Mechanical and metabolic requirements for active lateral stabilization in human walking
advertisement

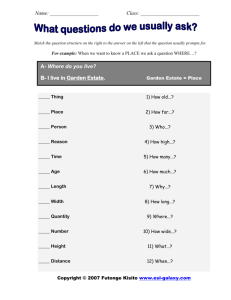
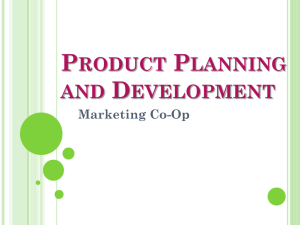
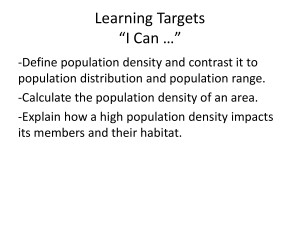
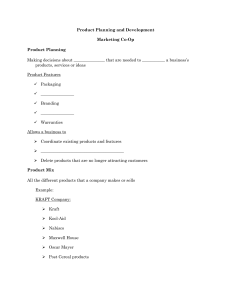
ARTICLE IN PRESS Journal of Biomechanics 37 (2004) 827–835 Young Scientist Pre-Doctoral Award Mechanical and metabolic requirements for active lateral stabilization in human walking J. Maxwell Donelana,*, David W. Shipmanb, Rodger Kramc, Arthur D. Kuod a Department of Physiology, University of Alberta, Edmonton, AB T6G 2H7, Canada Department of Integrative Biology, University of California, Berkeley, CA 94720-3140, USA c Department of Integrative Physiology, University of Colorado, Boulder, CO 80309-0354, USA d Department of Mechanical Engineering, University of Michigan, Ann Arbor, MI 48109-2125, USA b Received 16 June 2003; accepted 23 June 2003 Abstract Walking appears to be passively unstable in the lateral direction, requiring active feedback control for stability. The central nervous system may control stability by adjusting medio-lateral foot placement, but potentially with a metabolic cost. This cost increases with narrow steps and may affect the preferred step width. We hypothesized that external stabilization of the body would reduce the active control needed, thereby decreasing metabolic cost and preferred step width. To test these hypotheses, we provided external lateral stabilization, using springs pulling bilaterally from the waist, to human subjects walking on a force treadmill at 1.25 m/s. Ten subjects walked, with and without stabilization, at a prescribed step width of zero and also at their preferred step width. We measured metabolic cost using indirect calorimetry, and step width from force treadmill data. We found that at the prescribed zero step width, external stabilization resulted in a 33% decrease in step width variability (root-mean-square) and a 9.2% decrease in metabolic cost. In the preferred step width conditions, external stabilization caused subjects to prefer a 47% narrower step width, with a 32% decrease in step width variability and a 5.7% decrease in metabolic cost. These results suggest that (a) human walking requires active lateral stabilization, (b) body lateral motion is partially stabilized via medio-lateral foot placement, (c) active stabilization exacts a modest metabolic cost, and (d) humans avoid narrow step widths because they are less stable. r 2004 Elsevier Ltd. All rights reserved. Keywords: Biomechanics; Biped; Energetics; Locomotion; Gait 1. Introduction The dynamic stability of walking depends on the interaction between the passive dynamics of the musculoskeletal system and active control produced by the central nervous system (CNS). A passively stable musculoskeletal system is able to reject small perturbations without direct intervention by the CNS. But instability in the passive dynamics must be countered by active control, which requires coordinated sensing of perturbations, generation of appropriate response motor programs, and production of compensatory body motions. This places a computational demand on the CNS and a mechanical and metabolic demand on muscles. Active control is also subject to limitations in the precision of sensory receptors and muscles. There *Corresponding author. E-mail address: mdonelan@ualberta.ca (J.M. Donelan). 0021-9290/$ - see front matter r 2004 Elsevier Ltd. All rights reserved. doi:10.1016/j.jbiomech.2003.06.002 may therefore be significant advantages to harnessing any passive stability afforded by walking in order to minimize active control and its associated costs. Mathematical modeling suggests that the dynamics of bipedal walking is passively stable, with the exception of lateral motion. McGeer (1990) demonstrated that with little actuation and no active control, stable walking gaits can arise from the dynamic interactions between the legs and the ground. These gaits, when restricted to the sagittal plane, are passively stable. But passive dynamic walking models that move side-to-side and have human-like mass distribution are laterally unstable, even though they retain stability within the sagittal plane (Kuo, 1999). Applying these principles to human walking suggests a need for dedicated active feedback control of lateral motion (Fig. 1a). Kuo (1999) showed that medio-lateral foot placement is a particularly effective method for stabilizing lateral balance in passive walking models. Subsequent empirical ARTICLE IN PRESS J.M. Donelan et al. / Journal of Biomechanics 37 (2004) 827–835 828 Without External Lateral Stabilization gait dynamics CNS Control Lateral Stance/Swing lateral motion sagittal plane motion passive stability active feedback (a) With External Lateral Stabilization external stabilization CNS Control Lateral Stance/Swing lateral motion sagittal plane motion passive stability active feedback (b) Fig. 1. The dynamic stability of walking depends on the interaction between the passive dynamics of the musculoskeletal system and active control produced by the CNS. (a) In normal walking, ‘‘passive’’ feedback is available to stabilize motion in the sagittal plane, but stable lateral motion requires ‘‘active’’ feedback and active control by the CNS. (The solid lines denote pathways that are present or necessary. The dashed lines represent pathways that are not present or not necessary.) (b) External lateral stabilization provides passive feedback control to stabilize lateral motion making active feedback control no longer necessary. measurements demonstrated that humans have increased medio-lateral foot placement variability when walking with reduced visual information (Bauby and Kuo, 2000). This suggests that humans actively stabilize lateral motion using medio-lateral foot placement and that this active control mechanism is less precise when there is less sensory information. If subjects were passively stable, they would be expected to have no sensitivity to sensory information. Active stabilization of lateral balance in human walking may exact a significant metabolic cost for two reasons. First, active movement of the legs to adjust medio-lateral foot placement exacts a metabolic cost (Donelan et al., 2001; Shipman et al., 2002). Second, mechanical work is performed to redirect the center of mass (COM) during the transition between steps (referred to as step-to-step transition costs, Donelan et al., 2002). This work exacts a proportional metabolic cost and increases with the square of step width (Donelan et al., 2001). The consequence of this nonlinear dependence upon step width is that, for the same average step width, variability in medio-lateral foot placement will increase the average step-to-step transition cost. Lateral instability may play a role in determining the step width preferred by humans. The mechanical work of step-to-step transitions is minimized when humans walk with zero step width (Donelan et al., 2001). But the step width that minimizes metabolic cost—and is in fact preferred by humans—is about 0.13L (where L is leg length). Other factors must therefore increase metabolic cost for narrow step widths. One possibility is that walking with narrow steps is more unstable, requiring greater active control. This intuitive prediction is supported by mathematical modeling (Kuo, 1999). The trade-off between minimizing mechanical work to redirect the COM and the cost of active stabilization of lateral balance may determine the step width preferred by humans. We studied the mechanical and metabolic requirements of active lateral stabilization in human walking. A mathematical model, based on passive dynamics, predicts that walking could be completely stabilized using only external lateral forces (Fig. 2), thus removing the need for active control. Inspired by this model, we built a device that applied lateral stabilizing forces to human subjects as they walked on a force treadmill (Fig. 3). We hypothesized that external lateral stabilization would reduce the amount of active stabilization required to walk (Fig. 1b), resulting in less variability of mediolateral foot placement and a reduced metabolic cost. We also hypothesized that when subjects were allowed to choose their step width, they would prefer a narrower step width when externally stabilized, because the advantages of wider steps for active stabilization are eliminated if walking is made passively stable. 2. Methods 2.1. Model predictions A previously developed mathematical model, based on passive dynamics, predicts that walking is passively unstable in the lateral direction (Donelan et al., 2001; Kuo, 1999). Passive dynamic walking refers to a class of walking models that walk with little or no actuation and no active control. During single support phases, the legs act as freely swinging, coupled pendula. Double support phases function as transitions between single support phases and are modeled as instantaneous, inelastic collisions between foot and ground. The energy lost during each transition can be replaced by a toe-off impulse applied along the trailing leg, or by walking down a gentle slope (Kuo, 1999; McGeer, 1990). We previously studied stability in a simple three-dimensional model (Fig. 2a), with leg inertia condensed into point masses at the pelvis and feet, and the mass of the feet much smaller than that of the pelvis (Donelan et al., 2001; Garcia et al., 1998). The model predicted that ARTICLE IN PRESS J.M. Donelan et al. / Journal of Biomechanics 37 (2004) 827–835 3-D Walking Model K Stability analysis 40 φ ψ 2β swing swing leg leg m Front stance leg Eigenvalue magnitude M θ stance leg 20 stable zone m 0 0.0 Front view 829 Side view 0.5 1.0 1.5 2.0 Stabilizer Stiffness (K) (b) (a) Fig. 2. (a) Simple three-dimensional walking model with external lateral stabilization. Model