Globalisation, privatisation and healthcare – a preliminary report
advertisement

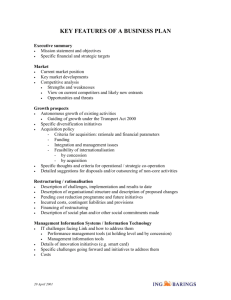
Public Services International Research Unit (PSIRU) 2001-01-H-Over Globalisation, privatisation and healthcare – a preliminary report by David Hall, Senior Research Fellow, PSIRU, University of Greenwich January 2001 This report was commissioned by Public Services International Comments on this paper, especially from PSI affiliates, are welcomed at psiru@psiru.org . Public Services International Research Unit (PSIRU) School of Computing and Mathematical Sciences, University of Greenwich 30 Park Row, London SE10 9LS, U.K. Email: psiru@psiru.org Tel: +44-(0)208-331-9933 Fax: +44 (0)208-331-7781 www.psiru.org Director: David Hall Researchers: Kate Bayliss, Steve Davies, Emanuele Lobina, Sam Weinstein The PSIRU was set up in 1998 to carry out empirical research into privatisation, public services, and globalisation. It is part of the School of Computing and Mathematics in the University of Greenwich, London. PSIRU’s research is centred around the maintenance of an extensive and regularly updated database of information on the economic, political, financial, social and technical experience with privatisation and restructuring of public services worldwide. This core database is financed by Public Services International (PSI), the worldwide confederation of public service trade unions. www.world-psi.org © Unless otherwise stated, this report is the copyright of the PSIRU and the organisations which commissioned and/or financed it Healthcare 29/05/16 Executive summary Abbreviations 3 4 1. Globalisation, privatisation and public services 1.1 Globalisation and public services Privatisation and internationalisation (see also Annexe A) 1.2 The channels of globalisation 5 5 5 6 2. The WTO threat to public services 2.1 WTO – the potential impact of GATS 2.2 GATS exemptions – government services and procurement 2.3 TRIPS 6 6 7 7 3. The influence of other international institutions 3.1 IMF and World Bank: general conditionality 3.2 World Bank –IBRD projects Tanzania Indonesia Bulgaria 3.3 World Bank: International Finance Corporation (IFC) Russia Dominican republic Brazil Nigeria India 3.4 World Bank: Multilateral Investment Guarantee Agency (MIGA) 3.5 Other international organisations and treaties WHO OECD Energy charter treaty Regional trade zones: NAFTA, Mercosur, Asean, EU 3.6 Public procurement 7 7 7 8 8 8 8 9 9 9 9 9 9 10 10 10 10 10 11 4. Governments and multinationals 4.1 Government decisions 4.2 Managed care schemes 4.3 The problem of trade unions 4.4 MNCs’ marketing - the annual global conference 11 11 12 12 12 5. The multinational companies 5.1 Insurance multinationals 5.2 Hospital multinationals 5.3 Clinical, laboratory and other services 5.4 Support services multinationals 13 13 14 14 15 6. Observations 6.1 Globalisation 6.2 Multinationals 15 15 16 Annexe A: Comments on privatisation/internationalisation chart 17 Annexe B: Current World Bank projects involving healthcare 18 _____________________________________________________________________________ PSIRU www.psiru.org Page - 2 - Healthcare 29/05/16 Executive summary The paper distinguishes between globalisation, which may have a negative development impact in any sector, and privatisation, which specifically damages public services. Various channels are identified of globalisation influencing the privatisation of healthcare, including international institutions, government policies, and the activities of multinationals themselves. The WTO provides two kinds of threat to health services. The first is the potential threat of GATS, which could force more privatisation in future. The second is the effect of TRIPS in supporting pharmaceutical profits at the expense of health needs. The World Bank has a major impact on privatisation of healthcare services through its projects, which often have greater privatisation as a stated objective. Other parts of the World Bank also support privatisation: the direct investment activities of the IFC, and the investment guarantees of MIGA. Other international organizations such as the WHO and OECD also influence privatisation. The various regional trade zones of the world have rules which may facilitate privatisation: healthcare policy changes in Alberta Canada, for example, could become a ‘one-way street towards privatisation of the health sector’ because of NAFTA. Procurement rules can also affect the introduction of private capital into public services. Government decisions to introduce healthcare privatisation have been and are being made in a number of developed and developing countries. These include service provision and also privatised insurance schemes like HMOs. The marketing activities of MNCs themselves are central to the processes of privatisation and globalisation. This marketing may involve international agencies and governments, as at the annual AIHS conference. The main multinationals active in health so far are listed in four categories: insurance, hospitals, clinical/labs etc, support services. Some general comments can be made from this preliminary review: The World Bank is a very significant force driving privatisation in healthcare, both through projects, investments, and institutional support for the multinationals. WTO and GATS provide a threatening background against which privatisation in one form or another is already happening in a wide range of countries . Trading and procurement rules of organisations like NAFTA and the EU may impact on privatisation of public services. The picture of multinational behaviour by private healthcare companies is not as coherent or as expansionist as in other sectors. Many of the USA groups are weak internationally The private hospital companies have not been very successful so far at expanding internationally. Cleaning and catering support services exhibit the ‘classic’ pattern of multinational dominance worldwide, at least in developed countries. The insurance companies, as insurers or with HMO schemes, are also expanding. There is multinational expansion in clinical diagnostic or therapy services, such as dialysis, blood products, MRI scans, in a number of countries _____________________________________________________________________________ PSIRU www.psiru.org Page - 3 - Healthcare 29/05/16 There is little sign of vertical integration of private healthcare companies, or of any consistent synergies with other services. Privatisation of services may be established first before globalisation Abbreviations EU GATS HMO IBRD IFC IMF MIGA MNC MRI NAFTA OECD PFI PPP TRIPS WHO WTO European Union General Agreement on Trade in Services Health management organisation (managed care) International Bank for Reconstruction and Development (‘core’ part of World Bank) International Finance Corporation (part of World Bank) International Monetary Fund Multilateral Investment Guarantee Agency (part of World Bank) Multinational company magnetic resonance imaging North American Free Trade Agreement Organisation for Economic Cooperation and Development Private Finance Initiative (UK) Public private partnership Trade-Related Aspects of Intellectual Property Rights World Health Organisation World Trade Organisation _____________________________________________________________________________ PSIRU www.psiru.org Page - 4 - Healthcare 29/05/16 1. Globalisation, privatisation and public services 1.1 Globalisation and public services There are many issues connected with globalisation and its impact especially on developing countries. These include economic development in general, development of national industries, exporting of profits, labour conditions, environmental impacts, and erosion of power of democratic institutions. This paper is concerned with the impact on public services in general, and health services in particular. In most sectors - e.g. agriculture, extraction, production and service industries - the problem of globalisation, in the sense of opening up these sectors to foreign capital, is its