INTERACTIVE PHOTOTHERAPY JUL 01 2015
advertisement

PHOTOTHERAPY
INTERACTIVE
INTEGRATING PHOTOMEDICINE
INTO INTERACTIVE ARCHITECTURE
by
ARCHNES
PHILLIP HAMPTON EWING JR.
MASSACHUSETTS INSTITUTE
OF TECHNOLOLGY
Bachelor of Architecture
Auburn University, 2012
JUL 01 2015
LIBRARIES
Bachelor of Interior Architecture
Auburn University, 2012
Submitted to the DepartmentofArchitecture in PartialFulfillment of the Requirementsfor the Degree of
MASTER OF SCIENCE IN ARCHITECTURE STUDIES
at the
MASSACHUSETTS
INSTITUTE OF TECHNOLOGY
June
2o,5
2015
Massachusetts Institute of Technology. All rightsreserved.
The author hereby grants to MITpermission to reproduce and to distributepubliclypaperand electroniccopies
of this thesis document in whole or in partin any medium now known or hereaftercreated
SIGNATURE OF AUTHOR:
Signature redacted
-------------------Department of Architecture
March 31, 2015
CERTIFIED BY:
Signature redacted-Kent Larson
PrincipalResearch Scientist
Thesis Supervisor
Signature redacted
ACCEPTED BY:
/V
Takehiko Nagakura
Chairof the DepartmentCommitteefor GraduateStudents
Thesis Supervisor: Kent Larson
Title: Principal Research Scientist, Media Laboratory, Massachusetts
Institute of Technology
Thesis Reader: Takehiko Nagakura
Title: Associate Professor, Department of Architecture, Massachusetts
Institute of Technology
Thesis Reader: Dennis Shelden
Title: Associate Professor of the Practice in Computation, Department of
Architecture, Massachusetts Institute of Technology
2
Interactive Phototherapy: Integrating Photomedicine into
Interactive Architecture
by
Phillip Hampton Ewing, Jr.
Bachelor of Architecture
Auburn University, 2012
Bachelor of Interior Architecture
Auburn University, 2012
Submitted to the DepartmentofArchitecture on March 31, 2015 in PartialFulfllment of the Requirements
for the Degree of Master of Science in Architecture Studies
Abstract
This thesis proposes both a physical platform and analytical model for implementing phototherapy
in the context of architectural space and dynamic user behavior. By doing so, a number of problems
across the fields of (i) healthcare innovation, (2) self-tracking or the "quantified self," and (3)
interactive architecture would be solved. First, if healthcare systems are to gain greater insight into a
number of conditions that are difficult to diagnose or treat, then passive monitoring and treatment
methods must be expanded and improved. Second, if self-tracking devices are to become more
accurate in monitoring and informing user health, then more contextual information about user
positions and activities with reference to space are needed. Third, if interactive architectural systems
are to have continuing relevance, then truly novel applications for augmenting the function of
spaces must be explored. The development of a so-called "interactive phototherapy" would provide
solutions by (i) increasing patient compliance to phototherapy regimens compared to more
conventional methods, (2) improving the accuracy of monitoring information relevant to user
health, and (3) expanding the functionality of architectural spaces to novel applications.
Interactive phototherapy - a user interaction-oriented approach to phototherapy - is developed
in three parts. First, we develop the CityHome, a project of the Changing Places group in the MIT
Media Laboratory, as a physical platform capable of meeting technical prerequisites for the
implementation of interactive phototherapy. Second, we explain a methodology for analyzing
interactive phototherapy that is accessible to architectural designers and related practitioners.
Third, we apply this methodology to evaluating hypothetical user interaction scenarios that may
occur in the CityHome.
3
4
Acknowledgem e nts
I would first like to thank the members of my thesis committee for
their support throughout the development of this project. A
special thanks to Kent Larson for graciously offering the
opportunity to work alongside the Changing Places group in the
MIT Media Laboratory on the development of the CityHome
project. Prior to the development of this project, I had the
opportunity to participate in a course instructed by Dennis
Shelden on a course concerning architecture and the Internet of
Things (IoT) - a course that was particularly helpful in the
formulation of some of the ideas contained in this book. In
addition, a thanks to Takehiko Nagakura for feedback and support
leading up to and at key moments throughout this project.
I would also like to thank my colleagues in the Design
Computation and Changing Places groups for their feedback
throughout this project.
A special thanks to Cynthia Stewart for answering questions and
resolving issues for the final submission of this book.
Finally, I would especially like to thank my parents, Phillip (Sr.)
and Angela Ewing, for their ongoing support leading up to
throughout both this project and my time at MIT.
