The New AdolesceNTs: AN ANAlysis of heAlTh coNdiTioNs, BehAviors, risks,
advertisement

The New Adolescents:
An Analysis of Health
Conditions, Behaviors, Risks,
and Access to Services Among
Emerging Young Adults
“Emerging young adults
are adrift in a perfect
storm of health risks”
Lawrence S. Neinstein, MD
2013
1
Acknowledgements
The New Adolescents: An Analysis of Health Conditions, Behaviors, Risks, and
Access to Services in the United States compared to California, Among Adolescents (12–17),
Emerging Young Adults (18–25) and Young Adults (26–34).
Senior Author:
Lawrence S. Neinstein, MD
Professor of Pediatrics and Medicine
Keck School of Medicine of USC
University of Southern California
Executive Director, Engemann Student Health Center
Chief, Division of College Health
Senior Associate Dean of Student Affairs
Contributors:
Yang Lu, Ph.D.
Assistant Professor of Research
Keck School of Medicine of USC &
Sol Price School of Public Policy
University of Southern California
Lauren Perez, MPH
Project Specialist
Engemann Student Health Center
University of Southern California
Bryan Tysinger, MPhil
Research Programmer
Sol Price School of Public Policy
University of Southern California
Executive Summary
4
1Demographics
8
2Mortality
3Injuries
12
16
Leonard D. Schaeffer Center for Health Policy and Economics, University of Southern California
4 Mental Health
22
The Community, Health Outcomes & Intervention Research Program, The Saban Research Institute
of Children’s Hospital Los Angeles
5 Substance Abuse
24
Division of College Health, Department of Pediatrics, Keck School of Medicine of USC and Division
of Student Affairs, University of Southern California
6 Reproductive Health
32
7 Sexually Transmitted Infections
38
8 Chronic Disease
46
9 Health Promotion and Prevention
58
10 Services 66
11References
78
Sponsors:
This report would not have been possible without the support and sponsorship of:
California Wellness Foundation
■
■
■
■
Acknowledgements:
The Senior Author would like to acknowledge the following individuals and institutions for their guidance and
support: Roberta Williams MD (Professor of Pediatrics, University of Southern California), D-Brent Polk MD
(Chair and Professor of Pediatrics, University of Southern California), Michael Jackson Ed.D. (V.P. of Student
Affairs, University of Southern California), Michele Kipke Ph.D. (Vice Chair of Research, Department of
Pediatrics, Childrens Hospital Los Angeles), Calvin Gordon MD, Beth Dameron and Alvina Sundang
(Kaiser Permanente, Northern California) and also the significant work and passion of my three associates and
contributors: Yang Lu PH.D, Lauren Perez MPH, and Bryan Tysinger, MPhil.
© 2013 The New Adolescents: An Analysis of Health Status, Lawrence Neinstein MD
2
Table of Contents
Executive Summary
Emerging young adults are the most uninsured age group in the United States, often losing their insurance
when they graduate high school or college. Although the Affordable Care Act has helped this situation, the
recent Gallup-Healthway poll estimated only a small decline of uninsured emerging young adults from 28%
uninsured 18 to 25 year olds in fall 2010 to 24.2% in second quarter of 2011 (http://www.gallup.com/
poll/153737/uninsured-rate-year-olds-plateaus.aspx).
■
Background
This report examines the health risks facing the nation’s 34.6 million emerging young adults, a group defined as
young people aged 18–25. They occupy the space between adolescence and young adulthood—they are separating
from home and parents, but in many instances are not yet completely independent adults. It is a potentially
precarious time of life.
As illustrated in the pages that follow, emerging young adults face greater behavioral and non-behavioral health
risks than either adolescents aged 12–17 or young adults aged 26–34. Yet compared to those two age groups,
emerging young adults often have the lowest perception of risk and the least access to care. Overall, emerging
young adults have the highest rates of motor vehicle injury and death, homicide, mental health problems, sexually
transmitted infections and substance abuse. They have the lowest rates of health insurance coverage. In short,
emerging young adults are adrift in a perfect storm of health risks.
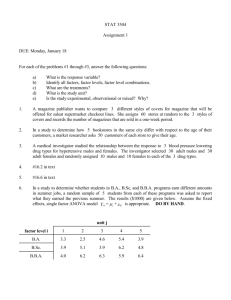
The figure below offers just one example of this perfect storm. Emerging young adults have the highest prevalence
of binge drinking (blue), the lowest perception of high risk (red) and the highest rate of needing but not receiving
treatment for this problem (green).
The Perfect Storm in Emerging Young Adults
Binge Drinking, Perceptions of Risk, and Access to Care
by Age Group, U.S. and California 2008-2009
50%
45%
40%
Binge Alcohol Use
in Past Month
35%
30%
Perceptions of Great
Risk of =/> 5 Drinks
Once or Twice a Week
25%
20%
Needing But Not
Receiving Treatment
for Alcohol Use in
Past Year
15%
10%
5%
0
As this report demonstrates, emerging young adults—a group sometimes referred to as “young invincibles”—need
access to broad health coverage to prevent significant negative health outcomes and treat acute and chronic medical
conditions. In the words of “young invincibles” (www.younginvincibles.org):
“We use the emergency room more than any age group under age 75 and 16 percent of us suffer from
chronic conditions; we need preventive and primary care.”
“If we are lucky enough to have jobs, they typically provide us with fewer benefits than older, more
experienced workers.”
Our goal in producing this chart book is to provide health care providers, health care networks and vendors,
institutions, and policy makers with the data they need to make informed decisions about broad health care coverage
and health prevention interventions in emerging young adults.
Methods
This chart book focuses on the health of emerging young adults aged 18–25 in California and the United States
and compares them to adolescents aged 12–17 and young adults aged 26–34. In addition, some of the data were
stratified by gender and ethnicity. Data were extracted in the following areas: demographics, mortality rates, injuries
(intentional and unintentional), mental health issues, substance use and abuse, reproductive health (pregnancy and
contraception), sexually transmitted infections (STIs), chronic conditions, health promotion and prevention, and
services (including utilization, cost and accessibility). Many existing national and state health databases have been
utilized to obtain this data including:
Behavioral Risk Factor Surveillance System Survey
Data (BRFSS), CDC
■
California Health Interview Survey (CHIS), UCLA
Center for Health Policy Research
■
18 - 25
U.S.
26+
12 - 17
18 - 25
26+
California
■
CDC WISQARS for injury and mortality data
■
Health, United States, NCHS
■
■
HIV Surveillance Reports, CDC
■
MEPSnet Household Component for 2009 Agency
for Healthcare Research and Quality
■
Why is emerging young adulthood fraught with health risks? Although outside the purview of this report, we
offer some observations from the recent health literature.
Evidence in brain development research that shows significant brain development still occurring in emerging
young adults in the prefrontal cortex, the area controlling emotions and rational decision making (Giedd Jay N,
2008 and Johnson SB et al, 2009).
■
A progressively increasing delay in attaining traditional life milestones including completing school, leaving
home, becoming financially independent, marrying and having a child. In 1960: 77% women and 65% of men
at 30 reached these five “milestones”. Among 30-year-olds in 2000, <50% of women and 1/3rd of men had
done so (US Census Bureau and Marantz Henig, 2010).
■
4
National Center for Chronic Disease Prevention
and Health Promotion
■
CDC WONDER for Population Projections
■
■
12 - 17
National Health and Nutrition Examination Survey
Data (NHANES)
■
Monitoring the Future national survey results on
drug use
■
MMWR reports on mental health, CDC
■
National Center for Health Statistics
■
National Survey of Family Growth
National Center for Chronic Disease, CDC
National College Health Assessment II (NCHA),
American College Health Association
SEER Cancer Statistics, National Cancer Institute
■
Sexually Transmitted Disease Surveillance reports
■
Sexually Transmitted Diseases in California,
California Department of Public Health
■
Substance Abuse and Mental Health Services
Administration reports on Drug Use and Health
■
Youth Risk Behavior Survey Data
National Center for Injury Prevention and Control
■
National Health Interview Survey (NHIS)
■
■
■
US Census Bureau
National vital statistics reports
■
Executive Summary
5
Executive Summary continued
Other data were obtained from existing research studies. In addition, some utilization data were obtained from
personal communications with Kaiser Permanente Northern California. The specific references to the data sources
are listed in the last section of this chart book.
Limitations
The use of existing national databases allows for a large nationally representative sample. However, the use of
existing data limits the ability to examine issues beyond the scope of the database. Specific limitations include:
The inability to use consistent age groups throughout. Some databases report data in age groups that differ from
the breakdown used in this chart book and the raw data are not available to make the necessary changes.
■
Data are not always available for stratification by gender or ethnicity.
■
National databases do not always include state-level data or may only be available from a different source,
which weakens the comparability of national and state level data.
■
The lack of availability of data in certain areas such as the epidemiology of chronic diseases. National registries
and monitoring systems do not exist for most of these conditions which makes the compilation of such data
challenging and limited.
■
The lag in the public availability of certain data which results in the lack of timeliness of some data.
■
Substance use and chronic diseases might be under-reported in survey data due to self-report bias.
■
Results and Key Points
The detailed results are listed in each section and highlighted by both “take home messages” and “bullet points.”
Overall, emerging young adults have the highest rates of motor vehicle accidents, homicides, substance abuse,
mental health issues and sexually transmitted infections while having the highest rate of being uninsured.
Demographics: In 2010, there were approximately 34.6 million emerging young adults in the U.S., including
4.3 million in California. In the U.S., whites are the largest racial/ethnic group, accounting for approximately 60
percent of the population in each age group. However, in California, in all three age groups, Hispanics/Latinos are
the largest racial/ethnic group, accounting for 43.3% of emerging young adults, 47.7% of adolescents and 42% of
young adults.
Mortality: Unintentional injuries are the leading cause of mortality among young people aged 12–34 with motor
vehicle accidents (MVA) accounting for the largest percentage. Emerging young adults aged 18–25 face the highest
risk. In 2010, MVA-related hospitalization and emergency department treatment of emerging young adults cost
the U.S. health care system $9 billion. Homicides and suicides are the second- and third-leading causes of death,
respectively, in young people aged 12–34.
Sexually Transmitted Infections: The highest incidence rates of chlamydia and gonorrhea are in young adult
males aged 20–24 and in older adolescent and young adult females aged 15–24. Incidence rates in young adults
are highest in African American females aged 20–24, followed by African American males aged 20–24. The highest
numbers of new cases of HIV occur in emerging young adults aged 20–24. Cervical and vaginal HPV infections are
the most common STIs in the young sexually active U.S. population with 74% of the 6.2 million new infections
each year occurring in those aged 15–24.
Chronic Diseases: In the U.S. there are over 16.3 million cases of the top seven common chronic diseases —
cancer, diabetes, heart disease, hypertension, stroke, mental disorders and pulmonary conditions. Three—cancer,
heart disease and mental disorders (suicide)—are among the top five causes of mortality in young adults. Many of
the most frequent chronic diseases either start or continue in the young adult years and others, such as heart disease,
stroke and diabetes, can be prevented with interventions during this period of life. Young adults aged 20–35 have
the lowest improvements in cancer survival rates during the past 25 to 35 years, potentially related to differences in
involvement in treatment protocols, treatment centers and access to health care.
Health Promotion and Prevention: Overall compliance with HPV, influenza, and pertussis vaccinations is low in
emerging young adults and young adults. In California and the nation, emerging young adult males are least likely
to always or almost always wear a seatbelt, and correspondingly have the highest fatal MVA-occupant injury rates.
Preventive health guidelines for emerging young adults are not consistent among medical and health organizations.
Services (Accessibility, Utilization and Cost): Emerging young adults have the highest uninsured rates in both
the U.S. and California with males more likely to be uninsured than females. Emerging young adults have the lowest
number of outpatient healthcare visits per person per year and the highest number of emergency room visits. Young
adults aged 18–24 are most likely to report no health care visits in the past 12 months. Emerging young adults had
the highest prevalence of $0 spending per person per year (26%). Regardless of age group, uninsured individuals are
more likely to spend $0 on annual health care expenditures.
Conclusions
Emerging young adults 18–25 have a higher prevalence of significant health risks compared to adolescent and
young adults. At the same time they have a lower perception of risk in many of these areas and are the largest
uninsured age group in the United States.
Recommendations
Broad health care coverage for emerging young adults is urgently needed. A national “emerging young adult”
health agenda—including thoughtful health care research, programs and national and state policies regarding
delivery and access to health care—must be developed for this at risk age group.
Mental Health: Emerging young adults compared to young adults aged 26–34 have higher rates of serious
psychological distress and suicidal thoughts, plans and attempts. Compared to adolescents, emerging young adults
are more likely to complete suicides.
Substance Abuse: As indicated above, emerging young adults have the perfect storm of alcohol risk: i.e., the
highest rate of past-month binge drinking but the lowest perception of risk and the greatest need for services but
lowest access to services. In addition, in both California and the nation, emerging young adults have the highest
rates of past-month tobacco and cigarette use, as well as higher rates of marijuana, cocaine and other illicit drug use.
Reproductive Health: Birth rates peak in young adults aged 25–29. While trends show a decrease in birth
rates since 1980 in adolescents and young adults until age 29, there has been a continuing rise in the percent of
pregnancies resulting in a life birth in this age group.
6
Executive Summray
7
1 Demographics
Figure 1.1C
2,500,000
Take Home Message:
This chapter provides a demographic snapshot of emerging young adults in California and the nation, and compares
them to adolescents 12–17 years, and young adults, defined as individuals 26–34 years. To perform our analysis, we
adjusted population data to account for the disparate number of years in each age cohort. This adjustment produced an
average that could be compared across groups. Our population statistics are from 2009, the latest year for which figures
are available.
There were 34.6 million emerging young adults in the U.S., including 4.3 million in California. In the nation and
the state, males slightly outnumber females among 18–25 year olds. In the U.S., whites are the largest racial/ethnic
group, accounting for approximately 60 percent of the population in each age group. However, the ethnic/ racial
composition of California differs sharply from the nation as a whole. In California, in all three age groups, Hispanics/
Latinos are the largest racial/ethnic group, accounting for 43.3% of emerging young adults, 47.7% of adolescents and
42% of young adults.
2,000,000
12 to 17
1,500000
18 to 25
26 to 34
1,000,000
Average Population per Year* by
Gender and Age Group, U.S. and
California, 2009
In the U.S. and California, males have
a larger population per age group than
females (Figures 1.1B, 1.1C).
500,000
0
Male
U.S.
Female
Male
Female
California
*adjusted by number of years/age group
Source: US Census Bureau (2009)
Figure 1.1A
2,500,000
Population by Gender and Age Group,
U.S., 2009
2,300,000
Among U.S. males aged 12–34, 20 year
olds form the most populous age group.
The female population peaks at 20 years
and 29 years.
1,900,000
50%
1,700,000
Male
1,500,000
Female
1,300,000
1,100,000
26 to 34
20,000,000
Black
Asian-PI
Hispanic
Figure 1.1E
50%
18,000,000
Percentage of Population by Race
and Age Group, California, 2009
45%
16,000,000
40%
14,000,000
12,000,000
10,000,000
8,000,000
12 to 17
35%
18 to 25
30%
26 to 34
25%
12 to 17
18 to 25
26 to 34
20%
6,000,000
15%
By contrast, Hispanics/Latinos are the
largest racial/ethnic group within each age
cluster in California, with 47.7%, 43.3%,
and 42% respectively in each age group
followed by whites, Asian-Pacific Islanders,
and blacks
10%
2,000,000
0
White
Source: US Census Bureau, American Fact Finder (2010)
4,000,000
Male
Source: US Census Bureau (2009)
8
18 to 25
30%
0%
12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34
Source: Population Projections, CDC Wonder
Emerging young adults make up the largest
age group in the U.S. and California, after
adjusting for the years in each cohort, and
emerging young adult males make up the
largest group (Figures 1.1B, 1.1C).
40%
Within each age cohort in the U.S., whites
are the largest racial/ethnic group with
approximately 60% in each age group,
followed by Hispanics/Latinos (19.5%,
18.2%, and 19.8% respectively) and blacks
(14.8%,14.6%, and 13.2% respectively)
10%
700,000
Population by Gender and Age group,
U.S. and California, 2009
12 to 17
20%
900,000
Figure 1.1B
Percentage of Population by Race
and Age Group, U.S., 2009
60%
2,100,000
500,000
Figure 1.1D
70%
U.S.
Female
Male
Female
California
5%
0%
White
Black
Asian-PI
Hispanic
Source: US Census Bureau, American Fact Finder (2010)
Demographics
9
1 Demographics continued
Figure 1.2A
Population projection trends by Age
group, U.S., 2010-2030
Compared to adolescents and young adults,
emerging young adults will experience the
greatest population decline (between 2010
and 2020) and gain (between 2020 and
2030), after adjusting for the years in each
cohort (Figures 1.2A, 1.2B, 1.2C & 1.2D).