has three degrees of freedom: stance (y) and swing (f leg angles in the sagittal plane, and roll angle (c)). Mass is concentrated in points located at the pelvis (M) and feet (m). Step width is adjusted by changing the splay angle, b: External lateral stabilization is provided by a spring with stiffness, K: (b) Stability analysis (see Appendix A) demonstrates that increasing stabilizer stiffness, K; decreases instability. Without external stabilizing forces, the walking model is very unstable (yintercept is much greater than 1). For normalized stiffness K > 1; the walking model is passively stable. Stability is described by the eigenvalue corresponding to the unstable lateral mode in the step-to-step dynamics, with a magnitude less than one forming the boundary of the stable zone. For all values of K; the least stable mode was for lateral motion. Force transducer Spring Force transducer Spring 8.5m Hip belt 8.5m Treadmill Force platform Fig. 3. External lateral stabilizer. Two lightweight elastic cords attached to a padded waist belt stabilized lateral motion by pulling laterally on walking subjects. walking is passively stable in the plane of progression but has one highly unstable mode (see current Appendix for details), confined mainly to the lateral motion. Active feedback control can be used to stabilize this mode, for example, through medio-lateral adjustments to foot placement (Bauby and Kuo, 2000). In the present study, we found that the external application of spring-like lateral forces can passively stabilize our walking model. We modified our previously developed model to include a purely lateral elastic restoring force, F ; applied to the pelvis F ¼ KL sin c; ð1:1Þ where K is the spring stiffness, L the leg length, and c the roll angle (Fig. 1a). The effect of the stabilizing spring is demonstrated most clearly when the model walks at zero step width, and F merely acts as proportional control about a pelvis trajectory that has no lateral motion. In the absence of disturbances, the spring exerts no force and has no effect on the walking model; it only counters disturbances out of the plane of progression. We studied the stability of this model by examining its response to small perturbations: a matrix describing the step-to-step dynamics will have eigenvalues with magnitude less than 1 for a stable system (see Appendix A). We found that increasing K acts to stabilize the model (Fig. 2b), reducing the need for active feedback control. For all values of K; the least stable mode was almost entirely associated with lateral motion; the lateral components accounted for more than 99.9% of the length of the eigenvector of the least stable mode. Similar predictions apply for more complex models and situations. The passive lateral instability holds for a wide range of step widths, although narrow steps are slightly more unstable (Kuo, 1999; McGeer, 1990). We found that the stabilizing effect of the external force from Eq. (1.1) also applies to non-zero step widths where the pelvis moves side to side. We also investigated the effect of a more realistic stabilizing spring by adding a damping term to Eq. (1.1). A small amount of damping results in stability at a smaller K; but at the cost of increased energy dissipation when the pelvis moves laterally. Finally, we found that these stability properties are retained in a more complex model with realistic anthropomorphic parameters (Kuo, 1999). 2.2. Experimental procedures We compared the mechanics and metabolic cost in 10 human adult subjects, walking on a treadmill with and ARTICLE IN PRESS J.M. Donelan et al. / Journal of Biomechanics 37 (2004) 827–835 830 without externally applied stabilization. All volunteer subjects (six male, four female, body mass 73.3714.2 kg; leg length 0.9570.05 m; mean7s.d.) were healthy and exhibited no clinical gait abnormalities. Before the experiments began, subjects gave their informed consent to participate in accordance with University of California policy. The equipment consisted of an external lateral stabilizer, a force treadmill and an indirect calorimetry system. The experimental design required the subjects to walk at a prescribed zero step width and then at their preferred step width, both with and without external lateral stabilization—a total of four walking trials for each subject. The external lateral stabilizer consisted of two lightweight elastic cords that attached to the subject and pulled in both lateral directions (Fig. 3). Each adjustable cord was made of 8.0 m of nylon cord in series with 0.5 m of rubber tubing. One end of each cord was attached to a force transducer, used to monitor stabilizing forces, and the force transducer was anchored to a wall. The other end was attached to each subject via a padded belt (taken from a hip-supported backpack) worn securely about the waist. The two cords had an effective spring constant of approximately 1700 N/m and