuberculosis in the United States was 8.0 per 100 000 persons (1), many prison systems have reported rates of 200 per 100 000 persons and higher (2–10). Transmission of tuberculosis from prisons into surrounding communities has been documented (5), and correctional facilities may be important reservoirs of infection (11–13). One study concluded that a prison was potentially linked to 9% of a state’s tuberculosis cases during a 5-year period (5), and another study indicated that 24% of the tuberculosis cases in a county were associated with its jail (14). Prisons house convicts after sentencing, usually for terms exceeding 1 year (15). In contrast, jails receive prisoners immediately after arrest and generally house inmates awaiting trial or those sentenced to terms less than 1 year (16). Most jails are operated by cities or counties and hold inmates from the local community. In 1993, nearly 10 million inmates were admitted to local jails (16). Only 6% of jails house more than 50% of the nation’s jail inmates (16). Incarcerated populations have high rates of substance abuse, HIV infection, tuberculous infection, low socioeconomic status, and other risk factors associated with active tuberculosis (15, 17). At least 14 reports of outbreaks of tuberculosis in U.S. prisons have been published since 1985 (3, 5–7, 18, 19), but only two published reports have concerned outbreaks in jails (14, 20). Memphis, Tennessee, has the fifth largest jail in the United States (16). In 1996, the number of reported cases of tuberculosis diagnosed in inmates from the Memphis jail increased. This report summarizes the results of the ensuing investigation. See editorial comment on pp 617-618. For author affiliations and current addresses, see end of text. © 1999 American College of Physicians–American Society of Internal Medicine 557 Methods We reviewed the medical records of all persons in whom tuberculosis was diagnosed from 1 January 1995 through 31 December 1997 while they were incarcerated in the Memphis Criminal Justice Center (subsequently referred to as the “jail”). We obtained medical records from the jail, the Memphis/ Shelby County Health Department Tuberculosis Clinic, and the hospital to which inmates were admitted for evaluations. For all inmates with active tuberculosis, computerized jail records were analyzed to determine dates of incarceration and cell locations for the 2 years before their diagnosis. A patient with a confirmed case of active tuberculosis had Mycobacterium tuberculosis isolated from a clinical specimen or met a clinical case definition (21). Clinical cases met the following criteria: 1) a positive result on a tuberculin skin test, 2) signs and symptoms compatible with tuberculosis (for example, an abnormal, unstable chest radiograph or clinical evidence of current disease), and 3) treatment with at least two antituberculosis medications. Inmate cases were defined as patients in whom confirmed tuberculosis was diagnosed while they were incarcerated in the jail or within 3 weeks of transfer from the jail to another penal facility in the same city. Persons with culture-positive pulmonary tuberculosis were considered infectious from 6 weeks before collection of the first positive specimen until 2 weeks after initiation of appropriate therapy. A positive tuberculin skin test result was defined as at least 10 mm of induration within 48 to 72 hours after administration of five tuberculin units of tuberculin purified-protein derivative by the Mantoux method. Efforts were made to contact inmates who received a diagnosis of active tuberculosis after 1 January 1995, including those living in the community or incarcerated in other correctional facilities. A standardized questionnaire was administered to persons who could be located; the questionnaire asked Figure 1. 558 about the patient’s lifestyle outside the jail before diagnosis of tuberculosis (for example, places frequented, behaviors, living and working situations, and exposure to persons with tuberculosis). Patients were also asked about incarceration history, possible contacts during incarceration, and activities while in jail. Jail administrators were interviewed and records were reviewed to determine baseline information on the jail population. The average age of inmates was calculated from a sample of 2552 inmates released or transferred from the jail on 12 randomly selected days in 1997. Inmate intake procedures at the jail were observed by two separate investigators on different days. Records from annual tuberculin skin test screening of jail staff, performed by the county health department on site at the jail, were reviewed. Medical records of staff with confirmed tuberculosis between 1 January 1995 and 31 