CHILDREN AND FAMILIES
EDUCATION AND THE ARTS
The RAND Corporation is a nonprofit institution that helps improve policy and
decisionmaking through research and analysis.
ENERGY AND ENVIRONMENT
HEALTH AND HEALTH CARE
INFRASTRUCTURE AND
TRANSPORTATION
This electronic document was made available from www.rand.org as a public service
of the RAND Corporation.
INTERNATIONAL AFFAIRS
LAW AND BUSINESS
Skip all front matter: Jump to Page 16
NATIONAL SECURITY
POPULATION AND AGING
PUBLIC SAFETY
SCIENCE AND TECHNOLOGY
TERRORISM AND
HOMELAND SECURITY
Support RAND
Browse Reports & Bookstore
Make a charitable contribution
For More Information
Visit RAND at www.rand.org
Explore the Pardee RAND Graduate School
View document details
Limited Electronic Distribution Rights
This document and trademark(s) contained herein are protected by law as indicated in a notice appearing
later in this work. This electronic representation of RAND intellectual property is provided for noncommercial use only. Unauthorized posting of RAND electronic documents to a non-RAND website is
prohibited. RAND electronic documents are protected under copyright law. Permission is required from
RAND to reproduce, or reuse in another form, any of our research documents for commercial use. For
information on reprint and linking permissions, please see RAND Permissions.
This product is part of the Pardee RAND Graduate School (PRGS) dissertation series.
PRGS dissertations are produced by graduate fellows of the Pardee RAND Graduate
School, the world’s leading producer of Ph.D.’s in policy analysis. The dissertation has
been supervised, reviewed, and approved by the graduate fellow’s faculty committee.
Where in Social and
Sexual Networks Should
HIV Interventions Target?
Identifying Similarities in Social
Contexts Characteristics and Mutual
Disclosure Behaviors of HIV Status
and MSM Identity Across Social
and Sexual Networks
Alexis K. Huynh
This document was submitted as a dissertation in August 2011 in partial fulfillment
of the requirements of the doctoral degree in public policy analysis at the Pardee
RAND Graduate School. The faculty committee that supervised and approved the
dissertation consisted of Harold Green, Jr. (Chair), Gery Ryan, and Jennifer Sayles.
PARDEE RAND GRADUATE SCHOOL
The Pardee RAND Graduate School dissertation series reproduces dissertations that
have been approved by the student’s dissertation committee.
The RAND Corporation is a nonprofit institution that helps improve policy and
decisionmaking through research and analysis. RAND’s publications do not necessarily
reflect the opinions of its research clients and sponsors.
R® is a registered trademark.
All rights reserved. No part of this book may be reproduced in any form by any
electronic or mechanical means (including photocopying, recording, or information
storage and retrieval) without permission in writing from RAND.
Published 2011 by the RAND Corporation
1776 Main Street, P.O. Box 2138, Santa Monica, CA 90407-2138
1200 South Hayes Street, Arlington, VA 22202-5050
4570 Fifth Avenue, Suite 600, Pittsburgh, PA 15213-2665
RAND URL: http://www.rand.org
To order RAND documents or to obtain additional information, contact
Distribution Services: Telephone: (310) 451-7002;
Fax: (310) 451-6915; Email: order@rand.org
Wher
W re In Social
S
l and Sexu
ual Ne
etwork
ks
Sho
ould HIV
H In
nterve
ention
ns Tarrget?
Iden
ntifying
g simila
arities in
i socia
al conte
exts, in
ndividua
al
chara
acteristtics and
d disclo
osure b
behavio
ors of H
HIV stattus
& MSM
M
id
dentity across
a
social and se
exual ne
etworks
s
Figure
F
1: The largest
l
referrall chain of the Brothers
B
Y Herrmanos Projectt Los Angeles C
County site
Alexis K. Huyn
nh
Pard
dee RAND
D Gradua
ate Schoo
ol
Disserta
ation Deffense
Aug
gust 2011
1
iii
Table of Contents Acknowledgements ................................................................................................................... vii Abstract......................................................................................................................................... ix Chapter 1: Introduction and Motivation .................................................................................. 1 Section 1.1: Significance .......................................................................................................... 1 Section 1.2: Specific Aims........................................................................................................ 2 Section 1.3: Organization of the Research ............................................................................ 6 Chapter 2: A Review of the Literature: Disclosure of HIV Status and MSM Identity ....... 8 Section 2.1: Framework ........................................................................................................... 8 Section 2.2: Social Contexts and Social Networks ............................................................. 10 Section 2.3: Disclosure of HIV Status and MSM Identity ................................................. 12 Section 2.4: Emotional Closeness ......................................................................................... 14 Section 2.5: Social Support .................................................................................................... 15 Section 2.6: Community Integration.................................................................................... 16 Section 2.7: Integration of Social Context Characteristics and Disclosure Behaviors of HIV Status and MSM Identity .............................................................................................. 17 Chapter 3: Data Description and Methods ............................................................................. 19 Section 3.1: Research Design ................................................................................................ 19 Section 3.1.a: Research Sites .............................................................................................. 19 Section 3.1.b: Sampling Frame and Recruitment ........................................................... 20 Section 3.2: Methods of Data Collection: Structured Interviews and Network Data .. 23 Section 3.3: Measures ............................................................................................................. 25 Section 3.4: Analysis Plan ..................................................................................................... 28 Section 3.5: Analytic Strategy ............................................................................................... 31 Chapter 4: Respondents’ Social Contexts and Individual Characteristics......................... 35 Section 4.1: Description of Respondents’ Social Contexts and Individual Characteristics ........................................................................................................................ 35 Section 4.2: Associations between Social Contexts and Individual Characteristics ..... 40 Section 4.3: Respondent and Social Contexts Characteristics Homophily .................... 49 Section 4.4: Discussion and Conclusion .............................................................................. 52 Chapter 5: Respondents’ Disclosure Behaviors of HIV Status and MSM Identity........... 55 Section 5.1: Rates of HIV Status and MSM Identity Disclosure ...................................... 55 Section 5.2: Associations between Disclosure Behaviors and Social Contexts and Individual Characteristics ..................................................................................................... 57 Section 5.3: Homophily in HIV Status and MSM Identity Disclosures.......................... 72 Section 5.4: Discussion and Conclusion .............................................................................. 75 Chapter 6: Dyadic Analyses: Mutual Disclosure of HIV Status and MSM Identity within Referral Pairs .............................................................................................................................. 81 v
Section 6.1: Homophily in Disclosure of HIV Status‐Mutual Disclosure to Specific Members in Sexual and Social Networks ........................................................................... 82 Section 6.2: Discussion and Conclusion .............................................................................. 90 Chapter 7: Conclusions and Discussion ................................................................................. 92 Section 7.1: Limitations ......................................................................................................... 92 Section 7.2: Summary of Findings and Implications ........................................................ 93 References ................................................................................................................................... 99 vi
Acknowledgements It has been a long road and at times seemingly unending. If asked to describe it to someone contemplating whether to embark on this journey, I would say it is a process of equal parts acquiring intellectual rigor and character building. In it all, I have been more than blessed to be working with my dissertation committee members: Hank Green, Gery Ryan, and Jennifer Sayles. They are each exemplars of the brightest and most innovative minds working on health policy issues confronting us today. I would like to thank Hank in particular, who for the better part of the last three years, have indulged me in my intense curiosity and took the time out weekly to teach me about the methods of social network analysis and the craft of research. I learn from your example. I would like to thank Trista Bingham for her generosity in entrusting me with the data set from the Brothers Y Hermanos project. I thank Lisa Klautzer for her committed and consistent efforts in providing feedback, critique, and a pair of caring eyes over the pages of my dissertation. I thank Lisa Husniyyah Owens and Sayo Morinaga for their enduring friendships and support. I thank my parents and my aunt (Di Huong) for teaching me about the dignity of work. Your grace inspires me. This dissertation was supported by the Agency for Healthcare Research and Quality (AHRQ) award for Health Services Dissertation (R36). I, the author, am solely responsible for the content of the dissertation. vii
Abstract Background: Disclosure of HIV status and men who have sex with men (MSM) identity both have public health significance (as a strategy to prevent further transmission by those infected with HIV) and personal health benefits for HIV‐positive individuals (such as greater treatment adherence, greater social support, higher self‐esteem, and lower levels of depression). Understanding where similarities in social context characteristics and disclosure behaviors lie in respondents’ various sexual and social networks has important implications for developing new and innovative HIV interventions. Methods: Data come from the Brothers Y Hermanos project and consist of cross‐sectional quantitative structured interviews with 565 Latino MSM in Los Angeles County. Measures of interest included individual characteristics (age, SES, ethnic‐identity, HIV‐risk characteristics), social context characteristics (emotional closeness, social support, size of MSM networks, community integration), and disclosure behaviors of HIV status and MSM identity. Network data were taken from the respondent‐driven sampling (RDS) recruitment framework: a referral pair was composed of a referral ‘source’ who asked someone they knew to be a part of the study and a referral ‘target’ who agreed and subsequently participated in the study. I utilized traditional quantitative analyses, including descriptive statistics, linear and logistic regression analyses in addition to more recently developed dyadic data analysis approaches to examine disclosure behaviors at the level of the individual respondent and at the level of the referral pair. Results: Respondents who referred each other to the Brothers Y Hermanos project were highly similar with respect to their individual characteristics and the social contexts in which they were embedded. Furthermore, referral pairs also mutually disclosed their HIV status and MSM identity to sexual and social network members. However, disclosure of HIV status and MSM identity remained highly individualized behaviors, dependent on the target of disclosure (sexual partners, parents, siblings, friends, or community members), and the respondents’ individual characteristics that embedded them in social contexts that facilitated or impeded disclosure of HIV status and MSM identity. Similarities in disclosure did seem to be impacted by features of their community, as measured by scales of community integration. Discussion: This study shows that the respondents in the Brothers Y Hermanos study were highly similar to each other across demographic characteristics, disclosure behaviors, but homophily was not associated with mutual disclosure. Interventions should address the possible barriers against disclosure (such as stigma in the Latino community and the sense of isolation that Latino MSM may feel) and take advantage of the facilitators (closeness to and social support from sexual and social network members). Furthermore, interventions should target specifically the Latino MSM community, given the role that community integration seems to play in disclosure behaviors. As there might have been possible influence within referral pairs with regards to their disclosure behaviors at the community level, interventions should incorporate network components to shape respondents’ community norms. ix
Chapter 1: Introduction and Motivation Section 1.1: Significance Understanding where similarities in social context characteristics and disclosure behaviors lie in individuals’ sexual and social networks has important implications for developing new and innovative network‐based public health interventions. This research answers questions regarding where the sources of support are in individuals’ social contexts that promote disclosure of HIV status and of men who have sex with men (MSM) identity. For example, are individuals who are emotionally closer to their family members better able to disclose their HIV status or MSM identity? Or is the role of integration in the Latino gay community more important than other social context characteristics in determining disclosure of MSM identity to friends and community members? Further, individuals exert influence and are influenced by members of their networks such as sexual partners, friends and acquaintances. Do friends who share similar social contexts also disclose their HIV status to their respective parents? Do sexual partners also disclose their MSM identity to their friends? The answers to these questions help determine which social networks and where within those networks interventions should target to promote disclosure of HIV status and MSM identity, which in turn may be associated with reduced risk of HIV transmission and improved health outcomes. This research is innovative in that it uses an ecological framework that examines the relational aspects of disclosure behaviors and explicitly uses social network analysis 1
(SNA) techniques to examine and understand the social contexts in which individuals are embedded. Section 1.2: Specific Aims Historically, network‐based interventions that aim to combat HIV/AIDS have targeted sexual partners.1,2 Furthermore, HIV‐related network based interventions have focused on risk reduction strategies such as engaging intravenous drug users (IDUs) in harm reduction methods,2 decreasing unprotected sexual intercourse and increasing condom use among high‐risk individuals.3‐5 However, it is equally important to examine aspects central to the lives of individuals at risk for transmitting or contracting HIV such as sexual risk behaviors, engagement and retention in HIV care, adherence to treatment and disclosure of HIV status and MSM identity. It might be that these individuals are embedded in similar social contexts that place them at risk for or reduce their risk of contracting HIV. Furthermore, these individuals might be more similar to their friends than their sexual partners in aspects related to HIV risk. In other words, the mode of HIV transmission might not be the same as the mode of information transmission or behavior influence. As such, network‐based interventions might be more effective if they target friendship networks rather than sexual networks and address more social aspects than risk reduction. Homophily, literally translated as love of the same, means that individuals sharing similar characteristics appear in relationships more often with each other than 2
with individuals with dissimilar characteristics.6 We know that individuals exert influence and are influenced by others who have similar individual, interpersonal, and community‐level, and behavioral characteristics. Consequently, homophily has important implications for network‐based interventions. The questions of where homophily exists and what role it plays in influencing individual health behaviors can help determine which type of networks to target to encourage individual behavioral change. Disclosure of HIV status has both public health significance and personal health benefits. The Centers for Disease Control and Prevention (CDC) recommends disclosure of HIV status as one of the strategies to prevent further transmission by those infected with HIV.7 One study found that individuals who disclosed their HIV status to their partners engaged in fewer acts of unprotected anal intercourse with their HIV‐negative partners.8 Another study found through mathematical modeling analysis that disclosure of HIV status can potentially reduce HIV transmission by 17.9% to 40.6%.9 Disclosure of HIV status also has health benefits for HIV‐positive individuals such as greater treatment adherence,10 greater social support, higher self‐esteem, and lower levels of depression.11 Disclosure of MSM identity is associated with HIV status disclosure8,12 and thus, can garner similar public and personal health benefits. Conversely, failure to disclose MSM identity is associated with deleterious effects such 3
as more severe HIV disease progression, greater depressive symptoms, and less social support.13 Hispanic men are disproportionately burdened by the HIV/AIDS epidemic. Hispanic men make up 32% of the reported 51,250 cumulative AIDS cases among men in Los Angeles County as of December 2009.14 Among Hispanic men, male‐to‐male sexual contact represents the primary mode of HIV transmission, making up 69% of the cumulative AIDS cases ever reported, and heterosexual contact makes up 3%.14 These epidemiological profiles suggest that Hispanic men might be at particularly high risk of transmitting HIV to or contracting HIV from their male and female sex partners. The objective of this research is to understand the effects of individual and social contexts characteristics on disclosure behaviors of HIV status and MSM identity and to understand the impact of similarities in the social context on similarities in disclosure behaviors across friendship and sexual networks. The data for the research came from a cross‐sectional study of Latino men in Los Angeles County as part of the Brothers Y Hermanos project. The proposed research has the following three aims: 1. Identify and describe respondents social contexts (e.g., emotional closeness, social support, size of overall and Latino MSM networks and integration in the Latino and/or communities), including how respondents’ social contexts may 4
vary by individual characteristics such as age, income, education, place of birth, acculturation level, sexual orientation, and reported HIV status. 2. Identify and describe HIV status and MSM identity disclosure patterns, including how such patterns may vary by respondents’ social contexts (e.g., emotional closeness, social support, size of overall and Latino MSM networks and integration in the Latino and/or gay communities) and individual characteristics such as age, income, education, place of birth, acculturation level, sexual orientation, and reported HIV status. 3. Investigate the associations between similarities in social contexts (e.g., in emotional closeness, social support, size of overall and Latino MSM networks and integration in the Latino and/or gay communities) and similarities in disclosure of HIV status and MSM identity. This research is innovative in that it seeks to understand disclosure behaviors of HIV status and MSM identity from the point of view of the social contexts and the relationships in which individuals are embedded. This research could provide insight for (1) identifying where sources of support exist in social contexts that enable and encourage individuals to disclose their HIV status and/or MSM identity, (2) where similarities exist across friendship and sexual networks that enable similar disclosure behaviors of HIV status and/or MSM identity, and (3) develop interventions based on a relational perspective that promote disclosure. 5