40,000,000
30,000,000
12 to 17
25,000,000
18 to 25
20,000,000
26 to 34
15,000,000
10,000,000
Population Projection Trends by Age
Group/Year*, U.S., 2010-2030
12 to 17
18 to 25
550,000
26 to 34
450,000
2010
2015
2020
2025
400,000
2030
Source: Population Projections, CDC Wonder
4,800,000
4,700,000
4,600,000
4,500,000
4,400,000
4,300,000
4,200,000
4,100,000
4,000,000
3,900,000
3,800,000
3,700,000
600,000
500,000
5,000,000
Figure 1.2B
Population Projection Trends by Age
Group/Year*, California, 2010-2030
650,000
35,000,000
0
Figure 1.2D
700,000
45,000,000
2010
2020
2030
*adjusted by number of years/age group
Source: Population Projections, CDC Wonder
12 to 17
18 to 25
26 to 34
2010
2015
2020
2025
2030
*adjusted by number of years/age group
Source: Population Projections, CDC Wonder
Figure 1.2C
Population Projection Trends by Age
Group, California, 2010-2030
7,000,000
6,000,000
5,000,000
12 to 17
4,000,000
18 to 25
3,000,000
26 to 34
2,000,000
1,000,000
0
2010
2020
2030
Source: Population Projections, CDC Wonder
10
Demographics
11
2 Mortality
Table 2.1
Take Home Message:
Unintentional injury, homicide, and suicide, respectively, are the three leading causes of death among young people
aged 12–34. Mortality rates are higher among males than females. Compared to adolescents and young adults, emerging
young adults aged 18–25 are more likely to die from unintentional injury and homicide. Homicide rates for emerging
young adults are higher in California than in the nation as whole. Cancer and heart disease are the fourth- and fifthleading causes of death, respectively, across all age groups.
Figure 2.1A
Overall Mortality Rates (per 100,000)
by Age Group, Race, and Gender,
U.S., 2008
Overall mortality rates are higher for
males than females across all age groups
in California and the nation
(Figures 2.1A, 2.1B).
Leading Causes of Death, Rates (per 100,000), U.S. and California, 2008
Unintentional injury, homicide and suicide are the leading causes of death among young people aged 12–34 in the
U.S. and California. Emerging young adults have the highest mortality rate for unintentional injuries and homicides
and young adults for suicides (Table 2.1).
Cancer and heart disease, respectively, are the fourth- and fifth-leading cause of death among young people in
California and the nation. The mortality risks from malignancies and heart disease increase with age (Table 2.1).
Unintentional injury is the leading cause of mortality among adolescents, emerging young adults, and young adults
in California and the nation. Emerging young adults face the highest risk (Table 2.1).
250
United States
200
150
Male
Female
100
50
0
12-17 18-25 26-34 12-17 18-25 26-34 12-17 18-25 26-34 12-17 18-25 26-34
White
Black
Hispanic
Asian/Pacific
Islander
Source: Centers for Disease Control and Prevention, National Center for Health Statistics. Underlying Cause of Death 19992008 on CDC WONDER Online Database, released 2011
Figure 2.1B
Overall Mortality Rates (per 100,000)
by Age Group, Race, and Gender,
California, 2008
Among all age groups, in both genders,
in both the U.S. and California, blacks
have the highest overall mortality rates and
Asian/Pacific Islanders have the lowest rates
(Figures 2.1A, 2.1B). Note that Hispanic
emerging young adult males have the
highest overall mortality rate compared
to the other two age groups for Hispanic
males.
250
200
18 - 25 Cause of Death
11.9 Unintentional Injury
4.0 Homicide
3.8 Suicide
2.7 Malignant Neoplasms
1.1 Heart Disease
0.9 Congenital Anomalies
0.3 Diabetes Mellitus
0.3 HIV
26 - 34
Cause of Death
39.1 Unintentional Injury
14.5 Suicide
12 Homicide
4.4 Malignant Neoplasms
3.2 Heart Disease
1.1 HIV
0.6 Diabetes Mellitus
0.6 Cerebrovascular
27.1
12.9
11
9
8.3
2.5
1.5
1.4
9
10
Respiratory Disease
Influenza & Pneumonia
Benign Neoplasms
0.3
0.2
0.6
0.5
1.1
0.9
Influenza & Pneumonia
Cerebrovascular
Liver Disease
Congenital Anomalies
California
150
Male
Female
100
50
0
Rank
1
2
3
4
5
6
7
8
12 - 17 Cause of Death
Unintentional Injury
Homicide
Suicide
Malignant Neoplasms
Heart Disease
Congenital Anomalies
Cerebrovascular
Chronic Low.
12-17 18-25 26-34 12-17 18-25 26-34 12-17 18-25 26-34 12-17 18-25 26-34
White
Black
Hispanic
Asian/Pacific
Islander
Source: Centers for Disease Control and Prevention, National Center for Health Statistics. Underlying Cause of Death 19992008 on CDC WONDER Online Database, released 2011
12 - 17 Rank
1
2
3
4
5
6
7
8
9
10
Cause of Death
Unintentional Injury
Homicide
Suicide
Malignant Neoplasms
Heart Disease
Congenital Anomalies
Influenza & Pneumonia
Anemias
Cerebrovascular
Chronic Low.
Respiratory Disease
18 - 25 Cause of Death
10.4 Unintentional Injury
5.9 Homicide
2.0 Suicide
3.2 Malignant Neoplasms
0.6 Heart Disease
0.5 Congenital Anomalies
0.2 Cerebrovascular
0.1 HIV
0.2 Diabetes Mellitus
0.1 Chronic Low.
26 - 34
Cause of Death
43.3 Unintentional Injury
24.7 Homicide
11.9 Suicide
6.9 Malignant Neoplasms
3.2 Heart Disease
1.3 HIV
0.9 Liver Disease
0.5 Diabetes Mellitus
0.4 Cerebrovascular
0.3 Congenital Anomalies
36.9
16.1
14.0
12.6
9.2
2.7
2.2
1.7
1.4
1.2
Respiratory Disease
Source: Centers for Disease Control and Prevention, National Center for Health Statistics. Underlying Cause of Death 1999-2008 on CDC WONDER Online Database, released 2011
12
Mortality
13
2 Mortality continued
Figure 2.1C
Top Three Causes of Mortality
Rates (per 100,000) by Age Group
and Gender, U.S., 2009
Homicides: Emerging young adult
males face the highest risk of homicide in
California and the nation. The majority of
these homicides involve firearms.
Among emerging young adults nationally,
males face six times the risk of homicide
compared to females. In California,
emerging young adult males face nearly
10 times the risk (Figures 2.1C, 2.1D).
Figure 2.1D
Top Three Causes of Mortality
Rates (per 100,000) by Age Group
and Gender, California, 2009
Suicides: Emerging young adults are
nearly four times more likely to kill
themselves than adolescents. Among
emerging young adult males, the risk of
suicide is six fold compared to females
(Figures 2.1C, 2.1D). In both the U.S
and California, in all age groups, suicide
rates are higher in males with the highest
rate being in males aged 26-34.
60
35
50
30
40
30
Unintentional
Injuries
25
Homicide
20
Suicide
15
20
0
5
Males
Females
12 to 17
Males
Females
18 to 25
Males
Females
0
26 to 34
Source: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury
Statistics Query and Reporting System (WISQARS) [online]. (2005)
40
35
Motor Vehicle
Drowning
Unintentional
Injuries
25
Homicide
20
Suicide
15
5
Motor vehicle accidents account for half of
unintentional-injury deaths in adolescents
and emerging young adults. Compared to
adolescents and young adults, emerging
young adults face the highest risk of motorvehicle-related fatalities
(Figures 2.1F, 2.1G).
Source: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury
Statistics Query and Reporting System (WISQARS) [online]. (2005)
Figure 2.1G
Unintentional Injury Death Rates
(per 100,000) by Type and Age Group,
California, 2009
20
12 to 17
18 to 25
26 to 34
15
10
10
Unintentional Injury Death Rates
(per 100,000) by Type and Age Group,
U.S., 2009
Poisoning
25
30
0
All
30
California has a lower rate of death from
motor vehicle accidents than the U.S. as
a whole (Figures 2.1F, 2.1G).
5
Male
Female
12 to 17
Male
Female
18 to 25
Male
Figure 2.1E
Unintentional injuries account for nearly
half of deaths among Americans aged
15–24 and the death rate has increased
5% (35.7/100,000 to 37.4) since 1997
(Figure 2.1E).
12 to 17
18 to 25
26 to 34
10
10
Female
0
26 to 34
Source: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury
Statistics Query and Reporting System (WISQARS) [online]. (2005)
Trends in Death Rates among
Persons 15-24, U.S., 1997-2007
Figure 2.1F
All
Motor Vehicle
Drowning
Poisoning
Source: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury
Statistics Query and Reporting System (WISQARS) [online]. (2005)
2007: 33,982 Deaths
Heart
Disease
3%
All Other
Causes
17%
Unintentional
Injuries
47%
Cancer 5%
Suicide
12%
Homicide
16%
Source: CDC/NCHS, Health, United States, 2010, Figure 28. Data from the National Vital Statistics System.
14
Mortality
15
3 Injuries
Figure 3.1B
2,500
Take Home Message:
Unintentional Injuries
As noted in section 2, unintentional injuries are the leading cause of mortality among adolescents, emerging
young adults, and young adults in California and the nation. Emerging young adults face the highest risk. Motor
vehicle accidents (MVA) account for the largest percentage of fatal unintentional injuries. Emerging young adults are
more likely to be injured or die in MVAs than adolescents or young adults. Compared to these two other age groups,
emerging young adults also have more MVA-related hospitalizations and emergency department (ED) visits. In 2005,
MVA-related hospitalization and ED treatment of emerging young adults cost the U.S. health care system $9 billion.
2,000
Male
Female
1,500
1,000
500
Intentional Injuries
Homicides and suicides are the second- and third-leading causes of death, respectively, in young people aged
12–34. Major non-fatal intentional injuries include non-sexual assault, sexual assault, firearm injury and suicide
attempts (covered in section 4). Of the three age groups studied, emerging young adults have the highest rate of nonsexual assault. Males are at greatest risk of non-sexual assault; females are at greatest risk of sexual assault. Across all
demographic groups, white females aged 12–25 are the likeliest victims of sexual assault. Emerging young adults are
at greatest risk of firearm injury compared to adolescents and young adults. Emerging young adult males have 10
times the risk of firearm injury compared to females in the same age group.
0
Figure 3.1A
Source: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury
Statistics Query and Reporting System (WISQARS) [online]. (2010)
Figure 3.1C
14
Non-Fatal Motor Vehicle Accident
Occupant Injury Rates (per 100,000)
by Gender, Race, and Age Group,
U.S., 2010
Non-fatal unintentional MVA injuries:
Emerging young adults have the highest
non-fatal injury rates from motor vehicle
accidents, compared to adolescents and
young adults.
Race: Emerging young adult and young
adult black females have the highest nonfatal MVA-related injury rate among all
age, gender and racial groups studied.
10
6
2,500
4
2,000
12 to 17
18 to 25
26 to 34
1,500
1,000
Fatal unintentional MVA injuries: Males
are at greater risk of MVA-related death
than females. Mortality rates peak in males
at age 19; in females, at age 18.
2
0
12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34
Male Female Male Female Male Female Male Female
White
Black
Hispanic
Other
Source: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury
Statistics Query and Reporting System (WISQARS) [online]. (2010)
Figure 3.1D
12
10
8
12 to 17
18 to 25
26 to 34
6
4
2
0
Male
U.S.
Female
Male
Female
California
Source: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury
Statistics Query and Reporting System (WISQARS) [online]. (2009)
16
Fatal mva-Occupant Injury Rates
(per 100,000) by Age and Gender,
u.s., 2009
Source: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury
Statistics Query and Reporting System (WISQARS) [online]. (2009)
500
0
Male
Female
8
3,000
Gender: Females are more likely to
experience non-fatal MVA-related injuries
than males. Non-fatal MVA-related injury
rates peak in females at age 18; in males, at
age 20.
12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34
12
Unintentional Injuries
Non-Fatal MVA-Occupant Injury Rates
(per 100,000) by Age and Gender,
u.s., 2010
Fatal mva-occupant injury rates
(per 100,000) by age and gender,
u.s. and california, 2009
Compared to adolescents and young
adults, emerging young adults are most
likely to die in motor vehicle accidents.
California: In California, as in the nation,
emerging young adults are more likely
than young adults or adolescents to die in
motor vehicle accidents; males have the
highest risk in each age group. However,
fatality rates are lower in California than
the U.S. as a whole.
Injuries
17
3 Injuries continued
Figure 3.1E
total number and cost per
hospitalization for non-fatal mvas
by age group, u.s., 2005
Hospitalizations and ED visits:
Emerging young adults have more
hospitalizations and emergency
department visits due to non-fatal MVAs
than other age groups studied
(Figures 3.1E, 3.1F).
$126,000
40,000
$122,000
30,000
$120,000
Number
Total number and cost per ed visit
for non-fatal mvas by age group,
u.s., 2005
Emerging young adults have 190% more
hospitalizations and 150% more emergency
department visits than adolescents;
emerging young adults have two-thirds
more hospitalizations and 37% more
emergency department visits than young
adults (Figures 3.1E, 3.1F).
12 to 17
18 to 25
number of hospitalizations for nonfatal mvas by gender and age group,
u.s., 2005
Gender: Males have higher numbers
of hospitalizations; females have higher
numbers of ED visits (Figures 3.1G, 3.1H).
$4,000
700,000
$6,000,000,000
$3,000
500,000
$2,500
400,000
$2,000
300,000
$1,500
$1,000
$500
12 to 17
18 to 25
26 to 34
Cost per
ED Visit
Number
100,000
$1,000,000,000
0
30,000
$2,500,000,000
15,000
Work Lost
Total Cost
Figure 3.1J
total, medical, and work lost costs
for ed visits for non-fatal mvas by
age group, u.s., 2005
$2,000,000,000
12 to 17
18 to 25
26 to 34
$1,500,000,000
$1,000,000,000
$500,000,000
5,000
0
Medical Cost
Costs: Compared to adolescents and young
adults, emerging young adults have the
highest medical costs, work-lost costs, and
total costs for ED visits and hospitalizations
due to non-fatal MVAs. Hospitalizations and
emergency room visits for emerging young
adults cost $6.5 billion and $2.6 billion,
respectively (Figures 3.2I, 3.2J).
Source: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury
Statistics Query and Reporting System (WISQARS) [online]. (2005)
$3,000,000,000
12 to 17
18 to 25
26 to 34
12 to 17
18 to 25
26 to 34
$3,000,000,000
35,000
20,000
total, medical, and work lost costs
for hospitalizations for non-fatal
mvas by age group, u.s., 2005
$4,000,000,000
$2,000,000,000
25,000
Figure 3.1I
$5,000,000,000
200,000
0
Female
Source: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury
Statistics Query and Reporting System (WISQARS) [online]. (2005)
$7,000,000,000
600,000
$3,500
Male
800,000
10,000
Male
Female
Source: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury
Statistics Query and Reporting System (WISQARS) [online]. (2005)
18
200,000
0
Source: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury
Statistics Query and Reporting System (WISQARS) [online]. (2005)
Figure 3.1G
12 to 17
18 to 25
26 to 34
50,000
0
26 to 34
$5,000
$4,500
$0
250,000
100,000
Source: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury
Statistics Query and Reporting System (WISQARS) [online]. (2005)
Figure 3.1F
300,000
150,000
10,000
$116,000
$114,000
Cost
Per Hosp
20,000
$118,000
number of ed visits for non-fatal
mvas by gender and age group,
u.s., 2005
350,000
50,000
$124,000
Figure 3.1H
400,000
60,000
$128,000
0
Medical Cost
Work Lost
Total Cost
Source: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury
Statistics Query and Reporting System (WISQARS) [online]. (2005)
Injuries
19
3 Injuries continued
Intentional Injuries
Figure 3.2A
estimated non-sexual assault rates
(per 100,000) by age group and
gender, u.s., 2010
Non-sexual assault victimization rates:
Emerging young adults face the highest
risk of non-sexual assault compared to
adolescents and young adults. Emerging
young adult males are 70% and 50% more
likely to be victimized than adolescent
males and young adult males, respectively.
The victimization rate for emerging young
adult females is 100% and 50% higher
than the rates for adolescent females and
young adult females, respectively
Gender: Across all age groups and races/
ethnicities, males have a higher rate of
non-sexual assault compared to females.
Race: For all age groups, blacks have
the highest rates of non-sexual assault
compared to other races/ethnicities.
Age: Victimization rates increase sharply
as white and black females and white
and Hispanic/Latino males move from
adolescence into emerging young
adulthood.
3,000
2,500
2,000
12 to 17
18 to 25
26 to 34
1,500
1,000
500
0
Figure 3.2B
160
Male Female Male Female Male Female Male Female
Total
White
Black
Hispanic
Source: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury
Statistics Query and Reporting System (WISQARS) [online]. (2010)
140
120
100
12 to 17
18 to 25
26 to 34
80
60
20
Male Female Male Female Male Female Male Female
Total
White
Black
Hispanic
Source: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury
Statistics Query and Reporting System (WISQARS) [online]. (2010)
Race: Black females have the highest rate
of being sexually assaulted in each age
group. Among emerging young adult
females, blacks are 63% and 216% more
likely to be assaulted sexually than whites
or Hispanics/Latinos, respectively.
Figure 3.2C
140
non-fatal firearm injury rates (per
100,000) by gender and age group,
u.s., 2010
120
100
12 to 17
18 to 25
26 to 34
80
60
40
20
0
Sexual assault victimization rates:
Females aged 12–25 have the highest
sexual assault victimization rates.
Gender: Across all age groups, females are
at greater risk for sexual assault than males.
Compared to their male counterparts,
emerging young adult females face 18
times the risk of sexual assault.
40
0
estimated sexual assault rates
(per 100,000) by gender, race and
age group, u.s., 2010
Total
Male
Female
Non-fatal firearm injury rates: Emerging
young adults face the greatest risk of nonfatal shootings. Compared to adolescents
and young adults, emerging young adults
are 220% and 75% more likely to be nonfatally shot, respectively. Emerging young
adult males are 8.6 times more likely to
suffer non-fatal firearm injury than their
female counterparts.