December 1997 were also reviewed. The Tennessee Department of Health registry of all persons in Memphis reported with active tuberculosis from January 1995 through July 1997 was cross-matched with the list of persons incarcerated in the Memphis jail since 1979. Deoxyribonucleic acid fingerprinting was performed on all available M. tuberculosis isolates from culture-positive inmates and guards. Fingerprinting was also done for a sample of community cases, chosen by selecting every fifth isolate from a list of all culture-positive cases of tuberculosis in Memphis from 1 January 1995 through 1 September 1997, sorted by date of treatment initiation. If no isolate was available for the case selected, the next community case on the list was substituted. The Tennessee Department of Health Laboratory had processed 99.5% of all specimens from culture-positive cases reported from Memphis during the study period. Isolates were fingerprinted at the Centers for Disease Control and Prevention by IS-6110 restriction fragment length polymorphism analysis (22). Bivariate statistical analyses were performed by us- Distribution of lengths of incarceration of inmates in the Memphis jail, 1995 to 1997. 19 October 1999 • Annals of Internal Medicine • Volume 131 • Number 8 results. Inmates who volunteer are counseled about and tested for HIV at the jail by county health department representatives. Of the inmates admitted to the jail during this 3-year period, less than 1% were screened for HIV there. Of 1622 HIV tests performed, 26 (1.6%) had positive results. ing chi-square tests calculated with Epi Info software (23). Results Jail Characteristics Inmate Tuberculosis Cases The jail housed approximately 2700 inmates at any time. More than 173 000 persons were admitted and discharged during the 3-year period. A mean of 159 inmates were admitted daily; the median length of stay was 1 day, and 8.3% of inmates stayed more than 30 days (Figure 1). Of persons admitted to the jail, 82% had previously been incarcerated there. The inmate population was 90% black and 90% male. The mean age of inmates was 32 years. Inmates were housed on seven floors. Some units held up to 36 inmates in a single large room; other units had 18 two-person cells, and the 36 inmates intermingled for much of the day. Inmates lived and ate with members of the same unit, although inmates from different units had the potential to intermingle at visitation; during gym, chapel, infirmary, and legal-room (library) visits; and during transport outside the facility. For security reasons, inmates were moved frequently within the jail. Active tuberculosis was diagnosed in 38 jail inmates from 1 January 1995 through 31 December 1997 (Figure 2). Ten cases were diagnosed in 1995, 19 in 1996, and 9 in 1997. The calculated incidence of active tuberculosis diagnosed in inmates who were physically in the jail was 274 per 100 000 during this 3-year period. Inmates with tuberculosis had been in the jail a median of 15 times before diagnosis. The median length of continuous incarceration before the diagnosis of tuberculosis was 138 days (range, 10 to 800 days) (Table). By comparison, the median length of incarceration for all inmates in the jail is 1 day (mean, 13.4 days). Ten (26%) of the inmates with active tuberculosis were given the diagnosis during evaluation for symptoms, 25 (66%) were discovered as a result of evaluation of a positive tuberculin skin test result, and 3 (8%) were found during contact investigations of other cases. Of the 38 inmates with a diagnosis of tuberculosis, 24 had positive cultures. Sixteen (67%) of the 24 jail inmate isolates of Mycobacterium tuberculosis Jail Screening Procedures Routine medical screening at intake to the jail consisted of two questions: “Are you seeing a doctor for anything?” and “Are you taking any medications?” This screening process took approximately 15 seconds per inmate. If the screening procedure did not reveal an obvious history of tuberculosis, the inmate was admitted into the general jail population. Jail protocol called for tuberculin skin test screening of all inmates still in the facility 10 days after admission. Inmates with evidence of possible tuberculosis on initial screening, in subsequent medical visits, or on tuberculin skin test screening were transported to a hospital emergency department or the county health department tuberculosis clinic for chest radiographs and evaluation. Those thought to have possible active tuberculosis were then transferred to a local hospital for isolation and completion of evaluation. Inmates given a diagnosis of active tuberculosis were returned to the jail after three sputum smears were negative for acid-fast bacteria. The jail does not have