CHAPTER 3 Tumours of the Fallopian Tube and Uterine Ligaments
advertisement

CHAPTER 3
Tumours of the Fallopian
Tube and Uterine Ligaments
Tumours of the fallopian tube are much less common than the
corresponding ovarian neoplasms; however, histologically the
same surface epithelial-stromal tumour subtypes are recognized. Sex cord-stromal and germ cell tumours are rare.
Hydatidiform moles and gestational choriocarcinoma are
uncommon complications of tubal ectopic pregnancy. The
wolffian adnexal tumour is also infrequent and typically occurs
in the leaves of the broad ligament.
The risk factors appear similar to those of the ovary. Fallopian
tube carcinomas are a component of the hereditary breastovarian cancer syndrome caused by BRCA1 and BRCA2
germline mutations.
WHO histological classification of tumours of the fallopian tube
Epithelial tumours
Malignant
Serous adenocarcinoma
Mucinous adenocarcinoma
Endometrioid adenocarcinoma
Clear cell adenocarcinoma
Transitional cell carcinoma
Squamous cell carcinoma
Undifferentiated carcinoma
Others
Borderline tumour (of low malignant potential)
Serous borderline tumour
Mucinous borderline tumour
Endometrioid borderline tumour
Others
Carcinoma in situ (specify type)
Benign tumours
Papilloma (specify type)
Cystadenoma (specify type)
Adenofibroma (specify type)
Cystadenofibroma (specify type)
Metaplastic papillary tumour
Endometrioid polyp
Others
Tumour-like epithelial lesions
Tubal epithelial hyperplasia
Salpingitis isthmica nodosa
Endosalpingiosis
Mixed epithelial-mesenchymal tumours
Malignant müllerian mixed tumour
(carcinosarcoma; metaplastic carcinoma)
Adenosarcoma
8441/31
8480/3
8380/3
8310/3
8120/3
8070/3
8020/3
8442/1
8472/1
8380/1
Soft tissue tumours
Leiomyosarcoma
Leiomyoma
Others
Mesothelial tumours
Adenomatoid tumour
Germ cell tumours
Teratoma
Mature
Immature
Others
Trophoblastic disease
Choriocarcinoma
Placental site trophoblastic tumour
Hydatidiform mole
Placental site nodule
Others
8890/3
8890/0
9054/0
9080/0
9080/3
9100/3
9104/1
9100/0
Lymphoid and haematopoetic tumours
Malignant lymphoma
Leukaemia
Secondary tumours
8950/3
8933/3
__________
Morphology code of the International Classification of Diseases for Oncology (ICD-O) {921} and the Systematized Nomenclature of Medicine (http://snomed.org).
Behaviour is coded /0 for benign tumours, /3 for malignant tumours, and /1 for borderline or uncertain behaviour.
1
WHO histological classification of tumours of the broad ligament
and other uterine ligaments
Epithelial tumours of müllerian type
Serous adenocarcinoma
Endometrioid adenocarcinoma
Mucinous adenocarcinoma
Clear cell adenocarcinoma
Borderline tumour (of low malignant potential), (specify type)
Adenoma and cystadenoma (specify type)
Miscellaneous tumours
Wolffian adnexal tumour
Ependymona
8460/3
8380/3
8480/3
8310/3
Papillary cystadenoma (with von-Hippel-Lindau disease)
Uterus-like mass
Adenosarcoma
Others
Mesenchymal tumours
Malignant
Benign
9110/1
9391/3
Secondary tumours
__________
1
Morphology code of the International Classification of Diseases for Oncology (ICD-O) {921} and the Systematized Nomenclature of Medicine (http://snomed.org).
Behaviour is coded /0 for benign tumours, /3 for malignant tumours, and /1 for borderline or uncertain behaviour.
204 Tumours of the fallopian tube and uterine ligaments
8450/0
8933/3
TNM and FIGO classification of carcinomas of the fallopian tube
TNM and FIGO classification 1,2
M1
T – Primary Tumour
TNM
FIGO
Categories
Stages
TX
T0
Tis
0
T1
I
T1a
IA
Note: Liver capsule metastasis is T3/stage III, liver parenchymal metastasis,
M1/stage IV. Pleural effusion must have positive cytology for M1/stage IV.
T1b
IB
T1c
IC
T2
II
T2a
T2b
T2c
IIA
IIB
IIC
T3 and/or N1
III
T3a
T3b
IIIA
IIIB
T3c and/or N1 IIIC
Primary tumour cannot be assessed
No evidence of primary tumour
Carcinoma in situ (preinvasive carcinoma)
Tumour confined to fallopian tube(s)
Tumour limited to one tube, without penetrating
the serosal surface
Tumour limited to both tubes, without penetrating
the serosal surface
Tumour limited to one or both tube(s) with extension
onto or through the tubal serosa, or with malignant
cells in ascites or peritoneal washings
Tumour involves one or both fallopian tube(s) with
pelvic extension
Extension and/or metastasis to uterus and/or ovaries
Extension to other pelvic structures
Pelvic extension (2a or 2b) with malignant cells in
ascites or peritoneal washings
Tumour involves one or both fallopian tube(s) with
peritoneal implants outside the pelvis and/or
positive regional lymph nodes
Microscopic peritoneal metastasis outside the pelvis
Macroscopic peritoneal metastasis outside the
pelvis 2 cm or less in greatest dimension
Peritoneal metastasis more than 2 cm in greatest
dimension and/or positive regional lymph nodes
IV
Distant metastasis (excludes peritoneal metastasis)
N – Regional Lymph Nodes 3
NX
Regional lymph nodes cannot be assessed
N0
No regional lymph node metastasis
N1
Regional lymph node metastasis
M – Distant Metastasis
MX
Distant metastasis cannot be assessed
M0
No distant metastasis
M1
Distant metastasis
Stage Grouping
Stage 0
Stage IA
Stage IB
Stage IC
Stage IIA
Stage IIB
Stage IIC
Stage IIIA
Stage IIIB
Stage IIIC
Stage IV
Tis
T1a
T1b
T1c
T2a
T2b
T2c
T3a
T3b
T3c
Any T
Any T
N0
N0
N0
N0
N0
N0
N0
N0
N0
N0
N1
Any N
M0
M0
M0
M0
M0
M0
M0
M0
M0
M0
M0
M1
__________
{51,2976}.