Section 1.3: Organization of the Research Having described the significance and specific aims of the research in this chapter, I will present a review of the literature on HIV status and MSM identity disclosure in Chapter 2. First, I will lay out a framework of disclosure behaviors of HIV status and MSM identity, which has been shown to be determined by individual and social context characteristics. Second, I will describe how social relationships can influence individual disclosure behaviors and how SNA is suited for studies that use respondent driven sampling (RDS) to recruit respondents. Then, I will review the literature on disclosure behaviors and how they are related to emotional closeness, social support, and community integration. Lastly, I will present an integrated review of the literature on social contexts characteristics and disclosure behaviors. In Chapter 3, I will describe the data and methods. First, I will discuss the research design, including the research sites, and the sampling frame and recruitment of the Brothers Y Hermanos study. Next, I will describe the methods of data collection for the structured interviews and how network data was constructed based on the RDS recruitment framework. Third, I will describe the measures and, finally, I will discuss the analysis plan and analytic strategy. In Chapter 4, I will describe the how the social contexts characteristics may vary by respondents’ individual characteristics. First, I will describe the respondents’ individual and social context characteristics. Then, I will discuss the associations 6
between social context and individual characteristics, including how respondents’ emotional closeness, social support, size of MSM networks and community integration may vary by their individual characteristics. Third, I will examine referral pairs’ homophily with respect to their individual and social context characteristics. Then, I will end with a discussion and conclusion section. In Chapter 5, I will examine the respondents’ HIV status and MSM identity disclosure behaviors. First, I will describe the rates of HIV status and MSM identity disclosure. Second, I will examine the associations between disclosure behaviors, social contexts and individual characteristics. Then, I will examine referral pairs’ homophily in HIV status and MSM identity disclosure. Last, I will discuss the findings and conclude. In Chapter 6, I will present dyadic analyses of similarity in disclosure behaviors of HIV status and MSM identity. First, I will examine the similarity in disclosures to specific members in sexual and social networks. Then, I will discuss and conclusion section. In Chapter 7, I will present the conclusions and recommendations. First, I will present a summary of the findings. Then, I will conclude with recommendations for intervention design to promote disclosure of HIV status and MSM identity among Latino MSM. 7
Chapterr 2: A Revie
ew of the L
Literature: D
Disclosure of HIV Staatus and M
MSM Identitty Section 2.1: Framew
work Figure 2. Conceptuaal Framewo
ork The Latino m
T
men who reeferred each
h other to the Brothers B
Y Hermanoss project th
hrough respond
dent driveen sampliing (RDS
S) are embedd
ded in onee another’s social nettworks and likeely exert influence on each otherr. They are frien
nds, acquain
ntances and
d sexual pa
artners. They arre likely to t have similar s
ind
dividual, in
nterpersonaal, commu
unity‐level and behavioral characteeristics and
d experiencce similar s tigmatizing
g or supportive influeences in their social conttexts that in
nfluence th
heir health behaviors. For examp
ple, individ
duals embedd
ded in conteexts that vieew positivee HIV statuss or identify
fying as meen who have sex with meen (MSM) as stigmatiizing are not n likely to
o disclose their HIV status or M
MSM identity. Converseely, individ
duals embedded in supportivee networkss are likelly to MSM identity. disclose their HIV sstatus or M
nceptual fra
amework fo
or how resp
pondents off the Brotheers Y Figure 2 preesents a con
nos Project make up each otherr’s social n
networks an
nd are inflluenced by
y one Herman
another’’s health behaviors. The Fram
mework iss an adap
ption and application
n of McLeroy
y’s Ecologiical Model for Health
h Promotio
on,15 which
h views ind
dividual heealth behaviors as deterrmined by individuall factors, in
nterpersonaal processees and prim
mary groups (family, frriends, co‐workers), institutionaal factors, communitty factors, and 8
public policy. The McLeroy Model moves away from a restricted view of health behaviors as determined by the individual alone and views health behaviors as determined by the individual and factors in his social contexts. In addition, the individual has a dynamic relationship with his social context in that he is affected by and also affects his social contexts. The McLeroy Model has the potential to provide a more accurate understanding of the causes of individual health behaviors at interrelated levels and therefore provides a range of intervention strategies for health behavior change. This research is adapted from the McLeroy Model in that it focuses on the individual factors, interpersonal processes, primary groups, and community factors and applies it to examine disclosure of HIV status and MSM identity. In Figure 2, the direction of the arrows represents the direction of influence of HIV status and MSM identity disclosure behavior, the size of the arrows represents the extent of influence, and the color of the arrows represents the type of ties between respondents. For example, it might be that respondents who were sexual partners mutually influence each other’s HIV status disclosure behaviors and the extent of that influence is large. In contrast, a respondent might influence a friend’s MSM identity disclosure of MSM identity but the direction of that influence is one‐way so that the respondent is not influenced by his co‐worker. Furthermore, the extent of this influence is relatively small. 9
Section 2.2: Social Contexts and Social Networks Social groups to which individuals belong and the relationships within those groups are important sources of influence on individual behaviors. Social network analysis (SNA) provides the quantitative tools for understanding interpersonal processes and social context characteristics associated with HIV status and MSM identity disclosure behaviors. SNA is particularly suited for studies that use RDS to recruit respondents. In RDS, respondents are asked to refer individuals that they know and who fit the eligibility criteria. Thus, respondents of RDS studies are embedded in one another’s social networks. The egocentric network approach focuses on respondents (egos) and their networks (alters) vis‐a‐vis individual and behavioral characteristics. In addition, this approach also enables the investigation of variables that describe the relationship between egos and their alters such as how emotionally close the egos feel to their alters and whether the egos have disclosed their HIV status to the alters. Dyadic analysis techniques within SNA can be used to analyze the referral pairs and accommodate the data structure that arises from the sampling by referral of RDS. Statistical analysis then can be applied to understand the relationship between the RDS referral pairs, similarities in social context factors, and disclosure of HIV status and MSM identity. Research on social networks and HIV among MSM has been limited and has focused mostly on sexual risk behaviors. However, the findings are resounding in that 10
network characteristics play a key role in risky sexual behaviors of MSM. One study found that the number of anal sex partners decreases with network density, defined as the connectedness of individuals in a social network.16 Furthermore, this study found that the number of additional oral sex partners increases with network size and decreases with increased network density.16 Another study found that having a larger male sexual network is associated with having unprotected anal or vaginal intercourse.17 Social networks also play a key role in determining network norms. One study found that low HIV risk behavior, defined as using condoms 100% of the time, is associated with perceived norms in social networks that support the use of condoms.18 Correspondingly, network based interventions have been developed to reduce risky sexual behaviors. These include intervening to reduce the likelihood of unprotected intercourse,3,4 the number of sexual partners who engage in unprotected intercourse,4 and increasing condom use.5 However, none of these studies examined the positive influences in individuals’ social networks that enable and encourage disclosure of HIV status and MSM identity. Nor have any of the studies examined the role of network members in influencing each other’s disclosure behaviors and the similarities in disclosure behaviors among network members, here defined as referral pairs. Given the structure of the survey data, SNA techniques are better suited for understanding disclosure behaviors of HIV status and MSM identity than other analytic techniques. In terms of research design, SNA, specifically dyadic analysis, allows the 11
referral pairs in RDS, rather than the individual alone, to be the unit of analysis. Furthermore, while the literature has noted the effect of social support, peer pressure and group norms on individual health behaviors, it has failed to understand the sources and extent of those influences from a relational perspective. SNA techniques overcome this limitation by providing an understanding of individual health behaviors, particularly disclosure behaviors of HIV status and MSM identity, from such a relational perspective. Section 2.3: Disclosure of HIV Status and MSM Identity Disclosure is defined as informing others of one’s own or another person’s HIV status or MSM identity.19 The literature delineates between different types and modes of disclosure: voluntary versus involuntary, and direct versus proxy. Voluntary disclosure occurs when the person who is HIV‐positive or MSM decides when, how and to whom to reveal his HIV status or MSM identity and that decision is made without coercion. Involuntary disclosure is when an individual’s HIV status is revealed without the permission of that individual. Direct disclosure is when disclosure is made in a straightforward manner. Lastly, proxy disclosure is when an individual’s HIV status is revealed indirectly or without being verbally articulated.20 This research focuses on voluntary and direct disclosure, that is, when an individual actively reveals his HIV status or his MSM identity. 12
Among MSM, reasons cited for disclosure of their HIV status to sexual partners include feelings for sexual partners, feeling responsible for partner’s health and fearing arrest.21 Conversely, reasons against disclosure to sexual partners among MSM include fear of rejection, being in denial, feeling that it’s nobody’s business, having an “it’s just sex” attitude, using drugs, and having sex in public places.21 For Latino MSM, perceived positive consequences are predictive of HIV status disclosure to casual sexual partners, close friends and family members. These reasons include “to feel honest about my life,” “to feel closer to the people” and “to get support, treatment and resources that I need”.22 Conversely, some barriers were significantly predictive against disclosure of HIV status to close friends and family members, but not to casual sex partners. For Latino MSM these include rejection, feeling of hurting others, and fear of negative effects on job situation, insurance or immigration.22 Disclosure of HIV status varies by the type of relationship between network members and the discloser. Within families, the members to whom MSM most often disclose their HIV status are mothers (67%), followed by sisters (50%), then by fathers (47%) and lastly, brothers (41%).23 However, comparing across different types of network members, MSM disclose their HIV status to friends more often than to family members, with 56% disclosing to friends compared to families at 50%.24 Among Latino MSM, 85% reported having disclosed their HIV status to their closest friends, 78% to their main male sexual partner, 37% to mothers, and 23% to fathers.11 Factors associated 13
with HIV status disclosure vary depending on to whom Latino MSM disclosed their HIV status: for mothers and fathers, more emotional closeness and whether parents are aware of respondent’s gay sexual orientation are predictive of HIV status disclosure; for close friends, only whether those friends are aware of respondents’ gay sexual orientation is predictive of HIV status disclosure.12 Previous research suggests that there is homophily in disclosure behaviors of HIV status among MSM sexual partners. In other words, individuals are more likely to disclose if their sexual partners first disclosed their HIV status to them.21 However, we do not know the extent of the similarities in disclosures among friends, acquaintances, or other types of relationships. Furthermore, we do not know if individuals are more similar to their friends and acquaintances or their sexual partners in terms of disclosure of HIV status and MSM identity. In terms of MSM disclosure, being “out” as an MSM is associated with higher likelihood of HIV status disclosure.8,12,25 However, it is unknown what motivates disclosure, the rates of disclosure and to whom MSM identity disclosure is made among Latino MSM. Section 2.4: Emotional Closeness Emotional closeness represents the strength of the bond and the trust that respondents have with their network members.12 It has been shown to be an important determinant of disclosure of HIV status12 and MSM identity.26 Emotional closeness and 14
trust were identified as reasons for disclosure of HIV status to sex partners.21,27 Furthermore, respondents who reported greater emotional closeness to their mothers and fathers are more likely to disclose their HIV status to them.12 Emotional closeness is also important in the mental health of HIV‐positive individuals such that individuals receiving support from an important person in their networks whom they were emotionally close to reported more positive mental health status compared to those having only general support or assistance.28 Section 2.5: Social Support Social support is defined as the availability of help and emotional comfort from members in individuals’ social networks.29 It is usually classified into five types of functional support: emotional, instrumental, informational, appraisal support, and social companionship. Emotional support is providing understanding and encouragement. Instrumental support or tangible support is the provision of material aid and behavioral assistance. Informational support is the offering of advice and guidance. Appraisal support is helping individuals with evaluating themselves. Lastly, social companionship is spending time in leisure activities and recreational activities.29 In contrast to the functional forms of support, structural support is the quantity of relationships such as the number of friends or relatives in individuals’ social networks and how closely those friends and relatives know each other.30 Furthermore, social support can be measured as perceived support or actual support provided, based on the 15
timing of the support given. Perceived support is based on individuals’ assessment of support available in the future while actual support is based on support received in the past.31 Social support has been shown to play a key role in disclosure behaviors of HIV status and MSM identity. One study found that friends are perceived to be more supportive than family members and are most often disclosed to about HIV status.32 Among family members, mothers and sisters are perceived as more supportive than fathers and brothers and are more often disclosed to about HIV positive status.32 Another study found that compared to Latinas, Latino MSM reported lower emotional and instrumental general support and lower HIV‐specific instrumental support.33 In addition, Latino MSM disclose their HIV status to fewer network members compared to Latinas.33 Social support also improves the physical and mental health outcomes of HIV‐positive individuals. Among gay HIV‐positive men, having frequent contact with family and high social participation slows HIV disease progression.34 The type of social support is also important. One study found that HIV‐positive Latinos rely on their health care providers for accessing and maintaining HIV‐specific care and rely on family and friends for emotional, household, and financial support.35 Section 2.6: Community Integration Community integration is defined as the extent to which individuals feel part of the various communities of which they are members.36 For Latino MSM, those 16
communities include the Latino community, the gay community, and the Latino gay community. Community integration can take many forms such as participating in Latino or gay‐specific social functions, patronizing businesses Latino or gay owned, or going to gay clubs and bars.36 Community integration enables individuals to mobilize social support in their networks to improve their physical and mental health outcomes and it could also determine their health behaviors.36 Previous studies have mostly focused on the effect of community integration on sexual risk behaviors. For example, one study found that among gay, lesbian and bisexual college students, limited involvement in gay and lesbian recreational and social activities is associated with more unprotected sex.37 Another study found that social participation with other gay men is associated with reduced risky sexual behavior among homosexual men.38 Still another study found that individuals whose primary participation in the gay community involves going to gay bars and clubs engage in more risky sexual behaviors.36 In terms of HIV status disclosure, one study found that among Latino MSM, greater involvement in the gay community is associated with less disclosure of HIV status to casual sex partners but more disclosure of HIV status to close friends.29 Section 2.7: Integration of Social Context Characteristics and Disclosure Behaviors of HIV Status and MSM Identity 17
Disclosure behaviors are embedded in social relationships and are thus related to social context characteristics such as reported emotional closeness, types of functional social support and structural support, and community integration. In addition, these social contextual factors together with disclosure behaviors have different effects on health outcomes depending on race/ethnicity. A study with HIV‐positive men found that White HIV‐positive men who disclosed their HIV status to their mothers and are receiving high HIV‐specific family support have slower disease progression.25 In contrast, for Latino men receiving low levels of HIV‐specific family support, disclosure of HIV status to mothers is associated with more disease progression. Another study found that among Latino gay and bisexual men, social support mediates the relationship between disclosure of HIV status and self‐esteem and depression.11 Disclosure results in greater social support which, in turn, has positive effects on psychological well‐being. In another study with gay Latino men, gay community social influence has different effects on disclosure of HIV status depending on to whom the disclosure is made. Greater gay community involvement is associated with less HIV status disclosure to casual sexual partners but more HIV status disclosure to close friends.22 18
Chapter 3: Data Description and Methods Section 3.1: Research Design This research uses data from the Brothers Y Hermanos project, consisting of cross‐sectional quantitative structured interviews with 565 Latino men who have sex with men (MSM) in Los Angeles County. The purpose of the Brothers Y Hermanos project was to identify and understand demographic, social, psychological, structural, cultural, and behavioral characteristics of Latino MSM associated with sexual and drug‐
use behaviors that place them at risk for or protect them against contracting or transmitting HIV. Respondents completed the structured interviews between April 2004 and June 2005. Section 3.1.a: Research Sites The Brothers Y Hermanos project, which targeted New York City, Philadelphia and Los Angeles County, was a multi‐site, multi‐phase study coordinated by the CDC. Phase 1 of the project involved qualitative formative research with focus groups and in‐
depth individual interviews with Black and Latino MSM. Phase 2 of the project involved a comprehensive quantitative survey in addition to HIV counseling and testing. This research will utilize data from the quantitative survey collected in Los Angeles County by the HIV Epidemiology Program at the Los Angeles County Department of Public Health as part of its Brothers Y Hermanos project. As part of its overall mission, the HIV Epidemiology Program is responsible for collecting, analyzing, and disseminating HIV/AIDS surveillance and epidemiologic 19
study data in Los Angeles County. The HIV Epidemiology Program, in its capacity as the Project Director of the Los Angeles County site for the Brothers Y Hermanos project, was responsible for the day‐to‐day operations of the project: training interview staff; shepherding oral and blood specimens through labs; keeping track of RDS coupons and compensation dispensed to respondents; and sending data to the CDC. The HIV Epidemiology Program worked with two community based organizations (CBOs), Bienestar and The Wall Las Memorias, that provided personnel and space to conduct counseling and testing activities. Section 3.1.b: Sampling Frame and Recruitment RDS is a recruitment strategy based on chain‐referral sampling.39 It involves a system of coupons to keep track of respondents enrolled in the study and who is recruited by whom. RDS has been used to recruit hard to reach populations such as intravenous drug users (IDUs) and sex workers.40 The RDS approach uses social network referrals as a means to approximate probability sampling that obtains unbiased estimates where the characteristics of interest of the final sample are independent from those of the initial sample. This equilibrium state is reached if the recruitment waves are extended far enough to recruit a large number of respondents to the study. The number of waves needed to reach equilibrium varies depending on the composition of the initial sample and the characteristics of interest.41 For example, in one study with IDUs the number of waves necessary to reach racial/ethnic equilibrium is fewer compared to the 20