threat to national development. This problem is significant whether the industry is in local private or public hands, whether privatisation is an issue or not. The worst effects of globalisation on public services - e.g. health, education, water, energy – on the other hand are specifically connected with privatisation: either through limiting social and economic solidarity in the financing of services, so undermining the basic principle of public services; or privatisation of service provision - once services such as health, education, transport, water, energy, waste management have been privatised, the provision is dictated by the requirements of profits. Whether the private companies involved are national or foreign is arguably a less important issue for public services than the impact of privatisation on financing or service provision. For example, UK rail privatisation is just as much of a problem in the hands of a UK-owned company like Railtrack or Virgin as in the hands of a foreign-owned multinational like Vivendi. The same can be said in developing countries the privatisation of support services in Malaysian hospitals to a Malaysian-owned company does as much damage to the public service as if it had been privatised to a multinational. There may still be negative development consequences of globalisation in these services, from the entry of foreign capital, but the distinctive damage to public services happens through privatisation. The chart attempts to illustrate these distinctions. It presents a categorization of providers according to the corporate form, the sector in which they are owned, and whether they are nationally or internationally based. It can be used to identify various structural changes. For comments on the different elements in this chart, see Annexe A. Privatisation and internationalisation (see also Annexe A) Public WHO, World Bank 2. International D Munic -ipal Corporatised Trusts, municipal enterprises Not-forprofit NGOs, churches, Foreign public enterprises International NGOs Private E PPPs Privatisation boundary 2 National health, universities C Privatisation boundary 1 State 1. National B Corporatisation boundary A Joint ventur es Global PPPs F Companies, PPPs National companies, partnerships Globalisatio n boundary Multinationals _____________________________________________________________________________ PSIRU www.psiru.org Page - 5 - Healthcare 29/05/16 1.2 The channels of globalisation There are a number of different channels through which the process of globalisation is driving the privatisation of public services. The most prominent at present is the role of the World Trade Organisation (WTO) and the liberalising drive of its agreement on trade in services. But the agents of change also include other international institutions – notably the international financial institutions (IFIs), the IMF and World Bank, and also bodies such as the WHO and OECD. They also include the rules of the regional trading zones, like NAFTA, or the EU, or Mercosur – these regions may already have in place trading rules and procurement rules that impact on privatisation of public services. And they include bilateral relations between countries, either through formal trade deals or through other international political relations, in which countries such as the USA may place conditions on other countries which concern privatisation or liberalisation of services. Most of all, there are the constant activities of the corporations themselves, engaging in individual and collective marketing of themselves, forming national and international political relations through a range of mechanisms including corruption and promoting both privatisation and trade liberalisation as inevitable historical trends. The various elements are not necessarily co-ordinated, and there may be contradictions between these elements. In November 2000 Suez-Lyonnaise is reported to have sounded a cautionary note about GATS at a meeting discussing the position of EU and France in pushing for further liberalisation through GATS. The company is said to have commented, “We are very careful with the terminology "liberalism". Therefore, we want to preserve the public service in the framework of the liberalisation, in the long term it is the only way we can ensure the profitability of our investment, by doing so we keep the confidence of the population in our investment and in general we know if we liberalised one sector it does not work. That is why we are developing public/private contracts." 1 Water privatisations are happening already, profitably, through agreements reached between the company and governments. An aggressive push for liberalisation of trade rules, which are not at present an obstacle in most countries, could just succeed in creating greater political opposition to the process. Finally, at the end of the chain are the decisions taken by governments to privatise or liberalise particular services. Such decisions have already been made in many countries, in healthcare as well as other services such as water, and are being discussed in others. The rest of this paper looks at some of these factors, and ends with a brief survey of internationally active healthcare companies. 2. The WTO threat to public services 2.1 WTO – the potential impact of GATS The World Trade Organisation (WTO), through the General Agreement on Trade in Services (GATS), is creating potential extra pressure for privatisation of public services, especially healthcare. There have been a number of detailed analyses of the potential impact of GATS in general 2, on health services in particular, 3 from the perspective of international trade unionism, 4 and from a development perspective.5 The key element in GATS is for countries to make ‘commitments’ to open a sector to trade. Countries are not obliged to open sectors, but can do so: a number of countries have already done so in some aspect of health services. 6 So far the impact of GATS is potential rather than actual: “the GATS is a framework agreement that is not yet in application”7. But the WTO is working to increase the sanctions for not offering to open sectors, by _____________________________________________________________________________ PSIRU www.psiru.org Page - 6 - Healthcare 29/05/16 insisting that states must prove they are not using anti-competitive policies to protect a sector: “The legal tests under consideration would outlaw the use of non-market mechanisms such as cross-subsidisation, universal risk pooling, solidarity, and public accountability in the design, funding, and delivery of public services as being anti-competitive and restrictive to trade”.8 2.2 GATS exemptions – government services and procurement At present GATS rules contain two clauses which exempt much of the public services area. The first is the direct supply of services by government, as long as the services are “supplied in the exercise of governmental authority” and “supplied neither on a commercial basis, nor in competition with one or more service suppliers”. . The second exemption – in article XIII - exempts government procurement, which includes contracts issued by public authorities for services of all kinds e.g. hospital cleaning. Between them, they mean that inhouse services and contracted-out work are so far not covered by GATS. But these exemptions have been explicitly targeted for removal or amendment by business. For example, in 1999 the European Services Network (ESN) proposed 9 that the procurement exemption should be removed: “The absence of multilateral rules for procurement is probably the most important non-tariff barrier affecting the services sector. The GATS 2000 global talks provide the right tool to improve the situation either by deleting Art. XIII of the GATS or by extending the Agreement on Government Procurement to all GATS member states.” The ESN also proposed a tightening of the exemption for direct services: “A major obstacle to the international fair competition is that public authorities try to get around public