2
A help desk for specific questions about the TNM classification is available at http://tnm.uicc.org.
3
The regional lymph nodes are the hypogastric (obturator), common iliac, external iliac, lateral sacral, para-aortic, and inguinal nodes.
1
205
Tumours of the fallopian tube
Malignant epithelial tumours
Definition
A malignant epithelial tumour of the tubal
mucosa, usually with glandular differentiation. In order to be considered a primary carcinoma of the fallopian tube, the
tumour must be located macroscopically
within the tube or its fimbriated end, and
the uterus and ovary must either not contain carcinoma or, if they do, it must be
clearly different from the fallopian tube
lesion.
ICD-O codes
Serous adenocarcinoma
Mucinous adenocarcinoma
Endometrioid adenocarcinoma
Clear cell adenocarcinoma
Transitional cell carcinoma
Undifferentiated carcinoma
8441/3
8480/3
8380/3
8310/3
8120/3
8020/3
Epidemiology
Primary fallopian tube carcinomas are
rare, amounting to 0.3-1.1% of gynaecological malignancies {158}. The risk factors appear similar to those of epithelial
ovarian cancer. Adenocarcinoma is the
most frequent tumour of the fallopian
tube {2566}.
I. Alvarado-Cabrero
A. Cheung
R. Caduff
tumour may protrude through the fimbriated end. On the sectioned surface the
adenocarcinoma usually consists of soft,
grey-brown, villous or polypoid tissue.
Tumour spread and staging
The tumour spread is very similar to that
of ovarian carcinoma and involves adjacent organs, the peritoneum and region al lymph nodes. Involvement of the adjacent ovary may make it difficult to determine whether the tumour is primary in the
tube or ovary. When the origin remains
unclear, the tumour is classified as tuboovarian carcinoma {1256}.
Surgical staging is performed according
to the FIGO classification system
{51,2976}.
Histopathology
All carcinoma subtypes documented in
the ovaries have been identified in the
fallopian tube. Serous carcinoma is the
most common cellular subtype. In one
series of 151 cases, 80% of the tumours
were serous {158}. In other large series,
about half of these carcinomas were
serous, one-fourth endometrioid, onefifth transitional cell or undifferentiated
and the remainder of other cell types
{75}.
Macroscopy
On macroscopic examination, the tube
shows abnormal dilatation or nodular
thickening resembling a hydrosalpinx or
haematosalpinx and contains a dominant localized tumour mass. When found
in the proximal part of the tube, the
Most serous carcinomas of the tube are
invasive tumours with a high histological
grade. In one series 50% of the cases
were grade 3 {75}. Occasional serous
A
B
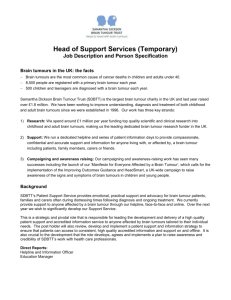
Serous adenocarcinoma
Fig. 3.01 Carcinoma of the fallopian tube. The sec tioned surface shows a dilated fallopian tube filled
with papillary tumour exhibiting foci of haemorrhage.
carcinomas have an extensive inflammatory cell infiltration that may simulate a
salpingitis of non-tuberculous type {472}.
Mucinous adenocarcinoma
These tumours are extremely rare and
often are associated with other mucinous
neoplasms of the female genital tract
{2617}. Reported cases have been predominantly in situ mucinous carcinomas
{2450}. A case of synchronous, trifocal
mucinous papillary adenocarcinoma
involving the uterine cervix and both fallopian tubes has been reported {1316}.
We are only aware of a single case of an
invasive mucinous adenocarcinoma. The
histological appearance of these
tumours resembles that of ovarian mucinous carcinomas, and goblet cells may
be prominent.
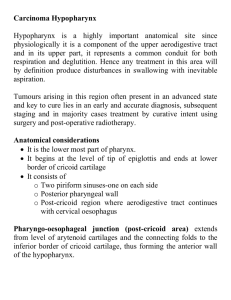
C
Fig. 3.02 Serous papillary adenocarcinoma of the fallopian tube. A Pedunculated papillary tumour arises from the wall of the tube. There is no invasion of the muscular
wall. B Note the well differentiated papillary fronds. C This papillary tumour shows prominent budding from the primary papillae. The nuclei show stratification and atypia.
206 Tumours of the fallopian tube and uterine ligaments
Endometrioid adenocarcinoma
Endometrioid carcinomas of the tube are
characteristically non-invasive or only
superficially invasive and have a generally favourable prognosis {1985}. The
typical variant is the most common form
of endometrioid carcinoma encountered
in the tube. By definition these tumours
closely resemble their uterine counterparts. Endometrioid carcinomas with a
prominent spindle-shaped epithelial cell
component {2942} or with the glands
lined exclusively by oxyphilic cells {2258}
also occur in the tube. An unusual form
of endometrioid carcinoma resembling
the patterns seen in the wolffian adnexal
tumour has been found relatively often in
the fallopian tube {641,1985}. These
tumours are characterized by a prominent pattern of small, closely packed
cells punctured by numerous glandular
spaces, a large number of which contain
a dense colloid-like secretion. The finding of areas with the typical appearance
of endometrioid carcinoma enables one
to make the correct diagnosis.
