This article appeared in a journal published by Elsevier. The attached
copy is furnished to the author for internal non-commercial research
and education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling or
licensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of the
article (e.g. in Word or Tex form) to their personal website or
institutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies are
encouraged to visit:
http://www.elsevier.com/copyright
Author's personal copy
Multiple Sclerosis and Related Disorders (2013) 2, 29–35
Available online at www.sciencedirect.com
journal homepage: www.elsevier.com/locate/msard
A proposed methodology to estimate the
cumulative life-time UVB exposure using
geographic information systems: An application
to multiple sclerosis
N. Schuurmana, O. Amrama, J. Saeedib, P. Rieckmannc, I. Yeed, H. Tremlette,n
a
Department of Geography, Simon Fraser University, Canada
National Neuroscience Institute, King Fahad Medical City, Riyadh, Kingdom of Saudi Arabia
c
Department of Neurology, Sozialstiftung Bamberg Hospital, Bamberg, Germany
d
Department of Medical Genetics, University of British Columbia, Vancouver, Canada
e
Faculty of Medicine, Division of Neurology, Multiple Sclerosis Program and Brain Research Centre, Vancouver Coastal health
Research Institute, University of British Columbia, Vancouver, Canada
b
Received 11 May 2012; received in revised form 12 July 2012; accepted 17 July 2012
KEYWORDS
Multiple sclerosis;
Ultraviolet B
exposure;
Geographic Information Systems (GIS);
NASA Total Ozone
Mapping
Spectrometer;
Ecological study;
Methodological study
Abstract
Background: The cause of multiple sclerosis (MS) is unknown; multiple risk factors have been
implicated, including environmental exposures, such as sunlight. Many studies have relied on
latitude alone as a crude proxy for sunlight exposure. We aimed to develop a protocol allowing
a more detailed estimate of cumulative ambient ultra-violet B (UVB) exposure at critical timeperiods over a patient’s life-course.
Methods: 4010 definite MS patients with a ‘movement history’ from birth to the study end (2005)
were selected from the University of British Columbia, Canada’s MS Genetic database. Patient’s
place of resident from birth were tracked, each place being geocoded (latitude and longitude) and
assigned a UVB value using the NASA Total Ozone Mapping Spectrometer (TOMS) dataset. Combined,
these data allowed an estimated UVB value for each patient based on year and location.
Results: Using this protocol, we provide a potentially more detailed cumulative UVB exposure
for critical periods in a patients’ life history based on their individual spatial migration
through time.
Conclusions: This protocol is intended to provide a framework for researchers to more
accurately estimate UVB exposures for individuals over the course of their life history and may
be useful for understanding etiology of MS and other chronic disease.
& 2012 Elsevier B.V. All rights reserved.
n
Corresponding author. Tel.: +1 604 8220759; fax: +1 604 8227897.
E-mail address: helen.tremlett@ubc.ca (H. Tremlett).
2211-0348/$ - see front matter & 2012 Elsevier B.V. All rights reserved.
http://dx.doi.org/10.1016/j.msard.2012.07.003
Author's personal copy
30
1.
N. Schuurman et al.
Introduction
Multiple sclerosis (MS) is a chronic, degenerative disease of
the central nervous system for which the exact etiology is
not yet understood. Multiple risk factors may be involved
including interactions between susceptibility genes and
environmental factors (Milo and Kahana, 2010; Sospedra
and Martin, 2005). Several clinical and epidemiological
studies support the hypothesis that vitamin D levels –
perhaps mediated by ultraviolet B exposure – are able to
modulate disease processes in MS (Ascherio and Munger,
2007; Simon et al., 2011; van der Mei et al., 2011). Early
papers reported that the frequency of MS was greater
between 45 and 64 degrees latitude – than at lower
latitudes (Kurtzke, 1977). These reports were organized
geographically (Kurtzke, 1980) in a map that revealed bands
of higher prevalence in Northern and Central Europe as well
as North America and parts of Southern New Zealand and
Australia(Kurtzke, 1980).