number of waves needed to reach equilibrium based on drug preferences or area of residence.41 However, the proposed research will not rely on whether equilibrium is reached. Instead, it will take advantage of network‐based referrals whereby respondents are embedded in similar social contexts and are likely to be similar to each other across key individual and social context characteristics to investigate the impacts of social network structure, specifically referral pairs, on individual behaviors and similarity in behavior within dyads. The Brothers Y Hermanos project utilized RDS to recruit MSM. The project assumed that Latino MSM can most efficiently identify other Latino MSM, especially those who could not be accessed in “gay‐identified” neighborhoods or public settings. The project’s aim was to estimate the site‐specific HIV prevalence and racial/ethnic‐
specific HIV incidence rates as accurately as could be done using probability sampling. Taking into account that respondents recruited via RDS are more similar to each other in their HIV status, a sample of at least 500 respondents was determined to be necessary to accomplish this aim. The final sample size was 565. To be eligible for the Brothers Y Hermanos project, respondents had to be male, 18 years of age or older, Latino, reside in Los Angeles County, and have had sex with a man in the past 12 months. Because respondents were recruited using RDS, respondents were required to present a coupon indicating they had been referred by another study respondent who had been designated to recruit additional respondents. Respondents 21
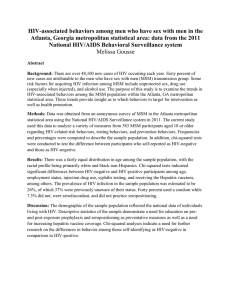
were additionally required to provide informed consent and must have been willing to be tested for HIV. To begin the RDS recruitment process, 20 original respondents known as seeds were chosen before data collection began. Seeds were diverse in terms of sexual orientation or identification, age, and HIV status. This was done to minimize the number of waves required to reach the equilibrium state where the HIV incidence and prevalence rates in the final sample would be unbiased. All respondents, seeds and alters (respondents who were recruited by seeds), were asked to recruit up to three individuals whom they knew personally and who met the above mentioned eligibility criteria. The number of additional referrals that respondents could recruit to the project was capped at three to foster long recruitment chains and to prevent the recruitment process from being dominated by any single respondent. This also allowed for the equilibrium state of HIV rates to be reached before reaching the target sample size of 500. Lastly, capping the number of referrals at three minimized the chance of respondents recruiting strangers in order to receive their incentive payment ($15 per additional individual recruited and $50 for completing the survey). Notably, however, of the 565 respondents, 463 (81.95%) originated from a single seed (See Figure 1). 22
Figure 1:: The largestt referral chaain of the Broothers Y Herrmanos Projject, Los Anggeles Countyy site Section 3.2: Method
ds of Data Collection:: Structured
d Interview
ws and Netw
work Data
The main m
T
mode of data
a collection
n was structtured interv
views. The comprehen
nsive quantita
ative surveey identifieed individ
dual‐level d
demograph
hic, social, psycholog
gical, structural, culturall and behav
vioral chara
acteristics aassociated w
with risk fo
or or protecction against H
HIV infectiion through
h sexual acttivities. Thee interviewss were adm
ministered u
using audio co
omputer‐asssisted self‐iinterview (ACASI). W
With ACASII, responden
nts can listeen to the interrview quesstions throu
ugh a head
dset and/or read the q
questions on
n the comp
puter screen42 and respon
nd by keyin
ng their an
nswers into the compu
uter.42 As an
n instrumeent of 23
data collection, ACASI has the advantage of increasing the probability of reporting on sensitive issues because it provides respondents with more privacy.43 Also, ACASI has been shown to have increased accuracy and lessened respondent burden compared to other methods.43 Data collection took place at the CBO partners, namely, Bienestar and The Wall Las Memorias. Respondents could either schedule the interviews by appointment or walk in. The walk‐in hours included evenings and weekend to accommodate those working during the day. Network data were constructed based on the referral patterns from the RDS recruitment framework. Respondents who recruited other respondent(s) to the study are known as senders. Respondents who were recruited by others are known as receivers. It could be that respondents can be both senders and receivers. That is, respondents can be recruited by others to the study, and in turn, these same respondents recruited additional respondents. A referral pair is composed of a sender and a receiver, and the type of tie between them. Applying social network analysis (SNA) to RDS data has several advantages. As stated previously, RDS operates on respondent referrals, thus the data are inherently relational within the limits of the RDS strategy. As a result, social network analytic tools can be used to understand the social and contextual characteristics that might empower and enable respondents to disclose their HIV status and/or MSM identity to their network members. Retaining the referral ties between respondents who brought each 24
other to the study, statistical analyses can be applied to understand the source and extent of the similarities between referral pairs in their social contexts and individual characteristics and disclosure behaviors. SNA can be used to understand whether similarities in social context characteristics are associated with similar disclosure behaviors. In particular, dyadic analysis within SNA is used to account for the fact that respondents can refer up to three additional other respondents to the project. In other words, dyadic analysis is used to account for the clustering around respondents. This research will take an egocentric approach to elucidate the referral ties that surround the respondents. Network questions included the type of relationship to the person who referred respondents to the study, the size of respondents’ MSM network and the proportion of the MSM network that is Latino. Section 3.3: Measures Using RDS, the Brothers Y Hermanos project collected three types of data: individual measures, global norms and referral ties. These closed‐ended respondent‐
level questions were about individual characteristics, emotional closeness, social support, size of overall and Latino MSM networks, community integration in the Latino and/or gay communities, and disclosure of HIV status and MSM identity. Individual measures The Brothers Y Hermanos project collected information on individual characteristics including age (number of years), education (7 categories, ranging from 25
“did not graduate from high school” to “doctoral degree (PhD or JD)”) , income (10 categories, ranging from less than $5,000 to $80,000 or more a year), place of birth (born in United States or elsewhere), level of acculturation (only Spanish, Spanish more than English, both equally, English more than Spanish, or only English), sexual orientation (heterosexual or “straight”, homosexual or “gay”, bisexual, or other1), and reported HIV status (negative, positive, did not get the result of the last test, or indeterminate2). Global Norms: Social contexts and Disclosure Behaviors. The global norms data collected enable this research to describe the social context that surrounds respondents who disclosed their HIV status and/or MSM identity. Receipt of social support variables included guidance and advice, reassurance of worth and affirmation, emotional support and integration, tangible or practical support, while provision of social support variables included companionship and nurturance and providing support to others. Response options to all social support questions were: strongly agree, agree somewhat, disagree somewhat, or strongly disagree. Emotional closeness variables asked respondents how close they feel towards their sexual partners including last unprotected anal sex (UAS) and protected anal sex (PAS) partners], mothers, fathers, brothers, sisters, ministers or priests, straight and gay friends and doctors. Response options for sexual partners included: very close, somewhat close and not too close. Note, the project did not ask respondents how close 1
Respondents’ whose sexual orientation was “other” were dropped in the analyses due to small numbers
Respondents’ whose reported HIV status was “did not get the result of the last test” or “indeterminate” were
dropped from the analysis due to small numbers
2
26
they feel towards their main sexual partners. For social network members, response options were: very close, somewhat close, not close, or I don’t have this person in my life. Size of MSM community variables asked respondents approximately how many MSM in Los Angeles they know personally. That meant respondents knew their name, who they were and how to contact them; they also knew respondents and respondents have seen them in the last 6 months. Furthermore, respondents were asked of those men, how many were Latino and 18 years of age or older. Response ranges were from 0 to 500. Community integration variables asked respondents how much they feel a part of the overall Latino community, the Latino gay community, and the larger white gay community in Los Angeles. Response options were: very much, somewhat, a little or not at all. Finally, disclosure variables asked whether respondents have disclosed their HIV status and/or their MSM identity to their sexual partners, mothers, fathers, brothers, sisters, ministers or priests, straight and gay friends and doctors. Disclosure of HIV status was two‐fold depending on whether the target(s) of disclosure were sexual partners or members in the respondents’ social networks. Respondents were asked if they directly told their sexual partners of their HIV status, regardless of whether or not the respondent’s HIV status was positive or negative. With social network members, 27
respondents were asked whether they told their family members, friends and community members of their HIV status only if they have previously indicated in the survey that they were HIV‐positive. Therefore, disclosure of HIV‐positive status to social network members involved disclosure of HIV sero‐positivity. Respondents were also asked whether they had told their family members, friends, and community members whether they have had sex with men. Response options to all questions about disclosure of HIV status and MSM identity were binary: yes or no. Referral Ties Respondents were asked if the person who referred them to the study was a friend, acquaintance, sexual partner, relative or co‐worker. The referral pairs (each composing of a sender and a receiver) will serve as the unit of analysis in dyadic analyses. Section 3.4: Analysis Plan In the following analysis plan, respondents’ individual characteristics included age, income, education, place of birth, acculturation, sexual orientation, and reported HIV status. Furthermore, some individual characteristics can be grouped or reclassified so that income and education can be thought as social economic status (SES), place of birth and acculturation can be thought of as ethnic‐identity, gay or bisexual sexual orientation can be thought as MSM‐identity, while sexual orientation and HIV status can be thought as HIV‐risk characteristics. 28
Social context characteristics included emotional closeness to sexual and social network members, social support, size of overall and Latino MSM networks, and integration in the overall Latino community, a Latino gay community, and the larger white gay community. Social context characteristics can also be reclassified where emotional closeness to sexual and social network members and social support can be thought as interpersonal characteristics, and size of overall and Latino MSM networks and community integration in the Latino and/or gay community can be thought as community‐level characteristics. Disclosure behaviors were disclosure of HIV status and MSM identity. Aim 1: Social Context Characteristics by Respondents’ Individual Characteristics The first aim of this study is to identify and describe respondents’ social contexts (e.g., emotional closeness, social support, size of overall and Latino MSM networks, and integration in the Latino and/or communities), including how respondents’ social contexts may vary by their individual characteristics such as age, income, education, place of birth, acculturation, sexual orientation, and/or reported HIV status. RQ 1.1: Description of respondents’ individual and social context characteristics. Who were the respondents of the Brothers Y Hermanos project in terms of age, income, education, place of birth, acculturation, sexual orientation, and/or reported HIV status? What were the levels of emotional closeness, social support, size of overall and Latino MSM networks and integration into the gay and/or Latino communities? 29
RQ 1.2: Social contexts by respondents’ individual characteristics. Did level of emotional closeness, social support, size of overall and Latino MSM networks and integration into the gay and/or Latino communities differ significantly with respect to respondents’ individual characteristics? RQ 1.3: Homophily across individual characteristics. Were referral pairs more similar than other respondents in terms of individual characteristics? RQ 1.4: Homophily across social context characteristics. Were social contexts similar within referral pairs? Aim 2: Disclosure Behaviors by Respondents’ Social Contexts and Individual Characteristics The second aim is to identify and describe HIV status and MSM identity disclosure patterns, including how such patterns may vary by respondents’ social contexts (e.g., emotional closeness, social support, size of overall and Latino MSM networks and integration in the gay and/or Latino communities) and individual characteristics such as age, income, education, place of birth, acculturation, sexual orientation, and/or reported HIV status. RQ 2.1: Description of disclosure rates. What percentage of respondents actively disclosed their HIV status and/or MSM identity to their network members? RQ 2.2: Disclosure patterns by respondent social contexts and individual characteristics. Did disclosure patterns of HIV status or MSM identity (to sexual 30
partners, family members, friends and community members) differ significantly with respect to respondents’ social contexts and individual characteristics? RQ 2.3: Disclosure homophily. Were disclosure patterns of HIV status or MSM identity (to sexual partners, family members, friends and community members) similar within referral pairs? Aim 3: Dyadic Analyses The third aim is to investigate the effects of similarities in social contexts (e.g., in emotional closeness, social support, and community integration and size of MSM network) on mutual disclosure of HIV status and MSM identity within referral pairs. RQ 3.1: Type of ties within referral pairs? What were the types of ties (friends, acquaintances, sexual partners, relatives, co‐workers) within referral pairs? RQ 3.2: Mutual disclosures to specific members. Did referral pairs who reported similar social contexts also both mutually disclose their HIV status and/or MSM identity to specific network members (e.g., sexual partners, mothers, fathers, brothers, sisters, straight friends, gay friends, priests and doctors)? Did the similarities vary by types of referral (e.g., friends, acquaintances, or sexual partners)? Section 3.5: Analytic Strategy This research utilizes traditional quantitative analyses in addition to dyadic analyses. For Aims 1 and 2, I utilize descriptive statistics, and linear and logistic 31
regressions to investigate the relationships between respondent individual characteristics, social context characteristics and disclosure behaviors of HIV status and MSM identity. I use descriptive statistics to answer RQ 1.1 (description of individual and social contexts characteristics), RQ 2.1 (description of disclosure rates), and RQ 3.1 (type of tie within referral pairs). These statistics allow me to understand the range and variation in respondents’ emotional closeness to sexual and social network members, social support, integration in the gay and Latino community, size of MSM community, disclosure of HIV status and MSM identity, and the type of ties between respondents who referred each other to the study. In the analyses, I recoded the response options for sexual orientation to heterosexual versus homosexual and bisexual, and the response options for reported HIV status to positive or negative, dropping out those observations with “did not get the result of the last test” and “indeterminate”. Among the social context characteristics, I recode the response options so that higher scores indicated more emotional closeness, greater social support, larger overall and Latino MSM networks, and more integration in the Latino and/or gay communities. I use linear regression and logistic regressions to answer RQ 1.2 (social contexts by respondent characteristics) and RQ 2.2 (disclosure patterns by respondent social contexts and individual characteristics). This allows me to understand the extent of the associations, if any, between respondent individual characteristics, social contexts and disclosure patterns. Multivariate analyses in RQ1.2 adjusted for respondents individual 32
characteristics (age, SES, ethnic‐identity, MSM‐identity, and reported HIV status). Multivariate analyses in RQ 2.2 adjusted for respondents’ social contexts (emotional closeness, social support, size of overall and Latino MSM networks, and community integration) and individual characteristics. I utilize dyadic analyses for the remaining RQs. For RQ 1.3 (homophily across individual characteristics), RQ 1.4 (homophily within social contexts), I create dyadic indices based on overall similarity, or consensus, to examine the extent of similarities within referral pairs in terms of individual and social contexts characteristics. For RQ 2.3 (disclosure homophily), I create dyadic indices based on positive similarity where both participants within referral pairs mutually disclosed to their respective sexual and social network members. I test for evidence against homophily within referral pairs using the Wilcoxon signed‐rank z‐statistic and the Pearson’s chi‐square statistic. I retained the most prevalent ties (friends, acquaintances, and sexual partners) in the analyses and, due to the small numbers of referral pairs, eliminated those who were relatives or co‐workers. Having created the dyadic indices for RQ 1.3 (individual characteristics homophily), RQ 1.4 (social contexts characteristics homophily), and RQ 2.3 (disclosure homophily), I utilize multivariate regression to answer RQ 3.2 (mutual disclosure to specific types of network members). Multivariate analyses in RQ 3.2 adjusted for referral pairs’ similarities in social context and individual characteristics. In all, the 33
dyadic analyses allow me to see whether and to what extent the similarities in social contexts are associated with mutual disclosure behaviors within referral pairs. Note, these regressions were liberal in the sense that respondents could be both senders and receivers. A more conservative approach would allow respondents to take one and only one role in the study. This dissertation is exploratory in nature and relies primarily on the results of the bivariate findings. I point out multivariate results when they provide additional insights. Due to concerns of adequate sample size in light of the number of explanatory variables, I only present results for models where the number of observations was equal or greater than 50. 34
Chapter 4: Respondents’ Social Contexts and Individual Characteristics This chapter answers four basic questions about the respondents of the Brothers Y Hermanos project. First, who were the respondents in terms of individual characteristics such as age, socio‐economic status (SES), ethnic‐identity, MSM‐identity and reported HIV status? Second, what were their social contexts such as emotional closeness to sexual and social network members, social support, size of overall and Latino MSM networks, and community integration in the Latino and/or gay communities? Third, how did the respondents’ individual characteristics embed them in the various social contexts? Fourth, what was the extent of the similarities of the respondents who referred each other to the project in terms of individual characteristics and social contexts? Section 4.1: Description of Respondents’ Social Contexts and Individual Characteristics This section answers the question of who were the Brothers Y Hermanos respondents (see Table 4.1), and what their social contexts look like. The sample was young, with 38% of respondents between 18 and 34 and 51% between 35 and 50. Most respondents fell on the lower end of the socioeconomic (SES) spectrum, with 62% making less than $10,000 in total yearly income. Two‐thirds (68%) of the respondents reported having graduated from high school (or GED), or less. Respondents were Latino by design. About a quarter of the respondents (27%) were born in the United 35
Table 4.1: Respondentsʹ Individual Characteristics
Characteristics
(N = 565)
% Sample (n)
Age
18 – 34
35 – 50
Over 50
Income
Less than $5,000
$5,000 - $9,999
$10,000 - $19,999
$20,000 - $29,999
$30,000 - $39,999
$40,000 - $49,999
$50,000 - $59,999
$60,000 - $69,999