Fig. 3.03 Undifferentiated carcinoma of the fallopian tube. Note the sheets of cells with scattered tumour
giant cells.
quency of transitional cell carcinoma of
the fallopian tube in previous reports has
varied from 11-43% {75,2974}. Transitional cell metaplasia of the epithelium
has been suggested as a possible
source of tubal carcinoma of the same
cell type {750}.
Clear cell adenocarcinoma
Undifferentiated carcinoma
These neoplasms constitute 2-10% of all
fallopian tube carcinomas {75,1181a,
3031}. The majority of the reported cases
have shown a tubulocystic pattern varying from flattened cuboidal epithelium to
an irregular pattern with prominent hobnail and clear cells. A papillary pattern
featuring the hobnail type of epithelium
lining fibrovascular stalks has also been
described {3031}.
Transitional cell carcinoma
These carcinomas are rare in the female
genital tract but occur relatively more
often than in the ovary {2676}. The fre-
A
These carcinomas fail to show evidence
of either glandular or squamous differentiation. The tumour displays a diffuse
growth pattern composed of sheets of
small cells resembling those of small cell
carcinoma of the lung. These densely
cellular tumours may have a relatively
conspicuous myxoid matrix. Some
tumours have large epithelial cells
arranged in nests surrounded by a dense
lymphocytic infiltrate resembling a lymphoepithelioma-like carcinoma. Extensive tumours areas consisting predominantly of multinucleated giant cells may
also be present {75}.
B
Hormone-producing carcinoma
Ectopic beta-human chorionic gonadotropin (β-hCG) production has been
reported in two women with serous or
undifferentiated carcinoma of the tube
{75,399}. Each of the tumours contained
syncytiotrophoblast-like cells, many of
which stained positively for β-hCG.
Unusual reported cases include a reninproducing tumour {3234} and an alphafetoprotein producing carcinoma that
had a hepatoid appearance {111}.
Miscellaneous epithelial tumours
Rare examples of unusual neoplasms
arising in the tube include cases of squamous cell {290,470,1747}, adenosquamous, glassy cell {75,1191} and lymphoepithelioma-like carcinoma {75}.
Genetic susceptibility
The discovery of the BRCA1 cancer predisposition gene in 1994 and the BRCA2
C
Fig. 3.04 Carcinoma of the fallopian tube. A The poorly differentiated tumour shows papillary fronds and gland-like spaces. B Note the syncytiotrophoblast-like multinucleated tumour giant cells in the centre. C The syncytiotrophoblast-like giant cells stain positively for beta-human chorionic gonadotropin (β-hCG).
Tumours of the fallopian tube 207
A
B
Fig. 3.05 Endometrioid carcinoma of the fallopian tube. A Closely packed tubules of endometrioid carcinoma are present adjacent to a focus of endometriosis composed of larger glands present on the left. B The tumour forms closely packed glands lined by pseudostratified epithelium.
cancer predisposition gene in 1995 has
allowed the identification of a group of
women who are at a greatly increased
risk of developing breast and ovarian
cancer {8,499}. Two previous series in
which 5% and 11% respectively of
patients with tubal cancer also had
breast carcinoma suggest an association
between breast cancer and tubal carcinoma {75,2225}. Recently, several highrisk "breast-ovarian cancer families" with
BRCA1 mutations and fallopian tube
cancer have been reported. Additionally,
a family history of fallopian tube cancer
was found to be predictive of the presence of a BRCA1 mutation in a panel of
26 Canadian "breast-ovarian cancer families" {2939}. A slightly increased risk of
ovarian cancer and of early-onset breast
cancer was found in the first-degree relatives of the fallopian tube cancer cases
{144}. Thus, fallopian tube carcinoma
should be considered to be a clinical
component of the hereditary breast-ovarian cancer syndrome and may be associated with BRCA1 and BRCA2 mutations. See Chapter 8.
Prognosis and predictive factors
The surgical stage is an independent
prognostic factor {75,158} and is critical
for determining whether adjuvant therapy
is appropriate. Stage I carcinomas that
occur in the tubal fimbriae appear to have
a worse prognosis than stage I tubal carcinomas that are nonfimbrial {74}.
Fig. 3.06 Lymphoepithelial-like carcinoma. The tumour is composed of pale
epithelial cells with large vesicular nuclei and prominent nucleoli. Note the lymphocytic infiltration.
208 Tumours of the fallopian tube and uterine ligaments
Borderline epithelial tumours
Borderline epithelial tumours of the fallopian tube are rare and include cases of
serous, mucinous and endometrioid
types {74}. Borderline serous tumours
involve the tube, including its fimbriated
portion, and have histological features
similar to those of the ovary {74,1421,
3257}. Mucinous tumours are sometimes
associated with mucinous metaplasia of
the fallopian tube or the Peutz-Jeghers
syndrome {1806,2617}. Patients that
have multiple organ involvement or
pseudomyxoma peritonei may have a
metastatic lesion to the tube, and in all
cases the appendix needs to be ruled
out as a source.
Fig. 3.07 Serous borderline tumour. The tumour consists of papillae with connective tissue cores lined by epithelium showing cellular stratification and tufting,
resembling its ovarian counterpart.
Two examples of adenofibroma of borderline malignancy have been reported
{74,3257}. One of the tumours appeared
in a pregnant woman and on ultrasound
was interpreted as an ectopic pregnancy; the other was detected incidentally
during an elective tubal ligation. Both
neoplasms were located at the fimbriated end of the fallopian tube. One tumour
was of serous type and the other
endometrioid.
Although relatively few cases of tubal
borderline tumours have had long term
follow up, the prognosis appears
favourable, and it has been suggested
that they can be managed conservatively {3257}.