Source: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury
Statistics Query and Reporting System (WISQARS) [online]. (2010)
20
Injuries
21
4 Mental Health
Figure 4.1B
12%
Take Home Message:
Depression and suicidal thoughts, attempts and deaths are major problems in emerging young adults. Compared
to young adults aged 26–34, emerging young adults have higher rates of serious psychological distress and suicidal
thoughts, plans and attempts. Compared to adolescents, emerging young adults are more likely to complete suicides.
It should be noted that people with health insurance are less likely to suffer from depressive disorder than people
without health insurance. For the U.S. overall, 8% of insured individuals and 15.2% of uninsured individuals had
depressive disorders. (Centers for Disease Control and Prevention. MMWR 2010; 59:1229-1235).
Current Depression Among Adults by
Age Group and Type, u.s., 2006-2008
10%
8%
Other
Depression
6%
Major
Depression
4%
Figure 4.1A
Serious Psychological Distress in
Past Month and Past Year, u.s.
(nsduh 2010) and California
(chis 2009)
Nationally: Emerging young adults have
higher rates of past-month and past-year
prevalence of serious psychological stress
compared to young adults (Figure 4.1a).
In the past year, nearly 18% of emerging
young adults report serious psychological
distress; in the past month, nearly 8%
report serious psychological distress.
California: The rates of serious
psychological distress appear lower in
California than in the nation for both
age groups.
20%
Depression: More than 11% of young
adults aged 18-24 have depression
compared to more than 9% of young
adults aged 25 to 34.
2%
18%
0
16%
14%
18-24
25-34
Source: Centers for Disease Control and Prevention. MMWR 2010; 59:1229-1235.
12%
18 to 25
26 to 34
10%
8%
6%
Figure 4.1C
8%
Suicide ideation, plan, and attempt
in past 12 months, u.s., 2010
7%
4%
2%
6%
0
5%
SPD in past Month
SPD in past Year
US (NSDUH)
SPD in past Month
SPD in past Year
CA (CHIS)
Source: United States Department of Health and Human Services. National Survey on Drug Use and Health, 2010 [US data]
and California Health Interview Survey. CHIS 2009 Adult Public Use File [CA data]
18 to 25
26 to 34
4%
3%
2%
1%
0
Suicide Ideation
Suicide Plan
Suicidal thoughts, plans and attempts:
The prevalence of past-year suicidal
thoughts, plans and attempts is higher
among emerging young adults than among
young adults. More than 6% of emerging
young adults report suicidal thoughts in
the past 12 months; nearly 2%, suicidal
plans; more than 1%, a suicide attempt.
Suicide Attempt
Source: United States Department of Health and Human Services. National Survey on Drug Use and Health, 2010
Figure 4.1D
7%
6%
5%
California
U.S.
4%
3%
2%
1%
0
18-29 > or = 30
Suicide Ideation
18-29 > or = 30
Suicide Plan
Suicide ideation, plan, and attempt
in past 12 months by age groups,
u.s. and california, 2009
U.S. and California: Prevalence rates of
suicidal thoughts, plans and attempts were
similar in the young adult population 18-29
comparing the U.S. and California but were
much higher in this age group than those
30 and over (Figures 4.1C & 4.1D).
18-29 > or = 30
Suicide Attempt
Source: Centers for Disease Control and Prevention. MMWR 2011;60(SS13): 1-28.
22
Mental Health
23
5 Substance Abuse
Alcohol
Take Home Message:
50%
Alcohol
40%
Emerging young adults have the “perfect storm” of alcohol risk: i.e., the highest rate of past-month binge
drinking* but the lowest perception of risk; the greatest need for services but lowest access to services. A subset of
emerging young adults, those aged 21–25, is more likely to drive under the influence of alcohol than any other age
group studied.
Tobacco
In both California and the nation, emerging young adults have the highest rates of past-month tobacco and
cigarette use, although the trend has been declining for 20 years.
Illicit Drug Use
Emerging young adults are more likely than other groups studied to use marijuana, cocaine and other illicit
drugs, and to abuse prescription pain relievers. Past-month trends in California and the nation are similar. As with
alcohol, emerging young adults have a “perfect storm” for drug abuse risk: they have lowest perception of marijuanarelated risk, the greatest need for drug abuse services, and the lowest treatment rates
Figure 5.1A
45%
Binge Alcohol Use
in Past Month
35%
30%
Perceptions of Great
Risk of =/> 5 Drinks
Once or Twice a Week
25%
20%
Needing But Not
Receiving Treatment
for Alcohol Use in
Past Year
15%
10%
5%
0
12 - 17
18 - 25
U.S.
26+
12 - 17
18 - 25
26+
California
Source: Substance Abuse and Mental Health Services Administration, State Estimates of Substance Use and Mental Disorders
from the 2008-2009 National Surveys on Drug Use and Health
Binge drinking, perceptions of risk,
and access to care by age group,
u.s. and california, 2008-2009
Emerging young adults have the “perfect
storm” of alcohol risk. They are four times
more likely than adolescents and twice as
likely as young adults to report past-month
binge drinking. They have the lowest
perception of binge drinking risk, the
greatest need for treatment, and the widest
treatment gap; 15% of emerging young
adults who need treatment fail to obtain it,
versus 5% of adolescents and young adults.
Figure 5.1B
35%
binge drinking and heavy alcohol
use by age, u.s., 2010
30%
25%
Binge
Heavy
20%
15%
10%
Binge drinking and heavy alcohol use peaks
between those aged 21–25, with nearly
30% of people in that age group reporting
binge drinking and 15% reporting heavy
alcohol use.
65+
60-64
55-59
50-54
45-49
40-44
35-39
30-34
26-29
21-25
18-20
16-17
14-15
0
12-13
5%
Source: Substance Abuse and Mental Health Services Administration, Results from the 2010 National Survey on Drug Use and
Health: Summary of National Findings
Figure 5.1C
25%
Driving Under the Influence in Past
Year by Age, u.s., 2010
20%
Young people aged 21–25 have the greatest
prevalence (23.4%) of driving under
the influence of alcohol. The prevalence
declines thereafter.
15%
10%
5%
0
*NSDUH Definitions
Binge use - Five or more drinks on the same occasion (i.e., at the same time or within a couple of hours of each other) on at least 1 day in the past 30 days.
Heavy use - Five or more drinks on the same occasion on each of 5 or more days in the past 30 days.
24
16-17
18-20
21-25
26-29
30-34
Source: Substance Abuse and Mental Health Services Administration, Results from the 2010 National Survey on Drug Use and
Health: Summary of National Findings
Substance Abuse
25
5 Substance Abuse continued
Alcohol
Figure 5.1D
100%
90%
80%
Alcohol
in Past
Year
70%
60%
Been
Drunk
50%
40%
5+ drinks
in a row
past two
weeks
30%
20%
40%
“Been drunk” in the past year and binge
drinking rates have declined from the
2008 peak among young people aged
19–28.
25%
44.4%
43.5%
43.4%
43.6%
30%
38.9%
38.7%
39.4%
43.5%
38.3%
38.4%
38.4%
38.1% 37.8%
39.1%
39.1%
35.4%
25%
Not Enrolled
Full Time
in College
Enrolled
Full Time
in College
20%
15%
10%
5%
12-17
18-25
U.S.
26+
12-17
18-25
California
26+
Figure 5.2B
40%
Binge alcohol use among adults
aged 18-22 in the past month by
college enrollment, u.s., 2002-2010
Cigarette use in past month by age,
u.s., 2010
35%
30%
Broken down by specific smaller age
groups, the prevalence of cigarette use in
the past month is above 35% in 21-25 year
olds and 26-29 year olds.
25%
In young people aged 18–22, a subset of
the emerging young adult population,
binge drinking is higher among full-time
college students than those not enrolled
full-time.
20%
15%
10%
5%
5%
0
Emerging young adults in California and
the nation have the highest rates of tobacco
and cigarette use.
Source: Substance Abuse and Mental Health Services Administration, State Estimates of Substance Use and Mental Disorders
from the 2008-2009 National Surveys on Drug Use and Health
44.2%
40.5%
40%
35%
15%
Figure 5.1E
45.5%
Cigarette
Use in Past
Month
20%
1986 1990 1995 2000 2002 2004 2006 2008 2010
44.8%
Tobacco
Product
Use in Past
Month
30%
Tobacco product and cigarette use
in past month by age group, u.s. and
california, 2008-2009
10%
Source: Johnston, L. D., O’Malley, P. M., Bachman, J. G., & Schulenberg, J. E. (2011)
45%
35%
0
50%
Figure 5.2A
45%
Trends in alcohol use, been drunk,
and binge drinking among 19 to 28
year-olds, u.s., 1986-2010
10%
0
Tobacco
0
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
Source: Substance Abuse and Mental Health Services Administration, Results from the 2010 National Survey on Drug Use and
Health: Summary of National Findings
12-13 14-15 16-17 18-20 21-25 26-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65+
Source: Substance Abuse and Mental Health Services Administration, Results from the 2010 National Survey on Drug Use and
Health: Summary of National Findings
Figure 5.2C
40%
35%
8th Grade
30%
10th Grade
25%
12th Grade
20%
College
Students
15%
19-28
Young
Adults
10%
5%
0
1991
1995
2000
2002
2004
2006
2008
Trends in any cigarette smoking past
month by grade and age group, u.s.,
1991-2010
The 30-day prevalence of cigarette smoking
among young people has been trending
downward since 1995. Smoking is more
common among young adults not in college
than college students.
2010
Source: Johnston, L. D., O’Malley, P. M., Bachman, J. G., & Schulenberg, J. E. (2011)
26
Substance Abuse
27
5 Substance Abuse continued
Figure 5.3A
Illicit drug use and illicit drug use
other than marijuna in past month
by age group, u.s. and california,
2008-2009
Emerging young adults in California and
the nation have the highest rates of pastmonth illicit drug use, regardless of whether
marijuana is included (~20%) or excluded
(~8%).
Illicit Drug Use
25%
12%
20%
Illicit Drug Use
in Past Month
15%
Illicit Drug Use
Other Than
Marijuana in
Past Month
10%
5%
0
12-17
18-25
U.S.
26+
12-17
18-25
California
8%
Emerging young adults in California
and the nation have the highest rates of
past-year drug dependence or abuse and
the greatest need for, but not receiving
treatment services.
4%
Illicit Drug
Dependence
or Abuse in
Past Year
6%
5%
Needing But
Not Receiving
Treatment for
Illicit Drug Use
in Past Year
3%
2%
1%
12-17
18-25
U.S.
26+
12-17
18-25
California
26+
4%
12-17
18-25
U.S.
26+
12-17
18-25
California
Cocaine use in past year and nonmedical use of pain relievers in
past year by age group, u.s. and
california, 2008-2009
Compared to other groups, emerging
young adults in California and the nation
have the greatest percentage of past-month
cocaine users and (~6% nationally) and
the highest nonmedical use of prescription
pain relievers (~12% nationally).
26+
Source: Substance Abuse and Mental Health Services Administration, State Estimates of Substance Use and Mental Disorders
from the 2008-2009 National Surveys on Drug Use and Health
Figure 5.3E
Trends in Illicit Drug Use in Past
Month by Age Group, U.S. 2002-2011
20%
15%
12-17
18-25
10%
The NSDUH study shows a slight increase
in illicit drug use between 2008 and 2011
in all age groups with largest increase in
emerging young adults.
26 or Older
5%
0
Source: Substance Abuse and Mental Health Services Administration, State Estimates of Substance Use and Mental Disorders
from the 2008-2009 National Surveys on Drug Use and Health
Figure 5.3C
Nonmedical
Use of Pain
Relievers in
Past Year
6%
25%
7%
0
8%
0
26+
9%
Illicit drug dependence or abuse
in past year and needing but not
receiving treatment by age group,
u.s. and california, 2008-2009
Cocaine
Use in
Past Year
10%
2%
Source: Substance Abuse and Mental Health Services Administration, State Estimates of Substance Use and Mental Disorders
from the 2008-2009 National Surveys on Drug Use and Health
Figure 5.3B
Figure 5.3D
14%
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
Source: Substance Abuse and Mental Health Services Administration, Results from the 2010 National Survey on Drug Use and
Health: Summary of National Findings
45%
Marijuana use in past month and
perception of great risk of smoking
marijuana once a month by age
group, u.s. and california, 2008-2009
40%
Emerging young adults in California and
the nation have the highest past-month
marijuana use (>15%) and the lowest
perception of marijuana-related risk.
20%
35%
Marijuana
Use in Past
Month
30%
25%
Perception
of Great Risk
of Smoking
Marijuana
Once a Month
15%
10%
5%
0
12-17
18-25
U.S.
26+
12-17
18-25
California
26+
Source: Substance Abuse and Mental Health Services Administration, State Estimates of Substance Use and Mental Disorders
from the 2008-2009 National Surveys on Drug Use and Health
28
Substance Abuse
29
5 Substance Abuse continued
Table 5.3A
Table 5.3B
annual prevalence of use for various types of drugs among respondents 1 to 4 years beyond high
school by gender and full-time colllege vs. others, u.s., 2011
Trends in annual prevalence of various types of drugs among respondents of model ages 19-28,
u.s., 1986-2011
In general, non-college students have higher past-year drug use than college students in all categories except
marijuana, Adderall and “being drunk.” Marijuana usage is about the same.
Trends: Longer term declines of annual drug usage appeared to end in 1992 or 1993. Among the sample of 19–28
year olds, this was true for the use of any illicit drug, marijuana, any illicit drug other than marijuana, hallucinogens,
narcotics other than heroin, crack, amphetamines, sedatives (barbiturates), and tranquilizers.
Total
Males
Females
Full-Time
College
Others
Full-Time
College
Others
Full-Time
College
Others
Any Illicit Drug
35.0
35.8
40.3
35.7
31.6
35.8
Any Illicit Drug other than marijuana
17.1
21.0
20.3
22.4
15.1
20.0
Marijuana
32.7
31.9
39.0
33.2
28.5
30.9
Inhalants
1.7
2.5
2.9
2.8
0.9
2.3
Hallucinogens
4.9
5.8
7.3
8.2
3.4
4.0
LSD
2.1
1.8
2.7
2.2
1.7
1.4
Hallucinogens other than LSD
4.4
5.4
6.6
7.5
2.9
3.7
Ecstasy (MDMA)
4.3
6.2
5.3
7.7
3.6
Salvia
3.6
5.5
7.3
9.7
Cocaine
3.5
4.9
4.3
Crack
0.4
0.9
Other Cocaine
4.0
1986
1989
1992
1995
1998
2001
2004
2007
2011
Any Illicit Drug
41.9
32.8
28.3
29.8
29.9
32.1
33.7
32.5
34.7
Any Illicit Drug other than marijuana
27.0
18.3
14.1
13.8
13.2
15.4
18.8
18.1
17.6
Marijuana
36.5
29.0
25.2
26.5
27.4
29.2
29.2
28.5
31.0
Inhalants
1.9
1.9
1.9
2.4
2.1
1.7
1.7
0.8
0.8
Nitrites
2.0
-
0.1
-
-
-
-
-
-
4.5
3.6
5.0
5.6
5.2
5.4
4.7
3.8
3.7
LSD
3.0
2.7
4.3
4.6
3.5
3.4
0.9
1.1
1.7
Hallucinogens other than LSD
2.5
1.8
1.9
2.5
3.0
3.5
4.5
3.6
3.2
PCP
Hallucinogens
0.8
-
0.3
0.3
0.6
0.6
0.1
0.3
0.3
Ecstasy (MDMA)
-
1.4
1.0
1.6
2.9
7.5
3.5
2.5
3.6
5.0
Salvia
-
-
-
-
-
-
-
-
2.5
1.1
2.7
Cocaine
19.7
10.8
5.7
4.4
4.9
5.8
7.1
6.2
4.7
6.0
3.0
4.0
Crack
3.2
2.5
1.4
1.1
1.1
1.3
1.3
1.0
0.6
0.6
0.5
0.3
1.2
4.0
5.1
3.6
3.3
4.3
0.2
0.7
0.3
0.6
0.2
0.8
*
0.2
*
0.4
*
*
0.3
0.4
*
0.4
0.5
0.4
7.2
11.2
8.5
10.6
6.3
11.7
OxyContin
2.3
4.0
2.2
6.1
2.3
2.3
Vicodin
4.9
9.9
5.6
9.3
4.4
10.4
9.0
7.9
11.6
7.9
7.4
8.0
Heroin
With a Needle
Without a Needle
Narcotics other than Heroin
Amphetamines, adjusted
Other Cocaine
Heroin
With a Needle
Without a Needle
10.3
5.1
3.9
4.5
5.3
6.4
5.6
4.3
0.2
0.2
0.4
0.4
0.5
0.3
0.3
0.5
-
-
-
0.1
0.1
0.3
0.1
0.1
0.4
-
-
-
0.3
0.6
0.9
0.3
0.3
0.2
3.1
2.8
2.5
3.0
3.4
5.0
9.0
8.7
7.9
OxyContin
-
-
-
-
-
-
3.1
2.9
2.8
Vicodin
-
-
-
-
-
-
8.9
8.9
7.1
10.6
5.8
4.1
4.6
4.5
5.8
6.2
5.6
7.2
Ritalin
-
-
-
-
-
-
2.7
2.4
1.5
-
-
-
-
-
-
-
-
6.6
Narcotics other than Heroin
Amphetamines, adjusted
Ritalin
1.9
2.0
2.8
2.3
1.3
1.9
Adderall
Adderall
9.0
7.1
11.2
7.4
7.5
6.9
Provigil
-
-
-
-
-
-
-
-
0.3
-
-
-
-
-
2.8
2.8
1.5
0.5
-
-
0.4
1.2
1.1
1.1
1.5
1.1
0.5
*
1.7
*
2.9
*
0.7
Methamphetamine
Methamphetamine
0.4
1.1
1.2
0.7
*
1.3
Crystal Methamphetamine
Crystal Methamphetamine (Ice)
0.5
0.7
0.2
0.3
0.7
0.9
Sedatives (Barbiturates)
2.3
1.7
1.6
2.1
2.5
3.7
4.4
4.2
3.2
Sedatives, adjusted
3.0
1.8
-
-
-
-
-
-
-
Methaqualone
1.3
0.3
-
-
-
-
-
-
-
5.4
3.7
3.4
3.4
3.8
5.5
7.4
7.1
5.9
Rophynol
-
-
-
-
-
-
0.1
0.3
-
GHB
-
-
-
-
-
-
0.5
0.4
0.3
Ketamine
-
-
-
-
-
-
0.6
0.3
0.5
88.6
88.1
86.2
84.7
84.0
84.3
84.4
84.0
83.5
-
-
60.9
61.6
59.6
63.1
63.8
65.8
64.0
Provigil
Sedatives (Barbiturates)
2.5
4.9
2.7
4.9
2.4
5.0
Tranquilizers
4.9
7.6
5.8
7.9
4.3
7.4
GHB
0.1
1.2
*
1.9
0.2
0.7
Ketamine
0.7
2.0
0.2
3.6
1.0
0.7
Alcohol
78.6
71.8
80.8
71.5
77.1
72.1
Been Drunk
63.8
52.9
69.7
51.2
60.2
54.1
Flavored Alcoholic Beverages
60.3
52.4
58.7
45.8
61.4
58.3
Cigarettes
28.1
39.9
32.8
41.4
25.1
38.8
Steroids
0.3
2.7
0.5
6.6
0.1
*
Tranquilizers
Alcohol
Been Drunk
Flavored Alcoholic Beverages
Cigarettes
Steroids
Source: Johnston, L.D., O’Malley, P.M., Bachman, J.G., & Schulenberg, J.E. (2011). Adapted from Table 8-2
30
0.2
-
-
-
-
-
-
62.7
58.9
56.3
40.1
38.0
37.9
38.8
41.6
41.1
39.0
36.2
31.5
-
0.5
0.4
0.5
0.4
0.4
0.5
0.7
0.2
Source: Johnston, L.D., O’Malley, P.M., Bachman, J.G., & Schulenberg, J.E. (2011). Adapted from Table 5-2
Substance Abuse
31
6 Reproductive Health
Take Home Message:
70%
Sexual Activity
60%
Reproductive health issues are of major significance in terms of preventing many health risks including
unintended pregnancy and sexually transmitted infections (STIs). The prevalence of sexual activity in the past 12
months increases with age and is between 70% and 80% in emerging young adults but varies depending on age,
race, and gender.
