Lower Extremity Critiques -- File 03 AP Pelvis Image # 31
advertisement

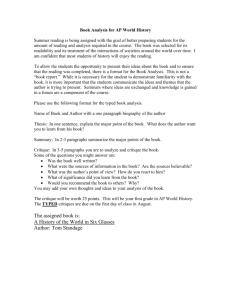
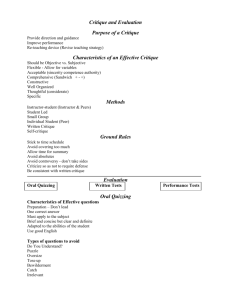
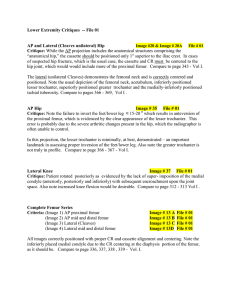
Lower Extremity Critiques -- File 03 AP Pelvis Image # 31 File # 003 Critique: Substantial rotation of the pelvis to/toward the patient’s right side. Note also the asymmetrical appearance of the ischial spine. The left ischial spine is not visualized, while the right spine is (greatly enlarged appearance). In addition to symmetry of the ischial spines, if visualized at all, to determine rotation, measure from the region of the patient’s ASIS, to the sacroiliac joint space (both sides). Due to the gross amount of rotation in this image, the measurement was obtained by measuring bi-laterally the inferior distance between the sacroiliac joint space yielding a difference of ≈ 4 cm. Wow! Compare to page 354-355 - Vol. I. Plantodorsal (axial projection) and Lateral Calcaneus Image # 3 File # 003 Critique: Correctly positioned plantodorsal (sufficient dorsiflexion) and lateral calcaneous demonstrating a fracture through the lateral process of the calcaneous. Also note that correct exposure factors were utilized. Note: since the plantodorsal and dorsoplantar projections have the same radiographic appearance, if performed correctly, you will not be required to differentiate between the two positions on film/slide tests. You will, however, be required to describe and explain the fundamental differences on the written portion of the test. Compare to pages 279, 280 281 - Vol. I. Plantodorsal (axial projection) and Lateral Calcaneus Image # 24 File # 003 Critique: The casted plantodorsal position demonstrates improper centering, as evidenced by the image’s placement an the top of the film. Also, the image fails to clearly demonstrate the subtalar joint space and the sustentaculum tali due to insufficient penetration. The lateral projection is correctly positioned and possesses ample penetration. Compare to pages 279, 280, 281 - Vol. I. Plantodorsal (axial projection) Calcaneus Image # 28 A & B File # 003 Critique: Image A demonstrates the effect when the CR is angled substantially greater than 40 0 . Note that the increased angulation in image A causes the fibula to encroach upon the sustentaculum tali and other structures distal to the joint space. In image B, (same patient), the CR angulation was corrected, causing the fibula to be positioned above the joint space, as it should be. Both projections demonstrate a comminuted fracture of the calcaneus. Ouch ! AP Standing Ankle Image # 125 File # 003 Ballinger-Vol., I pg 301 Critique: AP standing/weight-bearing ankle showing slight internal rotation. Note the lack of tissue space between the talus and the tibia, which is the purpose of this procedure. AP Ankle Stress Views Image # 143 File # 003 Critique: Properly positioned AP ankle showing stress applications of Valgus (outward stress) and Varus (inward stress). The purpose of Valgus and Varus is to show range of motion in the ankle joint. When Valgus exists in the knee joint, the patient is said to be “knock-kneed (genu valgum).” When Varus exists, the patient is said to be “bowlegged (genu varum).” Note: genu refers to the knee. Standing Feet (Lateral) Image # 119 & 119A File # 003 Ballinger - Vol. I, pg. 270 -271. Critique: Excellent positioning of the feet with the patients standing/weight bearing demonstrating loss of foot arch in 119B and moderate to normal arch in 119A. AP and Oblique Foot Image # 11 File # 003 Critique: Although the positioning is correct, the film orientation is incorrect, i.e., the cassette was transverse as opposed to being placed longitudinally with the long axis of the foot. AP Hip Image #120 File # 003 Critique: Lack of proper foot inversion. Note visualization of lesser trochanter. Also note splaying (flattening) of femoral head. Splaying is common in Legge-Perthes Disease (children) and in ischemic necrosis of bone (Bo Jackson Disease!) Splaying of femoral head probably contributed to the lack of foot/femoral inversion. Femur Image # 126 A File # 003 Image # 126 B File # 003 Image # 126 C File # 003 Critique: Correctly positioned distal lateral, AP proximal and distal AP. Note on image 126 A (Lateral) the presence of a large amount of callus, which indicates the healing process is well advanced. However, look at image 126 B (distal AP) and 126 C (proximal AP) and note that the healing process has been interrupted by re-fracture. In fact, the indwelling pin is also broken. The fractured callus is also seen on image 126 A.