Carcinoma in situ
Rare cases of tubal intraepithelial carcinoma have been reported, and one of
these occurred after tamoxifen therapy of
breast carcinoma {2747}. With the
exception of one case in which a small
papillary tumour was found {1875}, the
tumours are not detectable on macroscopic examination.
They are characterized by replacement
of the tubal epithelium by malignant glandular epithelial cells with pleomorphic
nuclei {178,2835}. Florid epithelial proliferation, sometimes even with a cribriform
or sieve-like pattern, may occur in association with salpingitis and should not be
mistaken for carcinoma in situ {472}.
Benign epithelial tumours
Polypoid adenofibromas, papillomas,
benign serous cystadenoma and
endometrioid tumours are rarely found in
the fallopian tube, including the fimbria
{74,1615}. They may be complicated by
torsion, especially during pregnancy.
Papilloma and cystadenoma
Serous papilloma and cystadenoma are
uncommon lesions of the fallopian tube.
Papillomas may be intramural or involve
the fimbriated end {74}. Papillomas typically are loosely attached to the tubal
mucosa and consist of delicate branching fibrovascular stalks lined by epithelial
cells that are indifferent in appearance or
resemble those of the fallopian tube lining. The lesion may cause tubal obstruc-
Fig. 3.08 Metaplastic papillary tumour. The tumour is composed of variably sized papillae showing a proliferation of atypical epithelial cells with cellular budding and abundant eosinophilic cytoplasm.
tion {1012,1407}. Cystadenomas are similar but lack papillary features {74}.
Mucinous cystadenomas also have been
reported {2617}.
Adenofibroma and
cystadenofibroma
Fallopian tube adenofibromas and cystadenofibromas are rare. About fifteen
examples of these tumours have been
documented {74,3257}. The age range is
from the third to the eight decade with a
mean age of 49 years. Most women are
asymptomatic, and the majority of the
tumours are incidental findings at the
time of an operation for another gynaecological disorder {3257}. The neoplasm
presents as a round, solitary mass (average 0.5-3 cm) that is either intraluminal or
attached to the fimbriated end or the
serosal surface and may have a smooth
or papillary surface. In one case the
tumour was bilateral {451}.
Histologically, two components are present, a connective tissue stroma without
nuclear pleomorphism or mitoses and
papillary structures on the surface or
tubal structures lined by epithelial cells.
The epithelial cell type has been serous
in most of the cases but occasionally
may be endometrioid {647}.
Metaplastic papillary tumour
Metaplastic papillary tumour is an
uncommon lesion that typically occurs as
an incidental histological finding in segments of fallopian tube removed during
the postpartum period for sterilization
{187,1425,2504}. Only rare lesions occur
in women who were not recently pregnant. The intraluminal tumour usually
involves part of the mucosal circumference and is composed of variable sized
papillae covered by atypical epithelial
cells that superficially resemble a serous
borderline tumour. The epithelial lining
shows cellular budding and the presence of abundant eosinophilic cytoplasm
in most of the tumour cells. Some of the
cells may contain intracellular mucin,
and extracelluar mucin may be abundant. Mitotic figures are rarely observed.
Endometrioid polyp
Endometrial (adenomatous) polyps
occur in the interstitial portion of the fallopian tube {1170,1180}. They are commonly found in radiographic studies of
infertile patients. They may obstruct the
lumen and result in infertility or tubal
pregnancy. They are often attached to
the tubal epithelium by a broad base
and, thus, macroscopically resemble
intrauterine endometrial polyps. They
may be occasionally associated with
ectopic endometrial epithelium elsewhere in the tube {342}.
Tumour-like epithelial lesions
Definition
Proliferations of the tubal mucosa that
simulate neoplasms.
Tubal epithelial hyperplasia
Pseudocarcinomatous hyperplasia in
chronic salpingitis may mimic adenocarTumours of the fallopian tube 209
incidental finding {659,1591}. Rarely,
endosalpingiosis can present clinically
as a cystic mass and can be confused
with a neoplasm on macroscopic examination {518a}.
Mixed epithelial and
mesenchymal tumours
Fig. 3.09 Prominent mucosal hyperplasia. A glandular proliferation producing a cribriform pattern simulates a neoplastic process within the plicae of the
fallopian tube.
cinoma histologically because of the
pseudoglandular and cribriform permeation of the tubal wall by hyperplastic
epithelium and the florid mesothelial
hyperplasia {472}. The typically young
age of the patients, the presence of
marked chronic inflammation, the
absence of a macroscopically detected
tumour or solid epithelial proliferation, the
mildness of the nuclear atypia and the
paucity of mitotic figures facilitate the differential diagnosis.
Recently, atypical hyperplasia of the fallopian tube has been observed in
patients on tamoxifen therapy for breast
cancer {2244}.
Salpingitis isthmica nodosa
Salpingitis isthmica nodosa is a manifestation of tubal diverticulosis and is associated with female infertility and ectopic
pregnancy {1064}. These nodules in the
isthmus are composed of hypertrophic
myosalpinx and glandular spaces lined
by tubal epithelium.
Endosalpingiosis
Endosalpingiosis is the benign transformation of the mesothelium into tubal
epithelium with ciliated and secretory
cells. Psammoma bodies and atypical
changes may be found {2919}.
Endosalpingiosis is distinguished from
endometriosis by the absence of
endometrial stroma since tubal type
epithelium can also occur occasionally in
endometriosis. Endosalpingiosis occurs
in the peritoneum and may involve the
serosal surfaces of the uterus and its
adnexa.
Endosalpingiosis may either present as
pelvic pain or may be discovered as an
Definition
Neoplasms composed of an admixture of
neoplastic epithelial and mesenchymal
elements. Each of these components
may be either benign or malignant.