Pregnancy and Birth Rates
Birth rates peak in young adults aged 25–29. While trends show a decrease in birth rates since 1980 in
adolescents and young adults until age 29, there has been a continuing rise in the percent of pregnancies resulting in
a live birth in this age group. The highest percent of Medi-Cal funded therapeutic abortions (TABs) in California is
in the young adult population aged 18–24.
Contraception
50%
Figure 6.1B
57.4%
55.6%
54.0%
48.9%
50.8% 50.2%
52.1%
52.2%
48.5% 48.0%
47.9%
49.8%
45.3%
45.7%
45.9% 45.7%
52.1% 47.7%
40%
42.9%
46.1%
30%
20%
10%
0
Alcohol, Drugs, and Sexual Behaviors and Risks
Alcohol is frequently used during sexual activity and can result in unprotected sexual activity and non-consensual
sexual activity.
1991 1993 1995 1997 1999 2001 2003 2005 2007 2009
Figure 6.1C
100%
90%
80%
70%
Received
Oral Sex
60%
50%
Sexual activity: Sexual activity in the past
12 months rises with age and is between
70% and 80% in emerging young adults
depending on gender and race.
Gave
Oral Sex
40%
Sexual Activity
any sexual activity within last 12
months by race, gender, and age
group, u.s., 2006-2010
High school students: 46% of high
school students report ever having sexual
intercourse and this has trended downward
since 1991 (54.1%). More males than
females report ever having sexual activity,
though the gap between them appears to
have decreased over time.
Source: Centers for Disease Control and Prevention (CDC). 1991-2009 High School Youth Risk Behavior Survey Data.
Condoms and birth control pills are the most frequently used methods of contraception. While condom use has
been increasing in high school students over time and is above 60%, the frequency of “always” using a condom is
much lower.
Figure 6.1A
Male
Female
Total
percentage of high school students
who ever had sexual intercourse by
gender, 1991-2009
30%
Oral sex: Participation in oral sex increases
with age and is fairly similar between males
and females.
20%
100%
10%
90%
0
80%
70%
15-17
60%
18-25
50%
26-34
40%
Male Female Male Female Male Female Male Female Male Female
14-15
16-17
18-19
20-24
25-29
Source: Herbenick D, Reece M, et al, 2010
Figure 6.1D
100%
30%
percent reporting lifetime vaginal
intercourse by age group and
gender, u.s., 2010
90%
20%
80%
10%
0
percent reporting lifetime oral sex
behaviors by gender and age group,
U.s., 2010
Hispanic
White
Male
Black
Source: National Survey of Family Growth 2006-2010
Hispanic
White
Female
Black
70%
Male
Female
60%
50%
40%
30%
20%
10%
0
14-15
16-17
18-19
20-24
25-29
30-39
Vaginal intercourse: Likewise, the percent
of individuals reporting lifetime vaginal
intercourse increases with age and there are
not large differences between males and
females, with the exception of those aged
20–24. 85.6% of females in this age group
reported ever having vaginal intercourse
compared to 70.3% of males.
Source: Herbenick D, Reece M, et al, 2010
32
Reproductiive Health
33
6 Reproductive Health continued
Figure 6.1E
lifetime number of opposite sex
sexual partners by gender and age
group, u.s., 2006-2010
Lifetime partners: Number of lifetime
sexual partners increases with age and is
consistently higher among males than
females. Among 18–25 year olds, twice as
many males reported having 11 or more
lifetime sexual partners than females (18%
vs. 9%, respectively).
Pregnancy and Birth Rates
Figure 6.2A
pregnancy rates and outcomes
(per 1,000) by age groups of mother,
u.s., 2006
Pregnancy Rates: Pregnancy rates increase
with age up through age 29 (Figure 6.2a,
b). The percentage of pregnancies that end
in births also increases with age, while the
percent ending in abortions decreases and
miscarriages remain fairly constant.
80%
70%
60%
40%
30%
pregnancy rates (per 1,000 women)
by age group and intention, u.s., 2006
Intention: The percent of total
pregnancies that are unintended decreases
with age. Despite the rates of unintended
pregnancies being highest in women
aged 20–24, this comprises 64% of all
pregnancies in comparison to 82% in the
15-19 age group.
20%
10%
0
Male
Female
15-17
Male
Female
18-25
Male
Female
26-34
0
Source: National Survey of Family Growth 2006-2010
<15
15-19
20-24
25-29
30-34
Source: Finer LB & Zolna MR, 2011
Figure 6.2D
120
180
160
15%
140
15%
100
26%
80
60
62%
20
13%
43%
Miscarriages
Abortions
Births
60
40
<14
14%
29%
20
56%
44%
Birth rates: Birth rates peaked at 108.3
per 10,000 in women aged 25–29 in
2010.
80
60%
40
birth rates (per 1,000) by age of
mother, u.s., 2010
100
23%
120
15-17
18-19
0
20-24
Total
10-14 yrs 15-19 yrs 20-24 yrs 25-29 yrs 30-34 yrs 35-39 yrs 40-44 yrs
Source: Hamilton BE, Martin JA, & Ventura SJ, 2011
Figure 6.2E
140
200
180
120
160
64%
140
33%
100
80
60
15-19
100
41%
120
82%
40
0
Abortion: The percent of unwanted
pregnancies that end in abortion range
from 37% among 15-19 year olds to 49%
among girls younger than 15 (Figure 6.2C).
Among women aged 20–24, 23% of all
pregnancies result in abortion, but this
number jumps to 41% when the pregnancy
is unwanted (Figure 6.2A, 6.2C).
30%
10%
20
Unintended
Intended
20-24
80
25-29
60
30-34
40
35-39
40-44
20
100%
<15
15-19
20-24
(% listed indicates percent of total pregnancies that are unintended)
Source: Finer LB & Zolna MR, 2011
34
40%
20%
Source: Kost K, Henshaw S, & Carlin L, 2011
Figure 6.2B
percent of unwanted pregnancies
ending in abortion by age of mother,
u.s., 2006
50%
0
1-5
6-10
11-25
26 +
50%
0
Figure 6.2C
60%
25-29
30-34
0
1990
1995
2000
2005
trends in birth rates (per 1,000) by
age group of mother, u.s., 1990-2010
Trends: Trends show a decrease of birth
rates in adolescents and young adults until
age 29 with rates rising over time in those
aged 30 and over. Young adults 20–24
show a decrease from 1990 to 2010 from
~120/1,000 women to ~ 90/1,000 women.
Adolescents aged 15–19 have shown an
almost 50% reduction in birth rates from
1990 to 2010 ~60/1,000 to 34.4/1,000.
2010
Source: Hamilton BE, Martin JA, & Ventura SJ, 2011
Reproductiive Health
35
6 Reproductive Health continued
90%
18%
80%
16%
70%
15 to 17
18 to 25
26 to 34
60%
50%
40%
contraceptive methods* used at
last sex among females who have
had sex in the past 12 months
by age group, u.s., 2006-2010
20%
Im
or pla
Pa nt
tch
Inj
ec
tio
n
Rin
g
Wi
thd
raw
Ste al
rili
zat
ion
Ot
he
r
Me No
tho
d
2%
IUD
0
0
7.5%
8.0%
8.5%
6.0%
5.5%
6.6%
4.6%
3.4%
2001
Only 8.9% of high school students
used both a condom and either birth
control pills or Depo-Provera to prevent
pregnancy before their last sexual
intercourse. However, the percent using
both of these methods has increased from
4.8% in 1999 to 8.9% in 2009.
7.8%
7.0%
1999
Total
7.5%
2003
2005
2007
percentage of high school students
who used both a condom and birth
control pills or depo-provera to
prevent pregnancy before last
sexual intercourse, 1999-2009
2009
Source: Centers for Disease Control and Prevention (CDC). 1991-2009 High School Youth Risk Behavior Survey Data.
100%
90%
80%
Alcohol, Drugs, and Sexual Behaviors and Risks
70%
15 to 17
18 to 25
26 to 34
60%
50%
18%
16%
10%
10%
0
8%
do
Im
or pla
Pa nt
tch
Inj
ec
tio
n
Rin
g
Wi
thd
raw
Ste al
rili
zat
ion
Ot
he
r
Me No
tho
d
12%
IUD
20%
Pil
l
14%
m
30%
Co
n
High school students: Almost two
thirds of sexually active high school
students reported using a condom the last
time they had sexual intercourse and this
has increased since 1991.
Female
9.8%
10%
4%
0
0.4%
Unprotected
Intercourse
Had Sexual Intercourse
without Giving Consent
Source: American College Health Association: NCHA Report Fall 2009
80%
70%
55%
59%
50%
30%
1.9%
2%
90%
40%
consequences as a result of drinking
in past 12 months among college
students, u.s., 2009
Alcohol and drugs: Alcohol and drugs
play a role in sexual activity in adolescents
and young adults and can lead to risky
behaviors.
4%
100%
60%
Figure 6.4A
16.2%
6%
*Respondents could select up to four methods
Source: National Survey of Family Growth 2006-2010
percent of currently sexually active
high school students who used a
condom at last intercourse, u.s.,
1991-2009
Male
12%
10%
40%
Figure 6.3C
14%
6%
*Respondents could select up to four methods
Source: National Survey of Family Growth 2006-2010
Figure 6.3B
Figure 6.3D
8%
30%
Pil
l
Methods: Among sexually active males
and females aged 18–25, condoms and
birth control pills were the most frequently
used contraceptive method at last sex at
55% and 37%, respectively for males and
41% and 32% for females
(Figure 6.3A, 6.3B).
20%
om
contraceptive methods* used at
last sex among males who have
had sex in the past 12 months by
age group, u.s., 2006-2010
100%
Co
nd
Figure 6.3A
Contraception
46%
61%
49%
63%
66%
65%
69%
70%
69%
57%
56%
55%
69%
Had Sexual Intercourse
without Getting Consent
Consequences: College students report
that secondary to alcohol, 16.2% had
unprotected sex, 1.9% had sexual
intercourse without giving consent and
0.4% had sexual intercourse without
getting consent.
Male
Female
51%
51%
51%
54%
Total
38%
20%
105
0
1991 1993 1995 1997 1999 2001 2003 2005 2007 2009
Source: Centers for Disease Control and Prevention (CDC). 1991-2009 High School Youth Risk Behavior Survey Data.
36
Reproductiive Health
37
7 Sexually Transmitted Infections
6,000
2,000
Male
The highest incidence rates of syphilis are in young adult males aged 20–29. Among young adults aged 20–29,
incidence rates for syphilis are highest in black males.
HIV
The largest number of HIV diagnoses are occurring among emerging young adults aged 20–24.
California/US: Incidence rates are slightly
lower in California than in the U.S. as a
whole. This is most noticeable in 15–24
year old females.
Male
Male
Female
Hispanic
Male
25-29
20-24
25-29
20-24
25-29
20-24
25-29
20-24
25-29
20-24
Female
Black
Source: Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2010. [U.S. data] and Sexually
Transmitted Diseases in California, 2010. [CA data]
Figure 7.1C
10-14
1,500
15-19
20-24
3,500
1,000
3,000
2,500
California
U.S.
2,000
1,500
1,000
Gender/Racial difference: Incidence
rates in young adults are highest in Black
females 20-24, followed by Black males
20–24, and Hispanic females 20–24.
Lowest incidence rates in young adults
20–29 were in white and Asian males.
Female
2,000
4,000
chlamydia rates (per 100,000) by
age group, gender, and race
among 20-29 year olds,
u.s. and california, 2010
Asian/PI
2,500
Chlamydia
Chlamydia Incidence rates: The highest
incidence rates of chlamydia are in young
adult males 20–24 and adolescent and
young adult females 15–24.
Female
White
25-29
0
20-24
1,000
Syphilis
chlamydia rates (per 100,000) by
age group and gender, u.s. and
california, 2010
California
U.S.
3,000
25-29
Similar to chlamydia, the highest incidence rates of gonorrhea are in young adult males aged 20–24 and in older
adolescent and young adult females aged 15–24. Incidence rates in young adults are highest in Black females 20–24,
followed by Black males 20–24.
4,000
20-24
Gonorrhea
5,000
25-29
The highest incidence rates of chlamydia among males is in young adult males aged 20-24 and among females the
highest rates are in adolescent and young adult females aged 15-24. Incidence rates in young adults are highest in
African American females 20–24, followed by African American males 20–24.
20-24
Chlamydia
Figure 7.1A
Figure 7.1B
7,000
Take Home Message:
25-29
30-34
500
0
2005
2006
2007
2008
2009
trends in chlamydia incidence
rates (per 100,000) by age group,
u.s., 2006-2010
Trends: Incidence rates were always highest
in the 20–24 age group both nationally and
in California.
U.S.: Nationally, incidence rates appear
to be increasing in 20–24 and 15–19 year
olds and rates are higher in these age groups
than in California.
2010
Source: Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2010.
500
0
10-14 15-19 20-24 25-29 30-34 10-14 15-19 20-24 25-29 30-34
Male
Female
Source: Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2010. [U.S. data] and Sexually
Transmitted Diseases in California, 2010. [CA data]
Figure 7.1D
2,500
2,000
10-14
1,500
15-19
20-24
1,000
25-29
California: Chlamydia incidence rates are
higher in the 25 to 29-year-old age group
in California than in the U.S..
30-34
500
0
trends in chlamydia incidence
rates (per 100,000) by age group,
california, 2005-2010
2005
2006
2007
2008
2009
2010
Source: Sexually Transmitted Diseases in California, 2010.
38
Sexually Transmitted Infections
39
7 Sexually Transmitted Infections continued
Gonorrhea
600
Figure 7.2A
500
gonorrhea rates (per 100,000) by
age group and gender, u.s. and
california, 2010
Gonorrhea Incidence rates: Similar to
chlamydia, the highest incidence rates
of gonorrhea are in older adolescent and
young adult females 15–24 and young
adult males 20–24 compared to younger
adolescents and young adults over 24.
600
15-19
300
400
California
U.S.
300
100
100
0
25-29
30-34
2005
2006
2007
2008
2009
2,000
250
15-19
200
20-24
150
25-29
100
30-34
1,000
10-14
trends in gonorrhea rates (per
100,000) by age group, california,
2005-2010
California: Incidence rates decreased in all
age groups from 2005–2009.
50
500
White
Black
Hispanic
25-29
Male
20-24
25-29
Female
20-24
25-29
Male
20-24
25-29
Female
20-24
25-29
Male
20-24
25-29
Female
20-24
25-29
Male
20-24
25-29
0
0
U.S.: Gonorrhea incidence rates were
higher in the U.S. than in California
regardless of age group.