Assignations of latitude have been variously derived based
on place of birth, location at puberty or place of symptom
onset or diagnosis (Detels et al., 1978; Hammond et al.,
2000; Sloka et al., 2008). There are two main shortcomings
with latitude correlation to date. First, selecting single
latitude for assignation of UVB exposure does not take into
account the role of the entire life history and movements
(e.g., what was the UVB exposure at key points in a patient’s
history). Related to this is that the current methods are not
able to account for increasingly mobile western populations
(Beretich and Beretich, 2009). Second, latitude correlations
do not measure actual ambient UVB exposure (i.e., the
actual level of UV radiation reaching earth). Notable exceptions include recent use of satellite data to determine
average UVB exposure at latitude (Beretich and Beretich,
2009; Sloka et al., 2008). Some have called for the calculation of more accurate population exposure estimates (Ebers,
2009), although to date, no standardized procedure has been
developed. This paper introduces a method to calculate UVB
exposure for patients at critical points as well as cumulative
exposure over the course of their life history using widely
available NASA data, with application to MS.
2.
with 180 cells longitude, 288 cells latitude and a cell
dimension of 1 1.25. The TOMS data UVB values consist
of 3 digit values that required conversion (using a standard
formula) in order to obtain the actual UVB value for each
location. As the TOMS data did not provide UVB values for all
locations within the study, a value of 999 (i.e., missing data)
was assigned to areas without data.
In preparation for analysis, a UVB value was assigned to
each year of each MS patient’s life. This value was
calculated by averaging daily NASA values over the year
(e.g. sum of all days/number of days of data). A UV
reference table was developed providing a UVB value for
each location for each year included in the study for each
patient. The reference table served the purpose of allowing
us to assign the correct UVB value to the ‘patient movement
table’ based on time and location. To populate the table, all
unique patients’ locations in the world were geocoded
(approximately 2500 locations). Annual UVB surfaces were
created for each year for which data were available. Days
for which no data were recorded were then subtracted (i.e.,
365 – days of no data). For years in which no UV data were
recorded, averaged surfaces were created based on years
for which data existed. Using the reference table, the
correct UVB value could be assigned to each patient based
on year and location.
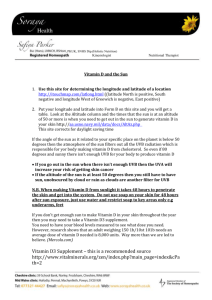
Figure 1 illustrates the development of the patient
movement table for assignation of a UVB value for each
patient year since birth.
2.1.
Data analyses
Geographic Information Systems (GIS) was the primary tool
used to analyze and visualize the data. In order to ensure
consistent projection within the software program, ArcGIS,
the NASA surface cell dimensions of 1 1.25 were resampled at a cell dimension of 1 1 (ArcGIS only reads
square cells). This required intermediary re-sampling with
the raster application IDRISI so that cells could be imported
into ArcGIS. After all the UVB surfaces were properly
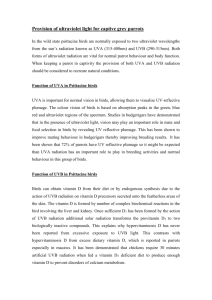
projected in ArcGIS, a reference table was created by
overlaying the surfaces with the geocoded cities and
extracting the UV value for each surface year. Figure 2.
Methods
3.
This was a retrospective study accessing patients with
definite MS ((Poser et al., 1983) or (McDonald et al., 2001)
criteria) through the University of British Columbia (UBC) MS
Clinic where detailed family histories are taken by a trained
genetic counsellor. From the ‘‘UBC MS Genetic database’’,
we identified MS patients with information detailing -their
movement since birth to study end (2005) as well as the
date (year) and location of each change in place of
residency were collated. This was linked to UVB data
obtained using the NASA Total Ozone Mapping Spectrometer
(TOMS) data set. TOMS data consists of several data sets
collected by NASA satellites during the period 1979 to 2005
(excluding 1994–95). Our study used TOMS’ Erythemal UVB
data as it provides a record of UVB values reflected from the
earth’s surface. This accounts for cloud coverage and only
captures UVB that reaches earth. The raw data is collected
and recorded daily by NASA and covers the world’s surface
Results
In total, 4010 definite MS patients were identified to have a
movement history. As a group, they had resided in 2656
different localities for which a unique latitude, longitude
and annualized UVB was assigned for every year of life. Of
the patients in the database, 82% were born in Canada, 4.2%
in the UK and 2.7% in the United States. Just over 10% were
born elsewhere in the world. Most of these patients (87.1%)
were of European ancestry and a breakdown of their ethnic
backgrounds is given in Table 2. Other demographic or
clinical information were not considered for this current
methodological study.
Table 1 gives an example of cumulative UVB exposure at
key points which might represent two patients’ lives (original details have been changed). The first patient, in red
(ID 1), resided in locations with relatively low sun exposure.