$70,000 - $79,999
$80,000 or more
Education
Did not graduate from high school
Graduated from high school or GED
Graduated from a technical school
2-year college degree (AA degree)
4-year college degree (BA)
Master’s degree (MA, MS, MPH)
Doctoral degree (PhD, JD)
Place of Birth
Non-U.S. born
U.S. born
Language speak with friends
Only Spanish
Spanish more than English
Both equally
English more than Spanish
Only English
Sexual orientation
Heterosexual or "Straight"
Homosexual or Gay
Bisexual
Other
Reported HIV status
Negative
Positive
Actual HIV status
Negative
Positive
37.52 (212)
51.15 (289)
10.97(62)
34.87 (197)
27.26 (154)
18.05 (102)
8.50 (48)
5.31 (30)
1.06 (6)
0.71 (4)
----0.35 (2)
29.03 (164)
38.94 (220)
11.33 (64)
9.73 (55)
8.50 (48)
1.24 (7)
0.71 (4)
72.74 (411)
27.08 (153)
27.26 (154)
28.50 (161)
19.65 (111)
13.98 (79)
10.44 (59)
4.07 (23)
69.73 (394)
23.19 (131)
2.48 (14)
37.88 (214)
51.15 (289)
43.72 (247)
56.28 (318)
36
States (U.S.) and the level of acculturation was low, with only 24% of respondents speaking English more than Spanish or only English with friends. The vast majority of respondents (93%) identified as either gay or bisexual. More than half (51%) reported being HIV‐positive from the most recent HIV test and 56% of the respondents tested HIV‐positive at the counseling and testing session after the study. Thus, twenty‐nine, or 5% of the respondents were HIV‐positive but unaware of their status before the study. With regards to respondents’ interpersonal relationships to their sexual partners, slightly more respondents reported being very close to their last protected anal sex (PAS) partners (33%) than being very close to their last unprotected anal sex (UAS) partners (30%) (See Table 4.2). Table 4.2: Emotional Closeness To Sexual and Social Network Members
Participants' Reported
Emotional Closeness to…
Not close at all
Last PAS Partner
Last UAS Partner
17.65 (54)
26.17 (67)
Not too close
% Sample (n)
21.24 (65)
28.43 (87)
15.63 (40)
28.52 (73)
Not close
Mother
Gay friends
Sister
Brother
Doctor
Straight friends
Father
Priest
Somewhat
close
13.04 (60)
6.68 (37)
14.52 (72)
22.53 (114)
19.08 (91)
12.89 (70)
41.55 (150)
47.20 (135)
Key statistics are bolded
37
Somewhat
close
% Sample (n)
22.83 (105)
29.78 (165)
28.02 (139)
30.43 (154)
35.01 (167)
50.46 (274)
26.04 (94)
33.57 (96)
Very close
32.68 (100)
29.69 (76)
Very close
64.13 (295)
63.54 (352)
57.46 (285)
47.04 (238)
45.91 (219)
36.65 (199)
32.41 (117)
19.23 (55)
Table 4.3: Perceived Availability and Provision of Social Support
Perceived Availability and Provision of
Functional Form of Social Support
Strongly agree
Agree somewhat
Disagree
somewhat
Strongly Disagree
% (n)
Guidance and Advice
There is no one I can talk to about the
important decisions in my life
I have someone who gives me advice when
I'm confused or need to sort things out
Reassurance of worth/Affirmation
I feel no one respects who I am
I have people who accept me as I am
Emotional support/Attachment
No one really understands my most private
worries and fears
If I was going through a hard time, I have
someone who would be right there with me
Tangible or Practical Support
If I was sick in bed, I have someone who
would help take care of me
There is no one I can depend on to lend me
$50 if I needed it for an emergency
Companionship
I often feel isolated and alone
I have someone who visits, calls or emails me
just to see how I am doing
Nurturance/Providing support to others
No one needs me to take care of them
I often provide advice and support to my
family and friends
22.78 (128)
22.24 (125)
17.26 (97)
37.72 (212)
53.11 (299)
28.6 (161)
6.39 (36)
11.9 (67)
12.48 (70)
61.96 (347)
18.72 (105)
24.82 (139)
21.93 (123)
5.89 (33)
46.88 (263)
7.32 (41)
26.12 (146)
28.26 (158)
19.5 (109)
26.12 (146)
59.64 (334)
23.93 (134)
6.96 (39)
9.46 (53)
52.50 (294)
25 (140)
9.29 (52)
13.21 (74)
24.29 (136)
15.89 (89)
19.11 (107)
40.71 (228)
28.75 (161)
24.46 (137)
17.86 (100)
28.93 (162)
53.83 (302)
25.13 (141)
7.31 (41)
13.73 (77)
21.29 (119)
21.82 (122)
22.72 (127)
34.17 (191)
58.82 (330)
27.81 (156)
6.95 (39)
6.42 (36)
Key statistics are bolded
With respect to members in their social networks, more than half of the respondents reported being very close emotionally to their mothers (64%), gay friends (64%) and sisters (57%). More respondents reported being very close to their brothers 38
(47%) and doctors (46%) than compared to their straight friends (37%) and fathers (32%). Less than one‐fifth of respondents reported being very close to their priests. Respondents reported high social support available (See Table 4.3). In general, more respondents reported strongly agreeing with positive statements of social support and conversely, strongly disagreeing with negative statements of social support. Of particular note is that about two‐thirds (60%) of respondents reported strongly agreeing with the statement “If I was going through a hard time, I have someone who would be right there with me” and more than half of the respondents (54%) reported strongly agreeing with the item: “I have someone who visits, calls or emails me just to see how I am doing”. However, similar proportions of respondents endorsed items: “I often feel isolated and alone” and “No one really understands my most private worries and fears.” Table 4.4: Size of MSM Networks
Size of overall MSM network
Size of Latino MSM network
Mean
19.23
14.09
SD
42.88
31.38
At the community level, while respondents’ MSM networks were not homogenous, they were mostly comprised of other Latino MSM (See Table 4.4). On average, respondents reported knowing personally about 19 other MSM in Los Angeles whom respondents have been in contact with in the past 6 months. Of those, on average, 14 were Latino MSM. In addition, respondents were more integrated in the 39
Latino communities than the gay communities (See Table 4.5). A larger proportion (56%) of respondents reported feeling very much part of the overall Latino community than compared to the Latino gay community (45%) or the larger white gay community (16%). Section 4.2: Associations between Social Contexts and Individual Characteristics This section answers the question of how respondents’ individual characteristics embedded them in the various social environments. That is, how did respondents’ age, SES, ethnic‐identity, MSM‐identity and HIV‐risk characteristics influence emotional closeness to their sexual partners and social network members, the types of social support available to them, the size of their MSM networks, and the extent of their integration in the Latino and/or gay communities. Table 4.5: Level of Community Integration
Not at all
Feel part of…
the overall Latino community in Los Angeles
a Latino gay community in Los Angeles
the larger white gay community in Los Angeles
4.45 (25)
10.68 (60)
32.92 (185)
A little
Somewhat
% (n)
12.10 (68)
27.76 (156)
16.19 (91)
28.29 (159)
25.44 (143)
25.98 (146)
Very much
55.69 (313)
44.84 (252)
15.66 (88)
Key statistics are bolded
Emotional Closeness and Respondent Characteristics Emotional Closeness to Sexual Partners Being U.S. born was positively associated with emotional closeness to sexual partners while education and HIV‐positive status were negatively associated with 40
Table 4.6: Bivariate Associations Between Individual Characteristics and Reported Emotional Closeness to Sexual and Social Network Members
Individual Characteristics
Age
Income
Education
Place of Birth (non-U.S. born)
U.S.-born
Level of Acculturation
Sexual Orientation
(Heterosexual)
Homosexual/Bisexual
Reported HIV Status (Negative)
Positive
Dependent Variable (Beta): Emotional Closeness
Closeness- Closeness- Closeness- ClosenessStraight
Sister
Gay
Priest
Friends
Friends
ClosenessLast UAS
Partner
ClosenessLast PAS
Partner
ClosenessMother
0.01
-0.04
-0.09*
0.14
-0.03
-0.15**
0.02
-0.02
-0.01
-0.06
-0.01
0.03*
0 .03
-0.05**
-0.01
-0.01
<0.01
0.03*
0.03
0.03
0.30**
0.05
0.01
-0.01
-0.002
0.03
-0.08
-0.01
0.22
-0.27
-0.02
-0.12
-0.37**
-0.12
0.11
-0.08
ClosenessBrother
ClosenessFather
ClosenessDoctor
0.16**
-0.01
-0.02
0.03
-0.08**
-0.04
0.09
-0.08**
<0.01
0.35**
-0.11**
-0.05**
0.06
0.01
-0.1
-0.02
-0.15*
-0.05*
-0.19**
-0.08**
-0.27**
-0.09**
-0.22
0.59**
-0.2
-0.35**
-0.24
-0.04
0.12*
<0.01
0.21**
0.05
0.23**
0.77**
*p-value < 0.10
**p-value < 0.05
emotional closeness to sexual partners. U.S.‐born respondents reported significantly more emotional closeness to their last PAS partners than did non‐U.S.‐born respondents. In contrast, respondents with more education reported significantly less emotional closeness to their last PAS partners, at both the bivariate and multivariate levels of analyses. Respondents whose last HIV test results were positive reported significantly less emotional closeness to their last UAS partners at both the bivariate and multivariate levels of analyses. 41
Table 4.7: Multivariate Associations Between Individual Characteristics and Reported Emotional Closeness to Sexual and Social Network Members
Individual Characteristics
Age
Income
Education
Place of Birth (non-U.S. born)
U.S.-born
Level of Acculturation
Sexual Orientation
(Heterosexual)
Homosexual/Bisexual
Reported HIV Status (Negative)
Positive
Dependent Variable (Beta): Emotional Closeness
Closeness- Closeness- Closeness- ClosenessSister
Father
Brother
Priest
(N = 420)
(N = 308)
(N = 426)
(N = 226)
ClosenessLast UAS
Partner
(N = 220)
ClosenessLast PAS
Partner
(N = 256)
ClosenessMother
(N = 387)
0.24*
-0.06
-0.06
0.25**
-0.04
-0.14**
-0.02
-0.01
0.01
0.02
-0.03
-0.01
0.07
-0.05
0.04
0.04
-0.08**
0.01
-0.02
0.08
0.22
0.01
0.06
-0.01
-0.14
0.02
-0.10
-0.03
0.44
-0.47
-0.14
-0.20
-0.48**
-0.14
0.11
0.09
ClosenessStraight
Friends
(N = 455)
ClosenessGay
Friends
(N = 465)
ClosenessDoctor
(N = 409)
0.10
0.03
-0.02
-0.04
-0.04*
0.06**
-0.01
-0.01
0.05**
0.18**
-0.03
-0.03
-0.13
-0.02
-0.09
-0.02
-0.10
0.04
0.06
-0.03
-0.17**
0.02
-0.40
-0.26
-0.27
-0.25
0.76**
-0.05
0.18*
-0.04
0.22**
-0.08
-0.05
0.68**
*p-value < 0.10
**p-value < 0.05
Social Network Members There was a grouping in respondents’ reported emotional closeness to social network members: mothers and sisters, fathers and brothers, friends, and community members. (Also see Table 4.6 and 4.7). At both the bivariate and multivariate level, respondents’ individual characteristics were invariant to reported emotional closeness to their mothers. Higher income respondents reported significantly less emotional closeness to their sisters while HIV‐positive
42
respondents reported marginally more emotional closeness to their sisters. Earning higher incomes, being U.S.‐born and more acculturated were associated with respondents reporting less closeness to their fathers while being HIV‐positive was associated with respondents being closer to them. Respondents who earned higher income and those who identified as gay or bisexual reported less closeness to their brothers. At the multivariate level, earning higher income was associated with respondents being less close to their brothers. At the multivariate level, more educated respondents were emotionally closer to their straight and gay friends. Not surprisingly, respondents who identified as gay or bisexual were closer to their gay friends but not to their straight friends at the multivariate level. Older respondents and those who were HIV‐positive reported being closer to their priests and doctors. These associations held true at the multivariate level for doctors. HIV‐positive respondents, although not older participants, were closer to their priests at the multivariate level. 43
Social Support and Respondent Characteristics At the interpersonal level, respondents’ relationships to their sexual and social network members enabled them to garner and also provide various functional types of social support. A striking pattern exists: across all types of support, Table 4.8: Bivariate Associations Between Perceived Social Support and Individual Characteristics
Guidance and
Advice
Individual Characteristics
Age
Income
Education
Place of Birth (non-U.S. born)
U.S.-born
Level of Acculturation
Sexual Orientation
(Heterosexual)
Homosexual/Bisexual
Reported HIV Status (Negative)
Positive
Dependent Variable (Beta): Functional Types Social Support
Reassurance of Emotional
Tangible or
Companionship
worth/
support/
Practical
Affirmation
Attachment
support
Nurturance/
Providing
support for
others
-0.18**
0.11**
0.12**
-0.11**
0.09**
0.11**
-0.09*
0.09**
0.11**
-0.15**
0.12**
0.09**
-0.18**
0.12**
0.10**
-0.13**
0.07**
0.09**
0.15*
0.09**
0.08
0.06**
0.02
0.04
0.10
0.07**
0.05
0.03
-0.08
0.01
0.36**
0.01
0.26
0.06
0.42**
0.01
-0.03
-0.10
0.03
-0.04
0.02
-0.05
*p-value < 0.10
**p-value < 0.05
older participants reported receiving less support and, in turn, provided less support to others in their networks (See Table 4.8 and 4.9). In contrast, higher income and more educated respondents reported receiving more social support and, 44
in turn, provided more support to others. (This also held true across various types of social support: guidance and advice, reassurance of worth, emotional support, tangible support, companionship and nurturance). More acculturated respondents reported receiving more guidance and advice, affirmation and tangible support. Respondents who identified as gay or bisexual reported receiving significantly more guidance and advice and companionship. Table 4.9: Multivariate Associations Between Perceived Social Support and Individual Characteristics
Guidance and
Advice
Individual Characteristics
Age
Income
Education
Place of Birth (non-U.S. born)
U.S.-born
Level of Acculturation
Sexual Orientation
(Heterosexual)
Homosexual/Bisexual
Reported HIV Status (Negative)
Positive
Dependent Variable (Beta): Functional Types Social Support
Reassurance of Emotional
Tangible or
Companionship
worth/
support/
Practical
Affirmation
Attachment
support
Nurturance/
Providing
support for
others
-0.16**
0.07**
0.10**
-0.08
0.05**
0.08**
-0.10*
0.05**
0.10**
-0.16**
0.10**
0.05
-0.17**
0.10**
0.06**
-0.10*
-0.03
0.09**
-0.01
0.06
-0.04
0.03
-0.07
0.01
-0.09
0.03
-0.10
0.02
-0.14
-0.02
0.04
-0.04
0.1
-0.09
0.3
-0.02
0.07
-0.04
0.08
0.08
0.09
-0.04
*p-value < 0.10
**p-value < 0.05
45
Size of MSM Networks and Respondent Characteristics As with social support, older respondents reported significantly smaller MSM networks, both overall and Latino networks (See Table 4.10 and 4.11). These associations remained significant at the multivariate level. Higher SES respondents had significantly larger MSM networks, both overall and Latino networks. The associations Table 4.10: Bivariate Associations Between Size of MSM Community and Individual
Characteristics
Dependent Variable (Beta): Size of MSM
Community
Individual Characteristics
Age
Income
Education
Place of Birth (non-U.S. born)
U.S.-born
Level of Acculturation
Sexual Orientation (Heterosexual)
Homosexual/Bisexual
Reported HIV Status (Negative)
Positive
Size of Overall
MSM Network
Size of Latino
MSM Network
-0.40**
0.16**
0.19**
-0.38**
0.10*
0.13**
0.22
0.11*
-0.10
-0.03
0.82**
0.64*
-0.33**
-0.19
*p-value < 0.10
**p-value < 0.05
between education and size of (overall and Latino) MSM networks remained marginally significant at the multivariate level. Respondents who identified as gay or bisexual reported significantly larger overall MSM networks. In contrast, HIV‐positive respondents reported significantly smaller overall MSM networks. 46
Table 4.11: Multivariate Associations Between Size of MSM Community and Individual
Characteristics
Dependent Variable (Beta): Size of MSM
Community
Individual Characteristics
Age
Income
Education
Place of Birth (non-U.S. born)
U.S.-born
Level of Acculturation
Sexual Orientation (Heterosexual)
Homosexual/Bisexual
Reported HIV Status (Negative)
Positive
Size of Overall
MSM Network
Size of Latino MSM
Networks
-0.41**
0.09
0.13*
-0.40**
0.05
0.12*
0.02
0.03
-0.12
-0.08
0.81*
0.62
-0.15
-0.07
*p-value < 0.10
**p-value < 0.05
Community Integration and Respondent Characteristics The extent of respondents’ integration in the various communities which they were a part of was associated with their ethnic‐identity (See Table 4.12 and 4.13). Specifically, U.S.‐born and more acculturated respondents were significantly less integrated in the overall Latino community and the gay Latino community. At the multivariate level, more acculturated respondents were significantly less integrated in the overall Latino community and the gay Latino community in Los Angeles. In contrast, respondents who identified as being gay or bisexual were more integrated in the Latino gay community and the larger white gay community. The associations held true at both the bivariate and multivariate levels of analyses. 47
Table 4.12: Bivariate Associations Between Extent of Community Integration and Individual
Characteristics
Dependent Variable (Beta): Extent of Community
Integration in…
Individual Characteristics
Age
Income
Education
Place of Birth (non-U.S. born)
U.S.-born
Level of Acculturation
Sexual Orientation (Heterosexual)
Homosexual/Bisexual
Reported HIV Status (Negative)
Positive
The Overall
Latino
Community
A Latino Gay
Community
The Larger White
Gay Community
-0.10*
-0.01
-0.03
-0.11
-0.02
-0.01
-0.04
-0.02
-0.04
-0.33**
-0.13**
-0.28**
-0.12**
0.09
0.04
-0.05
1.39**
1.03**
-0.06
0.08
0.13
*p-value < 0.10
**p-value < 0.05
Table 4.13: Multivariate Associations Between Extent of Community Integration and Individual
Characteristics
Dependent Variable (Beta): Extent of Community
Integration in…
Individual Characteristics
Age
Income
Education
Place of Birth (non-U.S. born)
U.S.-born
Level of Acculturation
Sexual Orientation (Heterosexual)
Homosexual/Bisexual
Reported HIV Status (Negative)
Positive
The Overall
Latino
Community
A Latino Gay
Community
The Larger White
Gay Community
-0.05
0.03
-0.01
-0.12*
0.02
-0.01
-0.04
0.03
-0.06*
-0.12
-0.16**
0.11
-0.18**
-0.03
-0.01
0.02
1.59**
1.19**
-0.12
-0.03
0 .09
*p-value < 0.10
**p-value < 0.05
48
Section 4.3: Respondent and Social Contexts Characteristics Homophily This section addresses the question: given that respondents who referred each other to the Brothers Y Hermanos study were embedded in one another’s social networks, how similar were they in the individual and social contexts characteristics? Individual characteristics homophily Respondents who referred each other to the Brothers Y Hermanos project were Table 4.14: Individual Characteristics Homophily Within Referral Pairs
Extent of
Homophily
Wilcoxon signedrank z-statistic
Similarities In…
Age
Income
Education
Acculturation
88.54%
87.82%
77.76%
75.35%
1.91
-0.49
0.73
-0.12
Place of Birth
Sexual Orientation
Reported HIV Status
Average homophily
72.02%
93.47%
76.02%
82.49%
Pearson's chisquare statistic
39.01**
0.35
99.83**
*p-value < 0.10
**p-value < 0.05
highly similar to each other in their individual characteristics (See Table 4.14). On average, there was 82% similarity within referral pairs on their individual characteristics. There was least similarity within referral pairs on the place of birth but nevertheless the extent of similarity on that measure was still high at 72%. Referral pairs reported most similarity on sexual orientation where there was 93% similarity. There was no evidence against homophily within referral pairs on measures of income, 49
education, acculturation or sexual orientation. However, there were statistically significant dis‐agreements within referral pairs on place of birth and reported HIV status, though this does not necessarily imply meaningful differences. Specifically, 136 of the respondent senders were born in the U.S. compared to 134 of the respondent receivers. Furthermore, 310 of the respondent senders reported being HIV‐positive compared to 265 of the respondent receivers. Social Context Characteristics Homophily The extent of similarity in emotional closeness to sexual and social network members was high, ranging from 56% to 73% (See Table 4.15). Referral pairs reported slightly more similarity in their reported emotional closeness to their respective PAS partners (62%) than compared to their respective UAS partners (61%). Within family members, referral pairs reported more similarity in their respective closeness to their mothers (64%) and sisters (61%) than compared to their fathers (56%) and brothers (57%). Among friends, referral pairs reported more similarity in their reported closeness to their gay friends (73%) than compared to their straight friends (64%). With respect to community members, referral pairs showed more similarity in their reported closeness to their doctors (66%) than compared to their respective priests or ministers (61%). 50
Table 4.15: Social Context Characteristics Homophily Within Referral Pairs Extent of Homophily
Wilcoxon
signed-rank
z-statistic
62.21%
60.68%
0.39
-1.30
63.50%
56.13%
61.13%
57.18%
73.08%
64.06%
65.86%
61.03%
1.99**
-0.49
-0.01
-0.35
-1.30
-0.35
0.88
0.24
74.83%
72.65%
71.10%
70.48%
67.96%
73.14%
-0.63
0.35
0.48
-0.92
0.99
0.08
69.49%
73.18%
0.03
0.09
72.71%
67.46%
60.03%
0.96
1.16
0.76
Similarities In Emotional Closeness
Sexual Partners
Last PAS partner
Last UAS partner
Social Network Members
Mother
Father
Sister
Brother
Gay friends
Straight friends
Doctor
Priest or minister
Similarities In Social Support
Reassurance of worth/affirmation
Emotional support/attachment
Guidance and Advice
Companionship
Tangible or practical support
Nurturance/providing support for others
Similarities In Size of MSM Community
Size of overall MSM network
Size of Latino MSM network
Similarities In Community Integration
Overall Latino community
Latino Lay community
Larger white gay community
*p-value < 0.10
**p-value < 0.05
There was no evidence against homophily within referral pairs with respect to emotional closeness to their sexual and social network members, with the exception of mothers. Sixty‐eight percent of the respondent senders reported feeling very close to their mothers as compared to 63% of the respondent receivers, which, though significant, might not represent a meaningful difference. 51