Figure 7.2D
400
300
California
U.S.
Trends: Incidence rates were always
highest in the 20–24 age group
(Figure 7.2C, 7.2D).
Source: Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2010.
2,500
1,500
trends in gonorrhea incidence
rates (per 100,000) by age group,
u.s., 2006-2010
2010
350
20-24
Gender/Racial difference: In young
adults, incidence rates are highest in Black
females 20-24, followed by Black males
20–24, with large drops in other ethnic
groups. The lowest rates in young adults
aged 20–29 were in the Asian/Pacific
population.
20-24
200
200
Transmitted Diseases in California, 2010. [CA data]
gonorrhea rates (per 100,000) by
age group, gender, and race among
20-29 years olds, u.s. and california,
2010
10-14
400
500
California/US: Incidence rates are much
0
10-14 15-19 20-24 25-29 30-34 10-14 15-19 20-24 25-29 30-34
lower in California then in the U.S. as a
Male
Female
whole for all age groups of females and most
Source: Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2010. [U.S. data] and Sexually
noticeably lower in males aged 15–24.
Figure 7.2B
Figure 7.2C
2005
2006
2007
2008
2009
2010
Source: Sexually Transmitted Diseases in California, 2010
Female
Asian/PI
Source: Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2010. [U.S. data] and Sexually
Transmitted Diseases in California, 2010. [CA data]
40
Sexually Transmitted Infections
41
7 Sexually Transmitted Infections continued
Figure 7.3A
syphilis rates (per 100,000) by
age group and gender, u.s. and
california, 2010
Syphilis Incidence rates: The incidence
rates of syphilis increase with age and
peak in the U.S. in 20-24 year olds. In
California males, the peak incidence is in
30–34 year olds.
Gender: Young adult males aged 20–24 in
the U.S. have a 3.9 times greater incidence
rate of syphilis compared to U.S. females.
Californian young adult males have rates
nearly 20 times that of Californian females
aged 20–24.
Figure 7.3C
16
Syphilis
14
25
12
10-14
10
20
California
15
U.S.
10
15-19
8
20-24
6
25-29
4
30-34
2
5
0
0
2006
2007
2008
2009
U.S.: Incidence rates have trended upward
between 2006 and 2010 and are highest
among 25–29 and 20–24 year olds.
2010
Female
Source: Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2010. [U.S. data] and Sexually
Transmitted Diseases in California, 2010. [CA data]
Figure 7.3D
14
trends in syphilis rates (per 100,000)
by age group, california, 2005-2010
12
California/US: Among females, incidence
rates are higher in the U.S. compared to
California.
10
10-14
15-19
8
Figure 7.3B
Trends: Incidence rates differ among and
age groups and in trends in the U.S. and
California (Figure 7.3C, 7.3D)
Source: Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2010.
10-14 15-19 20-24 25-29 30-34 10-14 15-19 20-24 25-29 30-34
Male
2005
trends in syphilis incidence rates
(per 100,000) by age group, u.s.,
2006-2010
100
6
syphilis rates (per 100,000) by age
group, gender, and race among 20-29
year olds, u.s. and california, 2010
90
4
Racial difference: In young adults, the
incidence rates are highest in Black males
20-29, followed by Black females 20–24
and Hispanic males 20–29. The lowest rates
in young adults aged 20–29 were in the
White and Asian/Pacific female population.
50
80
20-24
California: Between 2005 and 2010,
syphilis rates in California have fluctuated,
with 25 to 29 year olds and 30 to 34 year
olds having the highest rates in 2010.
25-29
30-34
2
70
60
California
U.S.
40
0
2005
2006
2007
2008
2009
2010
Source: Sexually Transmitted Diseases in California, 2010
30
20
25-29
Male
20-24
25-29
Female
Hispanic
20-24
25-29
Male
20-24
25-29
Female
Black
20-24
25-29
Male
20-24
25-29
Female
White
20-24
25-29
Male
20-24
25-29
0
20-24
10
Female
Asian/PI
Source: Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2010. [U.S. data] and Sexually
Transmitted Diseases in California, 2010. [CA data]
42
Sexually Transmitted Infections
43
7 Sexually Transmitted Infections continued
Figure 7.4A
number of diagnoses of hiv infection
by age group, u.s., 2010 (46 states
with confindential reporting)
HIV: The largest number of HIV diagnoses
are occurring among emerging young adults
aged 20–24.
35%
8,000
30%
7,000
25%
6,000
20%
5,000
15%
4,000
10%
3,000
5%
2,000
0
1,000
0
rate (per 100,000) of diagnoses of
hiv infection by age group and race,
u.s., 2010 (46 states with confidential
reporting)
Race: Rates of HIV diagnoses are highest
in Blacks regardless of age and peak at
148.3 per 100,000 among emerging young
adults aged 20–24. This is nearly 4 times
as high as Hispanics and 12 times as high
as whites of the same age group.
Male
Female
13-14
15-24
25-34
35-44
AIDS: The percent distribution of AIDS
diagnoses increases with age in both males
and females, peaks in the 35–44 year old
age group and declines thereafter.
45-54
13-14
15-19
20-24
25-29
30-34
35-39
Figure 7.4D
45%
trends in percent of all cases of
diagnosis of aids by age groups,
u.s., 2005-2009
40%
160
35%
140
30%
120
25%
Black
100
Hispanic
White
80
60
13-14
15-24
20%
25-34
15%
35-44
10%
5%
40
0
20
0
distribution percent of diagnosis
of aids by age at diagnosis and
gender, u.s., 2005-2009
Source: National Center for Health Statistics. Health, United States, 2010
Source: Centers for Disease Control and Prevention. HIV Surveillance Report, 2010; vol. 22.
Figure 7.4B
Figure 7.4C
40%
HIV/AIDS
2005
2006
2007
Trends: Since 2005, trends in the percent
of all cases of AIDS diagnosis have been
decreasing in the 35–44 year old age group
with a corresponding increase among
emerging young adults and young adults
aged 15–34.
2008
Source: National Center for Health Statistics. Health, United States, 2010
13-14
15-19
20-24
25-29
HPV
30-34
Source: Centers for Disease Control and Prevention. HIV Surveillance Report, 2010; vol. 22.
Figure 7.5A
7
6
5
Male
Female
4
3
2
rate (per 100,000 person-years) of
genital warts prevalence among
individuals in private health plans
by age group and gender, u.s., 2000
Genital warts: Rates peaked in females
20–24 (~6/1,000 person years), who had
about twice the rate of males the same age.
1
0
10-14
15-19
20-24
25-29
30-34
Source: Insinga RP, Dasbach EJ & Myers ER, 2003
44
Sexually Transmitted Infections
45
8 Chronic Disease
Take Home Message:
In the U.S. there are over 16.3 million cases of the top seven common chronic diseases — cancers, diabetes,
heart disease, hypertension, stroke, mental disorders and pulmonary conditions. Many of these are also significant
problems in young adults and three — cancer, heart disease, and mental disorders (suicide) — are among the top
five causes of mortality in young adults. These conditions can shorten lives and reduce the quality of life. Many
chronic diseases either continue or start in the young adult years and others such as heart disease, stroke and diabetes
can be prevented with interventions during the adolescent and young adult years. There is both a human and
economic cost to these chronic disease states. In the U.S. in 2003, the costs amounted to $277 billion in treatment
expenditures and $1,047 billion in lost productivity. In California, the respective costs were $27 billion and $106
billion.
Prevention: It is estimated that with reasonable improvements in preventing and managing chronic disease,
the U.S. could prevent 40.2 million chronic disease cases in 2023 and 4.3 million cases in California in 2023.
The avoided economic costs could be $218 billion (28%) for treatment in U.S. and $905 billion (27%) for lost
productivity. This would translate to savings in California of $19 billion (26%) and $98 billion (27%) respectively
(Source: Devol, R. and Bedroussian, A., October 2007).
Asthma
15%
Nationally, approximately 3% of emerging young adults have been told they have any kind of heart condition or
disease. In California, the prevalence of heart disease is around 1%. High total cholesterol increases with age.
Epilepsy
0
Nationally, obesity increases with age. Obesity prevalence rates have skyrocketed from 9.7% in females aged
20–34 in 1971–74 to 31.4% in 2005–2008; the numbers in males of the same age have increased from 8.9% to
25.4% over the same time period.
12-17
18-25 26-34
California
Male
Female
Total
5%
0
In the U.S. and California, the prevalence
of ever being diagnosed with asthma
decreases with each age group. The
prevalence of ever being diagnosed with
asthma in the U.S. in emerging young
adults is 16.2% in males and 16.9%
in females. These prevalence rates in
Californian emerging young adults are
slightly higher—18.3% in males and
17.9% in females.
Figure 8.1B
10%
Total
Non-Hispanic
White
Non-Hispanic
Black
lifetime asthma prevalence by race
and gender among 20-24 year olds,
u.s., 2010
Racial Differences: The prevalence of
asthma in young adults aged 20–24 is
lowest in Hispanics for both sexes. The
highest prevalence in this age group is
among black males.
Hispanic
Source: 2010 National Health Interview Survey (NHIS) Prevalence Data
12%
Obesity
26-34
15%
Renal Disease
According to the CDC, in 2005, the prevalence of self-reported disabilities among non-institutionalized U.S.
adults 18 and over was 21.8% encompassing 47.5 million Americans. The proportion of the population with a
disability increased with age and was 11% in those 18 to 44. Overall, more women in the U.S. have a disability
(24.4%) than men (19.1%) both overall and in all age groups (Centers for Disease Control and Prevention:
Prevalence and Most Common Causes of Disability among Adults).
18-25
U.S.
30%
14%
Disability
12-17
Sources: National Health Interview Survey 2010. Sample Adult File and Sample Child File [U.S. data] and 2009 California
Health Interview Survey [CA data]
1.8% of emerging young adult males and 0.9% of emerging young adult females have been diagnosed with
epilepsy.
Renal disease rates are higher among young adults aged 26–34 than emerging young adults for both genders.
Female
5%
20%
Cardiovascular
Male
10%
Diabetes
The lowest improvements in cancer survival rates in the past 25 to 35 years occur in young adults aged 20 – 35.
This may be related to many factors including potential differences in involvement in treatment protocols, treatment
centers and access to health care.
prevalence of ever being diagnosed
with asthma by age group and
gender, u.s., 2010 and california, 2009
20%
25%
Cancer
Figure 8.1A
25%
The prevalence of ever being diagnosed with asthma decreases with age and is slightly lower in the U.S. than in
California. Current asthma diagnosis is higher among emerging young adults than young adults.
The prevalence of diabetes, pre-diabetes and gestational diabetes increases with age in the U.S.
46
Asthma
Figure 8.1C
current asthma prevalence by age
group and gender, u.s., 2010 and
california, 2009
10%
8%
Male
6%
Female
4%
2%
0
12-17
18-25
U.S.
26-34
12-17
18-25 26-34
California
Currently have asthma: In the U.S.,
emerging young adults have a greater
prevalence of current asthma than young
adults. 7.7% of emerging young adult
males report currently having asthma
compared with 5.9% of young adult
males and 11.2% of emerging young adult
females compared with 8.6% of young
adult females.
Sources: National Health Interview Survey 2010. Sample Adult File and Sample Child File [U.S. data] and California Health
Interview Survey. CHIS 2009 Adult Survey and CHIS 2009 Teen Survey [CA data]
Chronic Disease
47
8 Chronic Disease continued
Figure 8.2A
diabetes and pre-diabetes
prevalence by gender and age
group, u.s., 2010
U.S.: The prevalence of diabetes, prediabetes and gestational diabetes increases
with age in the U.S. The rate for diabetes
is approximately 1% in emerging
young adults and nearly doubles in the
26–34-year-old population.
Gestational diabetes: The prevalence
of gestational diabetes increases with
age, although there are large differences
between national and state prevalence
rates in young adults aged 26–34.
Nationally 3.6% of women aged 26–34
have gestational diabetes compared to
6.2% in Californian women of same age
(Figures 8.2A, 8.2B, 8.2C).
Figure 8.2B
Diabetes and Pre-Diabetes
Prevalence by Gender and Age
Group, California, 2010
California: The prevalence rates of
diabetes in emerging young adults are
higher in females in California (1.5%
versus 1.1% U.S.) and lower in males
in California (0.4% versus 0.9% U.S.)
(Figures 8.2A, 8.2B).
Figure 8.2C
2.5%
Diabetes
Prevalence Ever Diagnosed with
Diabetes by Gender and Age Group,
U.S., 2009-2010
2.0%
4.0%
3.5%
12-17
1.5%
3.0%
18-25
2.5%
18-25
2.0%
26-34
1.0%
26-34
1.5%
The big increase in ever diagnosed with
diabetes appears to occur from adolescents/
emerging young adults into the young adult
age group.
0.5%
1.0%
0.0
0.5%
0.0
Have Diabetes
Pre-Diabetic
Have Diabetes
Male
Had Diabetes
When Pregnant
Pre- Diabetic
Male
Female
Source: Centers for Disease Control and Prevention (CDC). National Center for Health Statistics (NCHS). National Health and
Nutrition Examination Survey Data. 2009-2010
Female
Source: Centers for Disease Control and Prevention (CDC). Behavioral Risk Factor Surveillance System Survey Data 2010
Figure 8.2D
1.8%
1.6%
1.4%
1.2%
12-17
1.0%
18-25
0.8%
8%
26-34
0.6%
7%
0.4%
6%
0.2%
5%
18-25
4%
26-34
3%
0.0
2007
2008
2009
2010
Figure 8.2E
1.0%
0 Have Diabetes
0.9%
Pre-Diabetic
Male
Have Diabetes
Had Diabetes
When Pregnant
Pre- Diabetic
Female
Source: Centers for Disease Control and Prevention (CDC). Behavioral Risk Factor Surveillance System Survey Data 2010
In data from young adult members in
Kaiser Permanente Northern California
the percent of members with the diagnosis
of DM also increased with age (0.38% in
12–17 year olds, .67% in 18–25 year olds
and 1.55% in 26–34 year olds in 2010.)
There were no major changes in prevalence
in any age group between 2007 and 2010.
*DX equals 2 or more inpatient or outpatient diagnoses, one ER diagnoses, or on diabetic medications
Source: Northern California Kaiser Permanente, personal communication, 2011
2%
1%
Trends in Prevalence of Percent
of Members with DM* by Age
Group, Northern California Kaiser
Permanente, 2007-2010
0.8%
0.7%
12-17
0.6%
18-25
0.5%
26-34
0.4%
0.3%
0.2%
0.1%
0.0
0.0%
Male
Female
Lab Results Indicate Diabetic but
Undiagnosed by Gender and Age
Group, U.S., 2009-2010
Undiagnosed Diabetes: NHANES
provides an estimate of individuals who
have diabetes, but who have not been
diagnosed. In the emerging young
adult population, 0.14% of males and
0.18% of females meet the American
Diabetes Association criteria for a diabetes
diagnosis, but do not report being
diagnosed as diabetic.
Source: Centers for Disease Control and Prevention (CDC). National Center for Health Statistics (NCHS). National Health and
Nutrition Examination Survey Data. 2009-2010
48
Chronic Disease
49
8 Chronic Disease continued
Cancer
Figure 8.3A
Figure 8.3D
percentage of the u.s. population
< 65 years of age who are insured,
by age Plotted Against national
cancer mortality reduction,
1990-1998
improvement in 5-year relative
survival. all invasive cancer
excluding kaposi sarcoma
Between 1986-1995 and 1996-2005
the lowest improvement rates in cancer
survival were in older adolescents and
young adults aged 15 to 25.
There appears to be a relationship between
the percent insured and the average annual
reduction in cancer mortality and both
hit their lows in the emerging young
adult population ~18–24 suggesting an
insurance coverage gap in emerging young
adults.
Source: Siegel, S.E. (2010)
Source: Siegel, S.E. (2010)
Figure 8.3B
trends in improvement in average
annual percent change in cancer
mortality rates by age group, u.s.,
1975-2009
The trends in survival in Figure 8.3A
are confirmed in SEER data through
2009 showing the lowest average annual
improvement rates in survival for all
cancers in those aged 20 to 24.
Table 8.3A
2.5%
NIH and NCI Recommendations for Adolescents and Young Adults with Cancer (AYA)
The NIH and NCI has suggested a comprehensive approach to improving the approach, delivery of care and
treatment, awareness, prevention of adolescent and young adult (AYA) cancer patients.
2.0%
1.5%
1975-2009
2000-2009
1.0%
Identify Characteristics of Unique Cancer burden in AYA oncology patients
Improve awareness, prevention, access and quality care
Create tools to study AYA cancer
Ensure excellence in service delivery across cancer control continuum
Strengthen and promote, advocate, and support AYA Cancer Patient
0.5%
0.0
15-19
20-24
Source: Howlader N, Noone AM, Krapcho M et al.
25-29
30-34
35-39
Table 8.3B
Top Cancers in the U.S. and California, Incidence Rates (per 100,000) by Age Group and Gender, 2008
U.S.
California
Male12-17
Figure 8.3C
Rank Type of Cancer
National treatment trial accurals,
1990-1998 Plotted Against national
cancer mortality reduction,
1990-1998
Between 1990 and 1998, the lowest
reduction in cancer mortality and lowest
number of individuals enrolled in
National Cancer Trials was 20–24 year
olds suggesting a clinical trial enrollment
gap in emerging young adults.