The second patient, in yellow (ID 2), lived in several locations,
Author's personal copy
A proposed methodology to estimate the cumulative life-time UVB exposure using geographic information systems
31
Figure 1 Illustration of the protocol for UVB calculation with the resultant patient movement table that assigns an accumulated
UVB value for each patient for each year since birth. This protocol enables researchers to accurately calculate potential UVB
exposures for individuals—based on their specific geographical residences—over the course of their life history.
Figure 2 Illustrates the creation of the UV reference table by extracting the UVB value from each UVB surface for each unique
location. Note: UVB values are for illustration purposes only.
one of which had significantly higher levels of sun exposure. As
a result, for the patient in yellow, the total accumulative UVB
exposure at age 15 was much higher. By comparison the
latitude alone – which has commonly been used as a proxy for
UVB exposure – gives little information. Slightly more information is provided using the NASA data for UVB for a token year
for the latitude. However, a visual comparison between the
cumulative UVB potential exposure value and the UVB potential exposure value for single latitude indicates clear
differences.
The results from Table 1 provide a means of determining
cumulative UVB exposure at critical points in each MS
patient’s life. By contrast, latitude alone or even UVB for
a token year at nominal latitude contain much less information – and are perhaps misleading given variations in sunlight
at the places that share the same latitude and between
different years. In Figure 3, we illustrate the difference in
informational content for a hypothetical patient who was
born and raised in each of the sample cities in a strip of
latitude from 491 to 511 from Vancouver BC, Canada to the
London, England. For each city (e.g., Vancouver, Calgary,
Winnipeg and London), we calculated cumulative UVB
exposure from 1980 to 2005. It is noteworthy that Calgary
and London, while at the same approximate latitude, show
very different values for UVB. Vancouver and Calgary, on the
other, hand are separated by two degrees of latitude and
Author's personal copy
32
N. Schuurman et al.
Table 1 An example of two MS patients, with their respective moves and the cumulative UVB exposure at each move. In
addition the accumulated UVB at critical time-points and for the year 2005 are also shown (grey row). By comparison, we show
the relatively low informational value of latitude alone.
ID
Move sequence
Year moved
City
Province
Country
Birth
Age
CumUV
Latitude
1
1
1
1
1
2
3
5
1977
1994
1995
1997
Port Hardy
Burns Lake
Vancouver
Victoria
British
British
British
British
Columbia
Columbia
Columbia
Columbia
Canada
Canada
Canada
Canada
Y
N
N
N
17
18
20
28
1361.3
1433.9
1599.6
2241.7
501410 N
54110 N
491230 N
481250 N
2
2
2
2
ID
1
2
3
5
1949
1973
1977
1995
Vancouver
Winnipeg
Calgary
Vancouver
UV birth
British Columbia
Manitoba
Alberta
British Columbia
Canada
Canada
Canada
Canada
UV age
Y
N
N
N
24
28
31
56
2072.0
2408.1
2644.7
4792.4
491250 N
491540 N
51110 N
491130 N
UV 2005
1
2
80
86
Figure 3
period.
2241.7
4792.4
A two degree strip of latitude illustrating that latitude alone does not substitute for UVB exposure over a twenty-five year
yet have comparable figures. This variability points to a
need to calculate values for individual locations rather than
rely on latitude as a proxy.
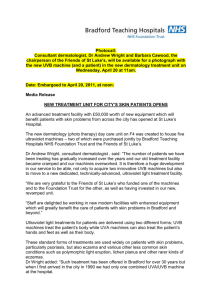
Figure 4 provides a visualization of the lifetime cumulative UVB exposures of each MS patient in the database. Note
that the majority live in British Columbia, Canada as might
be expected, however, their trajectories from country of
origin are also illustrated in the figure.Table 2.
4.
1205
1295
Discussion
We demonstrate that it is possible to calculate geographically specific ambient UVB exposure values for patients.
This is relevant particularly in the case of MS where several
clinical and epidemiological studies support the hypothesis
that ultraviolet B radiation (UVB) is able to modulate
disease processes and risk in MS, perhaps through vitamin
D (Ascherio and Munger, 2007; Milo and Kahana, 2010; Simon
et al., 2011; van der Mei et al., 2011). Studies have included
MS geographical distribution (Simpson et al., 2011), the
relation between the month of birth and MS risk (Staples
et al., 2010; Willer et al., 2004), the inverse association
between ambient UVB and MS relapses (Tremlett et al.,
2008) and lower levels of vitamin D during MS relapses
(Simpson et al., 2010; Soilu-Hanninen et al., 2008).