ICD-O codes
Malignant müllerian mixed tumour 8950/3
Adenosarcoma
8933/3
Malignant müllerian mixed tumour
As a group, these malignancies are
uncommon. The fallopian tube is the
least common site for malignant müllerian mixed tumours in the female genital
system, accounting for less than 4% of
the reported cases {1124}. Patients are
almost always postmenopausal (mean
age, 57 years) and usually present with
abdominal pain, atypical genital bleeding or abdominal distension {1124,1284}.
The histological appearance of these
tumours resembles that of ovarian malignant müllerian mixed tumour. The prognosis is poor {1124,1284,3079}.
Fig. 3.10 Malignant müllerian mixed tumour of fallopian tube. The fallopian tube is distended and distorted by a multinodular tumour mass that has
extended through the serosa.
Choriocarcinoma
Tubal choriocarcinomas account for
approximately 4% of all choriocarcinomas {660}. Most of the cases are discovered by chance during an ectopic pregnancy, but about 40% present with an
enlarging adnexal mass {2078}.
Histological examination shows typical
features of gestational choriocarcinoma.
In the older literature before the advent of
modern chemotherapy, choriocarcinomas associated with ectopic pregnancy
were frequently very aggressive, and
75% showed metastases at the time of
diagnosis. The response to modern
chemotherapy generally has been
encouraging {1717,1953}.
Placental site trophoblastic
tumour
Adenosarcoma
This tumour is exceedingly uncommon.
Only one well documented case that
arose in the fimbriated end of the tube
and recurred on the pelvic wall has been
reported {1036}. Another example of a
tubal tumour of this type was characterized by marked adenoacanthotic atypia
of its epithelial component {2605}.
This neoplasm is composed predominantly of intermediate trophoblast. It is
generally benign but occasionally may
be highly malignant {1540}. To date, only
one case of tubal placental site trophoblastic tumour has been reported
{2810}.
Hydatidiform mole
Gestational trophoblastic
disease
Definition
A heterogeneous group of gestational
and neoplastic conditions arising from
trophoblast, including molar gestations
and trophoblastic tumours.
ICD-O codes
Choriocarcinoma
9100/3
Placental site trophoblastic tumour 9104/1
Hydatidiform mole
9100/0
210 Tumours of the fallopian tube and uterine ligaments
Approximately thirty tubal hydatidiform
moles have been reported {1999}; however, only four valid examples of this
lesion were accepted in 1981 {2078}.
Those authors concluded that the
remaining "moles" were actually ectopic
pregnancies with villous hydrops. This
tumour usually occurs as an isolated
growth, but it may be associated with an
intrauterine pregnancy {1048}. The histological appearance may be that of a
complete, partial or invasive mole with clear
A
B
Fig. 3.11 Adenomatoid tumour. A The wall of the fallopian tube contains a solid mass. Note the uninvolved cross section of the tube on the right. B Variably shaped
small cystic spaces and tubule-like structures proliferate in the wall of the tube. The mucosa is on the right.
evidence of trophoblastic proliferation in
addition to hydropic swelling of the villi.
Placental site nodule
Placental site nodule is an asymptomatic
non-neoplastic proliferation of intermediate
trophoblast from a previous gestation that
failed to involute. This lesion has recently
been reported to occur at the site of an
ectopic gestation; two were located in the
fallopian tube and one in the broad ligament
in direct contact with the tube {391,1514}.
Other tumours
Adenomatoid tumour
ICD-O code
9054/0
The adenomatoid tumour is the most frequent type of benign tubal tumour and
usually is found as an incidental finding in
a middle-aged or elderly woman {1290}.
It typically appears as a grey, white or yellow nodular swelling measuring 1-2 cm in
diameter located beneath the tubal
serosa The tumour may be large enough
to displace the tubal lumen eccentrically
{2787}. Rare examples are bilateral
{3230}. It originates from the mesothelium
and is composed of gland-like structures
lined by flat to cuboidal cells {2787}.
Germ cell tumours
To date only about 50 teratomas of the tube
have been reported {1242,3051, 3189}.
Many of them were found incidentally,
measuring 1-2 cm in diameter, and none
has been diagnosed preoperatively. The
patients have the risk factors for ectopic
pregnancy such as prior salpingitis and
tubal occlusion {1953}. A malignant mixed
germ cell tumour has been reported {1652}.
Soft tissue tumours
Primary sarcomas of the fallopian tube
are exceedingly rare; approximately 37
cases have been reported in the literature in more than 100 years {1322}. The
clinical signs and symptoms are usually
non-specific and include lower abdominal pain and pelvic pressure. The age at
diagnosis varies from 21-70 years with a
median of 47 years.
Leiomyosarcoma is the most common
type and may arise from the tube or
broad ligament {1322}. Other reported
fallopian tube or broad ligament malignancies include chondrosarcoma {2245},
embryonal rhabdomyosarcoma {361},
myxoid liposarcoma {2708} and Ewing
tumour {1692}. The prognosis is poor,
although several long-term survivors
have been reported {1322}.
Malignant lymphoma and
leukaemia
Tubal involvement by lymphoma is rare
and is associated almost invariably with
simultaneous involvement of the ipsilateral ovary {2119}. In one large series more
than 25% of patients with ovarian lymphoma had tubal involvement, most often
by Burkitt or Burkitt-like (small noncleaved cell) lymphoma or diffuse largecell lymphoma {2119}. One example of
an apparent primary malignant lymphoma of the fallopian tube has been
observed {2605}. The tube may also be
infiltrated in cases of leukaemia {428}.
Secondary tumours
Metastatic tumours involving the tube
usually are the result of secondary
spread from carcinomas of the ovary or
endometrium {3145}. In most cases, the
spread is by direct extension. In one
study 89% of secondary carcinomas in
the tube were of ovarian origin, and the
remainder originated in the endometrium. Blood-borne metastases from breast
carcinomas or other extrapelvic tumours
may also occur {862,3145}. The authors
are aware of a case of adenocarcinoma
of the gallbladder metastatic to the fallopian tube {862}.