18-25
Type of Cancer
26-34
Male12-17
Type of Cancer
Rank Type of Cancer
18-25
Type of Cancer
26-34
Type of Cancer
1
Lymphocytic Leukemia
2.5
Testis
8.6
Testis
13.1
1
Lymphocytic Leukemia
2.7
Testis
8.7
Testis
12.3
2
Brain
2.4
Hodgkin Lymphoma
4.0
Melanoma of the Skin
6.3
2
Brain
2.1
Hodgkin Lymphoma
3.6
Melanoma of the Skin
5.5
3
Hodgkin Lymphoma
2.1
Non-Hodgkin Lymphoma
2.8
Non-Hodgkin Lymphoma
5.0
3
Hodgkin Lymphoma
2.0
Non-Hodgkin Lymphoma
2.7
Non-Hodgkin Lymphoma
4.7
4
Non-Hodgkin Lymphoma
2.0
Melanoma of the Skin
2.4
Hodgkin Lymphoma
4.0
4
Bones and Joints
1.9
Melanoma of the Skin
2.1
Hodgkin Lymphoma
3.2
5
Bones and Joints
1.9
Brain
2.2
Colon and Rectum
3.3
5
Non-Hodgkin Lymphoma
1.8
Brain
2.1
Brain
3.0
female12-17
Rank Type of Cancer
Source: Siegel, S.E. (2010)
50
1.
2.
3.
4.
5.
18-25
Type of Cancer
26-34
female12-17
Type of Cancer
Rank Type of Cancer
18-25
Type of Cancer
26-34
Type of Cancer
1
Brain
2.0
Thyroid
7.4
Breast
18.8
1
Hodgkin Lymphoma
1.9
Thyroid
6.9
Breast
17.6
2
Hodgkin Lymphoma
1.9
Melanoma of the Skin
5.2
Thyroid
16.4
2
Brain
1.9
Melanoma of the Skin
4.0
Thyroid
14.0
3
Thyroid
1.8
Hodgkin Lymphoma
4.4
Melanoma of the Skin
11.2
3
Lymphocytic Leukemia
1.9
Hodgkin Lymphoma
3.9
Melanoma of the Skin
9.2
4
Lymphocytic Leukemia
1.6
Non-Hodgkin Lymphoma
1.9
Cervix Uteri
9.1
4
Thyroid
1.8
Ovary
1.8
Cervix Uteri
8.7
5
Bones and Joints
1.3
Brain
1.8
Hodgkin Lymphoma
4.1
5
Bones and Joints
1.3
Non-Hodgkin Lymphoma
1.8
Hodgkin Lymphoma
3.4
Source: SEER* Stat, 2008
Chronic Disease
51
8 Chronic Disease continued
Figure 8.4A
prevalence ever told have heart
disease or condition by age group
and gender, u.s. and western states,
2010
Heart Disease: Approximately 3.1% of
male emerging young adult and 3.2%
of female emerging young adults report
being told they have a heart condition
or disease. The prevalence is lower in the
western United States among emerging
young adults (2.0% of males and 2.5% of
females).
prevalence ever told had any kind
of heart disease by age group and
gender, california, 2009
California: 0.6% of emerging young adult
males and 1.1% of emerging young adult
females report ever being told they have
any kind of heart disease. The prevalence
was lower in young adult males and about
the same in young adult females.
high total cholesterol prevalence
by age group, u.s., 1999-2008
16%
4.0%
14%
3.5%
12%
3.0%
10%
2.0%
Male
6%
Female
4%
1.5%
2%
1.0%
0
0.5%
0.0
20 to 24
25 to 44
8%
2.5%
18-25
U.S.
26-34
18-25
West
1999-2000 2001-2002 2003-2004 2005-2006 2007-2008
Figure 8.4D
30%
high total cholesterol prevalence
by age group, california, 2001-2007
25%
4.0%
3.5%
20%
3.0%
15%
2.5%
Male
2.0%
Female
20 to 24
25 to 44
10%
1.5%
5%
1.0%
0
2001
0.5%
0.0
High Total Cholesterol: In both the U.S.
and in California the prevalence rates of
high total cholesterol are higher in 25–44
year olds compared to the 20–24 year olds.
In 2005, rates in 20–24 year olds were
5.9% nationally and 12.2% in California.
Respective rates in 25–44 year olds were
16.8% and 25.9% (Figures 8.4C, 8.4D).
Source: Division for Heart Disease and Stroke Prevention: Data Trends & Maps Web site
26-34
Source: National Health Interview Survey 2010. Sample Adult File.
Figure 8.4B
Figure 8.4C
18%
Cardiovascular
2003
2005
2007
Source: Division for Heart Disease and Stroke Prevention: Data Trends & Maps Web site
18 to 25
Source: 2009 California Health Interview Survey
26 to 34
Figure 8.4E
16%
prevalence of hypertension by
age group, u.s., 2007-2008 and
california, 2009
14%
12%
10%
18-24
8%
25-44
6%
4%
Hypertension: Prevalence rates were
higher in emerging young adults aged
18–24 in California (6.3%) than in the
U.S. (2.8%). Respective rates in 25–44
year olds were 14.4% and 13.3%.
2%
0
U.S.
California
Source: Division for Heart Disease and Stroke Prevention: Data Trends & Maps Web site
52
Chronic Disease
53
8 Chronic Disease continued
Disability
Figure 8.5A
prevalence ever diagnosed with
seizure disorder or epilepsy by age
and gender, u.s., 2010 and california,
2005
NHIS estimates that 1.8% of emerging
young adult males and 0.9% of emerging
young adult females have been diagnosed
with epilepsy. In California, CHIS estimates
that in emerging young adults, 0.9% of
males and 1.4% of females have been
diagnosed with epilepsy.
Based on self-report, but in two different
surveys and in two different years, epilepsy
prevalence rates in emerging young adults
were higher in males nationally and
lower in adolescent females than those in
California. In young adults aged 26–34
in these two different surveys, prevalence
rates were higher nationally 1.8% in both
sexes compared to 1.4% in both sexes in
California.
Figure 8.7A
14%
Epilepsy
disability due to physical, mental or
emotional condition by age group,
u.s. and california, 2010
12%
2.0%
10%
1.8%
1.6%
8%
**
1.4%
18-24
6%
1.2%
Male
1.0%
**
0.8%
Female
25-34
4%
2%
0.6%
0.4%
0
U.S.
0.2%
0.0
18-25
U.S.
26-34
California
Source: Centers for Disease Control and Prevention (CDC). Behavioral Risk Factor Surveillance System Survey Data 2010
18-25
26-34
California
**Data is statistically unstable
Source: National Health Interview Survey 2010. Sample Adult File [U.S. data] and 2005 California Health Interview Survey
[CA data]
Figure 8.7B
2.5%
percent with diagnosis of autism*
by age group and gender, northern
california kaiser permanente, 2010
2.0%
1.5%
Male
Female
1.0%
0.5%
0.0
prevalence of being told have weak
or failing kidneys by age group and
gender, u.s. and western states, 2009
Renal disease rates are higher among young
adults aged 26–34 than emerging young
adults for both genders.
NHIS estimates approximately 0.5% of
emerging young adult males and 0.7%
of females nationally have been told the
individual has weak or failing kidneys
(Figure 8.6). In emerging young adults in
the NHIS study, rates are higher in females
both nationally and in western states.
54
12-17
18-25
In Northern California among a large
HMO setting, the diagnosis of autism
decreased in both males and females with
increasing age. In emerging young adult
males, the diagnosis of autism increased
from 0.7 percent in 2006 to 1.2% in 2010
(Figures 8.7B, 8.7C).
26-34
*Includes Autistic Disorder, Autistic Spectrum Disorders, Aspergers, PDD/PDD-NOS
Source: Northern California Kaiser Permanente, personal communication, 2011
Renal Disease
Figure 8.6A
In the U.S. and California, disability status
due to a physical, mental or emotional
condition increased with age and was
higher in the U.S. For emerging young
adults this was 10.3% versus 8.9% in
California.
1.2%
1.4%
1.0%
1.2%
0.8%
1.0%
Male
0.6%
Female
0.4%
Figure 8.7C
0.8%
Male
0.6%
trends in percent with diagnosis
of autism* among emerging
young adults (aged 18 to 25) by
gender, northern california kaiser
permanente, 2006-2010
Female
0.4%
0.2%
0.0
0.2%
18-25
U.S.
26-34
18-25
Source: National Health Interview Survey 2010. Sample Adult File
West
26-34
0.0
2006
2007
2008
2009
2010
*Includes Autistic Disorder, Autistic Spectrum Disorders, Aspergers, PDD/PDD-NOS
Source: Northern California Kaiser Permanente, personal communication, 2011
Chronic Disease
55
8 Chronic Disease continued
Figure 8.8A
prevalence of overweight or obese,
by gender and age group, u.s., 20092010
Prevalence rates: Nationally, the prevalence
of overweight and obesity increases with
age. Obese and overweight prevalence rates
in emerging young adults hit nearly 50% in
males and females and reach over 70% in
young adult males aged 26–34.
Figure 8.8C
35%
Obesity
Female
20 to 34
Female
12 to 19
30%
80%
25%
70%
Obese
(BMI > 30)
60%
50%
Overweight
(BMI 25-30)
40%
30%
Male
20 to 34
Male
12 to 19
15%
10%
5%
20%
0
10%
0
20%
12-17
18-25
Male
26-34
12-17
18-25
Female
trends in obesity prevalence
by gender and age group, u.s.,
1971-2008
Trends: Obesity prevalence rates have
skyrocketed from 9.7% in females aged
20–34 in 1971–74 to 31.4% in 20052008; the numbers in males of the same
age have increased from 8.9% to 25.4%
over the same time period.
1971-1974 1976-1980 1988-1994 1999-2002 2005-2008
Source: National Center for Health Statistics. Health, United States, 2010
26-34
Source: Centers for Disease Control and Prevention (CDC). National Center for Health Statistics (NCHS). National Health and
Nutrition Examination Survey Data. 2009-2010
Figure 8.8B
prevalence of being overweight or
obese by age group and gender,
california, 2010
California: Obesity rates increase with
age in California as well, with similar
prevalence rates to the national estimates.
80%
70%
60%
50%
40%
Obese
(BMI > 30)
30%
Overweight
(BMI 25-30)
20%
10%
0
12-17
Male
18-25
12-17
Female
18-25
Source: Centers for Disease Control and Prevention (CDC). Behavioral Risk Factor Surveillance System Survey Data 2010
56
Chronic Disease
57
9 Health Promotion and Prevention
Take Home Message:
3.0
Diet and Exercise
2.5
Emerging young adults eat less fruits and vegetables and more fast food than young adults. However, emerging
young adult males exercise more and spend fewer hours in sedentary activities than males aged 26–34.
2.0
Immuninzations
1.5
Overall compliance with HPV, influenza, and pertussis vaccinations is low in emerging young adults and young
adults.
Screening
Pap smear compliance increases with age. Screening for HIV increases with age and is consistently higher among
females than males.
Sleep
The percent of individuals that don’t get enough sleep 15+ days a month increases with age and is higher in
females.
Seatbelts
In California and the nation, emerging young adult males are least likely to always or almost always wear a
seatbelt, both nationally and in California, and correspondingly have the highest fatal MVA-occupant injury rates
(Figure 3.1D).
Figure 9.1B
18-25
26-34
1.0
0.5
0.0 Male Female Male Female Male Female Male Female Male Female
Hispanic
White
Black
Asian
Total
Preventive health guidelines for emerging young adults are not consistent among medical and health
organizations and are often overlooked.
Figure 9.1C
3.0
2.5
12-17
18-25
1.5
26-34
1.0
Diet and Exercise
Figure 9.1A
number of foods eaten per month
by type of food and age group,
u.s., 2010
Diet: Compared to young adults
nationally, emerging young adults
consume fewer fruits, salads, and
vegetables but eat more potatoes and
tomato sauce and drink more fruit juice
monthly than young adults.
average number of fast food meals
eaten in the past week by gender
and age group, california, 2009
Fast food: The average number of fast
food meals eaten in the past week peaks in
emerging young adults. Males consistently
consume more fast food than females
regardless of age.
0.5
30
0.0
25
Male
Female
Total
Source: California Health Interview Survey. CHIS 2009 Adult Survey and CHIS 2009 Teen Survey
20
18-25
15
26-34
10
Figure 9.2A
70%
60%
50%
5
0
Male
40%
Fruit
Juice
Fruit
Salad
Potato
Other
Salsa
Vegetables
Source: National Health Interview Survey 2010. Sample Adult File.
Tomato
Sauce
Female
30%
20%
10%
0
18-25
U.S.
26-34
18-25
26-34
California
Source: Behavioral Risk Factor Surveillance System Survey Data, 2009
58
California: In California, emerging young
adults consume fewer fruits and vegetables
daily than young adults regardless of race
or gender. The widest gap occurs between
emerging young adult Asian females, who
consumed an average of 1.1 cups per day,
and young adult Asian females, who ate
2.1 cups daily.
Source: California Health Interview Survey. CHIS 2009 Adult Survey
2.0
Preventative Health Care Guidelines
average daily cups of fruits/
vegetables excluding french fries
and beans by gender, race, and age
group, california, 2009
percent of individuals that meet
recommended physical activity
guidelines by age group and
gender, u.s. and california, 2009
Exercise guidelines: The Centers
for Disease Control and Prevention
recommend at least 75 minutes of
vigorous or 150 minutes of moderate
exercise per week for adults (Physical
Activity, 2011). Emerging young adult
males were the most compliant with these
guidelines (64% and 65% in the U.S. and
California, respectively).
Health Promotion and Prevention
59
9 Health Promotion and Prevention
Figure 9.2B
average number of hours of
sedentary activity in a typical day
by age group and gender, u.s., 2010
Sedentary activity: Sedentary activity is
highest in the adolescent age group with
males reporting an average of 7.4 hours
per day of sedentary activity and females
reporting 8.0 hours. Emerging young
adults report the fewest hours of sedentary
activity with 5.4 hours for males and 5.7
for females.
9
80%
8
70%
7
60%
6
Male
5
Female
4
One Shot
50%
Two Shots
40%
All Three
30%
3
20%
2
10%
1
0
Figure 9.3B
0
12-17
18-25
26-34
Source: National Health and Nutrition Examination Survey (NHANES) Data, 2009-2010
Male
18-25
Female
Male
26-34
Source: Behavioral Risk Factor Surveillance System Survey Data, 2010
Figure 9.3C
individuals receiving the flu shot
or spray in the past year, u.s. and
california, 2010
30%
25%
20%
U.S.
15%
California
10%
5%
0
18-25
Influenza: In the U.S., 25% of emerging
young adults received the flu shot or spray
in the past year compared to 31% of young
adults. Fewer Californians were vaccinated
with just 21% in both emerging young
adults and young adults.
26-34
Source: Behavioral Risk Factor Surveillance System Survey Data, 2010
Immunizations
50%
80%
percent of respondents that have
ever had the hpv vaccine by age
group and gender, u.s., 2010
45%
70%
HPV vaccine: 44.2% of emerging young
adult females and 4.4% of emerging young
adult males received the HPV vaccine
compared to 7.5% of young adult females
and 2.3% of young adult males (Figure
9.3a). However, many of the young adults
were beyond the approved range for the
vaccine during this survey.
30%
40%
25%
Male
50%
Female
40%
20%
30%
15%
20%
10%
10%
5%
0
Figure 9.3D
60%
35%
0
18-25
Source: Behavioral Risk Factor Surveillance System Survey Data, 2010
60
Gender: Among those who received at
least one HPV shot, females were much
more likely than males to have received all
three shots.
Female
35%
Figure 9.3A
number of hpv shots received
among individuals that reported
ever having the hpv vaccine by
gender and age group, u.s., 2010
26-34
No
Yes
Unsure
18-25
U.S.
26-34
percent of individuals reporting
receiving the pertussis vaccination
in the past 5 years by age group,
u.s. and california, 2010
Pertussis: A similarly low percentage of
emerging young adults and young adults
receive the pertussis vaccine. In the U.S.
and California immunization rates range
from 12% to 16%.
18-25
26-34
California
Source: Behavioral Risk Factor Surveillance System Survey Data, 2010
Health Promotion and Prevention
61
9 Health Promotion and Prevention
Sleep
Figure 9.4A
Figure 9.5A
40%
Screening
35%
100%
30%
percent of women that have had a
pap test in the past 3 years by age
group, u.s. and california, 2010
90%
25%
0 Days
20%
1-7 Days
Pap Smear: The percent of women who
received a Pap test in the past three years
increases with age and is consistently
higher in the U.S. compared to California.
The highest percent is in young adult
women in the U.S. at 89%.
60%
80%
70%
U.S.
50%
California
40%
30%
10%
0
15+ Days
10%
5%
0
20%
8-14 Days
15%
Male
18-25
Female
Male
26-34
percent reporting the number of days
in the past 30 days you did not get
enough sleep or rest by gender and
age group, u.s., 2010
Sleep: The percent of individuals not
getting enough sleep on 15+ days per
month is higher in young adults compared
to emerging young adults and higher in
females in both age groups.
Female
Source: Behavioral Risk Factor Surveillance System Survey Data, 2009
18 to 21
22 to 25
26 to 34
Source: Behavioral Risk Factor Surveillance System Survey Data, 2010
Figure 9.4B
percent of individuals ever having an
hiv test by age group and gender,
u.s., 2006-2010
HIV: The percent of individuals ever
having an HIV test increases with age and
is consistently higher among females than
males.
90%
80%
70%
60%
Male
50%
Female
40%
30%
20%
10%
0
15 to 17
18 to 25
Source: National Survey of Family Growth 2006-2010
Seatbelts
26 to 34
Figure 9.6A
100%
95%
90%
18-25
26-34
85%
80%
75%
Male
U.S.