The prevalence of MS has been shown to follow a north
south gradient in its geographical distribution in several
Author's personal copy
A proposed methodology to estimate the cumulative life-time UVB exposure using geographic information systems
33
Figure 4 Illustrates cumulative UVB exposure with increased exposure shown as a gradient from yellow to red with increase in age
depicted by the height of the lines. The white lines represent trajectories from place of origin. The figure demonstrates visually the
variation in relative UVB exposure – even amongst the majority of Canadian born patients.
Table 2 Ethnic background of BC MS patients included
in the study (n =4010).
Ethnic background
N
%
European
Asian
Othera
Mixed
Unknownb
Total
3492
164
25
220
109
4010
87.1
4.1
0.6
5.5
2.7
100.0
a
Other – African, Caribbean, First Nations, Central and
South American.
b
Unknown – 63 cases had known ethnicity either on the
maternal or paternal side; 46 had unknown ethnicities on
both sides.
countries (Simpson et al., 2011) such as the USA (Wallin
et al., 2004), Australia (van der Mei et al., 2001) and some
European countries including France (Vukusic et al., 2007)
and Spain (Llorca et al., 2005). In these countries, the
prevalence of MS increased with latitude with lower prevalence rates in the more equatorial regions, however,
there are exceptions, notably Norway (Kampman and
Brustad, 2008). Interestingly, in France and USA an inverse
relation between MS prevalence and the minimum autumnal
UV erythemal level was demonstrated.
In Newfoundland (Canada’s easternmost province), significant correlation was found between MS incidence and
UVB radiation, and the risk of developing MS was mostly
related to the geographical place of residence in the first
year of life (Sloka et al., 2008). In Tasmania (Australia),
lower risk of developing MS was associated with a higher sun
exposure in the first 6–15 years of life (van der Mei et al.,
2003).
Even the gestational environment might influence the risk
of developing MS later in life; (Willer et al., 2004) (Staples
et al., 2010) individuals born in the northern hemisphere in
November had a lower risk of developing MS than those born
in May (OR =1.19, 95%CI:1.14–1.25) (Willer et al., 2004)
although this was only found in those with relapsing-onset
MS, not primary-progressive (Sadovnick et al., 2007). The
inverse has been observed in the southern hemisphere
(Staples et al., 2010), with the greatest risk being those
born in November–December compared to May–June
(Staples et al., 2010).
Both UVB and vitamin D have been shown to modulate the
immune system, primarily in animals (including the animal
model of MS, experimental allergic encephalomyelitis
(EAE), (Cantorna et al., 1996), but also in humans
(Ponsonby et al., 2005; Smolders et al., 2008). Therefore,
exposure to UVB has been implicated in the etiology of MS,
either directly via its immunosuppressive effect or indirectly through vitamin D (Smolders et al., 2008) or perhaps
melatonin synthesis (Constantinescu, 1995) all of which
have immunomodulatory effects.
In this study, we do not examine the effects of UVB
exposure on the etiology of MS. However, we provide an
important first step towards more accurate analysis of these
possible effects through the development of a preliminary
protocol for calculating cumulative UVB exposure at critical
points in patients’ life histories. This protocol is intended to
provide an alternative to latitude based assumptions about
UVB exposure (based on geographic location) as it uses daily
UVB exposure to provide real potential cumulative exposure
rather than exposure estimated based on latitude alone. In
addition, it allows exposure to be calculated for key
moments in patients’ life histories (e.g., birth, onset of
puberty, onset of MS). This might be helpful in future
research to help address how lifelong UVB accumulation
affects MS. This protocol is generalizable across multiple
disease studies where UVB exposure is considered a possible
correlate and is fully adaptable to interrogate the importance of different UVB wavelengths or summer vs. winter
UVB levels.
Limitations of our study include the inability to directly
measure either actual sunlight exposure or serum vitamin D
levels for each patient over their individual life course –
which would depend on a complex range of factors such as
time spent outdoors, amount of skin exposed, skin colour
and diet - such a study would likely be logistically impossible
as well as prohibitively expensive. Nonetheless, cohort
studies where a sub-set of patients are followed for finite
periods of time would be useful to validate the association
between ambient UVB and serum vitamin D across the
seasons. Our study’s strength is its ability to provide
geographically specific potential UVB exposure data – even
as the patient moves through time and space during the
course of their life.
