The Response of Ontario Primary Care Physicians to Pay-for-Performance Incentives Jeremiah Hurley
advertisement

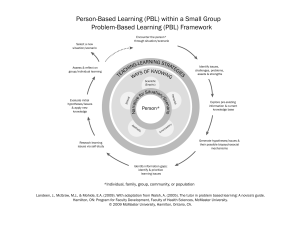
The Response of Ontario Primary Care Physicians to Pay-for-Performance Incentives Jeremiah Hurley1,2,3 Jinhu Li1,2,4 1 Department 2 Centre Gioia Buckley2,3 of Economics, McMaster University for Health Economics and Policy Analysis, McMaster University 3 Department 4 Melbourne Phil DeCicca1,2 of Clinical Epidemiology and Biostatistics, McMaster University Institute of Applied Economic and Social Research, University of Melbourne September, 2011 Acknowledgments This research was undertaken as part of the MOHLTC-CHEPA collaborative research program. We thank Marsha Barnes for initially sponsoring this project and Mary Fleming for continued support. We are greatly indebted to Delia D’Amore of the Ontario Ministry of Health and Long-Term Care for sharing her time and expertise answering our many questions regarding the data and the Ministry’s administrative processes related to payment policies and regulations. We also thank the following individuals from the MOHLTC whose assistance has been instrumental at various stages of this work: Teo Honrado, Mike Collisson, Terry Stevens, Jiahui Wong, Alex Firby, Kathryn Doresco, James Gonneau, Carol MacIsaac, Barry Monaghan, Patricia Durnford, Amy Johnston, Mahroo Afrashteh, Alana Salmon and Paul Kaufman. We thank Charles Sagoe of Cancer Care Ontario for his assistance in helping us obtain data extracted from CCOs Ontario Breast Screening Program Database. We thank Dr. Leslie Solomon for his expertise and helpful advice and Andrea Ruskova, Ji Li, Sumangala Shanmuganathan and Wendy Ho for excellent research assistance. Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 2 / 23 Pay-for-Performance Incentives In Ontario Primary Care • Late 1990s: introduced for Primary Care Network (PCN) practices • 2002: Incorporated into funding model for Family Health Network (FHN) Practices • 2004-2008 Agreement: expanded the incentives and the practices eligible for them Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 3 / 23 Pay-for-Performance Incentives In Ontario Primary Care • Late 1990s: introduced for Primary Care Network (PCN) practices • 2002: Incorporated into funding model for Family Health Network (FHN) Practices • 2004-2008 Agreement: expanded the incentives and the practices eligible for them Elsewhere • Pay-forperformance is perhaps one of the most widely advocated policies of the last decade. • UK NHS: Quality and Outcomes Framework • U.S.: private health plans and Medicare program • Australia: Practice Incentive Progam • Canada: British Columbia, Manitoba, Ontario, Nova Scotia Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 3 / 23 Evidence Regarding the Effectiveness of P4P The Overall Literature • limited empirical literature; much of it methodologically weak • available evidence is mixed Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 4 / 23 Evidence Regarding the Effectiveness of P4P The Overall Literature • limited empirical literature; much of it methodologically weak • available evidence is mixed UK NHS Primary Care • implemented system-wide, so no control group • only one part of a broader set of quality initiatives • Campbell et al. (2009) • interrupted time-series: 1998, 2003, 2005, 2007 • three conditions: asthma, heart disease and type-2 diabetes • 2005: increased quality for asthma and diabetes; no change for heart disease • 2007: increase had leveled off for all three conditions Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 4 / 23 Evidence Regarding the Effectiveness of P4P US Health Plans • Rosenthal et al. (2005), Mullen et al. (2010) • Large network HMO: compare physician groups exposed to incentives against physician groups not exposed to incentives. • Rosenthal et al.: cervical cancer screening, mammography and hemoglobin A1c testing • evidence of effect only for Pap smear coverage (3.6 percentage points, or about 10%) • Mullen et al.: expanded set of services • positive effect only for Pap smear coverage; possible negative effect for asthma medication and antibiotic usage Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 5 / 23 Evidence Regarding the Effectiveness of P4P Systematic Reviews Giuffrida et al. (1999), Armour et al. (2001), Town et al. (2005), Peterson et al. (2006), Christianson et al. (2008). Scott et al. (2011) • • • • evidence base is relatively weak evidence is mixed but overall suggests modest effects outcomes often process measures not necessarily related to quality expensive per unit of change achieved Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 6 / 23 Our Primary Research Question Have the performance-based incentive payments for five preventive care services and for six defined sets of physician services increased the provision of these services in the target populations? Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 7 / 23 Our Primary Research Question Have the performance-based incentive payments for five preventive care services and for six defined sets of physician services increased the provision of these services in the target populations? Preventive care services: • • • • • senior flu shots toddler immunizations cervical cancer screening breast cancer screening colorectal cancer screening Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 7 / 23 Our Primary Research Question Have the performance-based incentive payments for five preventive care services and for six defined sets of physician services increased the provision of these services in the target populations? Preventive care services: • • • • • senior flu shots toddler immunizations cervical cancer screening breast cancer screening colorectal cancer screening Six sets of physician services: • • • • • • obstetrical services hospital services palliative care services office procedures prenatal care home visits Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 7 / 23 The Ontario P4P Incentives in Our Study Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 8 / 23 Our Study • Design: before-after study with concurrent comparison group (difference-in-differences) • Treatment group: physicians in PCRs exposed to the incentives • Comparison group: physicians who remained in FFS practice (who were never exposed to the incentives) Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 9 / 23 Our Study • Design: before-after study with concurrent comparison group (difference-in-differences) • Treatment group: physicians in PCRs exposed to the incentives • Comparison group: physicians who remained in FFS practice (who were never exposed to the incentives) • Unit of analysis: individual physician practice Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 9 / 23 Our Study • Design: before-after study with concurrent comparison group (difference-in-differences) • Treatment group: physicians in PCRs exposed to the incentives • Comparison group: physicians who remained in FFS practice (who were never exposed to the incentives) • Unit of analysis: individual physician practice • Data: 1996-2008: OHIP claims data, Registered Persons Database, Corporate Provider Database, Client Agency Program Enrolment, Breast Cancer Screening Database • enabled us to define each physician’s practice population as of March 31 of each year. Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 9 / 23 Our Study • Design: before-after study with concurrent comparison group (difference-in-differences) • Treatment group: physicians in PCRs exposed to the incentives • Comparison group: physicians who remained in FFS practice (who were never exposed to the incentives) • Unit of analysis: individual physician practice • Data: 1996-2008: OHIP claims data, Registered Persons Database, Corporate Provider Database, Client Agency Program Enrolment, Breast Cancer Screening Database • enabled us to define each physician’s practice population as of March 31 of each year. • Features of our design • assumes that trend for FFS MDs represents well what would have happened without the incentives for those in the PCR practices • control for selected physician/practice characteristics • exploit variation in incentives across PCR groups • sub-groups analysis: baseline level of provision, physician age, practice size Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 9 / 23 Study Sample Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 10 / 23 Variable Definitions Dependent Variables Preventive Care Bonuses: proportion of a physician’s target practice population as of March 31 each year who had received the service in question during the relevant period prior to that March 31. Special Payments: dichotomous variable taking a value of 1 if a physician’s service provision met the criteria for the special payment of interest and 0 otherwise. Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 11 / 23 Variable Definitions Dependent Variables Preventive Care Bonuses: proportion of a physician’s target practice population as of March 31 each year who had received the service in question during the relevant period prior to that March 31. Special Payments: dichotomous variable taking a value of 1 if a physician’s service provision met the criteria for the special payment of interest and 0 otherwise. Independent Variables Physician Characteristics: age, sex, years in practice Practice Characteristics: location (urban/rural), size of practice population, age-sex distribution of patient population, activity levels (e.g., days worked per year, number of visits, intensity of visits per day), and practice model (FFS, FHN, FHG, CCM, FHO) Treatment Dummies: treatment/control group, pre/post policy, relevant interactions Other : year dummies, census division Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 11 / 23 Descriptive Statistics: Distribution Across Practice Types Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 12 / 23 Eligibility for Bonuses Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 13 / 23 Descriptive Statistics: Sample Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 14 / 23 Response to Contact Incentive Payment Proportion of Eligible Family Physicians Who Submitted at Least One Claim for the Contact Incentive Payment Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 15 / 23 Response to Preventive Care Bonuses Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 16 / 23 Response to Preventive Care Bonuses Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 17 / 23 Response to Preventive Care Bonuses Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 18 / 23 Response to Special Payments Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 19 / 23 Sub-group Analysis: Preventive Care Bonuses Physician Age • Pap Smear, Mammogram, Colorectal Cancer: younger physicians respond more than older Size of Practice Population • Senior Flu Shot, Mammogram, Colorectal Cancer: weak gradient whereby those with larger practice populations respond more than those with small practice populations Baseline Level of Provision • Senior Flu Shot, Mammogram, Colorectal Cancer: those in the low and middle quartiles of baseline provision responded more than those in the top quartile Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 20 / 23 Sensitivity Analysis: Preventive Care Bonuses The findings are robust to: • exclusion of shadow-billed tracking Q-codes among PCR physicians • change in practice definition of PCR physicians to include both rostered and non-rostered patients • exclusion of CCM or FHG PCR physicians who did not meet minimum roster size of 450 or 650 • dropping the first year of eligibility for bonuses Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 21 / 23 Conclusion and Implications • No evidence of any response to the special payments for obstetrical services, hospital services, palliative care, office procedures, prenatal care, or home visits • Evidence of modest response to 4 of the 5 Preventive Care Bonuses • largest responses for Colorectal Cancer Screening (FOBT) (increase in coverage from 15% to 23.5%) and Pap Smear (58.9% to 63%) • small response for mammogram (64.6% to 66.4%) and senior flu shot (55.4% to 58.2%) • no response for toddler immunization • The pattern of responses across incentives likely reflects: • differential costs of responding • strength of evidence regarding the effectiveness and appropriateness of the services • Overall, the findings suggest that, for these services at least, the pay-for-performance incentives do not represent a good financial investment Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 22 / 23 References Armour B, Pitts M, Maclean R, et al. “The Effect of Explicit Financial Incentives on Physician Behavior.” Archives of Internal Medicine 2001;161(10):1261-6. Campbell SM, Reeves D, Kontopantelis E, et al. “Effects of Pay for Performance on the Quality of Primary Care in England.” The New England Journal of Medicine 2009;361(4):368-78. Christianson JB, Leatherman S, Sutherland K. “Lessons From Evaluations of Purchaser Pay-for-Performance Programs: A Review of the Evidence.” Medical Care Research & Review 2008;65(6-suppl):5S-35. Giuffrida A, Gosden T, Forland F, et al. “Target payments in primary care: effects on professional practice and health care outcomes.” Cochrane Database of Systematic Reviews 1999(4). Mullen KJ, Frank RG, Rosenthal MB. “Can you get what you pay for? Pay-for-performance and the quality of healthcare providers.” The RAND Journal of Economics 2010;41(1):64-91. Petersen LA, Woodard LD, Urech T, et al. “Does pay-for-performance improve the quality of health care?” Annals of Internal Medicine 2006;145 (4):265-72. Rosenthal M, Frank R, Li Z, et al. “Early Experience with Pay for Performance: From Concept to Practice.” Journal of the American Medical Association 2005;294(14):1788-93. Town R, Kane R, Johnson P, et al. “Economic Incentives and Physicians’ Delivery of Preventive Care.” American Journal of Preventive Medicine 2005;28(2):234-40. Hurley et al. (Centre for Health Economics and Policy Analysis, McMaster University) 23 / 23