radiography facilities or negative-pressure isolation rooms. From 1995 through 1997, 173 815 inmates were admitted to the jail; 13 239 (7.8%) inmates underwent tuberculin skin testing. These inmates represented 36% of the target population of inmates incarcerated for more than 10 days. Of tuberculin skin tests placed, 10 110 (74%) were read; 431 (4.3%) of these were reported as yielding positive 19 October 1999 Figure 2. Cases of active tuberculosis disease diagnosed in guards (top) and inmates (bottom) from the Memphis jail, 1 January 1995 through 31 December 1997, by quarter in which disease was diagnosed. White bars indicate persons with isolates with DNA fingerprints matching the predominant strain in the jail, striped bars indicate those with a different DNA fingerprint, and black bars indicate culture-negative persons. • Annals of Internal Medicine • Volume 131 • Number 8 559 Table. Characteristics of the 38 Inmates in Whom Tuberculosis Was Diagnosed in the Memphis County Jail, 1 January 1995 to 31 December 1997 Characteristic Value Median age (range), y Men, n (%) Ethnicity, n (%) Black Non-Hispanic white Born in the United States, n (%) Median duration of continuous incarceration in the jail before diagnosis (range), d HIV status, n (%) Positive Negative Unknown Site of disease, n (%) Pulmonary Nonpulmonary Findings on chest radiography, n (%) Cavitary Infiltrate/densities Adenopathy Effusion Normal Laboratory results, n (%) Sputum smear–positive Culture-positive DNA fingerprint matched predominant jail strain (24 isolates tested) Drug-resistant organism 34 (19 –52) 38 (100) 37 (97) 1 (3) 38 (100) 138 (10 – 800) 5 (13) 27 (71) 6 (16) 34 (89) 4 (11) 4 (11) 22 (58) 8 (21) 2 (5) 2 (5) 11 (29) 24 (63) 16 (67) 0 had identical DNA fingerprints, with 11 matching bands on IS-6110 restriction fragment length polymorphism testing (Figure 3). Among the 8 inmates with fingerprints that did not match the predominant strain, 3 had isolates with an identical restriction fragment length polymorphism pattern with 12 bands; thus, 19 (79%) of 24 culture-positive inmates had isolates that matched those of two or more other inmates. Restriction fragment length polymorphism testing was done on 43 isolates from randomly selected community cases from the same city as the inmate cases. Of these, 28 (65%) were from men, 30 (70%) were from black persons, and 19 (44%) were from black men. Only 6 (14%) of 43 isolates from persons with active tuberculosis in the community had the 11-band epidemic pattern; 4 of these persons had been previously incarcerated in the jail. Culture-positive cases among inmates were significantly more likely to have isolates with a DNA fingerprint matching the predominant strain in the jail than were cases among persons in the community (P ⬍ 0.001). All M. tuberculosis isolates from culture-positive inmates were susceptible to all drugs tested. Of the 19 culture-positive inmates with isolates matching those of other inmates, 3 (16%) were housed in the same unit with another inmate who had an identical isolate during their presumed infectious period. Ten (53%) had been housed on the same floor as another inmate with a matching isolate during their infectious period. All inmates with 560 19 October 1999 • Annals of Internal Medicine • active tuberculosis had been incarcerated in the jail at the same time as other infected inmates during their potential infectious period. The periods of incarceration of the 16 inmates with the predominant M. tuberculosis strain are shown in Figure 4. Guard Tuberculosis Cases Active tuberculosis was diagnosed in five jail staff members during the 3-year period; all were guards. Two guards were culture-positive, and both had strains identical to the predominant inmate strain. Guards are frequently rotated to various duty stations, and all have direct contact with inmates. Both of the culture-positive guards were employed during periods overlapping the incarcerations of several inmates with matching isolates (Figure 4). Of the five guards with tuberculosis, four (80%) were female and all were black, with a mean age of 34 years and a mean length of employment of 47 months. All lived in the same city in which the jail is located. Of approximately 790 jailors at the facility, 56% were female, and 90% were black; the mean age was 38 years, and the mean length of employment was 79 Figure 3. Autoradiograph of IS-6110 restriction fragment length polymorphism patterns of Mycobacterium tuberculosis isolates. Lanes 1 and 11 are standards. Lanes 4 through 7 and 9 are from inmates whose isolates had the 11-band pattern matching that of 12 inmates and two guards. Lanes 2 and 3 are from two of three inmates with an identical 12-band pattern. Lane 8 