Author's personal copy
34
5.
N. Schuurman et al.
Conclusion
Insufficient methodological data in previous studies has
made replication of findings difficult, resulting in uncertainties. In particular, we suggest that individual latitudes
cannot be assigned a universal UVB value; rather UVB is
both spatially and temporally dynamic. As a result, UVB
must be calculated on at least an annual basis for each
location and for each patient throughout their lifetime. In
combination, these two protocols result in cumulative lifetime UVB exposure data for each patient. We have developed a set of standardized protocols for the calculation of
ambient UVB exposure over a lifetime – that takes into
account patients’ geographical movement. We anticipate
that the results will permit a standardized protocol for
calculation of UVB exposure. Our research has important
implications for ecological studies linking ambient UVB to
incidence and prevalence and progression in MS and answers
the calls of previous researchers for such a methodology
(Beretich and Beretich, 2009; Ebers, 2009). We welcome
discussion on refining these methods and encourage others
to apply these methods in different geographical areas.
Conflict of interest
All other co-authors have no conflicts or disclosure to
report.
Acknowledgments
We extend our thanks to Prof. Dessa Sadovnick’s group for
data access and the genetic counselors for data collection.
Nadine Shuurman is funded by Michael Smith Foundation
for Health Research Scholar.
Jameelah Saeedi was funded during her fellowship by
King Fahad Medical City, Riyadh, Kingdom of Saudi Arabia.
Helen Tremlett is funded by the Multiple Sclerosis Society
of Canada (Don Paty Career Development Award), Michael
Smith Foundation for Health Research and is the Canada
Research Chair for Neuroepidemiology and Multiple Sclerosis. She has received: research support from the US National
Multiple Sclerosis Society, CIHR, and UK MS Trust; speaker
honoraria and/or travel expenses to attend conferences
from the Consortium of MS Centres, US National MS Society,
the University of British Columbia Multiple Sclerosis
Research Program, Bayer Pharmaceutical (speaker, 2010,
honoraria declined), Teva Pharmaceuticals (speaker 2011),
ECTRIMS (2011), UK MS Trust (2011) and the Chesapeake
Health Education Program, US Veterans Affairs (2012,
honorarium declined). Unless otherwise stated, all speaker
honoraria are either donated to an MS charity or to an
unrestricted grant for use by her research group.
References
Ascherio A, Munger KL. Environmental risk factors for multiple
sclerosis. Part II: Noninfectious factors. Annals of Neurolology
2007;61:504–13.
Beretich BD, Beretich TM. Explaining multiple sclerosis prevalence
by ultraviolet exposure: a geospatial analysis. Multiple Sclerosis
2009;15:891–8.
Cantorna MT, Hayes CE, DeLuca HF. 1,25-Dihydroxyvitamin D3
reversibly blocks the progression of relapsing encephalomyelitis,
a model of multiple sclerosis. Proceedings of the National
Academy of Sciences of the USA 1996;93:7861–4.
Constantinescu CS. Melanin, melatonin, melanocyte-stimulating
hormone, and the susceptibility to autoimmune demyelination:
a rationale for light therapy in multiple sclerosis. Medical
Hypotheses 1995;45:455–8.
Detels R, Visscher BR, Haile RW, Malmgren RM, Dudley JP, Coulson
AH. Multiple sclerosis and age at migration. American Journal of
Epidemiolology 1978;108:386–93.
Ebers GC. Editorial regarding ‘‘Explaining multiple sclerosis prevalence by ultraviolet exposure: a geospatial analysis,’’ by
Beretich and Beretich. Multiple Sclerosis 2009;15:889–90.
Hammond SR, English DR, McLeod JG. The age-range of risk of
developing multiple sclerosis: evidence from a migrant population in Australia. Brain 2000;123:968–74.
Kampman MT, Brustad M. Vitamin D: a candidate for the environmental effect in multiple sclerosis - observations from Norway.
Neuroepidemiology 2008;30:140–6.
Kurtzke JF. Geography in multiple sclerosis. Journal of Neurology
1977;215:1–26.
Kurtzke JF. Geographic distribution of multiple sclerosis: An update
with special reference to Europe and the Mediterranean region.
Acta Neurologica Scandinavica 1980;62:65–80.
Llorca J, Guerrero P, Prieto-Salceda D, Dierssen-Sotos T. Mortality of
multiple sclerosis in Spain: demonstration of a north-South
gradient. Neuroepidemiology 2005;24:135–40.