procurement regulations by using so-called "in-house services" and therefore feel that by this they are not required to follow public procurement laws. Federal, regional and local governments must be strictly advised that any body governed by public law is obliged to follow public procurement regulations. This includes …. any association formed by one or more of such authorities or bodies governed by public law…” These areas may also be subject to pressure under procurement rules of governments or trading zones, such as the EU. See below for an example of how the EU procurement regulations and provisions on concessions may threaten to extend the portion of public services which may be forced open to private sector bids. 2.3 TRIPS The Trade-Related Aspects of Intellectual Property Rights (TRIPS) agreement, which concerns international patents, is administered by the WTO, but is separate from the GATS. TRIPS can also exacerbate the problems of public services, especially in healthcare, because it reinforces the rights of patent-holders such as the pharmaceutical companies. This makes the provision of drugs more expensive than it would otherwise be – and so boosts the revenues of the pharmaceutical companies, at the expense of other healthcare expenditure, as well as making some needed medicines - notably anti-AIDS drugs, for example – prohibitively expensive.10 When South Africa and Thailand recently announced that they would grant compulsory licences to make anti-AIDS drugs at low cost, the US threatened them with trade sanctions.11 3. The influence of other international institutions 3.1 IMF and World Bank: general conditionality Structural adjustment programmes (SAPs) introduced under the IMF carry a large number of conditions. In some cases these conditions explicitly refer to the privatisation, or commercialisation of public services. In Tanzania, for example, increases in charges for healthcare and education were required as a condition of the SAPs; in Ecuador the conditions included increases in energy prices12, in Ghana water privatisation was a condition both for an IMF restructuring package and as a general condition of World Bank assistance.13 3.2 World Bank –IBRD projects Specific loans from the World Bank may involve, and be conditional upon, privatisation of the provision of the relevant services. This is now a commonplace in energy (recent examples include Uttar Pradesh in India, _____________________________________________________________________________ PSIRU www.psiru.org Page - 7 - Healthcare 29/05/16 and Kenya) and water, where loans to Palestine, Ghana, and others have required privatisation of the water service.14 The imposition of these conditions makes privatisation almost unavoidable, assuming that the country needs the World Bank loan to develop the service further. The World Bank is currently operating over 200 projects which concern healthcare: a list is attached at Annexe B 15. Many of these projects are concerned, directly or indirectly, with restructuring of the public health system, and effectively require further privatisation. Three examples illustrate the ways in which private sector involvement, or private payment principles, form part of the agenda of these projects. Tanzania The Bank has a $22m “Health Sector Development Program” Project in Tanzania which is concerned with reforming the whole health sector. It’s first stated goal, “Strengthening Service Delivery” includes improving quality and financial viability of services and will explicitly “promote private sector involvement in delivery of health services”.16 Indonesia The Provincial Health Project for Indonesia starts with the stated aim of establishing ”effective health sector decentralization” in two provinces, and includes later elements of a market-based approach including “reviewing and piloting alternative insurance approaches” and “examining tax-based and other means of generating resources for health”.17 Bulgaria The project in Bulgaria is summarised as assisting the government to restructure and improve access, quality, and financial and operational sustainability – with no overt mention of private sector involvement. 18 However, the detailed project appraisal document 19 states that in the context of the Bank’s overall programme for Bulgaria, the key areas with respect to the health sector include “putting into place an efficient and sustainable health financing regime through an effective health insurance system and an increased role for the private sector; reducing structural inefficiencies by reducing excess capacity, strengthening sector management at the central and local levels, and promoting competition among providers”. Hospitals will be corporatised not for greater efficiency, but for ultimate handover to the private sector, so the project aims: “to complete the re-registration of the health care establishments as trade companies in the light of creating opportunities for subsequent privatisation, with guaranteed preferential participation of doctors and dentists working within the health care system.” 3.3 World Bank: International Finance Corporation (IFC) The IFC is a division of the World Bank, which invests solely in the private sector. As such, IFC loans in public services are bound to be restricted to privatised ventures. The IFC has a declared policy of being simply in favour of extending the role of the private sector in public services, including healthcare. Its chief executive, Peter Woicke, declared in September 1999: “….IFC is also moving aggressively to invest in sectors where we believe there is substantial scope for more private sector involvement. This ranges from water and transportation investments to healthcare, education, and the environment. Not that we believe the private sector should replace the public sector, but private education and healthcare can and must compliment the public providers of these services. And a little bit of competition will create innovation in these areas, often desperately needed, and hopefully this will have a positive spill-over effect on badly run public service providers.” 20. IFC has a special director for health and education projects, Karl Voltaire. _____________________________________________________________________________ PSIRU www.psiru.org Page - 8 - Healthcare 29/05/16 The IFC’s investments are quite simple financial investments in private facilities, usually clinics providing various diagnostic and therapeutic services, or hospitals, to private patients. The IFC investments so far have been with partly local and partly multinational partners (based in Finland, Portugal, Spain, and Singapore). Russia Most recently (January 2001), it has invested $2.1m in a new private clinic in St Petersburg, the New Medical Center (NMC). This is described as an “a one-stop facility for most preventive, diagnostic, and treatment services”, and is a venture of the private Finnish medical company Scanfert Oy, (see previous section). IFC’s press release is somewhat misleadingly titled “IFC invests to boost Russian healthcare system”: more accurately it states “IFC and its partners will be tapping into a potentially large market for high quality private facilities in Russia”. 21 Dominican republic IFC has made similar investment in Dominican Republic (April 2000), where it invested US$22 million in four private hospitals, to be run by Spanish hospital company Hospiten, in tourist destinations of the Dominican Republic. The hospitals are said to ‘serve local residents’, but are basically an investment in the tourist industry: “the lack of quality healthcare services has been identified as one of the major barriers to the development of tourism in the Dominican Republic”. 