is from an inmate whose isolate did not match those of other jail cases, and lane 10 is from a person living in the community. Volume 131 • Number 8 months. None of these characteristics differed significantly between the group with tuberculosis and that without. The results of annual tuberculin skin test screening of jail staff were available for 2 of the years in this study period. In October 1996, 706 staff were evaluated; 128 (18.1%) had previously had a positive test result, and 19 (2.7%) were reported with newly positive tuberculin skin test results. In October 1997, 686 jailors were evaluated; 537 (78%) had a tuberculin skin test reading of 0 mm, 140 (20%) had previously had a positive test result, and 8 (1.2%) had a skin test that had converted to 10 mm or greater since the preceding year. Those with a negative tuberculin skin test result had been employed at the jail for an average of 75 months, compared with 92 months for those with a positive test result and 94 months for convertors. All staff with documented conversions in 1997 were guards. Figure 4. Periods of incarceration, during the 2 years before diagnosis, of the 16 jail inmates (black lines) whose Mycobacterium tuberculosis isolates had the predominant DNA fingerprint and periods of employment of the two jail guards (striped lines) with the same strain. Boxes indicate periods in the jail when persons were presumably infectious. Inmate P was not considered infectious. Discussion Patient Interviews Several lines of evidence suggest that M. tuberculosis was transmitted in this jail. Thirty-eight cases of active tuberculosis were diagnosed in inmates during the 3-year period. Of the culture-positive inmate cases, 67% had isolates with a single identical fingerprint pattern on restriction fragment length polymorphism analysis; only 14% of isolates from persons with active tuberculosis in the community had this pattern. Of culture-positive inmates, 79% had isolates matching those of two or more other inmate cases. Inmates with active tuberculosis had median lengths of incarceration significantly longer than those of the overall jail population and had been incarcerated a median of 15 times. No common exposures among inmates with tuberculosis outside the jail could be identified. In addition, five guards were given a diagnosis of active tuberculosis during this period, and both guards with positive cultures had isolates identical to the predominant inmate strain. Molecular epidemiology played an important role in recognizing and defining this outbreak. Restriction fragment length polymorphism clustering is reported to be highly predictive for epidemiologic connections among patients in large, crowded, or shifting populations and in settings such as prisons and shelters (24). Additional testing of the predominant inmate strain for polymorphism in the genes encoding catalase-peroxidase and the A subunit of gyrase identified the strain as belonging to one of two genotypic groups found to be associated with large case clusters (25). The use of DNA fingerprinting to complement traditional epidemiologic techniques may be particularly useful in jails, where the barriers to other methods of investigation are higher than in many other settings. Of the 38 inmates with active tuberculosis diagnosed since 1 January 1995, 15 (39%) could be contacted. All 15 agreed to be interviewed. Nine were inmates with isolates matching the predominant strain, 4 had a different strain, and 2 were culture negative. No common gathering areas (for example, residences, workplaces, hotels, social service agencies, parks, clubs, bars, and street corners) or contacts outside the jail were identified by any two inmates. However, 14 (93%) of the inmates had participated in visitation or in chapel, library, or gym visits while in the jail. Health Department and Jail Registry Cross-Matching Cross-matching of the health department tuberculosis case registry and jail records indicated that, since 1995, 43% of persons with tuberculosis reported in Memphis had been incarcerated in the jail at some time before their diagnosis. Intervention When this outbreak was recognized, the local health department worked with the jail to institute a more thorough screening procedure during intake and to encourage referral of inmates suspected of having tuberculosis to the health department tuberculosis clinic for evaluation and treatment. The jail also made efforts to improve their rates of tuberculin skin testing and is preparing to place ultraviolet lights in high-traffic areas in the facility. To promptly recognize potential clusters of related cases, the health department now routinely does restriction fragment length polymorphism testing of isolates from persons with tuberculosis who have recently been incarcerated. 