Human Tissue Disposal Form Project Details
advertisement

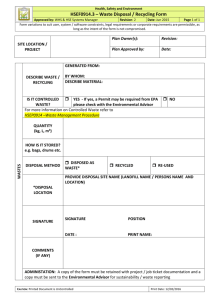
Human Tissue Disposal Form To be completed by the Lead Investigator Project Details Project Number Ethical Approval Number (if applicable) Project or sample collection title Lead Investigator or Person Responsible for the samples Date(s) samples acquired Disposal Details Proposed date of disposal Type of sample (e.g. urine; plasma)Type and amount of human samples for disposal Quantity of samples Tissue sample numbers (i.e. unique identifiers) Reason for disposal (include reference to consent , wishes of donor, or agreement on sample acquisition in e.g. MTA, as appropriate) Method and location of disposal I confirm that the information above is accurate and complete and that Tissue Register will be fully updated following completion of the disposal of the human samples: Signature of Lead Investigator:......................................................... Date:.......................... I authorise disposal of these human samples: Signature of Designated Individual:......................................................... Date:..........................