Health Services Research Funding: Cross Institution Perspectives &
advertisement

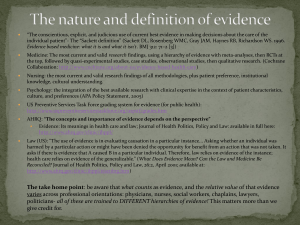
Health Services Research Funding: Cross Institution Perspectives & Dialogue About Priorities Carolyn M. Clancy, MD Francis Chesley, MD Agency for Healthcare Research and Quality AcademyHealth 2009 Annual Research Meeting Chicago – June 28, 2009 Health Care Reform in the Current Economic Environment 59% 37% It is more important than ever to take on h lth care health reform now We cannot afford to take on health care reform right now 4% Kaiser Family Foundation Health Tracking Poll (Conducted (April 2 2--8, 2009) Don’t Know/Refused More Say Reform Would Help Country Do you think (you and your family/the country as a whole) would be better off if the president and Congress passed health care reform, or don’t you think it would make much difference? Better Off Wouldn’t Make M h Diff Much Difference Worse Off It Depends 4% …you you and your family 43% 36% 14% 3% …the country as a whole 56% 21% 15% Kaiser Family Foundation Health Tracking Poll (Conducted April 22-8, 2009) Current Challenges g Concerns C about b h health l h spending di – about b $2 $2.3 3 trillion per year in the U.S. and growing Large variations in clinical care A lot of uncertainty about best practices involving treatments and technologies Pervasive problems with the quality of care that people receive T Translating l ti scientific i tifi advances d iinto t actual t l clinical practice Translating scientific advances into usable information for clinicians and patients HSR Perspectives and Priorities AHRQ R Resources & P Priorities i ii Research Opportunities & A ti iti Activities Comparative Effectiveness R Research: h Th The N New P Paradigm di Improving Quality & Access Q&A HHS Secretary y Kathleen Sebelius “It It is an honor to lead the Department of Health and Human Services and I am grateful for the opportunity to serve at such a pivotal moment in our history” Kathleen Sebelius Sworn in as the 21st Secretary of the Department of Health and Human Services A il 29 April 29, 2009 AHRQ’s Q Mission Improve the quality quality, safety safety, efficiency and effectiveness of health care for all Americans AHRQ Q Priorities Patient Safety Health IT Patient Safety Ambulatory P ti t Safety Patient S f t Safety & Quality Measures, Organizations N New P Patient ti t Safety Grants Drug Management and Patient-Centered Care P ti t Safety Patient S f t IImprovementt Corps Effective Health Care Program Comparative Effectiveness Reviews Comparative Effectiveness Research Clear Findings for Multiple Audiences Other Research & Dissemination Activities Medical Expenditure Panel Surveys Visit-Level Information on Quality & Cost-Effectiveness, e.g. Medical Expenditures Annual Quality & Disparities Reports Prevention and Pharmaceutical Outcomes U.S. Preventive Services Task Force MRSA/HAIs Updated p Portfolios Value – Goal: Support the development of health care activities that help reduce unnecessary waste while improving quality Innovations/Emerging I ti /E i Issues – Goal: Identify y and support pp ideas and projects that have the potential for highly innovative solutions to health care challenges AHRQ Q FY 2009 Funding g $372 million – $37 million more than FY 2008 – $46 million more than the president’s president s request FY 2009 appropriation includes: – $50 million for comparative effectiveness research, $20 million more than FY 2008 research – $49 million for patient safety activities – $45 million for health IT HSR Perspectives and Priorities AHRQ R Resources & P Priorities i ii Research Opportunities & A ti iti Activities Comparative Effectiveness R Research: h Th The N New P Paradigm di Improving Quality & Access Q&A Research Opportunities pp Health IT Funding Opportunities – PAR PAR--08 08--270 Utilizing Health Information Technology (IT) to Improve Health Care Quality (R18) – PAR PAR--08 08--269 Exploratory and Developmental Grant to Improve Health Care Quality through Health Information T h l Technology (IT) (R21) – PAR PAR--08 08--268 Small Research Grant to I Improve Health H lth C Care Q Quality lit th through h Health Information Technology (IT) (R03) Research Opportunities pp PA PA--09 09--071 AHRQ Health Services Research Demonstration and Dissemination Grants (R18) PA PA--09 09--070 AHRQ Health Services Research Projects (R01) PAR PAR--08 08--136 Researching g Implementation p and Change While Improving Quality (R18) PA PA--06 06--448 448AHRQ AHRQ Small Research Grant Program (R03) 2009 Priorities for K Award Funding PAR PAR--09 09--087 Mentored Research Scientist Research Career Development Award (K01) PAR PAR--09 09--086 Independent Scientist Award (K02) PAR PAR--09 09--085 Mentored Research Scientist Research Career Development Award (K08) Children’s Health Insurance Program Reauthorization Act of 2009 (CHIPRA) AHRQ Activities Focus on identifying Initial Core Health Care Quality Measure Set Memorandum of Understanding and OU and IntraIntra- Agency Agreement with CMS Federal Quality Workgroup Established AHRQ NAC Subcommittee Established – First Meeting July 2222-23, 2009 - PUBLIC – Report back to full NAC July 24 24, 2009 – Second Meeting Sep. 1717-18, 2009 (tentative) http://www.ahrq.gov/chip/chipraact.htm CHIPRA: Phase II Pediatric quality measures program – IA with CMS – Expert meeting on measure development, testing validation criteria testing, Evaluation of demos – IA with CMS Patient Safety y Organizations g (PSOs) ( ) 63 PSOs to Date (and growing) – PSO certification and listing is implemented by AHRQ. Compliance and confidentiality is enforced by the Office for Civil Rights Future Opportunity – Availability of data for research www.pso.ahrq.gov First Annual PSO Meeting – September 1616-18, 2009, AHRQ PSO Privacy Protection Center Launched Multi--Media Campaigns Multi Get Patients Involved AHRQ expands Ad Council campaign with ith a new series i off TV and d radio di public service announcements along with printed consumer resources http://www.ahrq.gov/questionsaretheanswer HSR Perspectives and Priorities AHRQ R Resources & P Priorities i ii Research Opportunities & A ti iti Activities Comparative Effectiveness R Research: h Th The New N Paradigm P di Improving Quality & Access Q&A U.S. Landscape for Comparative Effectiveness Research Well intentioned Ad hoc except for AHRQ AHRQ’ss mandate Limited capacity to do the research and translate the research into meaningful g and useable applications Shared Perspectives on p Effectiveness Comparative Comparative effectiveness should be a public good that: – Gives health care decision makers – patients, clinicians, purchasers and policy makers – access to the latest open and unbiased evidenceevidence-based information about treatment options – Informs choices and, where possible, is closely aligned with the sequence of decisions patients and clinicians face The Right Treatment for the Right Patient at the Right Time Comparative Effectiveness Research Comparative effectiveness research serves as a foundation for evidence on what services work best in health care Comparisons of medical options helps p clinicians and p patients make individualized treatment decisions The information base on what services improve quality quality, safety and effectiveness is enhanced Consumers play important roles in d developing l i and d using i the h information as citizens, community members, participants in policy deliberations and as patients Comparative Effectiveness and the Recovery Act The American Recovery and Reinvestment Act of 2009 includes $1.1 billion for comparative effectiveness ff ti research: h – AHRQ: $300 million – NIH: $400 million (appropriated to AHRQ and transferred to NIH) – Office of the Secretary: $400 $ million (allocated at the Secretary’s discretion) www.hhs.gov/recovery Federal Coordinating g Council Anne Haddix Haddix, CDC Elizabeth Nabel Nabel, NIH Thomas Valuck, CMS Jesse Goodman, FDA Peter Delany Delany, SAMHSA Michael Marge, Marge Office on Carolyn Clancy, AHRQ Disability Deborah Hopson Hopson, HRSA Neera Tanden,, HHS David Hunt, ONC Joel Kupersmith, VA James Scanlon Scanlon, HHS Michael Kilpatrick, p , DoD Garth Graham, Office of Ezekiel Emanuel, OMB Minority Health Other Aspects of y Act the Recovery Comparative Effectiveness Research conducted with funds appropriated under the Recovery Act, “shall be consistent with Departmental policies relating to the inclusion of women and minorities minorities.” Congress does not intend for the research money to be used to “mandate mandate coverage reimbursement or other policies for any public or private payer.” Details about the types of research being funded or supported must be submitted to Congress every six months, beginning Nov. 1, 2009 www.hhs.gov/recovery Meaningful g Use The Recovery Act calls for establishment of an incentive for providers who become “meaningful g users” of electronic health records A Federal Health IT Policy y Committee workgroup is developing criteria for a definition of meaningful use The focus: quality outcomes, health status and cost control http://healthit.hhs.gov Meaningful g Use: AHRQ’s Q Role AHRQ provides Federal partners with the best available evidence on how proposed criteria for meaningful g use might g help p to achieve the ultimate goal of high quality, high value health care – AHRQ grantees and contractors have been significant contributors to the public di discussion i on meaningful i f l use – The Agency also participates in internal Federal discussions about meaningful use AHRQ’s Role in Comparative Effectiveness Using Information to Drive Improvement: S i tifi IInfrastructure Scientific f t t to t Support S t Reform R f Providing information that can be used on the frontlines of treatment Helping to make decisions more consistent, transparent and rational 21st Century Health Care Ensuring the effectiveness data is more widely used Promoting an open and collaborative approach to comparative effectiveness The Effective Health Care Program at AHRQ A. Evidence synthesis (EPC program) – – Systematically reviewing, synthesizing, comparing existing evidence on treatment effectiveness Identifying relevant knowledge gaps B. Evidence generation (DEcIDE, CERTs) – – Development of new scientific knowledge to address knowledge gaps. Accelerate practical studies C. Evidence communication/translation (Eisenberg Center) – – T Translate l evidence id iinto iimprovements Communication of scientific information in plain language to policymakers, patients, and providers Transparent Collaborative Process with New Opportunities Expanded infrastructure and capacity for Comparative Effectiveness