Unintended Consequences of Quality Targets, Public Reporting, and No-Pay Policies

Unintended Consequences of
Quality Targets, Public Reporting, and No-Pay Policies
Don Goldmann, MD
Institute for Healthcare Improvement
Harvard Medical School
Harvard School of Public Health dgoldmann@ihi.org
No conflicts to declare
Mandates are Proliferating
•
Public Reporting of infection control rates and other health outcomes may:
–
Accelerate improvement in focused areas
–
Improve accountability
–
Improve consumer information and choice and/or
–
Provide a false sense of security and mask other deficiencies
–
Lead to unintended adverse consequences
–
Drain resources and will from other worthy quality and safety goals (“opportunity costs”)
The UK Healthcare System Offers a Case
Study in Target-Based Accountability
•
Numerous government mandated targets
•
Exploitation by an inflammatory press
•
Extreme executive accountability
•
Large-scale disenchantment with the multiplicity of targets in narrowly defined areas without additional resources or help with systems improvement
•
….But some exceptional results
July 25 th 2006
Impact quarterly cases of MRSA bacteraemia:
English NHS Mandatory Surveillance 2001 - 2008
English NHS Mandatory Surveillance
Performance Update
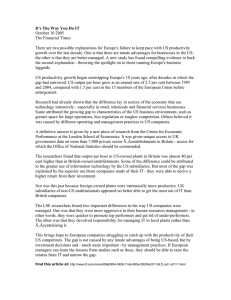
Average for 05/06 year = 98.2%
Performance in accident & emergency services, NHS in England:
Weekly national performance to 25 Dec 05
All type: 98.5%
100%
98%
96%
94%
92%
90%
88%
Type 1: 98.1%
86%
84%
82%
August ’03 and ‘04
Christmas ’03 and ‘04
80% jan 03 apr 03 jul 03 oct 03 jan 04 apr 04 jul 04 oct 04 Jan 05 apr 05 jul 05 oct 05 jan 06 significant improvement
Trajectory headline performance (all type)
Type 2&3 performance type1 performance
NHS trusts meet A&E waiting targets as demand rises…
Regional performance
–
North East: 98.6 per cent
–
North West: 97.8 per cent
–
Yorkshire and the Humber: 98.2 per cent
–
East Midlands: 98.1 per cent
–
West Midlands: 97.7 per cent
–
East of England: 98.2 per cent
–
London: 97.9 per cent
–
South East Coast: 98.1 per cent
–
South Central: 98.4 per cent
–
South West: 98.4 per cent
Health Services Journal
May 21, 2009
NHS Celebrates Success And Progress
In A&E
2008-09 4 th Q
Mid Staffordshire NHS Foundation Trust
–
Total attendances = 17,953
–
Percent disposition with 4 hours = 98.7%
Medical News Today
June 4, 2009
Healthcare Commission highlights
"appalling" emergency care at Mid
Staffordshire NHS Foundation Trust
Healthcare Commission report, 3/17/09
Failing hospital to review cases
•
Treatment of more than 3,000 patients at a hospital where the NHS's watchdog has said up to 400 people died needlessly could be reviewed.
–
Bosses at Stafford Hospital have pledged to look at 3,200 cases in the wake of a Healthcare Commission report.
–
The Commission said 400 more patients than normal died between 2005-08 as the emergency care was "appalling".
Tribute wall to patients who died at
Stafford Hospital
BBC News, 3/17/09
Cited Failures
•
Low staffing levels, inadequate nursing, lack of equipment, lack of leadership, poor training and ineffective systems for identifying when things went wrong
–
Unqualified receptionists carried out initial checks on patients arriving at the accident and emergency department
–
Patients were "dumped" into a ward near A&E (i.e., Emergency
Dept.) without nursing care so the four-hour A&E waiting time could be met
–
Heart monitors were turned off in the emergency assessment unit because nurses did not know how to use them
–
…and numerous other problems
•
Hospital was well within the national target of <4 hours spent in A&E from arrival to admission, transfer or discharge
Other Consequences
•
Increased A&E utilization
•
Increased short stay hospitalizations
•
Impact on HSMR calculation
CMS/Joint Commission Core Measure for Community-Acquired Pneumonia
•
Antibiotics for pneumonia within 8 hours of admission (later reduced to 4 hours and then consideration of 6)
–
Antibiotics administered to patients with a differential diagnosis including pneumonia to improve performance on publicly reported measure
–
Quinolone antibiotics for community acquired pneumonia supported by IDSA guideline
–
Quinolone antibiotics a risk factor for C. difficile
–
Increased use of antibiotics associated with increased antibiotic resistance
CMS “No-Pay” for Catheter-associated
UTI
•
Pressure to have a “present on admission” (POA) code for UTI
–
Very complex coding scheme
•
MD diagnosis required; nursing notes ignored
•
Burdensome communication with MDs required
•
Increase in screening cultures, especially for atrisk elderly women
•
Asymptomatic bacteriuria discovered
•
Antibiotics administered despite evidence-based guidelines
•
Increased risk of C. diff and antibiotic resistance