negligible damping (14 N-s/m), identified by oscillating a known mass between the cords and estimating the parameters from a second-order damped oscillator model. We used long length cords to ensure that any non-lateral forces exerted by the apparatus were negligible. For example, peak vertical displacements of the COM are approximately 0.04 m resulting in vertical forces of less than 0.1% body weight. We also estimated unwanted fore-aft forces to be less than 0.1% body weight. We used the center-of-pressure of ground reaction forces (see Fig. 4) to measure average step width and step length, as well as variability in step width and step length. We calculated instantaneous center of pressure using ground reaction forces and moments measured with the force treadmill (Kram et al., 1998). The ground reaction forces and moments were sampled at 100 Hz and low-pass filtered with a 25 Hz cut-off frequency (fourth-order, zero-phase-shift Butterworth digital filter). Step width was defined as the lateral distance between consecutive centers of pressure for the time sample immediately before heel-strike. We choose to use this time sample because the ground reaction forces and moments are large during this period of single support, thereby maximizing the signal-to-noise ratio. Step length was defined as the fore-aft distance between consecutive centers of pressure summed with the distance traveled during the step (the latter term is necessary to correct for treadmill belt speed). The distance traveled during each step was calculated from the product of treadmill velocity and the time between consecutive heel-strikes. We identified heel-strikes from the characteristic forward translation of the center of pressure that occurs at the beginning of double support. We calculated each subject’s instantaneous center of pressure, and the mean and root-mean-square (rms) of step width and step length, for 200 steps after the subject had been walking for 150 s. To account for differences in body size, we normalized all length measurements by leg length. The precision of our estimates of step width and step length was limited by the precision by which centers of pressure and timing of gait events could be detected. Compared to more direct kinematic methods of estimating these same measures (Bauby and Kuo, 2000), the force plate method is slightly less precise, but nonetheless adequate for detecting changes in step variability. We determined the COM position (see Fig. 4) using the vector sum of the external forces acting on the subject. In our experiment, the only substantial external forces acting on the subject are from gravity, the ground and the external lateral stabilizer. These were measured using the mass of the subject, the force treadmill, and force transducers in series with the stabilizing cords, respectively. We calculated COM acceleration by Condition: Prescribed Step Width COM without external stabilization COP COM with external stabilization COP (a) Condition: Preferred Step Width step width 0.2m 0.2m step length (b) Fig. 4. Center of pressure (COP) and COM trajectories for walking (a) at the prescribed zero step width, and (b) at the preferred step width. Data shown are averages of 200 steps from each subject walking with and without external lateral stabilization. Our definitions of step width and length are illustrated for the condition of walking at preferred step width, without external lateral stabilization. Foot placement varied from step to step, relative to the average step width and length. The scale is the same for both (a) and (b). ARTICLE IN PRESS J.M. Donelan et al. / Journal of Biomechanics 37 (2004) 827–835 dividing the vector sum of the external forces by body mass. COM position is the second time-integral of the acceleration subject to appropriate boundary conditions (Cavagna, 1975; Donelan et al., 2002). Applying a high pass filter, with a cut-off frequency of one-tenth of each subject’s step frequency, after each integration removed the effect of any low frequency bias (fourth-order, zerophase-shift Butterworth digital filter). We performed each integration over the same 200 steps used for center of pressure calculations. Using a large number of steps increases the accuracy of our boundary condition assumptions. We used indirect calorimetry to measure metabolic cost (McLean and Tobin, 1987). We measured the rates of oxygen consumption ðV’ O2 Þ and carbon dioxide production ðV’ CO2 Þ using an open circuit respirometry system (Physio–Dyne Instrument Co., Quogue, NY). After a resting trial in which subjects stood quietly, we conducted the remaining walking trials in random order. Each trial lasted seven minutes, including three minutes for the subjects to reach steady state (Poole and Richardson, 1997) and then three minutes for collection of average V’ O2 (ml O2 s1) and V’ CO2 (ml CO2 s1) data. We discarded the seventh minute of data due to a delay between