The extent of similarities within referral pairs in the receipt of social support ranged from 68% (tangible support) to 75% (reassurance of worth). Referral pairs had 73% similarity in nurturance or providing support to others. Referral pairs were more similar in the size of their Latino MSM networks (73%) than the size of their overall MSM networks (69%). With respect to community integration, referral pairs were most similar in the extent that they feel part of the overall Latino community (73%) followed by feeling part of the gay Latino community (67%) and the larger white gay community (60%). There was no evidence against homophily within referral pairs with respect to social support, MSM network size, or community integration. Section 4.4: Discussion and Conclusion To summarize, most of the respondents in the Brothers Y Hermanos study were young, had low SES, were not born in the U.S., had low level of acculturation, and identified as gay or bisexual. About half of the respondents reported being HIV‐
positive. More respondents reported being very close to their last PAS partners than to their last UAS partners, suggesting that condom use might be indicative of trust and intimacy between sexual partners. Respondents reported being very close to the women in their families (mothers and sisters). Furthermore, emotional closeness to mothers and sisters were not associated with respondents’ individual characteristics, suggesting that these members were a possible source of support and stability for respondents. Some respondent characteristics have opposing influences on respondents’ social versus 52
sexual networks. For example, HIV‐positive respondents were closer to their fathers, priests and doctors but less close to their last UAS partners. Likewise, more educated respondents were closer to their straight and gay friends but less close to their last PAS partners. Not surprisingly, respondents who identified as gay or bisexual were closer to their gay friends whom the shared a common sexual orientation with. Network size can be thought of as the potential for support available for respondents to draw on. My analyses found that size of MSM networks and functional forms of social support shared many similar associations with respondents’ individual characteristics. As respondents grow older, they reported smaller overall and Latino MSM networks. Correspondingly, older respondents reported receiving and providing less social support of all types. More educated and higher income respondents had larger overall and Latino MSM networks. Correspondingly, these higher SES respondents reported receiving and providing more social support of all types. Respondents who identified as gay or bisexual had larger overall MSM networks and also received more guidance, advice and companionship. This suggests respondents who accepted their sexual orientation were able to garner more support for themselves. Respondents felt most integrated in the overall Latino community, followed by the Latino gay community and least integrated in the larger white gay community. The associations between community integration diverge between ethnic‐identity versus sexual orientation. U.S.‐born and more acculturated respondents were less integrated in 53
the overall Latino community and a gay Latino community. Conversely, gay and bisexual respondents were more integrated in the Latino gay community and the larger white gay community. These findings suggest that public health media campaigns and outreach efforts should target Latino gay MSM specifically rather than just MSM of all race/ethnicities. Respondents who referred each other to the Brothers Y Hermanos project were highly similar in their individual characteristics and social contexts. The ranges of similarity within referral pairs were from 72% to 93% on respondent characteristics and 56% to 75% on social context characteristics. Building on the intuition of homophily theory, this suggests that respondents might be in the position to influence each other and interventions should find ways to take advantage of it. Having examined the respondents’ individual characteristics and social contexts, in the next chapter, I will examine if there are (and the extent of) associations between respondents’ disclosure of their HIV status and MSM identity and their individual characteristics and social contexts. 54
Chapter 5: Respondents’ Disclosure Behaviors of HIV Status and MSM Identity This chapter answers questions about respondents’ HIV status and MSM identity disclosure behaviors. First, what were the rates at which respondents disclosed their HIV status and MSM identity to their sexual and social network members? Second, what social contexts and individual characteristics were associated with respondents’ disclosure behaviors to sexual and social network members? Third, what was the extent of mutual disclosures of HIV status and MSM identity within referral pairs? Section 5.1: Rates of HIV Status and MSM Identity Disclosure This section answers the questions of who in their sexual and social networks did respondents disclose to about regarding their HIV status and MSM identity, and the rates of those disclosures. More respondents disclosed their HIV status (either negative or positive) to their main sexual partners (70%) than to their last unprotected anal sex (UAS) partners (48%) and protected anal sex (PAS) partners3 (44%) (See Table 5.1). With respect to their social network members, more respondents disclosed their HIV‐positive status to their gay friends (78%) and sisters (54%) than to anyone else in their networks. Perhaps surprisingly, doctors ranked third as targets of disclosures with 48% of the respondents disclosing their HIV‐positive status to doctors who were not treating them for HIV. Forty‐five percent of respondents disclosed their HIV‐positive status to their brothers, 3
Types of sexual partners were not necessarily mutually exclusive categories. It might be the case for some respondents that their main partners were also be their last UAS and/or PAS partners. 55
43% to their straight friends, and 41% to their mothers. Fewest respondents disclosed their HIV‐positive status to their fathers (22%) and priests or ministers (15%). Table 5.1: Rates of HIV Status Disclosure To Sexual and Social Network Members Disclosure of HIV status to…
Main MSM sex partner
Last UAS sex partner
Last PAS sex partner
Gay friends
Sister
Doctor
Brother
Straight friends
Mother
Father
Priest
Percent Disclosed
to About HIV
status
70.16%
48.63%
44.48%
Percent Disclosed
about HIVpositive status
78.44%
53.90%
47.96%
44.61%
43.12%
40.89%
21.93%
14.87%
N
258
255
308
N
269
269
269
269
269
269
269
269
As with HIV‐positive status disclosure, more respondents disclosed their MSM identity to their gay friends (79%) than to any other member in their social networks (See Table 5.2). Fifty‐three percent of respondents disclosed their MSM identity to their doctors, followed by 48% disclosing to their straight friends, 43% to their sisters, 38% to their mothers, and 36% to their brothers. Fewest respondents disclosed their MSM identity to their fathers (19%) and priests or ministers (12%). 56
Table 5.2: Rates of MSM Identity Disclosure To Social Network
Members
Disclosure of MSM Identity to…
Gay friends
Doctor
Straight friends
Sister
Mother
Brother
Father
Priest
Percent Disclosed
to About MSM
Identity
78.57%
52.86%
48.16%
43.06%
38.37%
35.71%
18.78%
11.84%
N
490
490
490
490
490
490
490
490
Section 5.2: Associations between Disclosure Behaviors and Social Contexts and Individual Characteristics This section answers the question of which of respondents’ social contexts and individual characteristics were associated with disclosure of HIV status and MSM identify. That is, how did being embedded in various social contexts influence disclosure behaviors. At the individual level, how did respondents’ age, SES, ethnic‐
identity, HIV‐risk characteristics influence disclosure of HIV status and MSM identity. Disclosure of HIV Status4 to Sexual Partners Respondents had increased odds of disclosing their HIV status to sexual partners to whom they were closer (See Table 5.3 and 5.4). Specifically, respondents who were closer to their last UAS partners had 1.47 times in the odds of disclosing their HIV status to them. At the multivariate level, respondents had 1.62 times in the odds of disclosing their HIV status to their last UAS partners with whom they
4
Disclosure to sexual partners involved disclosure of both HIV‐positive and HIV‐negative statuses.
57
Table 5.3: Bivariate Associations Between HIV Status Disclosure and Respondent Social Context and Individual Characteristics
Dependent Variables (Odds Ratios):
Disclosure of HIV Status To…
Disclosure of HIV-Positive Status To...
Main
Last UAS Last PAS
Mother
Father
Brother
Sister
Straight
Gay
partner
partner
partner
Friends
Friends
Social Context Characteristics
Emotional Closeness
1.47**
Last UAS partner
Last PAS partner
1.46**
Mother
1.08
Father
1.44*
Brother
1.81**
Sister
1.69**
Straight friends
2.06**
Gay friends
0.99
Priest/minister
Doctor
Social Support
Overall Social Support Received
1.31
2.57**
1.63**
1.11
1.70**
1.18
1.20
1.45*
1.64**
Size of MSM Community
Size of overall MSM network
1.01
1.00
1.00
1.01**
1.01**
1.00
1.00
1.01*
1.01*
Size of Latino MSM network
1.01
1.00
1.00
1.01*
1.02**
1.00
1.00
1.01
1.03**
Community Integration
Overall Latino community
0.85
0.94
0.87
0.90
0.86
1.21
0.96
0.96
0.89
Latino gay community
0.80
1.18
1.09
0.91
0.93
1.13
0.98
1.09
1.15
Larger white gay community
1.06
1.19
1.24**
0.93
0.93
0.85
0.96
1.17
1.18
Individual Characteristics
Age
0.99
1.01
1.00
0.95**
0.95**
0.99
0.99
0.99
0.96**
Income
0.99
0.91
0.84*
1.06
1.10
0.90
0.96
1.24**
1.26
Education
1.06
1.01
0.93
1.09
1.11
1.03
1.12
1.01
1.20
Place of Birth (non-U.S. born)
U.S.-born
0.91
1.14
1.20
2.52**
2.88**
1.13
1.63
2.65**
1.58
Level of Acculturation
1.16
1.14
1.21**
1.50**
1.55**
1.00
1.06
1.30**
1.36**
Sexual Orientation
(Heterosexual)
§§§
~~~
Homosexual or Bisexual
2.42
3.83*
4.88
0.67
1.41
0.79
7.59**
Reported HIV Status
(Negative)
Positive
2.27**
1.64*
1.11
*p-value < 0.10
~~~ Straight sexual orientation predicts failure to disclose perfectly
**p-value < 0.05
§§§ Straight sexual orientation predicts disclosure perfectly
58
Priest
Doctor
1.84**
1.22
1.07
1.69**
1.01*
1.00
1.01**
1.01*
1.33
1.39*
1.32*
1.12
1.29**
1.23*
0.97
1.05
1.07
1.00
1.17
0.91
1.32
1.03
1.45
1.03
~~~
0.92
were emotionally closer. On the other hand, respondents who were closer to their last PAS partners had 1.46 times in the odds of disclosing their HIV status to them. At the multivariate level, respondents had 1.43 times in the odds of HIV status disclosure to their last PAS partners with whom they were emotionally closer. Social support played a role in disclosure to last UAS partners although not to main sexual partners or last PAS partners. Respondents who reported higher receipt of social support had 1.63 times the odds of disclosure to their last UAS partners. At the multivariate level, respondents with more social support had 2.33 times the odds of disclosure to their last UAS partners. Respondents who were more integrated in the larger white gay community had 1.24 times in the odds of disclosure to their last PAS partners. This association was heightened at the multivariate level whereby more integrated respondents had 1.39 times in the odds of disclosing their HIV status to their last PAS partners. Acculturation was positively associated with disclosure. More acculturated respondents had 1.21 times the odds of disclosing their HIV status to their last PAS partners. At the multivariate level, more acculturated respondents had 1.53 times the odds of disclosure to their last PAS partners. Being HIV‐positive was associated with disclosure to main sexual partners but not to last UAS or PAS partners. HIV‐positive respondents had 2.27 times the odds of disclosing their HIV status to their main sex partners than compared to HIV‐negative 59
respondents. This association was heightened at the multivariate level whereby HIV‐
positive respondents had 3.39 times the odds of disclosure. The size of respondents’ MSM networks and the extent of community integration did not play any role in HIV status disclosure to main sexual partners or last UAS partners at the bivariate level. However, at the multivariate level, the size of respondents’ MSM networks played opposing roles in HIV status disclosure to their last PAS partners. Respondents with larger overall MSM networks had 0.97 times the odds of disclosing their HIV status to their last PAS partners at the multivariate level. However, respondents with larger Latino MSM networks had 1.03 times the odds of disclosure to their last PAS partners at the multivariate level. At the multivariate level, age and income were negatively associated with disclosure of HIV status to sexual partners. An increase of one year in age was associated with 0.97 times the odds of disclosure to main sexual partners. At the multivariate level, higher income respondents had 0.77 and 0.73 the odds of disclosure of HIV statues to their last UAS and PAS partners, respectively. It should be noted that all respondents who identified as straight failed to disclose their HIV status to their last PAS partners. Disclosure of HIV‐Positive Status to Social Network Members Emotional closeness played a positive role in disclosure of HIV‐positive status to all social network members except to mothers, gay friends, and doctors (See Table 5.3 60
and 5.4). Increased emotional closeness was associated with 1.81 times the odds of disclosure to brothers, 1.69 times the odds of disclosure to sisters, 2.06 times the odds of disclosure to straight friends, and 1.84 times the odds of disclosure to their priests. At the multivariate level, all these associations heightened: increased emotional closeness was associated with 1.90 times the odds of disclosure to brothers, 1.71 times the odds of disclosure to their sisters, 2.10 times the odds of disclosing to their straight friends and 2.22 times the odds of disclosing to their priests. Respondents who were closer to their fathers were marginally more likely to disclose their HIV‐positive status to them. Social support was significantly and positively associated with disclosure of HIV‐positive status to mothers, straight and gay friends, and doctors. Specifically, respondents who received higher levels of social support had 1.70 times the odds of disclosure to their mothers, 1.64 times the odds of disclosure to their straight friends, 2.57 times the odds of disclosure to their gay friends, and 1.69 times the odds of disclosure to their doctors. At the multivariate level, respondents who reported receiving higher level of social support had a 2.76 times the odds of disclosure to their gay friends and were marginally more likely to disclose to their mothers. An addition of one more MSM member in respondents’ networks was associated with a 1.01 to 1.03 times the odds of disclosure of HIV‐positive status to social network members. However, at the multivariate level, network size failed to remain significantly associated with disclosure to all social network members except priests. 61
At the multivariate level, network size had opposing influences on disclosure of HIV‐positive status to priests, depending on whether the network was composed of MSM overall or Latino MSM. An increase of one additional MSM member in respondents’ overall MSM networks was associated with 1.06 times the odds of disclosure of HIV‐positive status to priests at the multivariate level. However, an increase of one additional Latino MSM member in respondents’ MSM networks was associated with 0.92 times the odds of disclosure of HIV‐positive status to priests at the multivariate level. Respondents who were more integrated the gay Latino community had a 1.29 times the odds of disclosure to doctors who were not treating them for their HIV. Older respondents were less likely to disclose their HIV‐positive status to their parents and gay friends. A one‐year increase in age was associated with a 0.95 times the odds of disclosure to fathers and mothers and a 0.96 times the odds of disclosure to gay friends. 62
Table 5.4: Multivariate Associations Between HIV Status Disclosure and Respondent Social Contexts and Individual Characteristics
Dependent Variables (Odds Ratios):
Disclosure of HIV Status To…
Last PAS
Main
Last UAS
partner
partner
Partner
(N = 216 )
(N = 248)
(N = 226)
Mother
(N = 188)
Father
(N = 142)
Disclosure of HIV-Positive Status To...
Brother
Sister
Straight
Gay
(N = 220)
(N = 216)
Friends
Friends
(N = 223)
(N = 233)
Priest
(N = 111)
Doctor
(N = 233)
Social Contexts Characteristics
Emotional Closeness
Last UAS partner
Last PAS partner
Mother
Father
Brother
Sister
Straight friends
Gay friends
Priest/minister
Doctor
Social Support
Overall Social Support Received
Size of MSM Community
Size of overall MSM network
Size of Latino MSM network
Community Integration
Overall Latino community
Latino gay community
Larger white gay community
Individual Characteristics
Age
Income
Education
Place of Birth (non-U.S. born)
U.S.-born
Level of Acculturation
Sexual Orientation (Heterosexual)
Homosexual or Bisexual
Reported HIV Status (Negative)
Positive
1.62**
1.43**
1.12
1.52*
1.90**
1.71**
2.10**
0.72
2.22**
1.13
1.46
2.33**
1.48
1.64*
0.85
1.03
1.41
1.14
2.76**
1.18
1.32
0.99
1.03
1.02*
0.97*
0.97**
1.03**
1.01
1.00
1.00
1.02
1.00
1.00
0.98
1.02
1.01
0.99
0.98
1.05*
1.06**
0.92**
1.01
1.00
0.98
0.68*
1.17
0.72
1.20
1.14
0.72*
1.14
1.39**
1.30
0.80
0.88
1.20
0.86
0.96
1.16
0.96
0.81
0.87
0.90
0.95
0.89
1.02
1.07
0.74
0.91
1.35
1.69
1.14
0.86
1.02
1.07
1.07
0.97**
0.89
1.01
1.01
0.77**
0.98
0.99
0 .73**
1.02
0.96*
0.77*
1.03
0.97
0.88
1.15
0.99
0.92
1.16
0.99
0.96
1.25**
1.00
1.16
0.86
0.97
1.26
1.02
0.96
0.78
1.15
1.02
1.24
0.84
0.75
1.25
0.74
1.15
0.57
1.53**
2.10*
1.41**
2.04
1.54**
1.19
0.97
2.06*
0.93
2.36**
1.01
0.79
1.19
1.64
0.82
1.69
0.96
2.85
3.45
~~~
§§§
§§§
0.68
§§§
~~~
1.75
±±±
0.36
3.39**
1.51
0.98
*p-value < 0.10
~~~ Straight sexual orientation predicts failure to disclose perfectly
**p-value < 0.05
§§§ Straight sexual orientation predicts disclosure perfectly
±±± Observations dropped due to collinearity
63
SES was positively associated with disclosure of HIV‐positive status. Respondents with higher income had 1.24 times the odds of disclosure of HIV‐positive status to their straight friends. Respondents with higher education had 1.25 times in odds of disclosure to their sisters at the multivariate level. U.S.‐born respondents had increased odds of disclosure of HIV‐positive status to their parents and friends. U.S.‐born respondents had 2.52 times the odds of disclosure to mothers, 2.88 times the odds of disclosure to fathers, and 2.65 times the odds of disclosure to straight friends. At the multivariate level, U.S.‐born respondents had a 2.36 times the odds of disclosure to their straight friends. Likewise, acculturation was positively associated with disclosure of HIV‐positive status to parents and friends. More acculturated respondents had 1.50 times the odds in disclosing to their mothers, 1.55 times the odds in disclosing to their fathers, 1.30 times the odds in disclosing to their straight friends, and 1.36 times the odds of disclosing to their gay friends. At the multivariate level, more acculturated respondents had 1.41 times the odds in disclosing to their mothers and 1.54 times the odds in disclosing to their fathers. Respondents who identified as gay or bisexual had a 7.59 times the odds of disclosing their HIV‐positive status to their gay friends. All respondents who identified as straight disclosed their HIV‐positive status to their mothers, fathers, and sisters at the multivariate level of analysis. Conversely, all respondents who identified as straight 64
failed to disclose their HIV‐positive status to their straight friends at both the bivariate and multivariate level of analyses. All respondents who identified as straight failed to disclose their HIV‐positive status to their priests at the bivariate level. At the multivariate level of analysis, these observations were dropped due to collinearity.5 Disclosure of MSM Identity to Social Network Members As was with disclosure of HIV‐positive status, emotional closeness played a positive role in disclosure of MSM identity to all social network members except mothers and gay friends (See Table 5.5 and 5.6). Respondents had a 1.28 times the odds of disclosure to their brothers, 1.46 times the odds of disclosure to their sisters, 1.74 times the odds of disclosure to their straight friends, 2.43 times the odds of disclosure to their priests, and 2.17 times the odds of disclosure to their doctors if they were emotionally closer to these members in their social networks. At the multivariate level, respondents had 2.36 times the odds of disclosure to their brothers, 1.71 times the odds of disclosure to their straight friends, 2.42 times the odds of disclosure to their priests, and 2.67 increase the odds of disclosure to their doctors if they were closer to these members. Emotional closeness was marginally associated with increased odds of disclosure to fathers at the bivariate and multivariate levels of analyses. Social support was significantly and positively associated with disclosure of MSM identity to all social network members except doctors at the bivariate level. 5
The observations were dropped due to collinearity because the variable identifying as “straight” in sexual
orientation was highly correlated with other individual and social context characteristics, causing the coefficient
estimates to be erratic due to small changes in the model.