Research Prospective studies that include under under-represented populations Pushing forward on methods for Comparative Effectiveness Research Increasing I i iinvestments t t in i iinnovative ti broad dissemination and translation Moving Forward: Issues to Consider Comparative Effectiveness is a useful tool in a much larger toolkit – it is necessary but not sufficient It does d nott make k policy li or h health lth care d decisions, i i tell doctors how to practice medicine or make final decisions about what kind of treatments insurers will pay for It does weigh the evidence and present it in a way th t helps that h l consumers and d th their i d doctors t make k th the best possible decisions about health care choices It’s It s also an opportunity to identify what is not known/areas where research is needed HSR Perspectives and Priorities AHRQ R Resources & P Priorities i ii Research Opportunities & A ti iti Activities Comparative Effectiveness R Research: h Th The N New P Paradigm di Improving Quality & Access Q&A AHRQ’s National Reports on Quality and Disparities New Reports p Released May y 9th The median annual rate of change g for all q quality y measures was 1.4% – Of 190 measures, 132 (69%) showed h d some iimprovementt Some reductions in disparities of care according to race, ethnicity, and income – Disparities persist in health care quality and access Quality Q y Report: p Key y Findings g Median level of patients receiving needed care was 59% for core quality measures Q Qualityy improvements p spread p unevenly y across settings of care (hospitals, home care, longlongterm care, ambulatory care) Measures of patient safety in the Quality Report indicate a 1% annual decline Need N d consensus on single i l core sett off measures to be used by all payers and stakeholders to monitor improvement p Disparities p Report: p Key y Findings g 60% of measures of quality are not improving for Blacks, Asians, American Indians/Alaska Natives (AI/AN), Hispanics, poor populations; t d for trend f 6 years 80% of access measures stayed the same or got worse for Hispanics 60% of access measures stayed the same or got worse for Blacks and Asians 57% of access measures stayed the same or got worse for p g poor p populations p Illinois: Overall Health Care Quality Performance vs. All States, O -Year OneOne Y Performance P f Change Ch Average Weak Strong Very Weak Very Strong Performance Meter = Most Recent Year = Baseline Year 2008 National Healthcare Quality Report, State Snapshots Illinois Snapshot p Measure % of adult surgery patients who received prophylactic antibiotics within 1 hour prior to surgical incision % of children ages 1919-35 months who received all recommended vaccines % of smokers with heart attack who received smoking cessation counseling while hospitalized Performance Better than Average Average g Lower than A Average National Healthcare Quality Report, State Snapshots, 2008 Disparities Report: Biggest Gaps by Population Proportion of new AIDS cases was 9 9.4 4 times as high for Blacks as Whites Rate of new AIDS cases more than 3 times as high for Hispanics as for nonnon-Hispanic Whites AI/AN women more than twice as likely to lack prenatal care as White women Asians more likely than Whites to not get ti l care ffor illness timely ill or iinjury j Poor adults more than twice as likely as highhighincome adults not to get timely care for an illness or injury Efforts to Address Disparities Through g Data,, Research Partnerships p to raise awareness: – Health Disparities Roundtable (Office of Minority – – – – Health, AHRQ, Institute of Medicine) F d l Collaboration Federal C ll b ti on Health H lth Disparities Di iti Research (CDC, OMH, AHRQ) Disparities p Reducing g Advances Project j ((CDC,, NCI, ACS, Robert Wood Johnson Foundation, University of Texas Medical Branch) CMS Health Disparities Program (OMH, (OMH NIH and Administration on Aging) National Business Group on Health Racial and Ethnic Health Disparities Advisory Board (OMH, business, medicine, public health groups) Moving the Needle Quality y Improvement p on Q Themes emerging from draft legislation – New N ffocus on USPSTF – Increased focus on quality – Comparative Effectiveness Research and Health IT are critical iti l tto any quality lit improvement effort 21st Century Health Care: The Future Public Public--private funding and participation likely a necessity More effort to get better conditional reimbursement i b t study t d d designs/protocols i / t l Patients should be engaged as partners at the local and national levels Need to tackle important issues – – – – Ethical When to know when the evidence is sufficient Transparency Setting priorities 2009 AHRQ Q Annual Conference “Research to Reform: A hi i Achieving H Health lth S System t Ch Change” ” September 1313-16, 2009 Bethesda North Marriott Convention Center Bethesda, MD S Sessions i on topics t i including i l di the th following: f ll i - Increased Funding for Comparative Effectiveness - AHRQ AHRQ’s s Rapidly Expanding Health IT Portfolio - Implementation of Research Findings into Changes in Practice and Policyy MARK YOUR CALENDARS! HSR Perspectives and Priorities AHRQ R Resources & P Priorities i ii Research Opportunities & A ti iti Activities Comparative Effectiveness R Research: h Th The N New P Paradigm di Improving Quality & Access Q&A