22 Brazil In Brazil, IFC has invested $6.5m, in Innovative Health Services (IHS), a $25m joint venture with a Brazilian financial company, ICATU, and a Portuguese company, Jose de Melo Group. I.H.S. is a holding company which will invest in companies operating “in areas such as home care, occupational and preventive medicine, information technology, prescription benefit management and hospital services and management”. This has been done explicitly to cater for the growth in private health insurance in Brazil, because the insurance companies want more providers. IFC expects that the project will “create new options in healthcare, which may change the way such services are delivered in Brazil”. 23 Nigeria In Nigeria, IFC has invested twice in private clinics serving the private healthcare market. In 1999 it invested US$581,000 in Hygeia Nigeria Limited, a company headed by two local doctors, building five clinics and upgrading facilities at Lagoon Hospital in Lagos, to “extend the managed care coverage for the company's existing and potential clientele” 24. In 1997 it invested $290,000 in the Radmed Diagnostic Center. 25 India The IFC’s largest investment in health remains the $8 invested in a new private 270-bed hospital in Calcutta, India in 1997. The hospital is part of the Gleneagles chain, owned by the Singapore-based Parkway Holdings. 26 3.4 World Bank: Multilateral Investment Guarantee Agency (MIGA) Another section of the World Bank, MIGA, provides investment guarantees to protect mainly against political risk. Together with the IFC, MIGA has provided two remarkable forms of support for the private leasing of medical equipment by a USA firm – DVI – into Brazil. DVI Inc is a company which finances the leasing of medical equipment, mostly MRI scanners, but increasingly treatment equipment such as lasers. Until 1993 it also owned hospitals, but now focuses exclusively on leasing it. DVI “provides equipment financing and related services for users of diagnostic imaging, radiation therapy, and other medical technologies”. DVI has expanded internationally and now does business in Europe, Asia-Pacific, and Latin America. 27 For such _____________________________________________________________________________ PSIRU www.psiru.org Page - 9 - Healthcare 29/05/16 a company, the growing Brazilian market for health care – whether private or public – provides major opportunities for growth business, but there remain currency risks and political uncertainty. DVI has found the IFC and MIGA perfect business partners. First, the IFC formed a joint venture with DVI, called MSF Cayman, in the offshore tax haven favoured by money-launderers, the Cayman Islands. The role of MSF Cayman is to provide “cross-border loans and lease financing to private hospitals, clinics and physician groups throughout Latin America, for the purchase of state-of-the-art diagnostic imaging and radiation therapy equipment. The equipment includes magnetic resonance imaging (MRI), CAT scanners and other medical devices that are essential to the improvement of health care delivery worldwide … The developmental impacts of this project are significant particularly for cancer patients. It offers high-quality, cost-effective and more efficient alternatives to invasive surgery or travelling abroad to the United States or Europe for diagnosis and treatment”. 28 Then MIGA’s role was to provide insurance worth $75m to protect the investments against political risks, including the risk of restrictions being placed on the export of profits, and the risk of expropriation. A year later, in 2000, MIGA provided a further boost to the venture. This time it provided $150m worth of guarantees against political risks for notes issued by MSF secured on future revenues from dollardenominated contracts in Brazil. This insurance was worth a lot to MSF and DVI, because it raised the credit rating of the notes higher than the credit rating of Brazil itself – so international finance could be obtained by MSF at lower interest rates than they could have otherwise. Once again, MIGA claimed that this has development benefits: “This is a project with high development impact, which will help improve the provision of health care in Brazil.” 29 3.5 Other international organisations and treaties The activities of other international bodies also have an influence on the privatisation process. WHO The World Health Organisation (WHO) has an obviously influential role both as an advisor and actor in world health policy.30 OECD The Organisation for Economic Cooperation and Development (OECD), which exercises a powerful role as economic policy advisor, provider of comparative international economic information – including information on health services, and a growing regulatory role - although it abandoned its attempt to introduce a Multilateral Agreement on Investment (MAI). It is currently taking coordinated initiatives on bribery, offshore tax havens, and a code of conduct for multinational companies.31 Energy charter treaty The Energy Charter Treaty, as its name suggests, applies specifically in the energy sectors. It protects multinational investments in energy in various ways, including an absolute legally enforceable right for companies to export profits wherever they wish, in whatever currency they wish.32 Regional trade zones: NAFTA, Mercosur, Asean, EU Additionally, the various regional trade zones of the world have rules which may already affect trade in services between countries in each zone. These rules may make privatisation easier or more likely in various ways, for example by giving rights to investors anywhere in the zone to enter a market elsewhere. In Canada, for example, the modification of healthcare policies in Alberta province could lead to a ‘one-way street towards privatisation of the health sector’ because any attempt to reverse it could be met by investors demanding compensation under NAFTA. 33 _____________________________________________________________________________ PSIRU www.psiru.org Page - 10 - Healthcare 29/05/16 3.6 Public procurement Procurement rules can also affect the introduction of private capital into public services. This is an area which is currently exempt from GATS, but in the EU at least, is covered by European regulations. The EU has a set of common procurement rules for public authorities in all member states. They have to be adopted as part of accession to the EU, and therefore have a similar impact on accession countries in CEE. The main common principle is that they require every public authority in Europe, local, regional, and national, to invite tenders from any undertaking in any country in the EU for all contracts issued by that authority.34 There are some conditions to these requirements: direct service provision is not covered, because the directives do not require compulsory tendering of any work carried out by the public authorities themselves, or their own undertakings, then there is no requirement to invite tenders from private companies. (The directives are thus the precise opposite of the tendering legislation that operated in the UK under the Thatcher government, which insisted on tendering if the public authorities planned to do work themselves, but allowed contracts to be given to favoured private contractors without any competitive tendering). Tenders can be submitted by any organisation in Europe, public or private. Authorities cannot discriminate against public sector undertakings, so a municipal enterprise in Italy can tender for a contract in Spain, for example. The services directive has a list of the services covered, which have to be tendered. At present the list of services that have to be tendered includes services such as cleaning, catering, computing; but not health and social services themselves. In practice however there is a considerable amount of Europe-wide advertisement of health service work. The effect is that this work is open to both public and private sector bidders, nationally and internationally. Two small issues could change the effect of procurement directives dramatically. One is the scope of the definition of direct services which are exempt – for example, the private sector have already tried to exclude from this services provided by a consortium of local authorities (a common feature in continental Europe). The more ‘arms length’ or corporatised the public sector body, the more vulnerable it could be to this kind of shift. The other would be an extension of the list of services to include health and social services. 