65
Respondents with higher receipt of social support had 1.91 times the odds of disclosure to their mothers, 1.66 times the odds of disclosure to their fathers, 1.63 times the odds of disclosure to their brothers, 1.95 times the odds of disclosure to their sisters, 1.31 times the odds of disclosure to their straight friends, 1.56 times the odds of disclosure to their gay friends, 1.64 times the odds of disclosure to their priests. At the multivariate level, respondents with higher receipt of social support had a 1.60 times the odds of disclosure of MSM identity to their mothers, 1.63 times the odds of disclosure to their sisters, and 1.59 times the odds of disclosure to their straight friends. Respondents with larger MSM networks had increased odds of MSM identity disclosure to their social network members. At the bivariate level, an increase of one additional member in respondents’ overall and Latino MSM networks was associated with a 1.01 to 1.02 times the odds of MSM identity disclosure to parents, straight and gay friends, and priests, respectively. 66
Table 5.5: Bivariate Associations Between MSM Identity Disclosure and Respondent Social Contexts and Individual Characteristics
Mother
Social Contexts Characteristics
Emotional Closeness
Mother
Father
Brother
Sister
Straight friends
Gay friends
Priest/minister
Doctor
Social Support
Overall Social Support Received
Size of MSM Community
Size of overall MSM network
Size of Latino MSM network
Community Integration
Overall Latino community
Latino gay community
Larger white gay community
Individual Characteristics
Age
Income
Education
Place of Birth (non-U.S. born)
U.S.-born
Level of Acculturation
Sexual Orientation
(Heterosexual)
Homosexual or Bisexual
Reported HIV Status (Negative)
Positive
Father
Dependent Variables (Odds Ratios): Disclosure of MSM Identity To…
Brother
Sister Straight Gay
Friends Friends
Priest
Doctor
1.03
1.30*
1.28**
1.46**
1.74**
1.10
2.43**
2.17**
1.91**
1.66**
1.63**
1.95**
2.31**
1.56**
1.64**
1.30*
1.01**
1.01**
1.01**
1.01**
1.00*
1.01*
1.00*
1.00
1.01**
1.01**
1.01**
1.02**
1.01**
1.01**
1.00
1.00
0.81**
1.12
1.06
0.71**
1.00
1.09
0.84
1.14
1.08
0.94
1.19
1.08
0.95
1.13
1.00
0.79*
1.09
1.03
1.17
1.12
1.26
0.92
0.99
1.03
0.97**
1.13*
1.23**
0.98*
1.17**
1.29**
1.00
1.03
1.11
0.98**
1.12
1.24**
0.97**
1.21**
1.25**
0.99
1.14
1.31**
1.01
1.02
1.15
1.04**
1.08
1.29**
1.89**
1.25**
2.86**
1.48**
1.74**
1.12
1.90**
1.26**
1.67**
1.26
1.63*
1.24**
1.32
0.98
0.86
0.97
2.23
~~~
1.98
1.54
1.19
1.84
~~~
1.44
1.20
1.24
1.27
1.64**
0.85
1.04
1.37
6.66**
*p-value < 0.10
~~~ Straight sexual orientation predicts failure to disclose
perfectly
**p-value < 0.05
§§§ Straight sexual orientation predicts disclosure perfectly
67
Integration the overall Latino community was significantly and negatively associated with disclosure behaviors. Respondents who were more integrated the overall Latino community had 0.81 times the odds of disclosure to their mothers and 0.71 times the odds of disclosure to their fathers. At the multivariate level, respondents who were more integrated the Latino community were marginally less likely to disclose their MSM identity to their mothers and fathers. At the multivariate level, respondents who were more integrated the overall Latino community had 0.72 times the odds of disclosure to their brothers. Older respondents were less likely to disclose their MSM identity to their female family members and straight friends but more likely to disclose to their doctors. A one‐
year increase in respondents’ age was associated with 0.97 times the odds of disclosing to their mothers, 0.98 times the odds of disclosing to their sisters, and 0.97 times the odds of disclosing to their straight friends. At the multivariate level, a one‐year increase in respondents’ age was associated with 0.97 times the odds of disclosing to their mothers, and 0.96 times the odds of disclosing to their sisters and straight friends. Conversely, one‐year increase in respondents’ age was associated with 0.96 times the odds of disclosing to their doctors. Older respondents were marginally less likely to disclose their MSM identity to their fathers at the multivariate level. 68
Higher SES respondents were more likely to disclose their MSM identity to members in their social networks. Specifically, respondents with higher income had 1.17 times the odds in disclosure to their fathers, and 1.21 times the odds of disclosure to their straight friends. However, neither of these associations remained significant at the multivariate level. Respondents with higher education had 1.23 times the odds of disclosure to their mothers, 1.29 times the odds of disclosure to their fathers, 1.24 times the odds of disclosure to their sisters, 1.25 times the odds of disclosure to their straight friends, 1.31 times the odds of disclosure to their gay friends and 1.29 times the odds of disclosure to their doctors. At the multivariate level, more educated respondents had 1.32 times the odds of disclosure to their doctors. U.S.‐born respondents were significantly more likely to disclose to their family members and friends but not to their priests or doctors. U.S.‐born respondents had a 1.89 times the odds of disclosure to their mothers, 2.86 times the odds of disclosure to their fathers, 1.74 times the odds of disclosure to their brothers, 1.90 times the odds of disclosure to their sisters, 1.67 times in odds of disclosure to their straight friends. U.S.‐
born respondents were marginally more likely to disclose to their gay friends. U.S.‐born respondents were significantly more likely to disclose to their family members and friends but not to their priests or doctors. U.S.‐born respondents had 1.89 times the odds of disclosure to their mothers, 2.86 times the odds of disclosure 69
Table 5.6: Multivariate Associations Between MSM Identify Disclosure and Respondent Social Contexts and Individual Characteristics
Mother
(N =
337)
Social Contexts Characteristics
Emotional Closeness
Mother
Father
Brother
Sister
Straight friends
Gay friends
Priest/minister
Doctor
Social Support
Overall Social Support Received
Size of MSM Community
Size of overall MSM network
Size of Latino MSM network
Community Integration
Overall Latino community
Latino gay community
Larger white gay community
Individual Characteristics
Age
Income
Education
Place of Birth (non-U.S. born)
U.S.-born
Level of Acculturation
Sexual Orientation (Heterosexual)
Homosexual or Bisexual
Reported HIV Status (Negative)
Positive
*p-value < 0.10
Father
(N =
258)
Dependent Variables (Odds Ratios): Disclosure of MSM Identity To…
Brother
(N = 367)
Sister Straight
Gay
(N =
Friends Friends
365)
(N =
(N =
394)
403)
Priest
(N =
186)
Doctor
(N =
357)
1.01
1.43*
1.36**
1.38*
1.71**
1.00
2.42**
1.67**
1.60**
1.16
1.32
1.63**
1.59**
1.29
1.39
0.99
1.00
1.00
1.00
1.01
1.00
1.00
1.00
1.00
1.01
0.99
0.99
1.02
1.02
0.97
1.00
1.01
0.75*
1.17
1.13
0.68*
1.13
1.05
0.72**
1.23
1.13
0.86
1.28*
1.03
0.86
1.11
0.97
0.79
1.12
1.11
0.99
0.86
0.97
0.92
1.00
0.99
0.97**
1.05
1.11
0.97
1.05
1.26*
0.98
1.07
1.06
0.96**
1.18
1.17
0.96**
1.10
1.06
0.99
1.08
1.21*
1.01
1.06
1.28
1.00
1.17
1.32**
2.21**
1.02
3.10**
1.13
2.66**
1.01
1.87**
1.20
1.22
1.18
1.04
1.29*
2.54*
0.77
0.96
1.17
1.82
~~~
2.27
1.35
0.86
0.91
~~~
2.00
1.74**
2.60**
1.51
2.71**
1.23
1.46
1.68
4.41**
~~~ Straight sexual orientation predicts failure to disclose
perfectly
**p-value < 0.05
70
to their fathers, 1.74 times the odds of disclosure to their brothers, 1.90 times the odds of disclosure to their sisters, 1.67 times in odds of disclosure to their straight friends. U.S.‐
born respondents were marginally more likely to disclose to their gay friends. At the multivariate level, U.S.‐born respondents had significantly increased odds of disclosure to their family members but not to their friends. Specifically, U.S.‐born respondents had a 2.21 times the odds of disclosure to their mothers, 3.10 times the odds of disclosure to their fathers, 2.66 times the odds of disclosure to their brothers and 1.87 times the odds of disclosure to their sisters. Likewise, more acculturated respondents were significantly more likely to disclose their MSM identity to their family members (except brothers) and friends but not their priests or doctors. More acculturated respondents had a 1.25 times the odds of disclosure to their mothers, 1.48 times the odds of disclosure to their fathers, 1.26 times the odds of disclosure to their sisters and straight friends, and 1.24 times the odds of disclosure to their gay friends. The associations between acculturation and disclosure behaviors failed to remain significant at the multivariate level. All respondents identified as straight failed to disclose their MSM identity to their fathers and priests. Perhaps surprisingly, identifying as gay or bisexual were not associated with increased odds of MSM identity disclosure to the other members in respondents’ social networks. 71
Being HIV‐positive was significantly associated with disclosure of MSM identity. Specifically, respondents who were HIV‐positive had 1.64 times the odds of disclosure to their sisters and 6.66 times the odds of disclosure to their doctors. Adjusting for social contexts and individual characteristics, HIV‐positive respondents had 2.71 times the odds of MSM identity disclosure to their sisters and 4.41 times increase the odds of disclosure to their doctors. HIV‐positive respondents also had a 1.74 times the odds of MSM identity disclosure to their mothers and 2.60 times the odds of disclosure to their fathers when adjusting for their social contexts and individual characteristics. Section 5.3: Homophily in HIV Status and MSM Identity Disclosures The goal of this section is to examine the homophily in disclosure behaviors between respondents who referred each other to the Brothers Y Hermanos project. Specifically, this section examines the extent mutual disclosure of HIV status and MSM identity within referral pairs. That is, did respondents within referral pairs both disclose their HIV status, either positive or negative, to their sexual partners? Did respondents within referral pairs both disclose their HIV‐positive status or MSM identity to members their social networks? Homophily in Disclosure of HIV Status to Sexual Partners Referral pairs had more similarity in disclosure of HIV status to main sexual partners than to last UAS or PAS partners (See Table 5.7). Fifty‐one percent of referral pairs both disclosed their HIV status to their respective main sexual partners. In other 72
words, one respondent within the referral pair could have been HIV‐positive and the other respondent could have been HIV‐negative, both respondents could have been HIV‐positive or both respondents could have been HIV‐negative but 51% of referral pairs disclosed their HIV status, whatever it was, to their respective main sexual partners. In contrast, 26% and 24% of referral pairs disclosed to their respective last UAS and PAS partners, respectively. However, there was no evidence against homophily within referral pairs with respect to HIV status disclosure to sexual partners. Table 5.7: Homophily in HIV Status Disclosure Within Referral Pairs
Extent of Homophily
N
Sexual Partners
11
3
51.33%
Main MSM sex partner
11
Last UAS partner
6
25.86%
15
Last UAS partner
7
24.20%
Social Network Members
185
61.08%
Gay friends
185
33.51%
Sister
185
22.70%
Brother
185
22.16%
Doctor
185
20.54%
Straight friends
185
18.38%
Mother
185
5.95%
Father
185
2.70%
Priest
Pearson's Chi-Square
Statistic
0.50
0.93
1.33
0.20
3.51*
1.32
0.20
0.83
0.52
1.09
0.01
*p-value < 0.10
Homophily in Disclosure of HIV‐positive Status to Social Network Members Referral pairs had the greatest similarity in the disclosure of their HIV‐positive status to their gay friends. Sixty‐one percent of referral pairs mutually disclosed their HIV‐positive status to gay friends. Then, homophily in disclosure dropped off 73
dramatically. Thirty‐four percent of referral pairs mutually disclosed their HIV‐positive status to sisters, followed by 23% of referral pairs mutually disclosed to brothers, 22% of referral pairs mutually disclosed to doctors, 21% of referral mutually disclosed to straight friends and 19% of referral pairs mutually disclosed to mothers. It was rare that referral pairs agreed in their disclosure of their HIV‐positive status to their fathers and priests. Six and 3% of referral pairs mutually disclosed their HIV‐positive status to their fathers and priests, respectively. Irrespective of the extent of homophily, there was no evidence against it within referral pairs with respect to HIV‐positive status disclosure to social network members. Homophily in MSM Identity Disclosure to Social Network Members Likewise with HIV status disclosure, more referral pairs mutually disclosed their MSM identity to their gay friends than compared to anyone else in their social networks (See Table 5.8). Sixty‐three percent of referral pairs mutually disclosed their MSM identity to their gay friends. Then homophily in disclosure of MSM identity dropped off dramatically. Thirty‐six percent of referral pairs mutually disclosed their MSM identity to their doctors, followed by 23% to straight friends, 21% to sisters, 17% to mothers, and 14% to brothers. As with HIV status disclosure, few referral pairs agreed in their disclosure of their MSM identity to fathers and priests. Five and 2% of referral pairs mutually disclosed their MSM identity to their fathers and priests, respectively. There was no evidence against homophily within referral pairs with respect to disclosure of 74
MSM identity to social network members, except doctors. Of the 384 referral pairs, 232 of the respondent senders compared to the 202 respondent receivers disclosed their MSM identity to their doctors. Table 5.8: Homophily in MSM Identity Disclosure Within Referral Pairs
Extent of Homophily
N
Social Network Members
384
63.28%
Gay friends
384
36.46%
Doctor
384
23.44%
Straight friends
384
20.83%
Sister
384
17.45%
Mother
384
13.80%
Brother
384
5.21%
Father
384
1.82%
Priest
Pearson's Chi-Square
Statistic
0.07
14.09**
0.22
3.60*
2.95*
1.16
4.11**
0.52
*p-value < 0.10
**p-value < 0.05
Section 5.4: Discussion and Conclusion It is potentially alarming that less than half of the respondents disclosed their HIV status to their last UAS partners even though slightly more than half of the respondents reported being HIV‐positive. Furthermore, the rates of respondents’ disclosure of their HIV status to sexual partners did not correspond with their emotional closeness to these members. Slightly more respondents were very close to their last PAS partners than to their last UAS partners. But slightly more respondents disclosed their HIV status to their last UAS partners than to their last PAS partners. It might very well be, however, that respondents were in long term committed relationships with their last UAS partners. 75
At the individual level, HIV‐positive respondents and more acculturated respondents were more likely to disclose their HIV status. Conversely, higher income respondents were less likely to disclose their HIV status. Moreover, all respondents who identified as straight failed to disclose to their last PAS partners. At the interpersonal level, respondents who were emotionally closer to their sexual partners and received greater social support were more likely to disclose their HIV status to these members. At the community level, respondents who had larger Latino MSM networks and were more integrated in the larger white gay community were likely to disclose to their last PAS partners. The rates at which respondents disclosed their HIV‐positive status to social network members matched well with the rates of their disclosure of MSM identity. In both cases, respondents disclosed most often to gay friends and doctors and least often to their fathers and priests. The rates of disclosure of HIV‐positive status and MSM identity did not always corresponded with emotional closeness to social network members. For example, more respondents were closer to their mothers than anyone else in their social networks. However, mothers ranked sixth in the disclosure of HIV‐positive status and fifth in the disclosure of MSM identity. This suggests that although respondents were very close to their mothers, they might fear disappointing their mothers if they were to disclose that they were gay and/or HIV‐positive. Conversely, few respondents were very close to 76
their doctors but doctors ranked third in the disclosure of HIV‐positive status and second in the disclosure of MSM identity. It might be that respondents were more comfortable with doctors because these members are bound by professional ethics of confidentiality and doctors provide respondents with the needed care for their health. The rates of respondents’ disclosure of their HIV‐positive status and MSM identity to gay friends, fathers and priests did not always correspond with their emotional closeness to these individuals. Gay friends ranked second in emotional closeness and ranked first in the disclosure of HIV‐positive status and MSM identity. This suggests that emotional closeness may not be an important factor in disclosure to gay friends who may be a source of support for respondents. On the other end of the spectrum, few respondents reported feeling very close to their fathers and priests and correspondingly, few respondents disclosed their HIV‐positive status and MSM identity to these members. It might be that respondents did not disclose to their fathers and priests because these members were in positions to cast stigmatizing views of HIV‐
positive status and MSM identity. In other words, disclosure of HIV‐positive status and/or MSM identity might to fathers and priests might have more risks than benefits for respondents. Emotional closeness to mothers, gay friends and doctors did not influence respondents’ disclosure of their HIV‐positive status to these members. A similar pattern holds for MSM identity disclosure whereby emotional closeness did not influence 77
respondents’ disclosure of their MSM identity to their mothers or gay friends. As mentioned previously, respondents were very close to their mothers and yet few respondents disclosed their HIV‐positive status to their mothers. On the other hand, respondents disclosed to their gay friends and doctors irrespective of how emotionally close they were to these members. It might very well be that emotional closeness moderated disclosure of HIV‐positive status and/or MSM identity to certain social network members but not to others. Emotional closeness influenced respondents’ disclosure of their HIV‐positive status and MSM identity to their siblings, straight friends. Respondents disclosed their HIV‐positive status and MSM identity to these members if there were emotionally closer to them. Respondents who were closer to their fathers were marginally more likely to disclose their HIV‐positive status and MSM identity to them. Likewise, respondents with more receipt of social support were more likely to disclose their HIV‐