Tumours of the fallopian tube 211
Tumours of the uterine ligaments
Definition
Benign and malignant tumours that arise
in the broad ligament and other uterine
ligaments.
ICD-O codes
Serous adenocarcinoma
Endometrioid adenocarcinoma
Mucinous adenocarcinoma
Clear cell adenocarcinoma
Wolffian adnexal tumour
Ependymoma
Papillary cystadenoma (with
von Hippel-Lindau disease)
Adenosarcoma
8460/3
8380/3
8480/3
8310/3
9110/1
9391/3
8450/0
8933/3
Carcinomas
Less than 20 cases have been reported,
of which most were of serous, endometrioid and clear cell types {127a,604a,
715a,1481a,1850a,2402a,2775a,2912a}.
An association with endometriosis was
observed in some endometrioid and clear
cell carcinomas. The age of the patients
ranged from 28-70 years. The tumours
were cystic, solid or mixed, and their diameter ranged from 4.5-13 cm. All carcinomas were unilateral, but some had spread
beyond the broad ligament. Due to the
small number of cases and limited followup in many of the cases, the prognosis of
these tumours cannot be established.
Epithelial tumours of müllerian type
Definition
Epithelial tumours of müllerian type are
the most frequent neoplasms of the
broad and other ligaments {2919}. In
general, tumours of every müllerian cell
type and of every degree of malignancy
can occur in this location but are infrequent compared to their occurrence in
the ovary. The criteria for malignancy and
for the borderline category are the same
as described for müllerian type epithelial
tumours occurring in the ovary and the
peritoneum.
Borderline tumours
More than 30 cases, mostly serous cystic
tumours (age range 19-67 years; mean
age 33 years) have been re p o rt e d
{73,127,434,606,740,1341,1702,2626}.
One mucinous tumour has been reported
{1342}. The tumours measured 1-13 cm
in greatest diameter, were unilateral,
clearly separated from the ovary and
confined to the broad ligament.
Benign tumours
Serous cystadenoma is the most common
type {962}. As in the ovary, the distinction
S.F. Lax
R. Vang
F.A. Tavassoli
Fig. 3.12 Wolffian adnexal tumour. The tumour is
circumscribed and composed of closely packed
tubules.
from non-neoplastic serous cysts is ill
defined. A suggested distinction is that
serous cystadenomas have a thick wall
composed of cellular stroma resembling
ovarian stroma and lack folds and plicae
in contrast to the histology of serous cysts
{1236,1335}. Several Brenner tumours
ranging from 1-16 cm in diameter have
occurred {1120}, and they may be associated with serous or mucinous cystadenomas {169,1628,2302,3040}.
Wolffian adnexal tumour
Definition
A tumour of presumptive wolffian origin
characterized by a variety of epithelial
patterns.
Synonyms
Retiform wolffian adenoma, retiform wolffian adenocarcinoma.
Fig. 3.13 Wolffian adnexal tumour. The tumour is composed of crowded tubules.
212 Tumours of the fallopian tube and uterine ligaments
Sites of involvement
Wolffian tumours occur mainly within the
leaves of the broad ligament but may
appear as pedunculated lesions arising
from it. Less than 50 examples have
been described that are predominantely
located within the area where mesonephric remnants are distributed. They
occur mainly in the broad ligament but
also in the mesosalpinx, the serosa of the
fallopian tube, the ovary and the
re t roperitoneum {637,670,682,1400,
2653,2877,2926,3212}.
Clinical features
Patients range in age from 15-81 years,
and most present with a unilateral adnexal mass. Ultrasound studies may show
an ill defined mass {637}.
cytoplasm and round to spindle-shaped,
uniform nuclei. Sieve-like areas display
clusters of variably sized cysts lined by
attenuated cells. Most cases do not show
atypia or mitotic figures.
Macroscopy
These predominantly solid tumours
range from 0.5-18 cm in diameter. The
sectioned surface may contain variably
sized cysts and is yellow-tan to greywhite {2877}. The tumour is firm to rubbery and occasionally may have areas of
haemorrhage and necrosis.
Immunoprofile
The tumour cells are positive for most
cytokeratins and vimentin and are often
positive for calretinin (91%), inhibin
(68%) and CD10 {2110}. They are usual ly negative for epithelial membrane antigen, estrogen receptor (ER) and progesterone receptor (PR) and are negative for
cytokeratin 20, 34betaE12 and glutathione S-transferase {682,2926}.
Tumour spread and staging
Tumour implants may be present at the
time of diagnosis and indicate an
aggressive tumour {637,2653}.
Histopathology
The tumour shows a variable admixture
of diffuse, solid and sieve-like cystic
areas, with the solid pattern dominating
in the majority of cases. The diffuse, solid
areas show a compact proliferation of
ovoid to spindle-shaped cells reflecting
closed tubules bound by a basement
membrane and separated by variable
amounts of fibrous stroma or none at all.
The round to ovoid nuclei may show
indentations. The hollow tubules have a
retiform or sertoliform appearance. When
the closed tubules dominate, the lesion
resembles a mesenchymal tumour; a
PAS or reticulin stain helps unmask the
tubular pattern. The cells lining the
tubules are cuboidal to low columnar
with a minimal amount of eosinophilic
A
Cytometry
The ploidy of a metastatic tumour was
assessed and found to be diploid {2653}.
Electron microscopy
At the ultrastructural level, the tubules
are surrounded by basal lamina and
lined by cells with complex interdigitations, desmosomes and/or tight junctions
and a few microvilli along the luminal border; no cilia are identifiable {670}. The
cytoplasmic organelles are not distinctive and include lysosomes, a small
amount of smooth endoplasmic reticulum
and a few lipid droplets.
