Lower Extremity Critiques -- File 02 AP and Cleaves/Unilateral Hip Critique:
advertisement

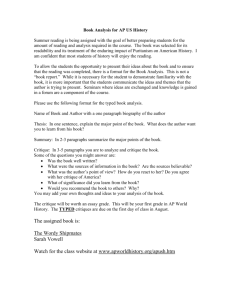
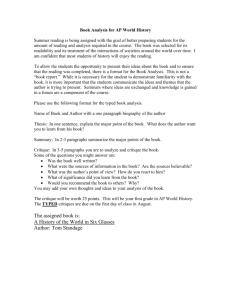
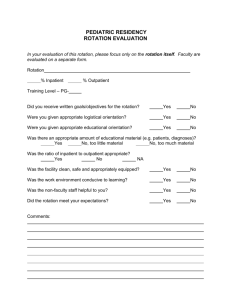
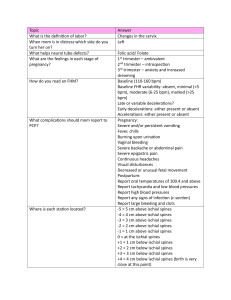
Lower Extremity Critiques -- File 02 AP and Cleaves/Unilateral Hip Image # 29 & Image # 29A File # 002 Critique: AP and lateral Cleaves appropriately centered and positioned. Projections demonstrate congenital hypoplasia (defective development of) with dislocation of the proximal femur. Note: letter A is an IUD. Compare to pages 362, 363 - Vol. I. Cleaves/lateral Hip Image # 16 File # 002 Critique: This pediatric case demonstrates an attempt to project the proximal femur laterally. Note that although there is slight part obliquity, there is no abduction of the proximal femur, and thus the femoral neck is not in profile. Obliquity of the body alone does not suffice for the expected unilateral cleaves position. In fact, does this film more closely resemble an AP rather than a lateral? Compare to page 363 & 365, Vol. I. AP Knee Critique: Light leakage covering ≈ 60% of the knee. Image # 4 File # 002 Transthoracic humerus Image # 14 File # 002 Critique: Other than body rotation, this film demonstrates an appropriately positioned transthoracic projection. Question: is this projection intended to demonstrate the distal humerus? Compare to page 174-175 - Vol. I. AP and Oblique Ankle Image # 17 File # 002 Critique: An appropriately positioned AP and Oblique ankle. Note the clearly defined ankle mortis due to separation of the talus and lateral malleolus despite the existing fracture and casting material. So how was dorsiflexion achieved in the oblique position ? The technique for resolving this dilemma will be discussed under special projections later in the semester. Compare to pages 290, 292, 293 - Vol. I. AP and Bi-lateral Cleaves Pelvis Image # 26 & 26 A File # 002 Critique: Both projections were taken to include a substantial amount of the proximal femur. Both images demonstrate off-centering to the left side of the patient’s MSP. In addition, both images demonstrate slight pelvic rotation to toward/to the patient’s right side, i.e., the ilia are asymmetrical. Compare to pages 354, 355 and 362, Volume I. Look closely at figure7-15 A & B page 355 ,and figure 7-24, page 362 and note the asymmetrical appearance. The aforementioned figures demonstrate rotation to the patient’s right side. Question, does the author note the rotation ? To determine rotation, measure from the region of the patient’s ASIS, to the sacroiliac joint space. In these images, the measurement difference is ≈ one cm. (Measure ranges from 12.5 on the right to 11.5/4 on the left). Typically, one can always identify rotation in this manner, and the side to which the patient is rotated is typically the side that measures the greatest, i.e., the side positioned downward will appear larger in the supine recumbent position. Would the aforementioned statement be true if the patient were prone ? No. Think about RAO versus LAO chests, abdomens, and which side is projected. Note: if the ischial spines are visible, (they are not always visualized) asymmetrical appearance of these structures would also indicate patient rotation to the side with the largest ischial spine. AP Pelvis Image # 2 File # 002 Critique: This image demonstrates a correctly positioned AP pelvis. There is minimal off\centering to the left of the patient’s MSP. Note the ischial spines not visualized, as they may not always be. Compare to page 365-355 - Vol. I. AP Pelvis Image # 1 File # 002 Critique: The cassette is clearly not one inch above the crest as it should be. This centering error results in minimal demonstration of the proximal femur. Also note the rotation of the patient to/toward his/her left side, as indicated by a slight increase in the width of the left ilium. Once again, to determine rotation, measure from the region of the patient’s ASIS, to the sacroiliac joint space (both sides). In this image, the measurement difference is ≈ 2 cm. Also note that the ischial spines are not visualized, which is probably normal for this patient. Compare to page 354 -355 - Vol. I. AP Pelvis Image # 15 File # 002 Critique: Note that there is substantial rotation to the patient’s left side, as evidenced by the larger left ilium (asymmetrical ilia, which were not measured). Also note that in this patient, the ischial spines are clearly visible, and the left ischial spine appears substantially larger (asymmetrical ischial spines), further indicating left-sided rotation. Once again, the ischial spines (if visualized) and the ilia should be symmetrical. Also note the image is not positioned vertically one inch above the ilium, on the left side. Compare to page 3354-355 - Vol. I.