positive status and MSM identity to their social network members. There might be a stigmatizing effect against disclosure of HIV‐positive status and MSM identity in the Latino community. Size of overall and Latino MSM networks had opposing influences in disclosure of HIV‐positive status to priests. Respondents with larger overall MSM networks were more likely to disclose their HIV‐positive status to their priests. However, respondents with larger Latino MSM networks were less likely to disclose to their priests. Likewise, respondents who were more integrated in the 78
overall Latino community were less likely to disclose their MSM identity to their parents and brothers. As a point of contrast, respondents who were more integrated in a gay Latino community were more likely to disclose their HIV‐positive status to their doctors. Age and SES had opposing effects in the disclosure of HIV‐positive status and MSM identity. Older respondents were less likely to disclose while higher income and more educated respondents were more likely to disclose. As mentioned in the previous chapters, older respondents were embedded in smaller MSM networks and had less receipt of social support. It might be these were the influences against disclosure for older respondents. Conversely, higher SES respondents had more resources such as larger MSM networks and more receipt of social support available to them that fostered disclosure. U.S.‐born and more acculturated respondents were more likely to disclose. This is perhaps because these respondents had more diversely composed MSM networks rather than networks made up of mostly Latino MSM, and were more integrated in the white gay community that would foster them to disclose. Respondents identifying as straight in their sexual orientation were either completely forthcoming or entirely withholding of their HIV‐positive status and MSM identity, depending on the target of the disclosure. All respondents who identified as straight disclosed their HIV‐positive status to their parents and sisters. However, all 79
respondents who identified as straight failed to disclose their HIV‐positive status to their straight friends. All respondents who identified as straight failed to disclosure their MSM identity to their fathers and priests. Respondents who were HIV‐positive were more likely to disclose their MSM identity to their social network members. As with individual and social contexts characteristics, we found no evidence against homophily in mutual disclosure of HIV status or MSM identity within referral pairs, with the exception of disclosure of MSM identity to doctors. Taken together, we see that referral pairs were highly similar in their individual characteristics and social contexts and their mutual disclosures of HIV status and/or MSM identity. This is in stark contrast to the intent of respondent driven sampling (RDS) which aims to approximate probability sampling to obtain estimates that are supposed to approximate independence from those in the initial sample. It might be that the seeds were not very diverse. However, this chapter showed that disclosure behaviors remained dependent on the target of disclosure and possibly to the risks and benefits to the respondents. In the next chapter, I examine whether similarities in individual characteristics and social context characteristics are associated with mutual disclosure behaviors, in which case it might suggest a process of influence between respondents within referral pairs. 80
Chapter 6: Dyadic Analyses: Mutual Disclosure of HIV Status and MSM Identity within Referral Pairs Having found that respondents who referred each other to the Brothers Y Hermanos project were highly similar in their social contexts and individual characteristics, this chapter examines whether respondents within referral pairs also mutually disclosed their HIV status and/or MSM identity. If that was the case, then it suggests that respondents within referral pairs might also have influence one another’s disclosure behaviors. Note, the focus of this chapter is not on respondents’ disclosure behaviors at the individual level, which was the focus of Chapter 5. Instead, this chapter focuses on positive similarity within referral pairs with respect to both respondents’ disclosure behaviors. That is, did respondents within referral pairs both mutually disclose their HIV status and MSM identity to members in their sexual and social networks and what might predict that mutual disclosure? Table 6.1: Type of Tie Within Referral Pairs
% Sample (n)
Type of Tie Within Referral Pairs (N = 532)
Friends
Acquaintances
Sexual partners
Relatives
Co-workers
Other ties
61.65 (328)
26.32 (140)
7.14 (38)
1.13 (6)
2.63 (14)
1.13 (6)
Of the 532 referral pairs, 62% were friends, 26% were acquaintances, 7% were sexual partners, 3% were co‐workers, 1% was relatives and 1% of referral pairs had ties 81
that were not represented in any of the above type of tie (See Table 6.1). I restricted the dyadic analyses to the most prevalent types of ties: friends, acquaintances and sexual partners. The goal is to see whether the type of tie might be associated with the mutual disclosure of the respondents within the referral pairs. Section 6.1: Homophily in Disclosure of HIV Status‐Mutual Disclosure to Specific Members in Sexual and Social Networks This section examines whether respondents within referral pairs with similar social contexts and individual characteristics also mutually disclosed their HIV statuses to sexual and social network members. Homophily in Disclosure of HIV Status to Sexual Partners Of all the various social contexts characteristics, only similarity in the receipt of social support was associated with mutual disclosure of HIV status to main sexual partners. That is, referral pairs with similar levels of support had increased odds of both respondents disclosing their HIV status to their respective main sexual partners. However, this association only remained marginally significant at the multivariate level. Referral pairs with the same HIV status (either negative or positive) had 4.50 times in the odds that both respondents mutually disclose their status to their respective last UAS partners. 82
Table 6.2: Bivariate Associations Between Similar Social Contexts and Individual Characteristics, Type of Tie and Mutual Disclosure of HIV Status To
Specific Network Member
Dependent Variables (Odds Ratios):
Mutual Disclosure of HIV status
Mutual Disclosure of HIV-Positive Status To…
To…
Main sex
Last UAS
Last PAS
Mother
Father
Brother
Sister
Straight
Gay
Priest
Doctor
Similar Social Context
partner
Partner
Partner
Friends
Friends
Characteristics
Emotional Closeness
Last UAS partner
0.96
Last PAS partner
1.41
Mother
0.51
Father
4.59
Brother
1.86
Sister
2.40*
Straight friends
2.20
Gay friends
2.26
Priest
0.28
Doctor
3.32*
Social Support
Overall Social Support Received
32.11**
0.44
0.55
0.95
0.02*
0.21
0.60
2.16
3.46
0.70
0.80
Size of MSM Community
Size of overall MSM network
0.66
2.99
2.80
0.40
0.42
0.80
0.51
0.50
0.52
0.41
0.45
Size of Latino MSM network
1.54
2.18
2.32
0.74
0.27
2.19
0.89
0.64
0.51
0.11
0.27**
Community Integration
Overall Latino community
0.33
1.34
2.10
1.22
1.73
2.51
0.72
3.09
0.37*
1.15
1.15
Latino gay community
1.30
1.01
1.62
0.57
1.52
0.88
1.03
13.47**
1.12
0.22
2.93*
Larger white gay community
0.78
1.47
1.72
2.49
6.25
3.57**
3.37**
2.26
1.35
1.02
5.51**
Similar Individual Characteristics
Age
0.48
0.05
0.48
0.17
0.02
35.90
3.36
12.84
0.08
<0.01**
4.30
Income
11.44
4.32
1.46
129.79**
124.04
16.98
3.76
0.50
6.43
2.51
1.19
Education
3.30
0.22
0.89
0.99
4.39
2.51
0.52
0.65
1.64
2.53
1.06
Place of Birth
1.32
1.08
0.77
1.06
0.57
1.53
0.91
0.67
0.86
1.59
1.05
Level of Acculturation
2.64
2.72
0.65
0 .69
0.73
1.42
1.16
1.62
1.14
0.24
2.02
Sexual Orientation
§§§
2.43
0.98
~~~
~~~
~~~
2.46
~~~
8.11*
~~~
0.54
Reported HIV Status
1.23
4.50**
1.87
Type of Tie Between Referral Pairs
0.71
1.32
0.97
0.47**
0.32*
0.67
0.77
0.80
1.74*
2.49
0.94
Friends
1.13
0.54
0.67
1.86
1.20
1.05
0.99
1.11
0.51**
0.51
1.10
Acquaintances
2.50
1.32
2.29
1.99
8.95**
3.73**
3.19*
1.71
1.52
¶¶¶
0.87
Sexual Partners
*p-value < 0.10
§§§ Disagreement in sexual orientation predicted disclosure
perfectly
**p-value < 0.05
¶¶¶ Type of tie that was not sexual partners predicted failure in mutual disclosure
~~~ Disagreement in sexual orientation predicted failure to disclose perfectly
€€€ Observations dropped due to collinearity
83
The type of tie within referral pairs was not associated with mutual disclosure of HIV status to sexual partners. Homophily in Disclosure of HIV‐Positive Status to Social Network Members At the interpersonal level, similarities in the level of emotional closeness to social network members and receipt of social support were not associated with increased odds of mutual disclosure of HIV‐positive status to social network members. This held true at both the bivariate and multivariate level of analyses. Referral pairs who were similarly integrated in the Latino gay community had 13.47 times in the odds that both respondents mutually disclosed their HIV‐positive status to their straight friends. Referral pairs who were similarly integrated in the larger white gay community had 3.57 and 3.37 times the odds of mutually disclosing their HIV‐positive status to their brothers and sisters, respectively. Interestingly, referral pairs who were similarly integrated in the larger white gay community had 5.51 times the odds of mutually disclosing their HIV‐positive status to their doctors who were not treating them for their HIV. At the multivariate level, referral pairs had 6.61 times the odds of mutual disclosure to their doctors. Size of overall and Latino MSM networks were not associated with mutual disclosure of HIV‐positive status at the bivariate level. However, referral pairs with similar size of Latino MSM networks had 14.05 times in the odds that both respondents 84
mutually disclosed their HIV‐positive status to their brothers at the multivariate level. Likewise, referral pairs who were similarly integrated in the overall Latino community had 7.97 times in the odds of mutually disclosing to their brothers at the multivariate level. For the most part, the type of tie within referral pairs was not associated with increased odds of mutual disclosure of HIV‐positive status to social network members. However, referral pairs who were sexual partners had 8.95 and 3.73 times in the odds of disclosing to their fathers and brothers, respectively. At the multivariate level with sexual partners as the comparison group, neither friends nor acquaintances had increased odds of mutual disclosure of their HIV‐positive status. 85
Table 6.3: Multivariate Associations Between Similar Social Contexts and Individual Characteristics, Type of Tie and Mutual Disclosure of HIV Status
To Specific Network Member
Dependent Variables (Odds Ratios):
Similar Social Context Characteristics
Mutual Disclosure of HIV status
To….
Main
Last UAS
Last PAS
partner
Partner
Partner
(N = 92)
(N = 86)
(N = 117)
Mutual Disclosure of HIV-Positive Status To…
Mother
(N = 87)
Brother
(N = 130)
Sister
(N = 124)
Straight
Friends
(N = 135)
Gay
Friends
(N = 141)
Doctor
(N = 137)
Emotional Closeness
Last UAS partner
Last PAS partner
Mother
Father
Brother
Sister
Straight friends
Gay friends
Priest
Doctor
Social Support
Overall Social Support Received
Size of MSM Community
Size of overall MSM network
Size of Latino MSM network
Community Integration
Overall Latino community
Latino gay community
Larger white gay community
Similar Individual Characteristics
Age
Income
Education
Place of Birth
Level of Acculturation
Sexual Orientation
Reported HIV Status
Type of Tie Between Referral Pairs
(Sexual Partners)
Friends
Acquaintances
1.72
0.94
0.54
1.59
2.29
1.34
4.17*
3.66
13.64*
0.79
0.43
0.07
0.09
0.65
2.71
11.86*
0.30
0.19
1.25
3.00
1.46
7.04
0.99
0.03**
2.31
0.08**
14.05**
0.28
2.70
0.17
2.54
1.38
0.38
1.68
0.20
0.11**
1.72
0.69
1.14
0.53
2.22
1.68
2.03
3.77
1.26
0.26
1.83
7.97**
0.31
1.76
0.68
0.95
1.31
0.74
7.18*
1.91
0.09**
0.64
0.79
0.45
1.58
6.61**
0.23
6.38
2.36
0.85
2.38
€€€
1.47
0.05
9.23
0.13
0.95
5.92
~~~
7.85*
6.90
0.50
1.46
1.61
0.22
~~~
3.18*
<0.01
66338.35**
0.65
0.54
2.42
€€€
70.21
4.04
2.12
3.01*
1.26
~~~
1.77
5.37
0.38
1.05
0.58
~~~
3.27
0.37
1.11
0.91
1.58
~~~
0.09
135.40**
0.57
0.82
0.24
§§§
112.59
11.63
0.98
1.30
0.79
§§§
0.60
0.69
0.92
0.34
0.27*
0.15**
0.15
0.62
0.69
0.63
0.34
0.36
0.61
0.89
0.74
0.34
1.81
1.73
*p-value < 0.10
§§§ Disagreement in sexual orientation predicted disclosure perfectly
**p-value < 0.05
~~~ Disagreement in sexual orientation predicted failure to disclose perfectly
€€€ Observations dropped due to collinearity
86
Homophily in Disclosure of MSM Identity to Social Network Members Similarities in the levels of emotional closeness to social network members, receipt of social support and size of overall and Latino MSM networks were not associated with mutual disclosure of MSM identity within referral pairs. Referral pairs who were similarly integrated in the Latino gay community were more likely to disclose to their gay friends. At the bivariate level, referral pairs had 2.44 times in the odds of both respondents mutually disclosing their MSM identity to their gay friends. At the multivariate level, referral pairs had 2.76 times in the odds of disclosure to their gay friends. Referral pairs who similar levels of acculturation had had 4.36 times in the odds of both respondents mutually disclosing to their sisters and 3.45 times in the odds of mutual disclosure to straight friends. Referral pairs who were sexual partners had 5.18 and 2.42 times in the odds of mutual disclosure of their MSM identity to their fathers and straight friends, respectively. However, at the multivariate level, using sexual partners as the comparison group, friends and acquaintances did not have increased odds of mutual disclosure of their MSM identity to the social network members. Referral pairs who were acquaintances had 2.18 times in the odds of mutual disclosure of their MSM identity to their doctors. 87
Table 6.4: Bivariate Associations Between Similar Social Contexts and Individual Characteristics, Type of Tie
and Mutual Disclosure of MSM Identity To Specific Network Member
Dependent Variables (Odds Ratios):
Mutual Disclosure of MSM Identity To Specific Member
Mother
Father
Brother
Sister
Straight
Gay
Priest
Similar Social Context
Friends
Friends
Characteristics
Emotional Closeness
Mother
0.66
2.69
Father
1.20
Brother
2.03*
Sister
Straight friends
0.87
Gay friends
1.30
Priest
0.89
Doctor
Social Support
Overall Social Support Received
0.44
0.76
2.23
0.04**
0.56
0.82
4.14
Size of MSM Community
0.28*
Size of overall MSM network
0.49
0.38*
0.31**
0.55
0.67
0.71
0.32
Size of Latino MSM network
0.32**
0.36**
0.31**
0.29**
0.63
0.07**
Community Integration
Overall Latino community
1.03
0.56
0.88
0.65
1.78
0.49*
0.86
Latino gay community
1.49
0.67
1.28
1.82
2.10*
2.44**
0.15
Larger white gay community
1.34
1.08
0.85
1.16
0.86
0.96
1.11
Similar Individual Characteristics
Age
0.84
2.93
1.14
2.33
1.16
1.14
<0.01**
Income
0.82
0.25
1.61
0.93
0.36
0.68
9.24
Education
2.85
1.46
2.15
1.89
2.27
0.84
0.52
Place of Birth
1.38
1.52
1.15
0.95
1.12
0.99
2.60
Level of Acculturation
3.13*
1.51
3.78
4.36**
3.45**
1.01
0.51
Sexual Orientation
1.01
§§§
1.83
2.93
0.94
1.23
~~~
Reported HIV Status
1.02
0.76
1.15
1.94*
1.43
1.15
2.16
Type of Tie Between Referral Pairs
0.84
0.28**
0.65
1.08
0.83
0.90
0.60
Friends
1.18
1.74
1.58
0.73
0.86
1.07
2.39
Acquaintances
1.08
5.18**
1.09
1.67
2.42**
1.17
¶¶¶
Sexual Partners
Doctor
2.40**
0.96
0.58
0.44**
0.62
1.52
1.27
1.24
3.73
0.52
1.03
2.52**
0.58
2.29**
0.51**
2.18**
1.03
*p-value < 0.10
~~~ Disagreement in sexual orientation predicted failure to disclose perfectly
**p-value < 0.05
¶¶¶ Type of tie that was not sexual partners predicted failure in mutual disclosure
88
Table 6.5: Multivariate Associations Between Similar Social Contexts and Individual Characteristics, Type of Tie
and Mutual Disclosure of MSM Identity To Specific Network Member
Dependent Variables (Odds Ratios):
Mutual Disclosure of MSM Identity To Specific Member
Mother
Father
Brother
Sister
Straight
Gay
Doctor
Similar Social Context
(N = 187) (N = 105) (N = 221)
(N = 211)
Friends
Friends
(N = 219)
Characteristics
(N = 266)
(N = 279)
Emotional Closeness
Mother
Father
Brother
Sister
Straight friends
Gay friends
Priest
Doctor
Social Support
Overall Social Support Received
Size of MSM Community
Size of overall MSM network
Size of Latino MSM network
Community Integration
Overall Latino community
Latino gay community
Larger white gay community
Individual Characteristics
Age
Income
Education
Place of Birth
Level of Acculturation
Sexual Orientation
Reported HIV Status
Type of Tie Between Referral Pairs
(Sexual Partners)
Friends
Acquaintances
*p-value < 0.10
**p-value < 0.05
0.70
6.44
1.02
(0.98)
2.14
0.58
1.52
1.88
2.36
0.03
0.35
0.14*
0.44
1.54
0.58
2.58
0.11**
0.69
0.10
0.54
0.77
0.38
0.96
2.05
0.22**
1.19
0.66
0.45
0.57
1.66
0.82
3.56*
0.96
0.12
0.15
1.37
0.76
0.69
0.51
1.53
1.48
2.51
1.32
1.15
0.21**
2.76**
0.89
0.35*
1.63
1.09
0.95
1.94
1.80
0.53
8.01**
1.71
1.32
0.09
0.96
19.74
1.39
5.95
~~~
5.56
1.65
4.36
3.03
0.64
4.54
~~~
1.14
1.08
1.17
1.77
0.84
3.72
~~~
2.02
0.50
0.38
2.58
0.72
2.32
2.15
1.13
0.17
1.25
0.61
1.08
0.92
0.82
1.29
0.98
23.21**
0.27*
0.90
2.48
0.56
1.45
0.69
1.91
0.18
0.63
0.90
1.90
0.48
0.56
0.12**
0.14**
0.59
0.62
0.63
0.65
~~~ Disagreement predicted failure to disclose perfectly
¶¶¶ Type of tie that was not sexual partners predicted failure in mutual
disclosure
89
Section 6.2: Discussion and Conclusion Similarities do not necessarily equate to influence, at least in the disclosure of HIV status to sexual partners. Similarities in social contexts and individual characteristics did not lead respondents who referred each other to the study to disclose their HIV status to their sexual partners in similar ways. However the type of tie between referral pairs did influence their disclosure behaviors. Compared to acquaintances, referral pairs who were sexual partners had increased odds that both respondents disclosed to their last PAS partners. It might very well be that these respondents disclosed their HIV statuses to each other. Referral pairs did influence one another’s disclosure of HIV‐positive status to their doctors and brothers. Referral pairs who were similarly integrated in the larger white gay community had increased odds of both mutually disclosing their HIV‐
positive status to their doctors. This is in juxtaposition with the findings from the previous chapter where community integration did not play a role in respondents’ disclosure of their HIV‐positive status to their doctors. In addition, referral pairs with similar sizes of Latino MSM networks and who were similarly integrated in the overall Latino community had increased odds of both respondents mutually disclosing their HIV‐positive status to their brothers. Again, in the previous chapter, we found that size of Latino MSM networks and community integration in the overall Latino community were not associated with HIV‐positive status disclosure to brothers. 90