breath expiration and breath analysis. We calculated metabolic power (W) for each trial using the following standard equation (Brockway, 1987): s ’ Pmet; gross ¼ 16:58mlWOs 2 V’ O2 þ 4:51mlWCO VCO2 : 2 ð1:2Þ We subtracted the metabolic power for standing from all walking values and divided by body mass to derive net metabolic power (W/kg). We also calculated dimensionless net metabolic cost of transport (COT) by dividing net metabolic power by the gravitational constant (9.81 m/s2) and by walking velocity (m/s). The metabolic measurements were collected during the same trial as the mechanics measurements. We measured the effects of external lateral stabilization as subjects walked at both a prescribed zero step width and at their preferred step width. In all conditions, subjects walked at a fixed treadmill speed of 1.25 m/s, with average step frequency and step length controlled by instructing subjects to match a metronome set to their previously determined preferred step frequency. The arms were crossed in all conditions, both to control against changes in arm motion, and because the external stabilizer interferes with normal arm swinging. The prescribed step width conditions were designed to detect changes in the metabolic cost of active control induced by external stabilization, independent of other potential metabolic costs that might change with step width. We chose a target of zero step width because our device stabilizes the body about a trajectory with zero lateral movement. Zero average step width was controlled by instructing subjects to walk on a single line marked on the treadmill belt. This condition 831 was repeated with and without external stabilization. We then used a separate set of conditions, in which subjects walked at their preferred (i.e. freely selected) step width, to determine whether external stabilization affects preferred step width. Subjects practiced all conditions prior to data collection. We performed our statistical comparisons using paired t-tests with a level of significance of po0.05. Reported p values less than 0.05 are from one-tailed tests and p values greater than 0.05 are from two-tailed t-tests. 3. Results For both the prescribed step width and preferred step width control trials (i.e. without external stabilization), subjects walked with a preferred step frequency of 1.7670.10 Hz (mean7s.d.), and a preferred step length of 0.75670.052L (where L is leg length). In the prescribed step width control condition, subjects walked with a step width of 0.01170.009L (Fig. 5), close to the target width. Foot placement variabilities, described by rms step width and step length, were 0.01670.004L and 0.029 0.007L, respectively. Peak-to-peak lateral displacement of the COM was 0.00570.003L. The net metabolic cost for the prescribed step width control condition was 3.1870.77 W/kg. In the preferred step width control condition, subjects walked with a preferred step width of 0.12170.029L (Fig. 6). Foot placement variabilities were 0.01670.003L (rms step width) and 0.02670.009L (rms step length). Peak-topeak lateral displacement of the COM was 0.03370.008L. Net metabolic cost for the preferred step width control condition was 2.9670.45 W/kg. For the prescribed step width conditions, external lateral stabilization reduced both foot placement variability and metabolic cost (Fig. 5). With external stabilization, subjects walked with a step width of 0.01070.007L, and a step length of 0.75670.052L, neither of which were significantly different from the control trials (p ¼ 0:64 and p ¼ 0:78; respectively). In contrast, foot placement variabilities decreased significantly, with a 33% decrease in rms step width to 0.01170.006L (p ¼ 3:1 104 ), and a 16% decrease in rms step length to 0.02370.004L (p ¼ 4:8 103 ). The reduction in step width variability was 201% greater than the reduction in step length variability (p ¼ 0:016). Peak to-peak lateral displacement of the COM was not significantly different from the control condition (0.00870.004L; p ¼ 0:22). External stabilization resulted in a 9.2% decrease in the metabolic cost of prescribed step width walking, to 2.8270.41 W/kg (p ¼ 0:025). For the preferred step width conditions, external lateral stabilization reduced preferred step width, foot ARTICLE IN PRESS J.M. Donelan et al. / Journal of Biomechanics 37 (2004) 827–835 Condition: Preferred Step Width Metabolic cost 0.04 0.00 0.00 (a) 0.2 2 0.1 1 0 0.0 0.3 0.12 0.12 0.08 0.08 0.04 0.04 0.00 0.00 (b) 0.00 0.00 Step width rms Step length rms Fig. 5. Effects of external lateral stabilization on subjects walking at the prescribed zero step width. (a) Average step width was unaffected by the external lateral stabilizer and was close to the target zero width. External stabilization resulted in decreases in (b) metabolic cost, and (c) step width and length variability. Values shown are means7s.d., N ¼ 10: Asterisk (), denotes a statistically significant