Female
percent of individuals that always
or almost always wear a seatbelt
by gender and age group, u.s. and
california, 2010
Seatbelts: Emerging young adult males
have the lowest percents of always or
almost always wearing a seat belt in both
in the U.S. and California (85% and 86%,
respectively).
Male
Female
California
Source: Behavioral Risk Factor Surveillance System Survey Data, 2010
62
Health Promotion and Prevention
63
9 Health Promotion and Prevention
Preventative Health Care Guidelines
Figure 9.7A
Consistency of Preventive Health Care Recommendations for Young Adults
Preventive Health Guidelines: Preventive health care recommendations for young adults are outlined in Table
9.7A. These guidelines come from a range of sources and address everything from immunizations to suicide
screening. Preventive health care guidelines for emerging young adults area not consistent among medical and health
Table 2. Consistency of Preventive Health Care Recommendations for Young Adults
organizations.
USPSTF8
Young Adult,
Aged 18-26 y
Bright
Futures 14
Adolescent,
Aged 11-21 y
Adolescent,
Aged 11-17 y
Substance use
Alcohol (screening and counseling)
Tobacco (screening and counseling)
Other illicit drugs (screening and counseling)
Reproductive health
STI screening and counseling
HIV
Chlamydia (female)
Chlamydia (male)
Syphilis
Gonorrhea
Birth control methods
Pregnancy
Mental health/depression
Suicide screening
Depression
Nutrition/exercise/obesity
Cholesterol level
Healthy diet
Hypertension/blood pressure
Obesity/BMI
Physical activity counseling
Infectious disease/immunization (CDC)
Td/Tdap
Human papillomavirus
Varicella
Measles, mumps, rubella
Influenza
Pneumococcal (polysaccharide)
Hepatitis A
Hepatitis B
Meningococcal
Polio
Safety/violence
Family/partner violence
Fighting
Helmets
Seat belts
Alcohol while driving
Guns
Bullying
ACOG23,24
Young Adult,
Aged 18-26 y
AAFP25
Young Adult,
Aged 18-26 y
ACP26
Young Adult,
Aged 18-26 y
Abbreviations: AAFP, American Academy of Family Physicians; ACOG, American Congress of Obstetricians and Gynecologists; ACP, American College of
Physicians; BMI, body mass index; CDC, Centers for Disease Control and Prevention; HIV, human immunodeficiency virus; STI, sexually transmitted infection;
Td/Tdap, tetanus, diphtheria/tetanus, diphtheria, pertussis; USPSTF, US Preventive Services Task Force.
a “” Indicates a recommendation; “”, if at risk.
Source: From “Young Adult Preventative Health Care Guidelines,” by EM Ozer, JT Urquhart, CD Brindis, et al, 2012, Archives of Pediatric and Adolescent Medicine, 166, p.245. Copyright 2012 by
American Medical Association. Reprinted with permission.
64 tive services that they recommend. The guidelines of the
COMMENT
Health Promotion and Prevention
65
10 Services
Take Home Message:
35%
Accessibility
30%
Emerging young adults have the highest uninsured rates in both the U.S. and California with males more likely
to be uninsured than females. Although the Affordable Health Care Act has helped this situation, the recent GallupHealthway poll estimated a small decline of uninsured emerging young adults from 28% uninsured 18 to 25 year
olds in fall 2010 to 24.2% in the second quarter of 2011 (Mendes E, 2012). Delaying or not getting necessary
medical care increases with age in the U.S. and California.
Utilization
Cost
Emerging young adults had the highest prevalence of $0 spending per person per year (26%). Regardless of age
group, uninsured individuals are more likely to spend $0 on annual health care expenditures. Emerging young
adult males have the lowest annual health care expenditures; young adult females have the highest. Private insurance
encompasses the greatest percentage of annual health care expenditures regardless of age group or gender. Annual
prescription medication costs increase with age among females and are lowest in emerging young adult males.
Uninsured rates: Emerging young adults
have the highest uninsured rates in both
the U.S. and California, with males
more likely to be uninsured than females
(Figures 10.1A, 10.1B).
25%
12-17
20%
18-25
26-34
15%
5%
0
Total
Male
Female
Source: 2009 California Health Interview Survey
Figure 10.1C
35%
30%
27.6
26.7 26.9 27.5 27.2
28.5 28.7 28.5 28.4
27.7 28.0
26.3
24.0 24.2
25%
20%
15%
Accessibility
Percent of Uninsured Individuals by
Gender and Age Group, U.S., 2009
Percent of Uninsured Individuals
by Gender and Age Group,
California, 2009
10%
Emerging young adults have the lowest number of outpatient healthcare visits per person per year and the highest
number of emergency room visits. Young adults aged 18–24 are most likely to report no health care visits in the past
12 months. Among emerging young adults, the most common outpatient and inpatient claims for emerging young
adults involve gynecology and obstetrics and the most common ER claim deals with musculoskeletal and connective
tissue disorders. The number of prescription medications per year increases with age for females and is lowest among
emerging young adult males in the U.S. Contraceptives are the top drug class used by emerging young adults.
Figure 10.1A
Figure 10.1B
15.0 15.7 15.4
16.6
18.8 18.4
17.8 18.0 17.9 18.0 18.0 18.3 18.1
25.4
24.2 24.5
19.9 19.6 20.1 19.7
10%
35%
5%
30%
0
Jan-08
25%
Jan-09
Jan-10
Jan-11
Trends in Uninsured Rates by Age
Group, U.S., 2008-2012
18-25
26-34
Although the Affordable Health Care Act
has helped this situation, the recent GallupHealthway poll estimated a small decline
of uninsured emerging young adults from
28% uninsured 18 to 25 year olds in fall
2010 to 24.2% in the second quarter of
2011.
Jan-12
Source: Mendes E, 2012
12-17
20%
18-25
26-34
15%
10%
5%
0
Total
Male
Female
Source: Medical Expenditure Panel Survey 2009
66
Services
67
10 Services
Table 10.1A
Type of Insurance Coverage by Gender and Age Group, U.S., 2009
7%
Insurance coverage: Nationally, uninsured rates peak in emerging young adults with a corresponding decline in
private insurance coverage.
6%
Type of Coverage
Age Groups
Figure 10.1D
8%
Male
Female
5%
12-27
4%
12 to 17
18 to 25
26 to 34
12 to 17
18 to 25
26 to 34
Uninsured
9.0%
30.3%
30.0%
9.2%
21.6%
16.8%
3%
Private
63.5%
58.6%
63.8%
61.9%
57.4%
69.3%
2%
Medicaid/SCHIP
29.9%
10.5%
6.2%
32.3%
22.0%
14.8%
Medicare
0.2%
0.4%
0.9%
0.6%
0.3%
0.8%
Other Public
0.5%
0.9%
0.1%
0.5%
1.0%
0.5%
Tricare
2.3%
1.6%
0.7%
2.1%
3.1%
1.6%
18-25
26-34
1%
0
Male
Percent of Individuals Reporting
Delayed or Unable to Get Necessary
Medical Care by Gender and Age
Group, U.S., 2009
Delay of care: Nationally, the percentage
of individuals reporting “delayed or unable
to get necessary medical care” increases
with age and is higher in females than
males except among adolescents.
Female
Source: Medical Expenditure Panel Survey 2009
Source: Medical Expenditure Panel Survey 2009
Figure 10.1E
4.0%
Table 10.1B
3.5%
Type of Insurance Coverage by Gender and Age Group, California, 2009
3.0%
Insurance coverage: Similarly, in California, emerging young adults have the highest uninsured rate with a
corresponding decline in employment based coverage. The highest rates of privately purchased coverage are in
emerging young adults at 14.3% and 9.1% among males and females, respectively.
2.5%
12-17
2.0%
18-25
1.5%
26-34
Type of Coverage
Age Groups
Male
Female
1.0%
12 to 17
18 to 25
26 to 34
12 to 17
18 to 25
26 to 34
Uninsured
5.7
31.6
30.1
6.9
22.4
19.3
0.5%
Employment-based
58.5
35.8
50.9
55.4
41.6
53.9
0.0
Privately purchased
4.3
14.3
5.7
4.6
9.1
5.6
Medicaid
22.5
13.2
10
22.9
20.3
16.9
Healthy Families / CHIP
6.7
0.9*
-
8.3
0.8*
-
Other public
2.3
4.2
3.4
1.9
5.9
4.3
Male
Percent of Individuals Reporting
Delayed or Unable to Get Necessary
Prescription Medications by Gender
and Age Group, U.S., 2009
Delay of care: The percentage of
individuals reporting “delayed or unable
to get necessary prescription medications”
is highest in emerging young adult females
at 3.8%.
Female
Source: Medical Expenditure Panel Survey 2009
* Indicates statistically unstable data.
Source: 2009 California Health Interview Survey
68
Services
69
10 Services
Figure 10.1F
Utilization of Services
20%
4.0
Delayed or Did Not Get Other
Medical Care Needed in the Past
12 Months by Age Group and Gender,
California, 2009
18%
3.5
California: In California, the percentage
of individuals that “delayed or did not get
needed medical care” increases with age
and is higher in females than in males.
10%
16%
3.0
14%
12-17
18-25
8%
26-34
6%
For prescription medications, the delay
was greatest in young adults.
Male
26-34
1.5
0.0
Female
Outpatient Visits
0.02 0.07 0.08
Inpatient Visits
Mean Number of Healthcare Visits
per Person per Year by Type of Visit
and Age Group, U.S., 2009
Healthcare visits: Emerging young
adults have the lowest mean number of
outpatient visits, but the highest number
of ER visits. Inpatient visits increase with
age.
0.14 0.22 0.16
ER Visits
Source: Medical Expenditure Panel Survey 2009
30%
12%
25%
10%
Figure 10.2B
Percent of Individuals Reporting no
Health Care Visits in Past 12 Months
by Age Group, U.S., 2009
20%
8%
12-17
6%
18-25
26-34
4%
Nearly a quarter of emerging young adults
aged 18–24 reported no health care visits
in the past 12 months compared to 12%
of those aged 6–17 and 22% of those aged
25–44.
15%
10%
5%
2%
Male
Source: 2009 California Health Interview Survey
70
18-25
14%
0
12-17
2.0
0.5
Source: 2009 California Health Interview Survey
Delayed or Did Not Get a Prescription
Medication in the Past 12 Months by
Age Group and Gender,
California, 2009
2.75
1.0
4%
2%
Figure 10.1G
3.03
2.5
12%
0
Figure 10.2A
3.58
Female
0
6-17
18-24
25-44
Source: National Center for Health Statistics. Health, United States, 2010
Services
71
10 Services
Table 10.2A
Table 10.2B
Top Ten Diagnostic Categories Based on a Percent of a Major U.S. Health Plan’s Members with
at Least One Outpatient Claim for Diagnostic Group by Category and Age Group, U.S., 2010-2011
Top Ten Diagnostic Categories Based on a Percent of a Major U.S. Health Plan’s Members with at
Least One Emergency Room Claim for Diagnostic Group by Category and Age Group, U.S., 2010-2011
Diagnostic categories: For outpatient visits the most common diagnostic categories are musculoskeletal and
connective tissue disorders in adolescents and gynecology and obstetrics for emerging young adults and young
adults.
For emergency room claims the most common diagnostic category is musculoskeletal and connective tissue
disorders in all age groups.
Ages 12 to 17
Ages 18 to 25
Ages 12 to 17
Ages 18 to 25
Ages 26 to 34
Musculoskeletal and
Connective Tissue Disorders
45.2%
Gynecology and Obstetrics
40.5%
Gynecology and Obstetrics
76.4%
Musculoskeletal and
Connective Tissue Disorders
7.44%
Musculoskeletal and
Connective Tissue Disorders
4.91%
Musculoskeletal and
Connective Tissue Disorders
4.88%
Ear, Nose, and Throat
Disorders
43.8%
Ear, Nose, and Throat
Disorders
25.0%
Musculoskeletal and
Connective Tissue Disorders
41.7%
Injuries
4.76%
Gastrointestinal Disorders
3.77%
Gastrointestinal Disorders
3.94%
Dermatologic Disorders
28.0%
Musculoskeletal and
Connective Tissue Disorders
21.2%
Ear, Nose, and Throat
Disorders
29.2%
Gastrointestinal Disorders
2.57%
Injuries
3.18%
Gynecology and Obstetrics
2.72%
Neurologic Disorders
1.70%
Gynecology and Obstetrics
2.11%
Injuries
2.43%
Pulmonary Disorders
19.7%
Dermatologic Disorders
18.9%
Dermatologic Disorders
21.2%
1.35%
Pulmonary Disorders
1.79%
Cardiovascular Disorders
2.39%
Psychiatric Disorders
18.9%
Pulmonary Disorders
17.0%
Genitourinary Disorders
17.8%
Ear, Nose, and Throat
Disorders
Immunizations
15.8%
Psychiatric Disorders
13.4%
Pulmonary Disorders
16.5%
Pulmonary Disorders
1.33%
Cardiovascular Disorders
1.76%
Pulmonary Disorders
2.01%
Eye Disorders
14.0%
Genitourinary Disorders
12.5%
Psychiatric Disorders
16.2%
Cardiovascular Disorders
1.23%
Neurologic Disorders
1.63%
Neurologic Disorders
1.80%
Gastrointestinal Disorders
8.9%
Gastrointestinal Disorders
10.9%
Gastrointestinal Disorders
15.5%
Psychiatric Disorders
0.91%
Ear, Nose, and Throat
Disorders
1.59%
Genitourinary Disorders
1.48%
Infectious Diseases
8.8%
Eye Disorders
10.3%
Cardiovascular Disorders
13.6%
Infectious Diseases
0.88%
Genitourinary Disorders
1.46%
7.5%
Immunizations
6.0%
Endocrine and Metabolic
Disorders
12.9%
Ear, Nose, and Throat
Disorders
1.39%
Genitourinary
Genitourinary Disorders
0.66%
Infectious Diseases
1.03%
Infectious Diseases
0.95%
Source: A Major U.S. Health Plan, personal communication, 2012.
72
Ages 26 to 34
Source: A Major U.S. Health Plan, personal communication, 2012.
Services
73
10 Services
Table 10.2C
Figure 10.2C
7
Top Ten Diagnostic Categories Based on a Percent of a Major U.S. Health Plan’s Members with
at Least One Inpatient Claim for Diagnostic Group by Category and Age Group, U.S, 2010-2011
For inpatient claims the most common diagnostic category is psychiatric disorders among adolescents and
gynecology and obstetrics in emerging young adults and young adults.
Ages 12 to 17
Ages 18 to 25
Average Number of Prescription
Medications (Including Refills) Per
Person Per Year by Age Group and
Gender, U.S. and Western States,
2009
6
5
4
Male
Female
3
Ages 26 to 34
Psychiatric Disorders
1.01%
Gynecology and Obstetrics
4.16%
Gynecology and Obstetrics
12.80%
Gastrointestinal Disorders
0.69%
Gastrointestinal Disorders
0.87%
Gastrointestinal Disorders
1.40%
Musculoskeletal and
Connective Tissue Disorders
0.47%
Psychiatric Disorders
0.63%
Cardiovascular Disorders
0.82%
Neurologic Disorders
0.36%
Pulmonary Disorders
0.48%
Neurologic Disorders
0.66%
Pulmonary Disorders
0.35%
Cardiovascular Disorders
0.46%
Pulmonary Disorders
0.63%
Gynecology and Obstetrics
0.30%
Musculoskeletal and
Connective Tissue Disorders
0.38%
Musculoskeletal and
Connective Tissue Disorders
0.57%
Cardiovascular Disorders
0.26%
Neurologic Disorders
0.36%
Genitourinary Disorders
0.50%
Injuries
0.19%
Drug Use and Dependence
0.35%
Psychiatric Disorders
0.35%
Infectious Diseases
0.17%
Infectious Diseases
0.24%
Infectious Diseases
0.33%
Endocrine and Metabolic
Disorders
0.16%
Genitourinary Disorders
0.21%
Endocrine and Metabolic
Disorders
0.31%
Prescription medications: Except
among adolescents, females report a
higher average number of prescription
medications per year nationally.
2
1
0
12-17
18-25
U.S.
26-34
12-17
18-25
West
26-34
Source: Medical Expenditure Panel Survey 2009
Source: A Major U.S. Health Plan, personal communication, 2012.
Table 10.2D
Top 10 Drug Classes by Age Group and Percent of Rx, U.S, 2007-2008
Among emerging young adults, contraceptives are the most frequently prescribed drug (18.4%) followed by
analgesics and psychotherapeutics.
Ages 12 to 17
%
Ages 18 to 25
%
Ages 26 to 34
%
Asthma
23.6
Contraceptives
18.4
Analgesics
12.6
CNS Stimulants
11.8
Analgesics
11.0
Contraceptives
9.8
Respiratory Agents
11.5
Psychotherapeutic
10.8
Cardiovascular Agents
9.8
Psychotherapeutic
9.9
Anti-infective
10.4
Anti-infective
9.3
Anti-infectives
9.7
Asthma
8.3
Psychotherapeutic
7.8
Analgesics
6.3
Anticonvulsants
6.1
Gastrointestinal Agents
7.0
Dermatological Agents
5.0
Respiratory Agents
5.2
Hormones
5.6
Anticonvulsants
4.5
Gastrointestinal Agents
4.9
Asthma
5.4
Hormones
3.7
Hormones
4.6
Antidiabetic Agents
5.4
Contraceptives
2.9
Antidiabetic Agents
4.3
Respiratory Agents
5.2
Source: NHANES 2007-2008
74
Services
75
10 Services
Figure 10.3A
Total Annual Health Care
Expenditures per Person by Age
Group, U.S., 2009
Healthcare spending: Emerging young
adults had the highest prevalence of $0
spending per person per year (26%).