McDonald WI, Compston A, Edan G, et al. Recommended diagnostic
criteria for multiple sclerosis: guidelines from the International
Panel on the diagnosis of multiple sclerosis. Annals of Neurology
2001;50:121–7.
Milo R, Kahana E. Multiple sclerosis: geoepidemiology, genetics and
the environment. Autoimmunity Reviews. 2010;9:A387–94.
Ponsonby AL, Lucas RM, van der Mei IA. UVR, vitamin D and three
autoimmune diseases–multiple sclerosis, type 1 diabetes, rheumatoid arthritis. Photochemistry and Photobiology 2005;81:
1267–75.
Poser CM, Paty DW, Scheinberg L, et al. New Diagnostic Criteria for
Multiple Sclerosis: guidelines for research proposals. Annals of
Neurology 1983;13:227–31.
Sadovnick AD, Duquette P, Herrera B, Yee IM, Ebers GC. A timing-ofbirth effect on multiple sclerosis clinical phenotype. Neurology
2007;69:60–2.
Simon KC, Munger KL, Ascherio A. XVI European Charcot Foundation
lecture: Nutrition and environment, can MS be prevented?
Journal of the Neurological Sciences 2011;311:1–8.
Simpson S, Blizzard L, Otahal P, Van der Mei I, Taylor B. Latitude is
significantly associated with the prevalence of multiple sclerosis: a meta-analysis. Journal of Neurology, Neurosurgery and
Psychiatry 2011;82:1132–41.
Simpson Jr. S, Taylor B, Blizzard L, et al. Higher 25-hydroxyvitamin
D is associated with lower relapse risk in multiple sclerosis.
Annals of Neurology 2010;68:193–203.
Sloka JS, Pryse-Phillips WE, Stefanelli M. The relation of ultraviolet
radiation and multiple sclerosis in Newfoundland. Canadian
Journal of Neurological Sciences 2008;35:69–74.
Smolders J, Damoiseaux J, Menheere P, Hupperts R. Vitamin D as an
immune modulator in multiple sclerosis, a review. Journal of
Neuroimmunology 2008;194:7–17.
Soilu-Hanninen M, Laaksonen M, Laitinen I, Eralinna JP, Lilius EM,
Mononen I. A longitudinal study of serum 25-hydroxyvitamin D
and intact parathyroid hormone levels indicate the importance
of vitamin D and calcium homeostasis regulation in multiple
sclerosis. Journal of Neurology, Neurosurgery and Psychiatry
2008;79:152–7.
Sospedra M, Martin R. Immunology of multiple sclerosis. Annual
Reviews in Immunolology 2005;23:683–747.
Author's personal copy
A proposed methodology to estimate the cumulative life-time UVB exposure using geographic information systems
Staples J, Ponsonby A-L, Lim L. Low maternal exposure to ultraviolet radiation in pregnancy, month of birth, and risk of
multiple sclerosis in offspring: longitudinal analysis. British
Medical Journal 2010;340:c1640.
Tremlett H, van der Mei IA, Pittas F, et al. Monthly ambient
sunlight, infections and relapse rates in multiple sclerosis.
Neuroepidemiology 2008;31:271–9.
van der Mei IA, Ponsonby AL, Blizzard L, Dwyer T. Regional variation
in multiple sclerosis prevalence in Australia and its association
with ambient ultraviolet radiation. Neuroepidemiology 2001;20:
168–74.
van der Mei IA, Ponsonby AL, Dwyer T, et al. Past exposure to sun,
skin phenotype, and risk of multiple sclerosis: case-control
study. British Medical Journal 2003;327:316.
35
van der Mei IA, Simpson Jr. S, Stankovich J, Taylor BV. Individual and
joint action of environmental factors and risk of MS. Neurologic
Clinics 2011;29:233–55.
Vukusic S, Van Bockstael V, Gosselin S, Confavreux C. Regional
variations in the prevalence of multiple sclerosis in French
farmers. Journal of Neurology, Neurosurgery and Psychiatry
2007;78:707–9.
Wallin MT, Page WF, Kurtzke JF. Multiple sclerosis in US veterans of
the Vietnam era and later military service: race, sex, and
geography. Annals of Neurology 2004;55:65–71.
Willer CJ, Dyment DA, Sadovnick AD, Rothwell PM, Murray TJ, Ebers
GC. Timing of birth and risk of multiple sclerosis: population
based study. British Medical Journal 2004;330:120–5.