19 October 1999 • Annals of Internal Medicine • Volume 131 • Number 8 561 Fortunately, no cases of drug-resistant tuberculosis were reported from this jail during the 3-year investigation period. In an era when susceptibility testing of M. tuberculosis isolates is routine, multidrug resistance is a readily available marker that captures attention and may lead to recognition of outbreaks in defined populations (such as prisoners). This investigation suggests that transmission of drug-susceptible tuberculosis may occur in correctional facilities for prolonged periods before recognition, for lack of a clear marker of relatedness between cases. The incidence of tuberculosis in inmates during the 3-year study period was 274 per 100 000 persons. In striking contrast, the rate of active tuberculosis in the United States in 1996 was 8 per 100 000 persons; in Tennessee, the rate was 10 per 100 000 persons, and in Memphis, the rate was 13 per 100 000 persons (1). In 1996, black men 25 to 44 years of age in the United States had a case rate of 41 per 100 000 persons (1), and black men in this age group in Memphis had a tuberculosis incidence of 61 per 100 000 persons, less than one fourth of the rate in the jail. This analysis includes only inmates in whom tuberculosis was diagnosed while they were incarcerated or within 3 weeks of discharge from the jail. Although the group includes persons who acquired tuberculosis before entering the facility, many others who may have been infected in the jail but were not given a diagnosis until after release are excluded. The number of persons exposed in the jail but given a diagnosis months or years later cannot be determined but could be substantial. Our investigation highlights the difficulties in investigating and controlling tuberculosis in jails. Despite a strong epidemiologic link of cases with the jail, even an extensive, retrospective analysis of records could not identify specific person-to-person lines of transmission among most of the inmates. As demonstrated in Figure 4, overlapping periods of incarceration could explain transmission among numerous inmates and guards infected with the same strain of M. tuberculosis. Even in the confines of a jail, high turnover and frequent movement of inmates provide opportunities for contacts that cannot be completely elucidated by routine investigation. Urban jails housing large numbers of inmates may play a substantial role in the epidemiology of tuberculosis in the surrounding community. Jail populations have a high prevalence of risk factors for communicable diseases. The potential for transfer of tuberculosis both into and out of such facilities is great. A large proportion (43%) of persons with tuberculosis in Memphis have had previous contact with the jail; although this does not imply that their disease was a result of their incarceration, 562 19 October 1999 • Annals of Internal Medicine • it does suggest that jails may provide a unique opportunity to screen and treat a population at high risk that might not otherwise have access to medical care. This could help limit the disease in the community as well as in the jail. Such interventions would require a substantial shift in priorities and application of resources. Correctional facilities have a mandate to safely separate inmates from society and have not traditionally been considered key participants in public health interventions. Successful models that integrate public health systems and health care in correctional facilities are being developed (26). Screening inmates for active tuberculosis at the time of admission and avoiding introduction of infectious persons into the jail population are critical to the prevention of the spread of disease within jails. Many prisons have programs that include placing a tuberculin skin test on all incoming inmates and repeating the tuberculin skin test annually. Prisons have a relative advantage in that inmates will be in the facility for extended periods. In contrast, jails present unique logistic obstacles to screening; many inmates are processed in and out daily, and many stay for very short periods. While inmates are in the jail, they are moved frequently and are often in court or difficult to find, making the reading of tuberculin skin tests challenging at best. This difficulty is evidenced by the low number of inmates screened successfully with tuberculin skin tests in this investigation and others (10, 27). Furthermore, the sensitivity of the tuberculin skin test in screening for active tuberculosis is not high; 10% to 25% of persons with active disease will have a negative skin test result (28). Screening for symptoms of