difference (po0.05). Distance (L) 0.01 0.03 0.03 Distance (m) Distance (L) (c) 0.01 0 0.0 Step width and length variability 0.03 0.02 1 0.04 0.04 * 0.1 with external stabilization Step width and length variability 0.02 2 without external stabilization with external stabilization * 3 0.2 (b) (a) without external stabilization 0.03 * 0.02 * 0.02 Distance (m) 0.04 3 4 * Cost of transport 0.08 Distance (m) Distance (L) 0.08 Cost of transport 0.3 0.12 0.12 4 * Metabolic cost 0.16 Distance (L) 0.16 Net metabolic power (W/kg) Average step width Average step width Net metabolic power (W/kg) Condition: Prescribed Step Width Distance (m) 832 0.01 0.01 0.00 0.00 Step width rms Step length rms (c) Fig. 6. Effects of external lateral stabilization on subjects walking at their freely selected step width. External stabilization resulted in decreases in (a) preferred step width (b) metabolic cost, and (c) step width and length variability. Values shown are means7s.d., N ¼ 10: Asterisk (), denotes a statistically significant difference (po0.05). 4. Discussion placement variability and metabolic cost. Compared to the control trials, subjects preferred a 47% narrower step width of 0.06570.043L (p ¼ 3:4 104 ) when externally stabilized (Fig. 6). No significant change was observed in step length (p ¼ 0:55). Foot placement variabilities decreased by 32% for rms step width and 14% for rms step length, to 0.01170.004L (p ¼ 1:1105 ) and 0.02270.006L (p ¼ 0:055; not statistically significant), respectively. The reduction in step width variability was 235% greater than the reduction in step length variability (p ¼ 0:036). Peakto-peak lateral displacement of the COM was 0.01470.008L, a 60% decrease from the control condition (p ¼ 3:8 106 ). External stabilization also resulted in a 5.7% reduction in the metabolic cost of preferred step width walking, to 2.7870.38 W/kg (p ¼ 0:015). We provided external lateral stabilization to walking subjects in order to understand the mechanical and metabolic requirements of active lateral stabilization in normal human walking. By reducing the active feedback control required of the CNS (Fig. 1b), we addressed four main questions. First, is walking passively unstable in the lateral direction? If so, by what mechanism do we actively stabilize? Does this active lateral stabilization exact a significant metabolic cost? Finally, does passive instability in the lateral direction affect our choice of preferred step width? The observed reductions in foot placement variability with external lateral stabilization—33% and 32% in prescribed and preferred step width conditions, respectively—are in agreement with our hypotheses that walking is passively unstable in the lateral direction, requiring balance to be maintained through active feedback control, largely by adjustments in foot placement. ARTICLE IN PRESS J.M. Donelan et al. / Journal of Biomechanics 37 (2004) 827–835 Active lateral stabilization also appears to exact a metabolic cost. Adjustments to foot placement are quite small, typically only a few centimetres per step. Yet, observed decreases in foot placement variability were accompanied by modest but significant decreases in metabolic cost. This is likely a result of two factors. First, reduced variability implies reduced lateral movement of the swing leg and this motion may cost metabolic energy (Donelan et al., 2001; Shipman et al., 2002). Second, reduced variability in medio-lateral foot placement results in lower step-to-step transition costs because transition costs are proportional to the square of step width (Donelan et al., 2001). In the freely selected step width conditions, part of the energetic advantage might alternatively be due to the narrower steps that subjects preferred when laterally stabilized. Narrower steps require less mechanical work to redirect the COM between steps, with a proportional reduction in metabolic cost (Donelan et al., 2001, 2002). But this does not apply to the zero step width conditions, which were designed to control for step width, and external stabilization still resulted in a 9.2% decrease in metabolic cost. Decreases in foot placement variability are the most likely explanation for the decrease in metabolic cost with external stabilization. Our results also imply that lateral instability affects the choice of preferred step width. The 43% decrease in preferred step width with external stabilization indicates that when there is no need to actively stabilize lateral balance, humans take advantage of lower costs for stepto-step transitions at narrow step widths. External stabilization presumably reduces the energetic costs that would otherwise accompany narrow steps if active control was necessary, resulting in a 5.7% decrease in metabolic cost at the freely selected step width. There remains, however, a greater metabolic cost at very narrow step widths (3.18 W/kg at zero step width vs. 2.96 W/kg at preferred