With respect to MSM identity disclosure, referral pairs seemed to influence each other’s behaviors to their gay friends and mothers. Referral pairs who were similarly integrated in the Latino gay community had increased odds of both respondents mutually disclosing their MSM identity to their gay friends. In addition, referral pairs who were similarly acculturated had increased odds of both respondents mutual disclosing to their mothers. Of note is that in the previous chapter, the extent of respondents’ integration in a Latino gay community was not associated with increased odds of disclosure of MSM identity to gay friends. In addition, acculturation was not significantly associated with MSM identity disclosure to mothers. 91
Chapter 7: Conclusions and Discussion In this section, I discuss the limitations of the dissertation and then conclude by summarizing the findings and discussing the implications for intervention design. Section 7.1: Limitations This dissertation has several limitations. First, I took a liberal approach to the dyadic analyses in the sense that respondents can be both senders and receivers. This is because in the framework of RDS, respondents who were referred to the Brothers Y Hermanos project can in turn refer other respondents to the project. The reason I took the liberal approach to the dyadic analyses was to maximize the number of referral pairs in the sample. However, one can also take a more conservative approach to the dyadic analyses whereby respondents can only be either senders or receivers but not both. This approach will reduce the number of referral pairs in the sample and might yield different, possibly more reliable, results. Second, this dissertation utilized cross‐
sectional data rather than longitudinal data in its analyses. As such, rather than establishing causality, only associations can be drawn between social contexts and individual characteristics and disclosure of HIV status and MSM identity. Third, this dissertation is exploratory in nature, aiming to describe the broad range of associations found in bivariate analyses rather than the limited set of associations found in more confirmatory multivariate analyses. Further, additional studies are needed to determine the content of HIV interventions that promote disclosure behaviors. 92
Section 7.2: Summary of Findings and Implications Further research will be required to recommend the specific content of disclosure interventions. However, findings from this dissertation will have relevance for the design of those HIV interventions. Respondents who referred each other to the Brothers Y Hermanos project were highly similar with respect to their individual characteristics and the social contexts in which they were embedded. Furthermore, referral pairs also mutually disclosed their HIV status and MSM identity to sexual and social network members. The extent of similarities within referral pairs was highest with respect to their individual characteristics (age, SES, ethnic identity, and HIV risk characteristics), ranging from 72% to 93%. The extent of similarities in social contexts characteristics (emotional closeness, social support, size of MSM networks, and community integration) ranged from 56% to 75%. Referral pairs were less similar with respect to their disclosure behaviors. Similarity in disclosure of HIV statuses to sexual partners ranged from 24% to 51%. Referral pairs had most similarity with disclosure to gay friends with respect to their HIV‐positive status and MSM identity (more than 60% in both instances). With respect to disclosure to the remaining social network members, similarity in disclosure of HIV‐positive status and MSM identity ranged from 2% to 36%. However, there was no statistical or meaningful difference in disclosure behaviors within referral pairs. The high homophily within referral pairs suggests that there was not much segmentation 93
among Latino MSM with respect to these characteristics. Interventions targeting Latino MSM should target this community as a whole, rather than subgroups within it. However, connection and similarity within referral pairs did not necessarily equate to possible influence, measured by associations between similarity in individual and social contexts and mutual disclosure behaviors. Disclosure of HIV status and MSM identity remained highly individualistic behaviors, dependent on the target of disclosure (sexual partners, parents, siblings, friends, or community members), and the respondents’ individual characteristics that embedded them in various social contexts that facilitated or impeded disclosure of their HIV status and MSM identity. Therefore, HIV interventions should be cognizant of the individualistic nature of disclosure behaviors. More respondents reported feeling very close to their mothers, sisters, and gay friends than to other members in their social and sexual networks. However, none of the respondents’ individual characteristics were associated with their closeness to their mothers and sisters, suggesting that these network members may represent a source of stability to the respondents regardless of whom they were. However, not many respondents disclosed to their mothers about their HIV‐positive status or their MSM identity. This suggests that while respondents were close to their mothers, they might fear rejection and disapproval from them. This might have been reflected in the finding that more than half of the respondents reported feeling isolated and alone and not 94
having anyone who understands their private worries and fears, which might very well be their HIV‐positive status or MSM identity. More respondents disclosed their HIV‐positive status and MSM identity to their sisters and gay friends. However, the motivations for respondents’ disclosure to their sisters seemed to be quite different from their motivations to disclose to their gay friends. In both cases of disclosure of HIV‐positive status and MSM identity, respondents disclosed to their sisters to whom they were closer. This suggests that the strength of tie between respondents and their sisters was key in their disclosure decisions. On the other hand, though more respondents disclosed to their gay friends than to anyone else in their social networks, their disclosure behaviors were not dependent on the extent of closeness they felt towards their gay friends. This suggests that the strength of tie was not key in disclosure to these network members. The rates of disclosure of HIV‐positive status and MSM identity to doctors were high even though not many respondents reported feeling very close to these members. However, the motivations for disclosure in each case were divergent. Respondents disclosed their HIV‐positive status to their doctors whom they were emotionally closer. This is of note considering that these doctors were not treating respondents for their HIV. However, emotional closeness did not play a role in the disclosure of MSM identity. This suggests that respondents may view their MSM identity as something private while their HIV status not necessarily so. 95
Community level characteristics (size of overall and Latino MSM networks, and integration in the overall Latino community, the Latino gay community and the larger white gay community) were associated with disclosure of HIV‐positive status and MSM identity at the bivariate level but not at the multivariate level, with two exceptions. Respondents with larger overall MSM networks were more likely to disclose to their priests. However, respondents with larger Latino MSM networks were less likely to disclose to their priests. Second, respondents who were more integrated in the overall Latino community were less likely to disclose their MSM identity to their brothers. This suggests that there might be a stigmatizing effect with respect to HIV‐positive status and MSM identity in the Latino community. HIV interventions should address (or at least consider) the possible stigma found in the Latino community. Disclosure of HIV status to sexual partners (main sexual partner, last UAS and PAS partners) is considered separately as it involved disclosure of both HIV‐positive and HIV‐negative statuses. However, as was the case with many social network members, respondents disclosed to their sexual partners to whom they were emotionally closer. Of note is that respondents were more likely to disclose if they were more integrated in the larger white gay community. This suggests that the larger white gay community might be more open about the issue of HIV/AIDS, thus facilitating disclosure of HIV status. 96
As mentioned previously, there was no evidence against homophily within referral pairs with respect to disclosures of HIV status and MSM identity. In other words, if the respondent disclosed his HIV status and/or MSM identity to members of his sexual and social networks, it was likely that the person he referred to the study also disclosed his HIV status and/or MSM identity to that member. However, for the most part, similarities in social contexts were not associated with referral pairs mutually disclosing their HIV status or MSM identity. There might have been possible influence on one another’s disclosure behaviors within referral pairs at the community level (specifically the extent of community integration). Referral pairs who were similarly integrated in the larger white gay community had increased odds of both respondents mutually disclosing their HIV‐
positive status to their doctors. Likewise, referral pairs who were similarly integrated in a Latino gay community had increased odds of both respondents disclosing their MSM identity to their gay friends. Furthermore, referral pairs who were sexual partners had increased odds of mutually disclosing their HIV‐positive status to their fathers, brothers, and sisters. With regards to MSM identity disclosure, referral pairs who were sexual partners had increased odds of both respondents mutually disclosing their MSM identity to their fathers and straight friends while referral pairs who were acquaintances had increased odds of mutual disclosure of their MSM identity to their doctors. Other than these few significant associations, no other similarities in social contexts and 97
individual characteristics were associated with respondents within referral pairs both disclosing their HIV‐positive status and MSM identity to social network members. However, taken together, the findings suggest that referral pairs affect the norms of the communities in which they were a part which can promote disclosure. Therefore, interventions should incorporate a peer‐based component that addresses community norms. 98
References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. Rhodes F, Wolitski RJ, Thornton‐Johnson S. An experiential program to reduce AIDS risk among female sex partners of injection‐drug users. Health & Social Work. 1992;17(4):261‐272. Latkin C, Donnell D, Metzger D, et al. The efficacy of a network intervention to reduce HIV risk behaviors among drug users and risk partners in Chiang Mai, Thailand and Philadelphia, USA. Social Science & Medicine. 2009;68(4):740‐748. Kelly J, Amirkhanian Y, Kabakchieva E, et al. Prevention of HIV and sexually transmitted diseases in high risk social networks of young Roma (Gypsy) men in Bulgaria: randomised controlled trial. British Medical Journal. 2006;333(7578):1098. Amirkhanian Y, Kelly J, Kabakchieva E, et al. A randomized social network HIV prevention trial with young men who have sex with men in Russia and Bulgaria. AIDS. 2005;19(16):1897. Zhang H, Wu Z, Zheng Y, Wang J, Zhu J, Xu J. A Pilot Intervention to Increase Condom Use and HIV Testing and Counseling Among Men Who Have Sex With Men in Anhui, China. Journal of Acquired Immune Deficiency Syndromes. 2010;53:S88. McPherson M, Smith‐Lovin L, Cook J. Birds of a feather: Homophily in social networks. Annual Review of Sociology. 2001;27(1):415‐444. CDC. Advancing HIV Prevention: New Strategies for a Changing Epidemic. Morbidity & Mortality Weekly Report. 2003;52(15):329 ‐ 356. Rosser BRS, Horvath KJ, Hatfield LA, Peterson JL, Jacoby S, Stately A. Predictors of HIV disclosure to secondary partners and sexual risk behavior among a high‐risk sample of HIV‐positive MSM: results from six epicenters in the US. AIDS Care. 2008;20(8):925. Pinkerton S, Galletly C. Reducing HIV transmission risk by increasing serostatus disclosure: A mathematical modeling analysis. AIDS & Behavior. 2007;11(5):698‐705. Stirratt MJ, Remien RH, Smith A, Copeland OQ, Dolezal C, Krieger D. The role of HIV serostatus disclosure in antiretroviral medication adherence. AIDS & Behavior. 2006;10(5):483‐493. Zea MC, Reisen CA, Poppen PJ, Bianchi FT, Echeverry JJ. Disclosure of HIV status and psychological well‐being among Latino gay and bisexual men. AIDS & Behavior. 2005;9(1):15‐26. Zea MC, Reisen CA, Poppen PJ, Echeverry JJ, Bianchi FT. Disclosure of HIV‐
positive status to Latino gay menʹs social networks. American Journal of Community Psychology. 2004;33(1):107‐116. 99
13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. Ullrich PM, Lutgendorf SK, Stapleton JT. Concealment of homosexual identity, social support and CD4 cell count among HIV‐seropositive gay men. Journal of Psychosomatic Research. 2003;54(3):205‐212. County of Los Angeles Public Health HIV Epidemiology Program. HIV/AIDS Semi‐Annual Surveillance Summary. January 2010.1 ‐ 34. McLeroy KR, Bibeau D, Steckler A, Glanz K. An ecological perspective on health promotion programs. Health Education & Behavior. 1988;15(4):351. Smith A, Grierson J, Wain D, Pitts M, Pattison P. Associations between the sexual behaviour of men who have sex with men and the structure and composition of their social networks. Sexually Transmitted Infections. 2004;80(6):455. Choi K, Ning Z, Gregorich S, Pan Q. The influence of social and sexual networks in the spread of HIV and syphilis among men who have sex with men in Shanghai, China. Journal of Acquired Immune Deficiency Syndromes. 2007;45(1):77‐84. Peterson JL, Rothenberg R, Kraft JM, Beeker C, Trotter R. Perceived condom norms and HIV risks among social and sexual networks of young African American men who have sex with men. Health Education Research. February 1, 2009 2009;24(1):119‐127. Stein MD, Freedberg KA, Sullivan LM, et al. Sexual Ethics: Disclosure of HIV‐
Positive Status to Partners. Archives of Internal Medicine. February 9, 1998 1998;158(3):253‐257. Varga C, Sherman G, Jones S. HIV‐disclosure in the context of vertical transmission: HIV‐positive mothers in Johannesburg, South Africa. AIDS Care. 2006;18(8):952‐960. Gorbach P, Galea J, Amani B, et al. Don’t ask, don’t tell: patterns of HIV disclosure among HIV positive men who have sex with men with recent STI practising high risk behaviour in Los Angeles and Seattle. Sexually Transmitted Infections. 2004;80(6):512. Zea MC, Reisen CA, Poppen PJ, Bianchi FT, Echeverry JJ. Predictors of disclosure of human immunovirus‐positive serostatus among Latino gay men. Cultural Diversity & Ethnic Minority Psychology. 2007;13(4):304‐312. Serovich J, Esbensen A, Mason T. HIV disclosure by men who have sex with men to immediate family over time. AIDS Patient Care & STDs. 2005;19(8):506‐
517. Serovich J, Esbensen A, Mason T. Disclosure of positive HIV serostatus by men who have sex with men to family and friends over time. AIDS Patient Care & STDs. 2007;21(7):492‐500. 100
25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. Fekete E, Antoni M, Lopez C, et al. Menʹs serostatus disclosure to parents: Associations among social support, ethnicity, and disease status in men living with HIV. Brain, Behavior, & Immunity. 2009;23(5):693‐699. Boon S, Miller R. Exploring the links between interpersonal trust and the reasons underlying gay and bisexual malesʹ disclosure of their sexual orientation to their mothers. Journal of Homosexuality. 1999;37(3):45‐68. Klitzman R. Self‐disclosure of HIV status to sexual partners: a qualitative study of issues faced by gay men. Journal of the Gay & Lesbian Medical Association. 1999;3(2):39‐49. Reich W, Lounsbury D, Zaid‐Muhammad S, Rapkin B. Forms of social support and their relationships to mental health in HIV‐positive persons. Psychology, Health & Medicine. 2010;15(2):135‐145. Sherbourne C, Stewart A. The MOS social support survey. Social Science & Medicine. 1991;32(6):705‐714. House J, Kahn R. Measures and concepts of social support. Clinical Psychology. 1985;42:802‐811. Schwarzer R, Leppin A. Social support and health: A theoretical and empirical overview. Journal of Social & Personal Relationships. 1991;8(1):99. Kalichman S, DiMarco M, Austin J, Luke W, DiFonzo K. Stress, social support, and HIV‐status disclosure to family and friends among HIV‐positive men and women. Journal of Behavioral Medicine. 2003;26(4):315‐332. Wohl A, Galvan F, Myers H, et al. Social Support, Stress and Social Network Characteristics Among HIV‐Positive Latino and African American Women and Men Who have Sex with Men. AIDS & Behavior. 2010:1‐10. Persson L, Östergren P, Hanson BS, Lindgren A, Naucler A. Social network, social support and the rate of decline of CD4 lymphocytes in asymptomatic HIV‐positive homosexual men. Scandinavian Journal of Public Health. 2002;30(3):184‐190. George S, Garth B, Wohl A, Galvan F, Garland W, Myers H. Sources and Types of Social Support that Influence Engagement in HIV Care among Latinos and African Americans. Journal of Health Care for the Poor & Underserved. 1999;20(4). Fergus S, Lewis M, Darbes L, Butterfield R. HIV risk and protection among gay male couples: The role of gay community integration. Health Education & Behavior. 2005;32(2):151. Rosario M, Hunter J, Maguen S, Gwadz M, Smith R. The coming‐out process and its adaptational and health‐related associations among gay, lesbian, and bisexual youths: Stipulation and exploration of a model. American Journal of Community Psychology. 2001;29(1):133‐160. 101
38. 39. 40. 41. 42. 43. Joseph KM, Adib SM, Joseph J, Tal M. Gay identity and risky sexual behavior related to the AIDS threat. Journal of Community Health. 1991;16(6):287‐297. Heckathorn DD. Respondent‐Driven Sampling II: Deriving Valid Population Estimates from Chain‐Referral Samples of Hidden Populations. Social Problems. 2002;49(1):11‐34. Abdul‐Quader A, Heckathorn D, Sabin K, Saidel T. Implementation and analysis of respondent driven sampling: lessons learned from the field. Journal of Urban Health. 2006;83:1‐5. Heckathorn DD. Respondent‐Driven Sampling: A New Approach to the Study of Hidden Populations. Social Problems. 1997;44(2):174‐199. Turner C, Forsyth B, O’Reilly J, et al. Automated self‐interviewing and the survey measurement of sensitive behaviors. Mick P. Couper et al., Computer Assisted Survey Information Collection. New York: Wiley. 1998:455–473. Kurth AE, Martin DP, Golden MR, et al. A Comparison Between Audio Computer‐Assisted Self‐Interviews and Clinician Interviews for Obtaining the Sexual History. Sexually Transmitted Diseases. 2004;31(12):719‐726. 102