tuberculosis is recommended as the first line of defense in situations with a high prevalence of tuberculous disease (9, 28). All inmates should have a systematic interview to determine the presence of symptoms of active disease and whether they have had tuberculosis before or have been told to take medications for this disease. If symptoms such as cough lasting longer than 2 weeks, hemoptysis, chest pain, weight loss, fever, or night sweats are present, inmates should be isolated pending prompt evaluation. Screening inmates for active tuberculosis with chest radiographs may also be appropriate in jails with a high prevalence of disease or risk factors for tuberculosis among inmates (9, 10, 27–29). The availability of new highspeed, low-dose miniature chest radiograph technology makes this a safer and more practical option than in the past. Several jail systems are using universal chest radiograph screening for all jail admissions (30). Routine cross-matching of incoming inmates with local tuberculosis registries may also be useful in Volume 131 • Number 8 some settings to identify persons with histories of incompletely treated disease or other risk factors requiring follow-up. In addition, jail staff should be educated about signs and symptoms of tuberculosis and encouraged to facilitate prompt evaluation of inmates suspected of having the disease. Reduction of crowding (31), appropriate use of preventive therapy, and use of high-efficiency particulate air filtration and ultraviolet germicidal irradiation in high-risk areas can also help control tuberculosis in correctional facilities (9, 28, 32). Control of tuberculosis in jails and prisons should be an integral part of interventions directed toward eliminating the disease in a community. Cooperation between jail medical staff and public health tuberculosis programs is critical in ensuring appropriate treatment and follow-up of patients as they move between correctional facilities and the community. 2. Hutton MD, Cauthen GM, Bloch AB. Results of a 29-state survey of tuberculosis in nursing homes and correctional facilities. Public Health Rep. 1993;108:305-14. 3. Valway SE, Greifinger RB, Papania M, Kilburn JO, Woodley C, DiFerdinando GT, et al. Multidrug-resistant tuberculosis in the New York State prison system, 1990-1991. J Infect Dis. 1994;170:151-6. 4. Braun MM, Truman BI, Maguire B, DiFerdinando GT Jr, Wormser G, Broaddus R, et al. Increasing incidence of tuberculosis in a prison inmate population. Association with HIV infection. JAMA. 1989;261:393-7. 5. Stead WW. Undetected tuberculosis in prison. Source of infection for community at large. JAMA. 1978;240:2544-7. 6. Bergmire-Sweat D, Barnett BJ, Harris SL, Taylor JP, Mazurek GH, Reddy V. Tuberculosis outbreak in a Texas prison, 1994. Epidemiol Infect. 1996;117:485-92. 7. Koo DT, Baron RC, Rutherford GW. Transmission of Mycobacterium tuberculosis in a California state prison. Am J Public Health. 1991;87:279-82. 8. Fountain FF Jr. Tuberculosis in Shelby County and Tennessee correctional facilities. Tenn Med. 1997;90:138-40. 9. Prevention and control of tuberculosis in correctional facilities: recommendations of the Advisory Council for the Elimination of Tuberculosis. MMWR Morb Mortal Wkly Rep. 1996;45(RR-8):1-26. 10. Skolnick AA. Correction facility TB rates soar; some jails bring back chest roentgenograms [News]. JAMA. 1992;268:3175-6. 11. Abeles H, Feibes H, Mandel E, Girard JA. The large city prison—a reservoir of tuberculosis. Tuberculosis control among sentenced male prisoners in New York City. Am Rev Respir Dis. 1970;101:706-9. 12. Snider DE Jr, Hutton MD. Tuberculosis in correctional institutions. JAMA. 1989;261:436-7. 13. Bellin EY, Fletcher DD, Safyer SM. Association of tuberculosis infection with increased time in or admission to the New York City jail system. JAMA. 1993;269:2228-31. 14. Pelletier AR, DiFerdinando GT Jr, Greenberg AG, Sosin DM, Jones WD Jr, Bloch AB, et al. Tuberculosis in a correctional facility. Arch Intern Med. 1993;153:2692-5. 15. Glaser JB, Greifinger RB. Correctional health care: a public health opportunity. Ann Intern Med. 1993;118:139-45. 16. Bureau of Justice Statistics. Jails and jail inmates 1993-1994; census of jails and annual survey of jails. In: BJS Bulletin. Washington, DC: Department of Justice; 1995. 17. Bureau of Justice Statistics. Profile of Jail Inmates 1996. Washington, DC: Department of Justice, Bureau of Justice Statistics, National Center for Justice Statistics; 1998. 18. Tuberculosis transmission in a state correctional institution—California, 19901991. MMWR Morb Mortal Wkly Rep. 1992;41:927-9. 19. Valway SE, Richards SB, Kovacovich J, Greifinger RB, Crawford JT, Dooley SW. Outbreak of multi-drug-resistant tuberculosis in a New York State prison, 1991. Am J Epidemiol. 