Differential diagnosis
The main tumours in the differential diagnosis are Sertoli cell tumour, SertoliLeydig cell tumour, and well differentiated endometrioid carcinoma. The presence of a sieve-like pattern and the
absence of Leydig cells help distinguish
wolffian tumours from all these lesions.
The absence of immunoreactivity with
either ER or PR also would distinguish
wolffian tumours from well differentiated
endometrioid carcinomas; the latter are
invariably positive for ER and PR; however, positive immunostaining does not
exclude the possibility of a wolffian
tumour {682}.
Prognosis and predictive factors
The tumour stage as well as cytological
atypia and frequent mitotic figures are
important predictors of aggressive
behaviour. Careful follow-up of all women
with wolffian adnexal tumours is prudent
{637,2653}.
Most wolffian adnexal tumours are
benign and adequately treated by unilateral salpingo-oophorectomy. About 10%
either recur or metastasize. Recurrences
and metastases to the lungs and liver
have been reported within 1 year or as
late as 8 years after diagnosis
{637,2653}. The metastatic tumour often
has more atypia compared to the primary. Some aggressive tumours have
had no significant atypia or mitotic activity in either the primary or the metastatic
lesion {2653}.
Ependymoma
Definition
Tumours closely resembling neoplasms
of the central nervous system that show
ependymal differentiation.
B
Fig. 3.14 Wolffian adnexal tumour. A The pattern of closely packed tubules simulates a Sertoli cell tumour. B Reticulin stain accentuates the tubular pattern.
Tumours of the uterine ligaments 213
A
B
Fig. 3.15 Papillary cystadenoma associated with VHL. A A cystic lesion with multiple papillary excrescences is characteristic. B The papillae are lined by a single
layer of cuboidal to low columnar cells with bland nuclei; there is no atypia or notable mitotic activity.
Localization
Only four ependymomas have been
described in the uterine ligaments, three
in the broad ligament and one in the
uterosacral ligament {208,727,1068}.
Clinical features
Patients were 13-48 years of age with a
mean of 38 years and presented with a
mass associated with lower quadrant
tenderness.
Macroscopy
The tumours are solid or multicystic, soft
in consistency and vary from 1 cm to
massive in size. The sectioned surface
shows haemorrhage and necrosis in the
larger tumours.
Histopathology
The lesions are characterized by papillae
lined by flat to columnar ciliated cells
with central to apical, round to elongated
nuclei that protrude into cystic spaces. In
more cellular solid areas, the cells form
true perivascular ependymal rosettes
and pseudorosettes. Mitotic figures may
be few or numerous. A few psammoma
bodies and small nodules of mature cartilage may be present.
At the ultrastructural level the cells have
cilia, blepharoplasts and intermediate filaments {208,727}.
Differential diagnosis
The papillary architecture and psammoma bodies closely resemble serous papillary carcinoma. The ependymal cells
are immunoreactive for glial fibrillary
acidic protein, however, helping to distin-
guish the two lesions. The cells are also
positive for cytokeratin and vimentin.
Prognosis and predictive factors
These are malignant tumours capable of
spread beyond the ligaments {208,727,
1068}. Two of the reported cases had
spread beyond the broad or uterosacral
ligament at presentation, whilst a third
had two recurrences over a 24 year period.
Papillary cystadenoma associated
with von Hippel-Lindau disease
Definition
A benign tumour of mesonephric origin
that occurs in women with von HippelLindau (VHL) disease.
Clinical features
Reported in women 20-46 years of age,
one case was not only bilateral but also
the first manifestation of the disease; the
remaining three were unilateral {939,949,
988,1505}.
Imaging
Ultrasonography shows a sonolucent
mass containing an echogenic region
{1505}. By computed tomography the
lesion appears as an adnexal mass with
both water attenuation and soft tissue
attenuation areas and curvilinear calcification {939}.
Macroscopy
The tumours are up to 4 cm in diameter
and cystic with polypoid papillary protrusions.
214 Tumours of the fallopian tube and uterine ligaments
Histopathology
Histologically, the lesion is characterized
by a complex, arborizing, papillary architecture. Generally, a single layer of nonciliated cuboidal cells with vacuolated to
lightly eosinophilic cytoplasm and bland
round nuclei line the papillae {939,
949,988,1505}. The papillary stalks vary
from cellular to oedematous and hyalinized. Atypia and necrosis are absent,
and mitotic figures are rare to absent.
The cells contain glycogen but not mucinous material. A prominent basement
membrane is evident beneath the epithelial cells. The cyst wall is fibrous and may
have small bundles of smooth muscle or
focal calcification.
Genetic susceptibility
VHL disease is an autosomal dominant
disorder with inherited susceptibility to a
variety of benign and malignant neoplasms including haemangioblastomas
of the retina and central nervous system,
renal cell carcinoma, pancreatic microcystic adenomas and a variety of other
cysts, adenomas and congenital abnormalities. Papillary cystadenomas of
mesonephric origin are rare VHL-associated lesions that occur more often in the
epididymis but also rarely in the
retroperitoneum and broad ligament in
women; only four examples of the latter
have been documented.
Genetics
The tumour suppressor gene responsible
for VHL disease has been mapped to
chromosome 3p25 and subsequently
identified. Genetic studies on a variety of
cases have been described. Cases
reported in the uterosacral and broad ligaments have occurred in women under
50 years of age {48}.
Macroscopy
The lesions form a cystic mass.
Histopathology
The inner lining consists of benign
endometrial glands and endometrial stroma with an arrangement resembling
endometrium. The outer layer of the cyst
wall consists of thickened smooth muscle bundles appearing similar to
myometrium.
Immunoprofile
Lesions may express ER and PR in the
endometrial and myometrial components.
