This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this
material constitutes acceptance of that license and the conditions of use of materials on this site.
Copyright 2011, The Johns Hopkins University and Adnan A. Hyder. All rights reserved. Use of these materials
permitted only in accordance with license rights granted. Materials provided “AS IS”; no representations or
warranties provided. User assumes all responsibility for use, and all liability related thereto, and must independently
review all materials for accuracy and efficacy. May contain materials owned by others. User is responsible for
obtaining permissions for use from third parties as needed.
Section C
Measuring Research Need and Research Investments:
Global Estimates and Dialogue
Population and BOD by Country Income Level, 2000
Low-middle
High
Population in thousands
(%)
4,976,748
(85%)
907,828
(15%)
Total DALYS (in
thousands)
(%)
1,274,259
(92%)
108,305
(8%)
3
The Burden of Disease by Group
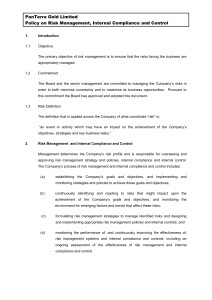
The burden of disease by group (DALYs/100,000 pop.), 2000
Low-and
middle-income
High-income
Comm. dis. (incl.
mat., perin., & nutr.)
11,206
863
Non-communicable
diseases
10,200
9,664
Injuries
4,198
1,403
4
Comparison of Groups of BOD: HICs, China, & Africa
5
Rationale
Health research is essential to the design and implementation of
health interventions, health policies, and health service delivery
Financing health research and development (R&D) is critical to its
success
Information on investments for health research, however, is
fragmented
6
Resource Flows for Health Research: First Estimates
Preliminary assessments done for the year 1992
US$56 billion invested annually in health research worldwide
R&D investments in diarrhea, pneumonia, and TB—about 20% of
global disease burden—totaled just 0.2% of global health
expenditure in 1992
7
The Problem Is …
Less than 10% of global research funds are invested in exploring
health problems affecting 90% of the world’s population … now
called the “10/90” gap in health research
Captures the huge discrepancy between the magnitude of disease
burden in the world and the allocation of research funding
These are estimates and the exact figures are not known
8
Second Estimates
Global health R&D funding for 1998 (in US$ billion)
Total
Percent
Advanced/transition
34.5
47
Developing
2.5
3
Pharma industry
30.5
42
Private non-profit
6.0
8
73.5
100
Public funds
Private funds
Total
9
R&D Estimates for Selected Developing Countries, 1998
R&D as %
of health
Brazil
1.2
Cuba
1.4
Costa Rica
1.08
Argentina
0.98
India
0.88
Malaysia
0.4
10
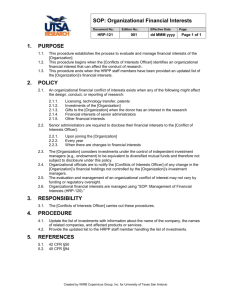
Health R&D as Percentage of GDP, 1998
Data Source: Global Forum for Health Research. (2001). Monitoring financial flows for health research.
11
Observations for 1998
In comparison with 1992, there seems to be an increase in total
research funds for 1998
Research on conditions accounting for highest burden still underfunded
Biomedical research well-funded vs. health economics and social
sciences research
12
Global Health Research Spending, 1990–2001
13
Third Estimate
Global health R&D funding for 2001 (in US$ billion)
Total
Percent
Public funds
44
Private for-profit
48
Private non-profit
8
Total
106
100
14
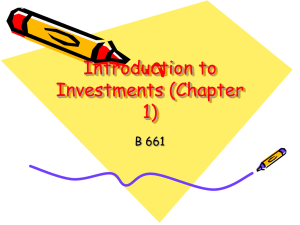
Global Distribution of R&D Expenditures, 2001
15
International Activities Funding, NIH
16
Global R&D 2001 (1)
US$106 billion includes the largest known contributors
Most of increase from 1998, in expenditures by the private sector,
was in HIC
R&D efforts of many low- and middle-income countries are still
largely unknown or unaccounted
Measuring is far from precise and there are still huge gaps in our
knowledge
17
Global R&D (2)
Gates was the top foundation in health-giving, at US$518.9 million
in 2001, focusing on diseases of highest burden worldwide
HICs have also increased their investments through Official
Development Assistance programs
Most of the spending done by high-income countries is in high
income-countries generating products tailored to health care
markets of high-income countries
A small share is funded and carried out by low- and middle-income
countries
18
Global R&D (3)
An even smaller share is funded by high-income countries but
carried out in and for the benefit of low- and middle-income
countries
In fact, few LMICs have met the target set by the 1990 Commission
of Health Research for Development of 2% of national health
expenditures on health R&D
Mexico, Cuba, India, and Brazil have met target
Even a small shift in budgets of LMICs to allocate more money for
health research that addresses the urgent health needs of their
populations could make a big difference
19
Public Funding of Health R&D
20
Global Investments in Health R&D
21
Resource Flows
Reflections on resource flows
22
Issues: 1
Global allocation for diseases not done collectively or uniformly
Relation between priorities in developing countries and funding
sources (national vs. international) is critical
Funding for social science, health economics and such research very
poor
23
Issues: 2
Cost of R&D to develop drugs and vaccines is immense—but “magic
bullet” effect
Fraction of public funds into fundamental research leading to a
marketed drug
Funding by developed countries to Northern institutions for R&D on
problems relevant to developing countries
24
Issues: 3
Institutional structures to focus attention on research investments
absent at global level
The “politics” of resources heavily influenced by clinical and visible
products
The social accountability of research investments not considered
Decision making at institutional and national levels not consistent
with priorities
25
Future Actions?
Concerted efforts needed to reduce global inequities in investments
in health and health research
-
HOW?
Reasonable for the poorest countries to concentrate health
resources on delivering health services and on research on
operational and health systems research
- TRUE?
26
Thanks To ...
Global Forum for Health Research
www.globalforumhealth.org
Dr. Andres DeFrancisco
Dr. Abdul Ghaffar
27