1994;140:113-22. 20. King L, Geis G. Tuberculosis transmission in a large urban jail. JAMA. 1977; 237:791-2. 21. Case definitions for infectious conditions under public health surveillance. MMWR Morb Mortal Wkly Rep. 1997;46(RR-10):1-55. 22. Cave MD, Eisenach KD, McDermott PF, Bates JH, Crawford JT. IS6110: conservation of sequence in the Mycobacterium tuberculosis complex and its utilization in DNA fingerprinting. Mol Cell Probes. 1991;5:73-80. 23. Dean AD, Dean JQ, Coulombier D, Brendel KA, Smith DC, Burton AH, et al. Epi Info, Version 6: A Word Processing, Database and Statistics Program for Epidemiology on Microcomputers. Atlanta: Centers for Disease Control and Prevention; 1994. 24. Braden CR, Templeton GL, Cave MD, Valway S, Onorato IM, Castro KG, et al. Interpretation of restriction fragment length polymorphism analysis of Mycobacterium tuberculosis isolates from a state with a large rural population. J Infect Dis. 1997;175:1446-52. 25. Sreevatsan S, Pan X, Stockbauer KE, Connell ND, Kreiswirth BN, Whittam TS, et al. Restricted structural gene polymorphism in the Mycobacterium tuberculosis complex indicates evolutionarily recent global dissemination. Proc Nat Acad Sci U S A. 1997;94:9869-74. 26. Conklin TJ, Lincoln T, Flanigan TP. A public health model to connect correctional health care with communities. Am J Public Health. 1998;88: 1249-50. 27. Puissis M, Feinglass J, Lidow E, Mansour M. Radiographic screening for tuberculosis in a large urban county jail. Public Health Rep. 1996;111:330-4. 28. Controlling TB in Correctional Facilities. Atlanta: Centers for Disease Control and Prevention; 1995. 29. Layton MC, Henning KJ, Alexander TA, Gooding AL, Reid C, Heman BM, et al. Universal radiographic screening for tuberculosis among inmates upon admission to jail. Am J Public Health. 1997;87:1335-7. 30. Wilcock K, Hammett TM, Widom R, Epstein J. Tuberculosis in correctional facilities, 1994-1995. Washington, DC: Department of Justice, Office of Justice Programs, National Institute of Justice; 1996. 31. MacIntyre CR, Kendig N, Kummer L, Birago S, Graham NM. Impact of tuberculosis control measures and crowding on the incidence of tuberculous infection in Maryland prisons. Clin Infect Dis. 1997;24:1060-7. 32. Hammett TM, Harvey S. Tuberculosis in Correctional Facilities. Washington, DC: Department of Justice, Office of Justice Programs, National Institute of Justice; 1994. Presented in part at the 36th Annual Meeting of the Infectious Diseases Society of America, Denver, Colorado, 12 to 15 November 1998. From the Centers for Disease Control and Prevention, Atlanta, Georgia; and the Tennessee Department of Health and Vanderbilt University School of Medicine, Nashville, Tennessee. Acknowledgments: The authors thank Donna Hurst and William L. Moore, MD, of the Tennessee Department of Health; David Crowder and Gail Grant at the Centers for Disease Control and Prevention; Yvonne Madlock, Martha Woloshyn, RN, Linda Hamer, RN, Harold Brown, Francis Fountain, MD, and the staffs of the Memphis/Shelby County Health Department, Correctional Medical Services, Inc., the Memphis/Shelby County Criminal Justice Center, and the Shelby County Correctional Center for assistance with the investigation; Dr. James Musser, Baylor College of Medicine, for genetic polymorphism testing; and Kenneth G. Castro, MD, and Laura J. Fehrs, MD, Centers for Disease Control and Prevention, for their thoughtful review of the manuscript. Requests for Reprints: Timothy F. Jones, MD, Tennessee Department of Health, CEDS, Cordell Hull Building, 4th Floor, 425 5th Avenue North, Nashville, TN 37247-5281. For reprint orders in quantities exceeding 100, please contact Barbara Hudson, Reprints Coordinator; phone, 215-351-2657; e-mail, bhudson@mail .acponline.org. Current Author Addresses: Drs. Jones and Craig: Tennessee Department of Health, CEDS, Cordell Hull Building, 4th Floor, 425 5th Avenue North, Nashville, TN 37247-5281. Dr. Valway: Division of Tuberculosis Elimination, National Center for HIV/STD/TB Prevention, Centers for Disease Control and Prevention, Mailstop E-10, 1600 Clifton Road, NE, Atlanta, GA 30333. Dr. Woodley: Division of Bacterial and Mycotic Diseases, National Center for Infectious Diseases, Centers for Disease Control and Prevention, Mailstop F-08, 1600 Clifton Road, NE, Atlanta, GA 30333. Dr. Schaffner: Departments of Medicine and Preventive Medicine, A1124 Medical Center North, Vanderbilt University School of Medicine, Nashville, TN 37232-2637. References 1. Reported Tuberculosis in the United States. Atlanta: Centers for Disease Control and Prevention; 1997. 19 October 1999 • Annals of Internal Medicine • Volume 131 • Number 8 563