4. Governments and multinationals 4.1 Government decisions The introduction of privatisation is ultimately by government decisions, as a result of a mix of influences – national politics, international pressures, financial and economic crises or opportunities. As in other policy areas, the dictatorship of General Pinochet in Chile was a pioneer in restructuring and privatisation of health services in ways which are now more familiar – decentralisation of authority, ‘targeting’ of services to the poor, introduction of private health insurance competing with public systems but only for the money of the relatively rich and relatively healthy.35 Privatisation of services has since been introduced into a number of countries (extensively in India, for example). In Europe at present there are proposals for further privatisation of services in both UK and Germany (under social democratic governments)36. In Malaysia, there has been systematic and deliberate privatisation of both hospitals and support services in recent years. Both supplies and support services were privatised in huge monopoly contracts, accounting between them for 22% of the health budget. Private hospitals and clinics have been expanding, and privatised health insurance has been proposed. 37 _____________________________________________________________________________ PSIRU www.psiru.org Page - 11 - Healthcare 29/05/16 4.2 Managed care schemes A number of developing countries, especially in Latin America - notably Brazil and Argentina - started introducing ‘managed care’ schemes in the last 20 years. A key aspect of these schemes is that they exert downward pressure on payments to hospitals, reducing risk and improving margins at the expense of health workers. 38 In Brazil, these schemes have developed over a number of years, with over 700 existing today, served by a large number of private hospitals. Multinationals started to invest into this system in the late 90s, including Aetna (then USA-based, now part of ING) which set up a $375 million arrangement with Sul America; American International Group, with a $460 million investment in Unibanco Seguros; Cigna, in a partnership with Bank Excel and Golden Cross; and ITT Hartford Life in a joint venture with Icatu Seguros. In July 2000 it was reported that the Baylor system in Texas established relations with Brazilian Groups Care and APPH to form Hospitalium, a joint venture with a R$250 million budget (in Brazilian currency) to buy Brazilian hospitals.39 There is a similar picture in the Philippines, where a number of HMOs developed. Again, three US-based multinational insurers – United HealthCare, Aetna, and CIGNA – have invested in these managed care ventures. 40 4.3 The problem of trade unions Trade unions and organised health workers are often a specific target of health restructuring. In Mexico, for example, supporters of privatisation claim that the three biggest issues about introducing more privatisation were the effect on standards, of care, the risk-selection policies of insurers, and “the effect of shifting jobs from the control of the unions to the private sector” 41. The point is thus about increasing the vulnerability of health workers to exploitation, but also about reducing the political influence of the trade unions: the education union and social security workers union are described as “the last bastion of support for preserving the state's role as corporate provider of health care” 4.4 MNCs’ marketing - the annual global conference The marketing activities of MNCs are central to the processes of privatisation and globalisation. From the companies’ point of view, many of the international agencies are in effect supporting these efforts, to the extent of forming global partnerships.42 There is an annual trade conference on the global potential for private healthcare, organised by a body called the Academy for International Health Studies (AIHS), which is not an academic institution but a USA private healthcare business association. The December 2000 conference shows how the multinationals are working with each other, with governments, and with international bodies in this global marketing effort.43 The multinationals involved in the conference were principally the insurance companies: Aetna International (Netherlands); Allianz Group (Germany); Aon Healthcare Alliance (USA); CIGNA International Healthcare (USA); UnitedHealthcare International (USA). Astra/Zeneca Pharmaceuticals (UK) was also involved. The conference treats healthcare, worldwide, as simply a marketing opportunity. There were workshops on “private health sector investment - opportunities and obstacles” in Argentina, Australia, Brazil, Chile, Egypt, Germany, Indonesia, Israel, Mexico, Nigeria, Philippines, Poland and South Africa. Seminar themes included: “Globalization of American Managed Care: Trends, Opportunities and Challenges”; “Employee Benefits for the Multinational Corporation: Health Plan Challenges”; “Global Demographic Trends: Implications for Payers, Providers and Pharmaceuticals”. The conference was attended by the World Bank and the WHO, who made a joint presentation to a plenary session of a “"State of the World's Healthcare Report”. The conference had been started with a keynote _____________________________________________________________________________ PSIRU www.psiru.org Page - 12 - Healthcare 29/05/16 address from Jeffrey Sachs, Chair of the WHO Commission on Macroeconomics and Health, on "Health Care Globalization in the 21st Century: Issues and Challenges”. The conference was attended by high-ranking ministers and officials from many countries, and finished with a “Ministries of Health” forum on "Perspectives on Public-Private Partnerships" (the conference had hoped to host a formal inter-ministerial conference). 5. The multinational companies This section gives a preliminary list by category of the main companies which have business in health services in more than one country. It thus does not list private companies which are very important in their own country but do not operate beyond there (for example, Clininvest, the healthcare chain of SuezLyonnaise des Eaux, which does not operate outside France; or a number of USA health insurance and HMO companies, which do not operate outside the USA). It represents the result of initial paper-and-web research by PSIRU into multinational company activities in healthcare. (January 2000) The data on these companies’ activities is now being collected into PSIRU’s database, and will be available through the PSIRU website (www.psiru.org). 5.1 Insurance multinationals Company Aetna International AIG Allianz Cigna United Health Adeslas (Aguas de Barcelona) BUPA Base Netherlands USA Germany USA USA Spain Other countries Many (excluding USA) Many UK Spain, Ireland, Thailand, Hong Kong Many Philippines, Hong Kong Argentina Activity Insurance Insurance Insurance Insurance Insurance Hospitals, insurance Hospitals, insurance, Aetna International was sold by its USA group to ING, the Netherlands insurance and finance company, in December 2000. It no longer has any connection with the USA insurance group Aetna. AIG and Allianz are both very large insurance companies for whom health insurance is a small part of their business. Allianz specialises in offering healthcare for multinationals’ employees. Cigna has a substantial health insurance business, and has expanded into a number of countries including Mexico. United Health, a large HMO operator in the USA, now has health schemes in Philippines and Hong Kong. Adeslas is the largest healthcare company in Spain, as an insurer and as an owner of private hospitals and clinics. It also operates in Argentina where it owns and runs private hospitals. BUPA has expanded its insurance services to a number of countries, both in Europe and elsewhere. It has hospitals in Spain, but as a consequence