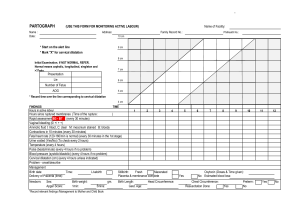
Partogram and Obstructed Labour H. Gee MD, FRCOG Consultant Obstetrician
advertisement

Partogram and Obstructed Labour H. Gee MD, FRCOG Consultant Obstetrician When is a Woman in Labour? Good Management of Labour First StagePatterns of Aberrance Patterns of Aberrance • Prolonged Latent Phase – Slow cervical dilatation before Active Phase established – 20 hrs Nullips & 14 hrs Multips • Primary Dysfunctional Labour – Progress< 1 cm/hr before Active Phase slope established – Incidence: Nullips 26%, Multips 8% • Secondary Arrest – Cessation after normal active phase dilatation – Incidence: Nullips 6%, Multips 2% PARTOGRAM- EAST AFRICA’S GIFT TO THE WORLD • • • • • • Invented in Africa 1960’s Identify delay Identify increasing risk To determine place of delivery No comparative or controlled trials Common sense value recognised Cervical Dilatation (cms,) Active Phase Cervicograms - Philpott & Castle 10 8 6 4 2 0 2 4 6 8 10 Time (hrs.) WHO Partograph Study • Reduced incidence of prolonged labour (8.3% vs 4.5%) • Decreased need for augmentation (32% vs 13%) • Increased spont vag del (74% vs 78%) • Decreased caesarean section (9.8% vs 6.8%) * * not Statistically Sig Lancet 1994 343;1399-1404 (Nullips) Why not done? Result from Malawi audit Partograph assessment by progress of labour and augmentation, by type of facility Results from Malawi audit Second Stage • Descent • Rotation • Duration – Passive – Active(Pushing) Current situation • Midwife tells you CS needed – Problems • Is she right? • Do you understand the problem & implications. • Are there alternatives? – e.g. forceps/vacuum in second stage New situation • You are team leader because of this course – When called • You assess patient – Power/passages /passenger – You improve care by whole team Parity & Obstruction • Nulliparous – Inertia • Multiparous – Uterine Rupture COMPONENTS OF LABOUR • The powers Uterine contractions • The passages bony pelvis, and soft tissues • The passenger fetus Powers • Essential for good progress – Cervical Dilatation – Flexion – Rotation • Assessed by Palpation – Frequency 3-5 in 10 min. • Augmented by Oxytocin & Amniotomy The Passages • Bony pelvis – Absolute cephalo-pelvic disproportion • Kyphosis, Scoliosis, poliomyelitis, maternal dwarfism, ricketts, pelvic fracture. • Soft tissue • fibroids, ovarian tumour, pelvic kidney, fat, cervical stenosis, cervical cancer, vaginal\vulval atresia, vaginal septum. The Passages Disproportion • Head Not Engaged – > 4/5 Palpable abdominally – VE: high head, caput+++, moulding+++ • CS essential • PPH – Risk increased in Prolonged/Obstructed labour The Passenger-1 – Large Fetus • Idiopathic – Increasing Parity • Pathologic macrosomia, – diabetes • Fetal abnormalities – hydrocephalus – conjoined twins – hydrops fetalis The Passenger-2 • Malposition – Occipito-Posterior – Mento-Posterior • Malpresentation • • • • compound presentations shoulder brow face Signs of Obstruction • Maternal – Tachycardia – Pyrexia – Ketosis – Dehydration • Fetal – Fetal heart rate abnormalities Treatment • General – Re-hydration – Anti-biotics (if infection suspected) • Specific – According to diagnosis • Caesarean section Caesarean Section in Obstruction • Cesarean Section Problems – Impacted head – dis-impact before start – PPH • IV sytno/ergometrine/misoprostol ready – Bladder Injury • Leave catheter in for 10 days if blood stained – Infection • IV antibiotics Post delivery • Reflective practise- team leader • Critical incident review – WHY Poor Outcome? • • • • NO TRAINING NO EQUIPTMENT POOR COMMUNICATION MATERNAL HEALTH VERY POOR Improve Partogram Use • 4 hourly ward rounds/teaching • Critical incident review – What was wrong? • Audit • Change • Re-audit