step width), regardless of external stabilization. This prevents the preferred step width from being zero, which would minimize step-tostep transition costs. The additional metabolic cost may be for moving the swing limb laterally to avoid colliding with the stance limb at very narrow step widths (Donelan et al., 2001; Shipman et al., 2002). Another disadvantage of very narrow steps is that they afford a smaller margin of safety between the COM and center of pressure. If the COM passes laterally outside the center of pressure at any time during a step, large compensatory motions are usually needed to avoid falling. The margin of safety may be quantified by the difference between peak-to-peak lateral displacements of the COP and COM. In the control conditions, this margin was 0.08870.023L for preferred width walking and 0.00670.009L for prescribed zero width walking. The margin of safety for lateral COM motion therefore 833 decreases by 94% (p ¼ 3:9 107 ) when walking at zero step width. The preferred step width appears to depend on tradeoffs between active stabilization, step-to-step transitions, and lateral limb motion. The step width preferred by humans does not minimize lateral motion of the COM. Minimization of COM displacement in the vertical and lateral directions has been hypothesized to reduce the energetic cost of walking, with ‘‘six determinants of gait’’ that help to achieve this minimization (Saunders et al., 1953). However, we found that even in the control conditions, the metabolic cost of walking increased by 7.4% when walking with narrower steps even though subjects reduced their lateral COM displacement by 85%. Our mechanistic interpretation is that metabolic cost is not determined by COM displacement per se, but rather by the work performed to redirect the COM (Donelan et al., 2001), to which COM displacement bore a rough correlation. Factors, such as lateral limb motion, also contribute to the higher metabolic cost of narrow walking (without external stabilization), making COM displacement a poor predictor of energy expenditure. Our conclusions are subject to several experimental limitations. First, our protocol required subjects to walk with their arms crossed, which may be less stable than normal walking, perhaps magnifying the effect of external stabilization. Second, components of the external stabilizer unavoidably dissipate energy, thereby increasing the positive work required of our subjects. This disadvantage acts to reduce, rather than amplify, the differences we observed. Third, the external stabilizer may produce unwanted forces in the vertical or fore-aft directions. We estimate that these non-lateral forces are small (see Section 2). Finally, the stabilizer might reduce metabolic cost by providing a moment about the hip that would act to support the trunk. To prevent this, the stabilizer forces were applied with a line of action passing very close to the hip. These limitations may have a slight effect on our quantitative findings but we feel that they are insufficient to affect our main conclusions. In addition to providing stabilizing forces, our external lateral stabilizer may have a secondary effect of providing subjects with additional sensory feedback of lateral motion. The device applies forces to the waist proportional to the lateral position of the COM. Cutaneous receptors could potentially sense these forces, increasing the information available to the CNS for estimating COM motion. Just as reduced vision results in increased step variability (Bauby and Kuo, 2000), augmented feedback from lateral forces could be partially responsible for the observed decreases in step variability. However, if this were the case we would have expected a learning effect as subjects gained experience with these lateral forces and incorporated ARTICLE IN PRESS 834 J.M. Donelan et al. / Journal of Biomechanics 37 (2004) 827–835 them into their control strategy. Instead, subjects showed an immediate and consistent decline in step variability and metabolic cost. External lateral stabilization decreased both step width and step length variability. We focused on step width variability because medio-lateral foot placement is an indicator of active control of lateral balance. But some changes in step length variability are also to be expected because in human walking there is a coupling between medio-lateral and fore-aft motion (Bauby and Kuo, 2000). Whether subjects were walking at the prescribed or freely selected step width, the decreases in step width variability exceeded those in step length variability. The ability to artificially provide lateral stability while walking may have applications in rehabilitation medicine. Partial body weight support is commonly used for patient groups lacking the strength to provide sufficient vertical forces (e.g. Hesse, 2001). External lateral stabilization could potentially be useful for patients that have