of their ownership of the 3rd largest private insurance company, Sanitas, which owns 2 hospitals – not as an expansion of the UK hospital business.44 _____________________________________________________________________________ PSIRU www.psiru.org Page - 13 - Healthcare 29/05/16 5.2 Hospital multinationals Company HCA Sun Healthcare Tenet Paracelsus Capio Base USA USA USA Germany Sweden Parkway Holdings Singapore Afrox South Africa Other countries UK, Switzerland (UK) Spain Switzerland, USA UK, Norway, Denmark, Poland Malaysia, Indonesia, Sri Lanka, India, UK Zimbabwe Activity Hospitals Hospitals Hospitals Hospitals Hospitals, clinical services Hospitals Hospitals, occupational health The big USA hospital companies – HCA, Sun and Tenet – have all reduced their international operations in recent years, but still have a presence in Europe. Paracelsus operates outside Germany in Switzerland and the USA, where its indirectly owned subsidiary has had financial problems. Capio has grown rapidly in the last few years from its base in a privatised hospital in Stockholm. However most of its other operations, including the overseas ones, are specialist clinics rather than general hospitals. Capio was owned by Swedish venture capitalists Bure but was floated as an independent company in September 2000. Parkway Holdings has a significant number of hospitals in south and southeast Asia. It also owned a hospital in London, but this has had financial problems and in 2000 it was seeking to sell it. Afrox is a South African company which has operations in Zimbabwe and is hoping to expand outside Africa. 5.3 Clinical, laboratory and other services Company Fresenius Scanfert Oy AstraZeneca Healthsouth Quest Diagnostics Worldcare Home Germany Finland UK/Sweden USA* USA USA Other places USA, others Portugal, Russia (USA) UK, Australia UK, Mexico many Sector Dialysis, clinical services Clinical services Drugs, cancer care Clinical services Laboratories Telemedicine Fresenius is a German company, which started manufacturing kidney dialysis machines and has now expanded into providing dialysis clinics in many countries. It now offers other clinical services too, and hospital management. Scanfert Oy is a Finnish company, which has recently expanded into St Petersburg (Russia) with the backing of the World Bank’s IFC division. AstraZeneca is an unusual case of a drugs multinational which also has a subsidiary in health services – a cancer clinic chain in the USA. Healthsouth is a major USA operator of outpatient surgery, which has expanded into diagnostic centres, and occupational medicine centres in the US, Australia, Puerto Rico, and the UK _____________________________________________________________________________ PSIRU www.psiru.org Page - 14 - Healthcare 29/05/16 Quest Diagnostics is a major laboratory testing company which has expanded beyond the USA into UK and Mexico. Worldcare is a telemedicine company which has formed a consortium of leading USA hospitals, and seeks to sell telemedicine services worldwide. 5.4 Support services multinationals Company ISS Sodexho Rentokil/Initial Granada/Compass EDS Home Denmark France UK UK USA Elsewhere many Many Many Many Many Main service Cleaning, care homes catering cleaning catering Computing ISS is a cleaning and hotel services multinational, with hospital cleaning contracts in a number of countries. It has diversified into residential care in Scandinavia, and is involved in 6 hospital concessions in the UK, under the private finance initiative (PFI) which has encouraged consortiums with support services companies.45 Sodexho is a French-based catering multinational, with hospital catering contracts in many countries. It has withdrawn from its venture into residential care homes in Scandinavia. It also has a hospital PFI concession in the UK. Rentokil/Initial and Granada/Compass are the other two major cleaning and catering multinationals, each with many contracts in hospitals in many countries. 6. Observations This is a preliminary report, based on a first trawl through evidence on the behaviour of healthcare multinationals and some of the global institutions. Some general comments seem possible, both on the forces of globalisation and on the companies themselves. 6.1 Globalisation The divisions of the World Bank appear to be very significant forces driving privatisation in healthcare, both through projects, investments, and institutional support for the multinationals. The WHO also seems to be associating itself with the policy collapse into ‘public-private-partnerships’ that is happening in other services too. While the WTO and GATS is a clear background to these developments, privatisation in one form or another is happening in a wide range of countries already. Campaigns against privatisation at the country level require international support in addition to the global opposition to GATS. Both trading rules and procurement rules of organisations like NAFTA and the EU may impact on privatisation of health services. These effects are additional to the threats from the WTO, the World Bank, etc. _____________________________________________________________________________ PSIRU www.psiru.org Page - 15 - Healthcare 29/05/16 6.2 Multinationals The picture of multinational behaviour by private healthcare companies is not as coherent or as expansionist as in other sectors (including other public service sectors such as water, waste management, and energy). Many of the USA groups, both the hospital companies and the HMO insurers, have experienced financial and performance problems in recent years. The extreme illustration of the weakness of these groups was the sale of Aetna’s entire international health division. (In this case, healthcare does echo a similar international weakness of US companies in water and waste). The private hospital companies have not been very successful so far at expanding internationally. This is true not only for the USA groups but also the French companies. Vivendi withdrew from the UK 4 years ago and Suez-Lyonnaise has never expanded Clininvest outside France, yet these two groups are extremely internationally aggressive in all other public service sectors. Within Europe, companies which are very large in their own country, - e.g. Paracelsus – show little sign of expanding into neighbouring countries. Even Parkway Holdings, the most successful international hospital group, is selling its UK hospital. Cleaning and catering support services exhibit the ‘classic’ pattern of multinational dominance worldwide, at least in developed countries. These companies may also establish themselves in more general hospital concessions, but so far this has happened only with the UK’s PFI scheme. The insurance companies, as insurers or with HMO schemes, are also expanding. Some of this appears to be simply into ‘niche’ markets, for example, of multinationals’ employees, but there is also some investment into developing countries HMOs. This expansion is obviously dependent on countries adopting policies which create this market. There is also evidence of international expansion in clinical diagnostic or therapy services, such as dialysis, blood products, MRI scans. There is evidence of this kind of service being privatised in a number of countries, including Brazil (see the IFC/MIGA financed schemes above), India (where Delhi council hospitals are to franchise private companies to provide CT scan, cardiac doppler and echo, respiratory lab, incinerator services and other high investment medical technologies 46), Canada (where private MRI scans have opened up in a basically public healthcare system 47), and this seems to be the market which companies like Fresenius, Capio and Scanfert are expanding into (and which the World Bank/IFC seems keen to finance). There is little sign of vertical integration of private healthcare companies, or of any consistent synergies with other services. There are almost no signs of pharmaceutical companies buying insurers or service providers and no consistent merger patterns. In