Figure 10.3C
$3,500
Cost of Services
$3,000
80%
$2,500
70%
60%
50%
40%
30%
$2,000
Any
Insurance
$1,500
Out of
Pocket
12-17
$1,000
18-25
26-34
$500
0
20%
12-17
10%
0
$0
$1-$4,999
80%
Uninsured status: Uninsured individuals
in all age groups had a higher prevalence
of spending $0 on health care.
50%
40%
18-25
Female
26-34
Figure 10.3D
60%
50%
40%
Out of
Pocket
30%
Private
Insurance
12-17
20%
18-25
26-34
Public
Insurance
10%
70%
60%
30%
0
20%
12-17
10%
0
12-17
$5,000+
90%
Total Annual Health Care
Expenditures per Person by Insurance
Status and Age Group, U.S., 2009
26-34
Annual health care expenditures: Annual
health care expenditures per person are
lowest among emerging young adult males
at $1,216. Among females, annual health
care expenditures increase with age and
peak at $3,167.
Source: Medical Expenditure Panel Survey 2009
Source: Medical Expenditure Panel Survey 2009
Figure 10.3B
18-25
Male
Annual Health Care Expenditures
per Person by Age Group, Gender,
and Source of Payment, U.S., 2009
Insured Uninsured Insured Uninsured Insured Uninsured
$0
$1-$4,999
$5,000+
Source: Medical Expenditure Panel Survey 2009
18-25
Male
26-34
12-17
18-25
Female
Percent of Annual Health Care
Expenditures Covered by Age Group,
Gender, and Source of Payment,
U.S., 2009
Type of insurance: Private insurance
encompasses the greatest percentage of
annual health care expenditures regardless
of age group or gender.
26-34
Source: Medical Expenditure Panel Survey 2009
Figure 10.3E
$500
$450
Total Average Annual Rx Costs by
Age Group and Gender, U.S. and
Western States, 2009
$400
$350
$300
Male
Female
$250
$200
$150
$100
Prescription medications: In both
the U.S. and western states, annual
prescription medication costs are lowest
in emerging young adult males. Costs
increase with age among females.
$50
0
12-17
18-25
U.S.
26-34
12-17
18-25
West
26-34
Source: Medical Expenditure Panel Survey 2009
76
Services
77
11 References
Executive Summary
Marantz Henig, Robin. Why are so many people in their 20s taking so long to grow up. New York Times. August 18, 2010.
Mendes E: In U.S., Uninsured Rate for 18- to 25-Year-Olds Plateaus, Gallop Poll, April 3, 2012 (http://www.gallup.com/poll/153737/uninsured-rate-year-olds-plateaus.aspx)
Giedd Jay N: The Teen Brain: Insights from Neuroimaging, Review Article. JAH 42: 335-343, 2008
Johnson SB, Blum RW, Giedd JN: Adolescent Maturity and the Brain: The Promise and Pitfalls of Neuroscience Research in Adolescent Health Policy. JAH 45:216-21, 2009.
Chapter 1:
Population Projections, United States, 2004 - 2030, by state, age and sex, on CDC WONDER On-line Database, September 2005. Accessed at http://wonder.cdc.gov/population-projections.html
US Census Bureau. (2009). State Single Year of Age and Sex Population Estimates: April 1, 2000-July 1, 2009-RESIDENT. [Data file]. Available from http://www.census.gov/popest/data/index.html.
US Census Bureau, American Fact Finder. (2010). 2010 Census Summary File 1. [Data file]. Available from http://factfinder2.census.gov/faces/nav/jsf/pages/wc_dec.xhtml.
Chapter 2:
National Center for Health Statistics. Health, United States, 2010: With Special Feature on Death and Dying. Hyattsville, Maryland. 2011.
Centers for Disease Control and Prevention, National Center for Health Statistics. Underlying Cause of Death 1999-2008 on CDC WONDER Online Database, released 2011. Data for year 2008
are compiled from the Multiple Cause of Death File 2008, Series 20 No. 2N, 2011, data for year 2007 are compiled from Multiple Cause of Death File 2007, Series 20 No. 2M, 2010, data for years
2005-2006 data are compiled from Multiple Cause of Death File 2005-2006, Series 20, No. 2L, 2009, and data for years 1999-2004 are compiled from the Multiple Cause of Death File 1999-2004,
Series 20, No. 2J, 2007. Accessed at http://wonder.cdc.gov/ucd-icd10.html on Mar 26, 2012 4:42:14 PM
Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS) [online]. (2005) [cited 2012
March 19]. Available from URL: www.cdc.gov/ncipc/wisqars.
Chapter 3:
Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS) [online]. (2010). [cited Year
Month (abbreviated) Day]. Available from URL: www.cdc.gov/ncipc/wisqars
Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS) [online]. (2009). [cited Year
Month (abbreviated) Day]. Available from URL: www.cdc.gov/ncipc/wisqars
Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS) [online]. (2005). {cited Year
Month (abbreviated) Day}. Available at: www.cdc.gov/injury/wisqars.
Chapter 4:
California Health Interview Survey. CHIS 2009 Adult Public Use File. Release 1 [computer file]. Los Angeles, CA: UCLA Center for Health Policy Research.
Centers for Disease Control and Prevention. Current Depression Among Adults---United States, 2006 and 2008. MMWR 2010;59:1229-1235.
Centers for Disease Control and Prevention. Suicidal Thoughts and Behaviors Among Adults Aged ≥18 Years — United States, 2008–2009. MMWR 2011;60(SS13): 1-28.
NCHA: American College Health Association. American College Health Association-National College Health Assessment II: Reference Group Data Report Fall 2009. Baltimore: American Health
Association; 2010
United States Department of Health and Human Services. Substance Abuse and Mental Health Services Administration. Center for Behavioral Health Statistics and Quality. National Survey on Drug
Use and Health, 2010 [Computer file]. ICPSR32722-v1. Ann Arbor, MI: Inter-university Consortium for Political and Social Research [distributor], 2011-12-05. doi:10.3886/ICPSR32722.v1
Chapter 5:
Johnston, L. D., O’Malley, P. M., Bachman, J. G., & Schulenberg, J. E. (2011). Monitoring the Future national survey results on drug use, 1975–2010: Volume II, College students and adults ages
19–50. Ann Arbor: Institute for Social Research, The University of Michigan.
Substance Abuse and Mental Health Services Administration, State Estimates of Substance Use and Mental Disorders from the 2008-2009 National Surveys on Drug Use and Health, NSDUH Series
H-40, HHS Publication No. (SMA) 11-4641. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2011.
Substance Abuse and Mental Health Services Administration, Results from the 2010 National Survey on Drug Use and Health: Summary of National Findings, NSDUH Series H-41, HHS
Publication No. (SMA) 11-4658. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2011.
Chapter 6:
American College Health Association. American College Health Association-National College Health Assessment II: Reference Group Data Report Fall 2011. Hanover, MD: American Health
Association; 2010
Finer LB, Zolna MR. Unintended pregnancy in the United States: incidence and disparities, 2006. Contraception 2011; 84:478-485
Centers for Disease Control and Prevention (CDC). 1991-2009 High School Youth Risk Behavior Survey Data. Available at http://apps.nccd.cdc.gov/youthonline. Accessed on April 18, 2012.
Centers for Disease Control and Prevention (CDC). Youth Risk Behavior Surveillance - United States, 2011 Data. Available at http://www.cdc.gov/mmwr/pdf/ss/ss6104.pdf. Accessed on December
26, 2012.
Kost K, Henshaw S, and Carlin L, U.S. Teenage Pregnancies, Births and Abortions: National and State Trends and Trends by Race and Ethnicity, 2010, http://www.guttmacher.org/pubs/USTPtrends.
pdf.
Hamilton BE, Martin JA, Ventura SJ. Births: Preliminary data for 2010. National vital statistics reports; vol 60 no 2. Hyattsville, MD: National Center for Health Statistics. 2011.
Herbenick D, Reece M, Schick V, Sanders SA, Dodge B, and Fortenberry JD. Sexual behavior in the United States: Results from a national probability sample of men and women ages 14-94. J Sex
Med 2010;7(suppl 5): 255-265.
National Survey of Family Growth 2006-2010. Public Use Data Files. National Center for Health Statistics. Available from http://www.cdc.gov/NCHS/nsfg/nsfg_2006_2010_puf.htm
StataCorp. 2011. Stata Statistical Software: Release 12. College Station, TX: StataCorp LP.
Chapter 7:
Centers for Disease Control and Prevention. HIV Surveillance Report, 2010; vol. 22. http://www.cdc.gov/hiv/topics/surveillance/resources/reports/. Published March 2012. Accessed [4/9/2012].
Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2010. Atlanta: U.S. Department of Health and Human Services; 2011.
Gillison ML, Broutian T, Pickard RKL, Maura L, Tong Z, Xiao W, Kahle L, Graubard BI, Chaturvedi AK. Prevalence of oral HPV infection in the United States, 2009-2010. JAMA. 2012.
doi:10.1001/jama.2012.101.
Insinga RP, Dasbach EJ, Myers ER. The Health and Economic Burden of Genital Warts in a Set of Private Health Plans in the United States. Clinical Infectious Diseases 2003; 36: 1397-403.
National Center for Health Statistics. Health, United States, 2010: With Special Feature on Death and Dying. Hyattsville, MD. 2011
Sexually Transmitted Diseases in California, 2010. California Department of Public Health, STD Control Branch, October 2011.
78
Chapter 8:
2010 National Health Interview Survey (NHIS) Prevalence Data. 2010 Lifetime and Current Asthma. National Center for Health Statistics. Available from http://www.cdc.gov/asthma/nhis/2010/
data.htm.
California Health Interview Survey. 2005 California Health Interview Survey. AskCHIS. Los Angeles, CA: UCLA Center for Health Policy Research.
California Health Interview Survey. 2009 California Health Interview Survey. AskCHIS. Los Angeles, CA: UCLA Center for Health Policy Research.
California Health Interview Survey. CHIS 2009 Adult Survey. UCLA Center for Health Policy Research. Los Angeles, CA: November 2011.
California Health Interview Survey. CHIS 2009 Teen Survey. UCLA Center for Health Policy Research. Los Angeles, CA: November 2011.
Centers for Disease Control and Prevention (CDC). Behavioral Risk Factor Surveillance System Survey Data. Atlanta, Georgia: U.S. Department of Health and Human Services, Centers for Disease
Control and Prevention, 2010.
Centers for Disease Control and Prevention (CDC). National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Data. Hyattsville, MD: U.S. Department of
Health and Human Services, Centers for Disease Control and Prevention, 2008-2009.
Centers for Disease Control and Prevention (CDC). National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Data. Hyattsville, MD: U.S. Department of
Health and Human Services, Centers for Disease Control and Prevention, 2009-2010. http://www.cdc.gov/nchs/nhanes/nhanes2009-2010/nhanes09_10.htm.
Centers for Disease Control and Prevention. Prevalence and Most Common Causes of Disability Among Adults---United States, 2005. MMWR 58(16):421-426.
Devol, R. and Bedroussian, A. (October 2007). An Unhealthy America: The Economic Burden of Chronic Disease—Charting a New Course to Save Lives and Increase Productivity and Economic
Growth. Available from http://www.chronicdiseaseimpact.com/ebcd.taf
Dempsey AF, Gebremariam A, Koutsky LA, & Manhart L. (2008). Using risk factors to predict human papillomavirus infection: Implications for targeted vaccination strategies in young adult
women. Vaccine, 26(8): 1111-1117.
Division for Heart Disease and Stroke Prevention: Data Trends & Maps Web site. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention (CDC), National
Center for Chronic Disease Prevention and Health Promotion, Atlanta, GA, 2010. Available at http://www.cdc.gov/dhdsp/.
Gillison ML, Broutian T, Pickard RKL, Tong Z, Xiao W, Kahle L, Graubard BI, & Chaturvedi AK. (2012). Prevalence of Oral HPV Infection in the United States, 2009-2010. JAMA, 307(7): 693703.
Howlader N, Noone AM, Krapcho M, Neyman N, Aminou R, Altekruse SF, Kosary CL, Ruhl J, Tatalovich Z, Cho H, Mariotto A, Eisner MP, Lewis DR, Chen HS, Feuer EJ, Cronin KA (eds).
SEER Cancer Statistics Review, 1975-2009 (Vintage 2009 Populations), National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2009_pops09/, based on November 2011 SEER
data submission, posted to the SEER web site, April 2012.
National Center for Health Statistics. Health, United States, 2010: With Special Feature on Death and Dying. Hyattsville, Maryland. 2011.
National Health Interview Survey 2010. Sample Adult File. Public Use Data Files. National Center for Health Statistics. Available from http://www.cdc.gov/nchs/nhis/nhis_2010_data_release.htm.
National Health Interview Survey 2010. Sample Child File. Public Use Data Files. National Center for Health Statistics. Available from http://www.cdc.gov/nchs/nhis/nhis_2010_data_release.htm.
Northern California Kaiser Permanente, personal communication, 2011
Siegel, SE. (2010). Adolescents and Young Adults (AYA) with Cancer: The Lost and ? Found Generation. [PowerPoint Slides].
StataCorp. 2011. Stata Statistical Software: Release 12. College Station, TX: StataCorp LP.
Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) SEER*Stat Database: Incidence - SEER 9 Regs Research Data, Nov 2011 Sub (1973-2009) <Katrina/Rita
Population Adjustment> - Linked To County Attributes - Total U.S., 1969-2010 Counties, National Cancer Institute, DCCPS, Surveillance Research Program, Surveillance Systems Branch, released
April 2012, based on the November 2011 submission.
Surveillance Research Program, National Cancer Institute SEER*Stat software (seer.cancer.gov/seerstat) version <version number>.
Chapter 9:
California Health Interview Survey. CHIS 2009 Adult Survey. UCLA Center for Health Policy Research. Los Angeles, CA: November 2011.
Centers for Disease Control and Prevention (CDC). Behavioral Risk Factor Surveillance System Survey Data. Atlanta, Georgia: U.S. Department of Health and Human Services, Centers for Disease
Control and Prevention, 2009.
Centers for Disease Control and Prevention (CDC). Behavioral Risk Factor Surveillance System Survey Data. Atlanta, Georgia: U.S. Department of Health and Human Services, Centers for Disease
Control and Prevention, 2010.
Centers for Disease Control and Prevention (CDC). National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Data. Hyattsville, MD: U.S. Department of
Health and Human Services, Centers for Disease Control and Prevention, 2009-2010.
National Center for Health Statistics. Health, United States, 2010: With Special Feature on Death and Dying. Hyattsville, MD. 2011
National Health Interview Survey 2010. Sample Adult File. Public Use Data Files. National Center for Health Statistics. Available from http://www.cdc.gov/nchs/nhis/nhis_2010_data_release.htm.
National Survey of Family Growth 2006-2010. Public Use Data Files. National Center for Health Statistics. Available from http://www.cdc.gov/NCHS/nsfg/nsfg_2006_2010_puf.htm
Ozer EM, Urquhart JT, Brindis CD, Park MJ, & Irwin CE. (2012). Young Adult Preventive Health Care Guidelines: There But Can’t be Found. Archives of Pediatric and Adolescent Medicine,
166(3):240-247.
StataCorp. 2011. Stata Statistical Software: Release 12. College Station, TX: StataCorp LP.
U.S. Department of Agriculture, Agricultural Research Service. 2010. Nutrient Intakes from Food: Mean Amounts Consumed per Individual, by Gender and Age, What We Eat in
America,NHANES 2007-2008. Available: www.ars.usda.gov/ba/bhnrc/fsrg.
Chapter 10:
Personal communication, large insurance company 2012.
California Health Interview Survey. 2009 California Health Interview Survey. AskCHIS. Los Angeles, CA: UCLA Center for Health Policy Research.
Centers for Disease Control and Prevention (CDC). National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Data. Hyattsville, MD: U.S. Department of
Health and Human Services, Centers for Disease Control and Prevention, 2007-2008.
Centers for Disease Control and Prevention. (2011). National Center for Chronic Disease. Physical Activity for Everyone: Guidelines: Adults. http://www.cdc.gov/physicalactivity/everyone/
guidelines/adults.html
Mendes E: In U.S., Uninsured Rate for 18- to 25-Year-Olds Plateaus, Gallop Poll, April 3, 2012 (http://www.gallup.com/poll/153737/uninsured-rate-year-olds-plateaus.aspx)
MEPSnet Household Component for 2009. February 2009. Agency for Healthcare Research and Quality, Rockville, MD. http://www.meps.ahrq.gov/data_stats/mepsnet/mepsnethc09.shtml
National Center for Health Statistics. Health, United States, 2010: With Special Feature on Death and Dying. Hyattsville, MD. 2011
References
79
“Emerging young adults
are adrift in a perfect
storm of health risks”
This report would not have been possible without the support and sponsorship of:
California Wellness Foundation
■
Leonard D. Schaeffer Center for Health Policy and Economics, University of Southern California
■
The Community, Health Outcomes & Intervention Research Program,
The Saban Research Institute of Children’s Hospital Los Angeles
■
Division of College Health, Department of Pediatrics, Keck School of Medicine of USC
and Division of Student Affairs, University of Southern California
■
© 2013 The New Adolescents: An Analysis of Health Status, Lawrence Neinstein MD
80