the strength to support their body weight, but have difficulty controlling balance. By reducing the need for active feedback control, external stabilization could allow these patients to exercise, or to practice stabilizing strategies and other aspects of gait mechanics, with greater safety and confidence. Acknowledgements This research was supported in part by an NSERC fellowship to J.M. Donelan, NIH grant AR44688 to R. Kram and NIH grant DC0231201A1 to A.D. Kuo. These experiments were conducted at the University of California, Berkeley. In this equation, xk is the state of the system at the beginning of the kth step, and xkþ1 is the state at the beginning of the next step. A passive walking gait has states x (termed fixed points) for which, apart from switching support from the left leg to the right, each step is identical to the preceding one x ¼ f ðx Þ: ðA:2Þ Passive dynamic walking gaits typically have two limit cycles called long and short period gaits due to their difference in step period. We have restricted our study to the long period gait as it is most similar to human walking (McGeer, 1990). Stability is examined by evaluating the effect of small deviations about the fixed point, using a linearized approximation of Eq. (A.2) ðx x ÞEJðx Þðx x Þ; ðA:3Þ kþ1 where Jðx Þ ¼ k qf : qxk x ðA:4Þ The eigenvalues of the Jacobian matrix Jðx Þ determine whether or not a perturbation (xk 2x ) will be amplified or attenuated by the beginning of the next step. If it is amplified, the limit cycle is unstable. Conversely, if the perturbation is attenuated by the end of the first step, it will continue to shrink in subsequent steps—the system is locally stable and the passive dynamic walker will return to its periodic gait. The complex-valued eigenvalues must all be within the unit circle for the system to be stable. The corresponding eigenvectors describe modes along which the perturbations are decoupled from each other. References Appendix A This appendix summarizes our stability analysis of the passive dynamic walking model. These methods are standard techniques for determining stability in nonlinear dynamical systems (Strogatz, 1994), first applied to walking by McGeer (1990). A step by a passive dynamic walker is divided into single and double support phases. For single support, the equations of motion, subject to appropriate initial conditions, are integrated forward in time until the swing leg contacts the ground. This is followed by double support, modeled as an instantaneous, inelastic collision returning initial conditions for the next single support phase. These two phases are combined to form a vector-valued non-linear difference equation with the step-to-step function, f xkþ1 ¼ f ðxk Þ: ðA:1Þ Bauby, C.E., Kuo, A.D., 2000. Active control of lateral balance in human walking. Journal of Biomechanics 33, 1433–1440. Brockway, J.M., 1987. Derivation of formulas used to calculate energy-expenditure in man. Human Nutrition-Clinical Nutrition 41C, 463–471. Cavagna, G.A., 1975. Force platforms as ergometers. Journal of Applied Physiology 39, 174–179. Donelan, J.M., Kram, R., Kuo, A.D., 2001. Mechanical and metabolic determinants of the preferred step width in human walking. Proceedings of the Royal Society of London Series B-Biological Sciences 268, 1985–1992. Donelan, J.M., Kram, R., Kuo, A.D., 2002. Simultaneous positive and negative external mechanical work in human walking. Journal of Biomechanics 35, 117–124. Garcia, M., Chatterjee, A., Ruina, A., Coleman, M., 1998. The simplest walking model: stability, complexity, and scaling. Journal of Biomechanical Engineering 120, 281–288. Hesse, S., 2001. Locomotor therapy in neurorehabilitation. NeuroRehabilitation 16, 133–139. Kram, R., Griffin, T.M., Donelan, J.M., Chang, Y.H., 1998. Force treadmill for measuring vertical and horizontal ground reaction forces. Journal of Applied Physiology 85, 764–769. ARTICLE IN PRESS J.M. Donelan et al. / Journal of Biomechanics 37 (2004) 827–835 Kuo, A.D., 1999. Stabilization of lateral motion in passive dynamic walking. International Journal of Robotics Research 18, 917–930. McGeer, T., 1990. Passive dynamic walking. International Journal of Robotics Research 9, 62–82. McLean, J.A., Tobin, G., 1987. Animal and Human Calorimetry. Cambridge University Press, New York. Poole, D.C., Richardson, R.S., 1997. Determinants of oxygen uptake-Implications for exercise testing. Sports Medicine 24, 310–322. 835 Saunders, J.B., Inman, V.T., Eberhart, H.D., 1953. The major determinants in normal and pathological gait. Journal of Bone and Joint Surgery 35A, 543–558. Shipman, D., Donelan, J.M., Kram, R., Kuo, A.D., 2002. Metabolic cost of lateral leg swing in human walking. A presentation at the World Congress of Biomechanics in Calgary, Alberta, Canada. Strogatz, S.H., 1994. Nonlinear Dynamics and Chaos: With Applications to Physics, Biology, Chemistry, and Engineering. AddisonWesley, Reading, MA.