fact demergers have been more striking – Aetna selling its international business, Capio being sold off by its parent finance group, Sodexho selling its venture into residential care. Globalisation may not necessarily arrive at the first stage of privatisation. In Brazil and Philippines with HMOs, the privatised systems were first established by local companies and then the multinationals arrived, through joint ventures or acquisition. _____________________________________________________________________________ PSIRU www.psiru.org Page - 16 - Healthcare 29/05/16 Annexe A: Comments on privatisation/internationalisation chart The term “privatisation” is used to describe various boundaries in different situations. In transition countries of central and eastern Europe and the former Soviet Union, the shift of responsibilities from the central state into the hands of elected local authorities - across the boundary between A and B - is sometimes described as ‘privatisation’. The corporatisation of public service organizations – crossing the boundary between B and C – usually involves the introduction of business accounting if not plc/corporate status, and may be a change as significant as that to private ownership itself. The strict boundary of the private sector – between C and D – may not be of such great significance in countries such as Germany where church and charitable organizations are incorporated into the public health system: in this case the boundary between A, B, C and D on the one hand, and E or F on the other, may be of greater relevance. Finally, the difference between a joint venture where the public sector has some stake – E – and a 100% privately owned undertaking – F – is often treated as very important for presentational reasons, whereas both supporters and opponents of privatisation tend to agree that such PPPs bring nearly all the expected consequences of full privatisation. The horizontal division between national and international provides the distinction, in the final private column, between services being privatised to locally owned businesses, and privatisation to foreign-owned or multinational companies. It is worth mentioning the other parts of the international section. The classification by sector of international activities also helps raise the question of the differences between the activities of multinational corporations, and international activities by public sector and NGO organisations. The segments in the international band include activities of multilateral public sector bodies such as the WHO or the World Bank; international NGOs, e.g. in many primary health care projects in developing countries; global PPPs between the multilaterals and the private sector 48; and global charities like the Gates’ Foundation. All of these are now significant elements in healthcare systems of many countries. There is even some international trading of healthcare by public sector organisations. For example, at least one of the central European spas, Piestany, in Slovakia, was in the mid-1990s both providing free treatment to Slovaks under the national health service, while at the same time treating foreign fee-paying patients, mainly from Saudi Arabia. _____________________________________________________________________________ PSIRU www.psiru.org Page - 17 - Healthcare 29/05/16 Annexe B: Current World Bank projects involving healthcare Project Name HIV/AIDS Rapid Response Project Project Id Total Amount at Board* (USD$M) P060329 Health & Population(Supp). P073278 Social Development Fund Project Education Sector Investment Loan Project P041566 P040650 Malaria/HIV/AIDS Project P065713 HPSP HIV/AIDS Prevention Project P069933 District AIDS and Reproductive Health (DARE) Project P066486 Rural and Small City Water Project P049924 Health Sector Management Project P064926 Multisectoral HIV / AIDS Project P069886 15 Country Gambia, The P065372 60 Tanzania Health Investment Fund Project P051174 10 Moldova Integrated Early Childhood Development Project P068463 40 Eritrea Health Sector Reform Project P008797 40 Romania Health Sector Reform Project P055157 Water Supply and Sanitation for Low Income Communities Project (02) P059477 Health Sector Development Project P058627 22 Tanzania Provincial Health Project P049545 38 Indonesia Health Sector Reform Project P053200 Policy Support Project P064149 National Nutrition Project P050751 92 Bangladesh Tehran Sewerage Project Loan P069946 145 Iran, Islamic R Primary Health Care and Nutrition Project (02) P069943 87 Iran, Islamic R 45 India Health Sector Support Project P055122 41.51 Chad Immunization Strengthening Project P067330 142.6 India P050657 110 India Project Name P010505 P047319 P050483 Project Id 100.48 India 50 Senegal 28.9 Yemen, Republic Total Amount at Board* (USD$M) Country Primary Health Care Project P049894 5.4 Tajikistan Health Sector Management Project P051418 9.5 Slovenia Hlth, Nutn & Popultn Water Supply & Santn Hlth, Nutn & Popultn Economic Policy Hlth, Nutn & Popultn Hlth, Nutn & Popultn Hlth, Nutn & Popultn Agriculture Education Education Sector Hlth, Nutn & Popultn Hlth, Nutn & Popultn Board Approval Date Active 1/16/01 Active 12/21/00 Active 12/20/00 Active 12/20/00 Active 12/18/00 Active 12/12/00 Active 12/12/00 Active 10/17/00 Active 9/14/00 Active 9/12/00 Social Protection Hlth, Nutn & Popultn Hlth, Nutn & Popultn Hlth, Nutn & Popultn Hlth, Nutn & Popultn Hlth, Nutn & Popultn Hlth, Nutn & Popultn Hlth, Nutn & Popultn Hlth, Nutn & Popultn Economic Policy 63 Bulgaria .3 77 Indonesia .4 6. Lesotho 5 8 Central African Uttar Pradesh Health Systems Development Project District Poverty Initiatives Project - Rajasthan Quality Education for All Project Child Development Project Multisector Hlth, Nutn & 7 Rwanda Popultn 30 Senegal Social Protection 44.99 Mali Education Hlth, Nutn & 40 Eritrea Popultn Banglade Hlth, Nutn & 40 sh Popultn Hlth, Nutn & 50 Kenya Popultn Water Supply & 32 Ecuador Santn Hlth, Nutn & 5 Samoa Popultn Hlth, Nutn & 59.7 Ethiopia Popultn Social Action Fund Project Economic Reform Technical Assistance Project P059501 Sector Proje ct Statu s Active 8/22/00 Active 8/22/00 Active 7/27/00 Active 6/27/00 Active 6/22/00 Active 6/15/00 Active 6/15/00 Active 6/15/00 Active 6/13/00 Active 5/30/00 Active 5/25/00 Active 5/18/00 Active 5/18/00 Active 5/12/00 Active 4/27/00 Active 4/25/00 Active 4/25/00 Active Active Active 4/25/00 4/11/00 3/21/00 Projec Board t Approval Status Date Active 3/7/00 Active 1/20/00 _____________________________________________________________________________ PSIRU www.psiru.org Page - 18 - Healthcare 29/05/16 P058358 Health Sector Reform Program Project P062932 80 Peru P050667 182.4 India Uttar Pradesh District Primary Education Project (03) Mindanao Rural Development Project (APL) P058842 4 Solomon Islands Health Sector Development Project Hlth, Nutn & Popultn Hlth, Nutn & Popultn 27.5 Philippines Health Sector Support Project (02) P051741 40 Madagascar Health Project P035780 21.24 Lithuania Health Insurance for the Poor Project P063388 4.9 Argentina Active 1/6/00 Active 12/16/99 Education Active 12/16/99 Agriculture Hlth, Nutn & Popultn Hlth, Nutn & Popultn Hlth, Nutn & Popultn Active 12/2/99 Active 12/2/99 Active 11/30/99 Active 11/24/99 Marmara Earthquake Emergency Reconstruction Project Project Id Project Name Total Amount at Board* (USD$M) Country Health Surveillance System and Disease Control Project P055482 52.5 Argentina EC SUPP SOC DEV II/HLTH & NUTRIT. P068739 20.2 Ecuador Social Action Project (02) P064510 12 Burundi Health System Project P051273 29 Croatia Fisheries Project (04) P009468 Social Protection Initiatives Project P066336 Structural Reform Support Project Western Poverty Reduction Project P052154 P046564 Health Sector Reform Project P060392 25 Bolivia Rural Water Supply and Sanitation Project (04) P057352 46 China Project Name Project Id Sector Hlth, Nutn & Popultn Hlth, Nutn & Popultn Social Protection Hlth, Nutn & Popultn Agriculture 28 Bangladesh Egypt, Arab 5 Rep 16.5 Georgia 160 China Total Amount Country at