Fig. 3.16 Uterus-like mass. The cystic mass resembles the uterus and is composed of a layer of
endometrium consisting of glands and stroma
overlying smooth muscle.
tumours from patients with VHL disease
have demonstrated loss of heterozygosi ty at chromosome 3p within the VHL
gene region. Two papillary cystadenomas (one from broad ligament, the other
retroperitoneal) were studied by polymerase chain reaction and single-strand
conformation polymorphism with four
polymorphic markers spanning the VHL
gene locus (D3S1038, D3S1110,
D3S2452, 104/105) {2640}. Both tumours
showed loss of heterozygosity at one or
more of the markers providing evidence
that somatic loss of the VHL gene is
responsible for the genesis of these papillary cystadenomas {2640}.
Prognosis and predictive features
All lesions reported so far have been
benign.
Uterus-like mass
Definition
A tumour-like lesion composed of
endometrial tissue and smooth muscle,
histologically resembling the uterus.
Clinical features
Patients present with a pelvic mass. Most
arise within the ovary, but extraovarian
Differential diagnosis
"Endomyometriosis" is likely the same
entity as uterine-like mass. "Endometriosis with smooth muscle metaplasia" is
histologically related to uterus-like mass,
if not the same. Adenomyoma is distinguished from uterus-like mass by lacking
the uterus-like organization. A uterus-like
mass lacks the classic features of
endometrioid carcinoma and extrauterine adenosarcoma.
Genetics
A deletion on the short arm of chromosome 2 has been identified.
Prognosis and predictive factors
Benign behaviour would be expected.
Adenosarcoma
A single case of a high grade adenosarcoma arising from the round ligament
was reported {1396}.
Mesenchymal tumours
Mesenchymal tumours originating from
the broad and other ligaments are rare.
Almost any kind of malignant or benign
mesenchymal tumour may occur.
Malignant tumours
Sarcomas are extremely rare, the most
frequent being leiomyosarcoma, {465,
689,1192,1608,1630,2210} for which the
same diagnostic criteria should be
applied as for its uterine counterpart.
Approximately 10 cases have been
reported, and the prognosis is poor.
Other sarcomas re p o rted include
endometrioid stromal sarcoma arising in
endometriosis {2220}, embryonal rhabdomyosarcoma (occurring in children
and having a poor prognosis) {991},
alveolar rhabdomyosarcoma (in an
adult) {558}, mixed mesenchymal sarcoma {2822}, myxoid liposarcoma {2708}
and alveolar soft part sarcoma {2017}.
Benign tumours
The most common tumours are leiomyomas and lipomas {340,962}. It is often
difficult to determine the site of origin of
leiomyomas within the broad ligament. It
has been suggested that leiomyomas
be designated as ligamentous only if
clearly separated from the myometrium.
A leiomyoma of the broad ligament was
imitated by Dracunculosis {70}.
Lipomas are usually small and located
within the mesosalpinx {847} and may
be mixed with leiomyomas. Cases of
other mesenchymal tumours of the
broad and round ligament have been
reported including two benign mesenchymomas {2069}, neuro f i b ro m a s ,
schwannomas {246,1047,2910} and a
fibroma with heterotopic bone formation
{2899}. Massive ascites and bilateral
pleural effusion has been described in
association with broad ligament leiomyoma and with paraovarian fibro m a
(pseudo-Meigs syndrome) {357,364,
992}.
Miscellaneous tumours
A variety of miscellaneous tumours have
been described. Many of them are of
ovarian type, such as germ cell and sex
c o rd - s t romal tumours. Although the
question of origin from accessory ovarian tissue may be raised, in most cases
no pre-existing ovarian tissue is identified. Mature teratomas, in particular dermoid cysts, occurred bilaterally within
accessory ovaries of the broad ligament
{941}. A dermoid cyst containing pituitary tissue occurred in the uterosacral
ligament {1179}. A yolk sac tumour was
found in the broad ligament {1270}.
Other reported cases included granulosa cell tumours, but some of these
were in fact wolffian adnexal tumours
{962,1427,2347,2997}. Several broad
ligament tumours of the thecoma-fibroma group, some of which had estroTumours of the uterine ligaments 215
genic effects, have been re p o rt e d .
Several cases of steroid cell tumour with
possible origin from accessory ovaries
or adrenocortical remnants have been
described {38,2462,2538,2996}. Three
phaeochromocytomas, two that caused
hypertension and elevated vanillylmandelic acid levels and one non-functional
tumour {54,58,122}, and a carcinoid
{1325} have been described.
Secondary tumours
A
B
Fig. 3.17 Cotyledonoid dissecting leiomyoma. A Viewed posteriorly, an exophytic, congested, multinodular
mass resembling placental tissue arises from the right cornual region of the uterus and extends laterally.
B In the extrauterine component, a cotyledonoid process composed of smooth muscle is covered by connective tissue containing congested vessels.
216 Tumours of the fallopian tube and uterine ligaments
Any type of malignant tumour originating from the uterus, its adnexae, other
sites within the abdomen or from any
other organ of the body may spread to
the uterine ligaments by direct extension, lymphatics or blood vessels. In
particular, intravenous leiomyomatosis
{523, 1122,1940,2051}, diffuse uterine
leiomyomatosis {2394} and endometrial
stromal sarcoma from the uterus may
present as a mass within the broad ligament. Although it is far more common to
spread to the broad ligament from the
uterus, intravenous leiomyoma may
exceptionally arise in the broad ligament {1154}. Cotyledonoid dissecting
leiomyoma, the Sternberg tumour, is an
unusual benign uterine smooth muscle
neoplasm that spreads to the broad ligament {2470}. It is characterized by dissecting growth within the uterus, degenerative changes and a rich vascular
component but does not have intravascular extension.