Board* (USD$M) 44 Brazil P055388 Integrated Drug Prevention Pilot Project P058526 Basic Health Project P044523 10 Health Project (09) P036953 60 China Health Project P046499 42.5 Kazakhstan Social Sector Support Project P060943 60 Malaysia Health Sector Reform Project P039749 35 Jordan P055003 4.9 Mauritania P050732 P044840 22 Guinea 15 Moldova Nutrition, Food Security and Social Mobilization Project Village Communities Support Project Social Investment Fund Project Project Name Project Id 4.75 Argentina Total Amount at Board* (USD$M) BosniaHerzegov Country HN/NUTRI/HEALTH (SUPL) P064866 10.4 Honduras Public Works Project (02) P060132 Municipal Development Project (02) P055480 10.1 Chile Health Sector Development Program P040652 40 Mali Health Financing and Management Project P005525 66 Morocco Maharashtra Health Systems Development Project P050651 50 Yemen, Republic 134 India Active 10/14/99 Active 10/7/99 Active 10/5/99 Active 10/5/99 Active 7/20/99 Social Protection Active 6/29/99 Economic Policy Agriculture Hlth, Nutn & Popultn Water Supply & Santn Active Active 6/29/99 6/24/99 Active 6/15/99 Active 6/3/99 Sector Animal and Plant Health Protection Project Projec Board t Approval Status Date Agriculture Hlth, Nutn & Popultn Hlth, Nutn & Popultn Hlth, Nutn & Popultn Hlth, Nutn & Popultn Social Protection Hlth, Nutn & Popultn Hlth, Nutn & Popultn Agriculture Social Protection Sector Hlth, Nutn & Popultn Urban Development Public Sector Mgmt. Hlth, Nutn & Popultn Hlth, Nutn & Popultn Hlth, Nutn & Popultn Projec Board t Approval Status Date Active 5/27/99 Active 5/5/99 Active 5/4/99 Active 5/4/99 Active 4/8/99 Closed 3/30/99 Active 3/25/99 Active 3/15/99 Active 2/23/99 Active 2/16/99 Proje ct Statu s Board Approval Date Active 1/28/99 Active 1/28/99 Active 12/22/98 Active 12/17/98 Active 12/17/98 Active 12/8/98 _____________________________________________________________________________ PSIRU www.psiru.org Page - 19 - Healthcare 29/05/16 Population and Reproductive Health Project P041568 11.3 Guinea HEALTH P058520 12 Latvia Health Sector Development Program Project P000756 100 Ethiopia Social Action Fund Project (02) P049599 66 Malawi Hlth, Nutn & Popultn Hlth, Nutn & Popultn Hlth, Nutn & Popultn Social Protection Active 12/1/98 Active 11/12/98 Active 10/27/98 Active 10/15/98 1 French foreign trade Secretary Meeting minutes' on GATS meeting 17 November 2000 (translated) Eg “How the World Trade Organization’s new “services” negotiations threaten democracy” by Scott Sinclair Canadian Centre for Policy Alternatives; 2000 3 Rewriting the regulations: how the World Trade Organisation could accelerate privatisation in health-care systems Allyson M Pollock, David Price Lancet 2000; 356: 1995-2000 4 “The WTO and the General Agreement on Trade in Services: What is at stake for public health“ Public Services International and Education International (PSI & EI) July 2000 5 World Development Movement Report (WDM) “In whose service? The threat posed by the General Agreement on Trade in Services to economic development in the South” by Ellen Gould and Clare Joy December 2000 http://www.wdm.org.uk/cambriefs/WTO/Inwhoseservice.htm 6 PSI & EI, p.14 and annexe 7 Sinclair, section 2 8 Pollock and Price, Lancet 2000; 356: 1995 9 European Services Network “ESN POSITION PAPER ON GATS 2000 AND PUBLIC PROCUREMENT Final Version 2 - April 23, 1999 10 PSI & EI, p.15 ICFTU, Brussels, 8/6/00 12 DR BANKENSTEIN'S MONSTERS: THE WORLD BANK, THE IMF AND THE ALIENS WHO ATE ECUADOR by Gregory Palast The Observer, London Sunday, 8 October 2000 13 Source: Sarah Grutsky, Globalization Challenge Initiative 11 See PSIRU papers on “Independent Power Producers: A review of the issues” and “Privatisation of water and energy in Africa”, both available at www.psiru.org/reports 14 The source of the material in Annexe B is the World Bank’s website www.worldbank.org. The various tables and reports are generated in response to queries submitted by scripts. 16 World Bank Project ID P058627 17 World Bank Project ID P049545 18 World Bank Project ID P055157 19 Document of The World Bank Report No. 20339 BUL PROJECT APPRAISAL DOCUMENT ON A PROPOSED LOAN IN THE AMOUNT OF US$63.3 MILLION TO THE REPUBLIC OF BULGARIA FOR A HEALTH SECTOR REFORM PROJECT May 30, 2000 20 Peter Woicke Annual Luncheon Speech 25 September 1999 “A New Direction” http://www.ifc.org/ifc/pressroom/speeches/amlunch/amlunch.html 21 “IFC INVESTS TO BOOST RUSSIAN HEALTH CARE SYSTEM“ IFC Press Release No. 01/36 Jan 2001 22 “IFC INVESTS IN HOSPITAL NETWORK IN THE DOMINICAN REPUBLIC” IFC Press Release 102, April 7 2000 23 “IFC MAKES FIRST HEALTHCARE INVESTMENT IN BRAZIL“ IFC Press release 99/124 March 19, 1999 24 IFC INVESTS IN HEALTHCARE AND MANUFACTURING IN NIGERIA” IFC Press release 00/25 Sept 9 1999 25 http://www.ifc.org/ifc/ABN/cic/nigeria/english/invest.htm#radmed 26 “IFC TO INVEST US$8 MILLION IN MODERN MULTI-SPECIALITY PRIVATE HOSPITAL IN CALCUTTA INDIA” IFC Press Release No. 98/50 November 20, 1997 27 Hoovers profile of DVI Inc. www.hoovers.com 28 “MIGA Insures Ground-breaking Health Care Project in Brazil” MIGA Press release August 6, 1999 29 MIGA: “Latin Report: Public-Private Insurance” September 2000 30 www.who.org 31 See www.oecd.org, www.oecd.org/els/health 32 See www.encharter.org, www.encharter.org/English/Secretariat/index.html. The website is recent. Learning form the lesson of the MAI, the Energy Charter Treaty was never available on the internet until it came into force in 1998. 33 Legal Opinion Appleton Associates 10/4/2000”NAFTA Investment Chapter Implications of Alberta Bill-11 34 The existing procurement directives are currently being consolidated. The proposed new directive provisions are published in “Proposal for a DIRECTIVE OF THE EUROPEAN PARLIAMENT AND OF THE COUNCIL on the coordination of procedures for the award of public supply contracts, public service contracts and public works contracts”. Brussels, 30.8.2000 COM(2000) 275 final/2 2000/0115 (COD) 15 _____________________________________________________________________________ PSIRU www.psiru.org Page - 20 - Healthcare 29/05/16 35 Restructuring and privatization of health care services: Selected cases in the Americas by Sandra Polasyk. ILO Action Programme on Privatization, Restructuring and Economic Democracy. November 1999 36 Restructuring and privatization of health care services: Selected cases in western Europe by Stephen Bach. ILO Action Programme on Privatization, Restructuring and Economic Democracy. November 1999 37 “Privatisation, the State and Healthcare Reforms: Global Influences & Local Contingencies in Malaysia” by Chan Chee Khoon, Citizens' Health Initiative. Paper presented to 9th International Congress of the World Federation of Public Health Associations Beijing, People’s Republic of China September 2-6, 2000 http://prn.usm.my/chi.html 38 How the United States Exports Managed Care to Third-World Countries. By Howard Waitzkin and Celia Iriart, Monthly Review May 1, 2000 39 “AIHS Country workshop report” Modern Healthcare International 17/7/2000 40 “AIHS Country workshop report” Modern Healthcare International 17/7/2000 41 “AIHS Country workshop report” Modern Healthcare International 17/7/2000 www.modernhealthcare.com 42 See Buse &.Walt Bulletin of the World Health Organization, 2000, 78 (4) 43 See www.aihs.com/summit/summitabout.html for information on speakers and agenda. 44 “A Spanish revolution; With surging economy, private sector plays vital role in healthcare system” FT 13/11/2000 45 ISS Half-yearly results August 2000 46 THE HINDU December 18, 2000: MCD move on hospitals to hit poor 47 Modern Healthcare International 13/11/2000 “Clash in Canada: Privatization legislation and NAFTA open healthcare market to protests” For a review of the extent of these Global PPPs see “Global public–private partnerships: parts I and II– a new development in health?” K. Buse &G.Walt Bulletin of the World Health Organization, 2000, 78 (4) 48 _____________________________________________________________________________ PSIRU www.psiru.org Page - 21 -