5
6
TABLE OF CONTENTS
A bstract .......................................................................................... 3
A cknow ledgem ents ........................................................................... 5
1 / Introduction .............................................................................. 11
1. 1 Thesis Statem ent ................................................................................................................. 11
1.2 Research M otivations .......................................................................................................... I I
1. 3 Previous W ork .................................................................................................................... 12
1.4 Proposal .............................................................................................................................. 17
2
Light and M edicine .................................................................... 21
2.1 Overview ............................................................................................................................. 21
2.2 W avelength ......................................................................................................................... 21
2.3 Units of M easurement ......................................................................................................... 22
2.4 Emission Properties ............................................................................................................ 24
2.5 Eye Sensitivity to Light ........................................................................................................ 25
2.6 Physiological Responses to Light ......................................................................................... 26
2.7 Implem entation .................................................................................................................. 29
2.8 Discussion ........................................................................................................................... 31
3 / The C ityH orne Project ................................................................. 39
3.1 Overview ............................................................................................................................. 39
3.2 Contributors ....................................................................................................................... 39
3.3 Background ......................................................................................................................... 39
7
3.4 Spatial Configuration .......................................................................................................... 40
3.5 Structural/M echanical Configuration ................................................................................. 46
3.6 User Interfaces .................................................................................................................... 46
3.7 Software/Hardware Details ................................................................................................. 49
3.8 Discussion ........................................................................................................................... 50
4
Calculating Phototherapy ............................................................ 53
4.1 Overview ............................................................................................................................. 53
4.2 Background ......................................................................................................................... 53
4.3 Existing Lamp ..................................................................................................................... 55
4.4 Calculating Illuminance ...................................................................................................... 57
4.4.1 Falloff ........................................................................................................................ 57
4.4.2 Angle of Emission ...................................................................................................... 58
4.4.3 Angle of Incidence ..................................................................................................... 62
4.4.4 1 mplementatio n ......................................................................................................... 64
4.5 Illuminance to Irradiance .................................................................................................... 67
4.6 Irradiance to Dosage ........................................................................................................... 69
4.7 Discussion ........................................................................................................................... 71
5
Designing Phototherapy .............................................................. 75
5.1 Overview ............................................................................................................................. 75
5.2 Design Development ........................................................................................................... 75
5.2.1 Linear Array ............................................................................................................... 75
5.2.2 Area Array .................................................................................................................. 78
5.3 Scenario A: W aking ............................................................................................................. 80
5.3.1 Setup Param eters ....................................................................................................... 82
5.3.2 Lying in Bed ............................................................................................................... 82
5.3.3 Sitting on Sofa ............................................................................................................ 84
5.4 Scenario B: W ashing ............................................................................................................ 85
5.4.1 Setup Param eters ....................................................................................................... 87
5.4.2 Showering .................................................................................................................. 87
5.4.3 Brushing Teeth .......................................................................................................... 88
5.5 Scenario C: Working ........................................................................................................... 89
5.5.1 Setup Param eters ....................................................................................................... 91
5.5.2 Sitting at Desk ............................................................................................................ 91
5.5.3 Reading on Sofa .......................................................................................................... 92
5.6 Discussion ........................................................................................................................... 93
6 / C onclusio n ............................................................................... 97
6.1 Sum mary ............................................................................................................................. 97
6.2 Further Research ................................................................................................................. 99
6.3 Concluding Rem arks ......................................................................................................... 101
A ppendix ...................................................................................... 103
Figures .................................................................................................................................... 103
Tables ..................................................................................................................................... 105
Figure References .......................................................................... 109
Bibliography ................................................................................. III
10
1I
INTRODUCTION
1.1 Thesis Statement
Phototherapy can be deployed as an interactive, user-oriented system at the architectural level in
order to more effectively improve our health and promote wellness. In doing so, this so-called
interactivephototherapywould be a solution to needs across the fields of (i) healthcare innovation,
(2)
self-tracking, and (3) interactive architecture. First, if healthcare systems are to gain greater
insight into a number of conditions that are difficult to diagnose or treat, then continuous, noninvasive monitoring and treatment methods that can be readily deployed outside of clinical
environments are needed. The emerging self-tracking or "quantified self" paradigm is one example
of a category of tools poised to meet this need. Second, if self-tracking systems are to acquire more
accurate, reliable data, then contextual information about a user's position, condition and/or
activities are needed to supplement raw sensor data. The emerging paradigm of interactive
architecture has an interest in developing tools that monitor and respond to information about a
user's position, condition and/or activities within a space. Third, if interactive architectural systems
are to have continuing relevance, then truly novel applications for augmenting the function of
spaces must be explored. Healthcare innovation would be an example of a relatively unexplored
application in interactive architecture. Thus, there is a loop of interdependencies between the fields
of healthcare innovation (HI), the quantified self (QS), and interactive architecture (IA) for which a
form of interactive phototherapy could be a solution.
1.2 Research Motivations
Light, in the form of phototherapy, happens to be a particularly convenient modality for promoting
user health - although it is by no means the only modality suitable for the task. With regards to
medicine, light is arguably one of the least invasive mediums at hand. For example, the use of pulse
oximetry for measuring blood oxygen (02) saturation - as well as estimating heart rate and blood
pressure - has become standard use in clinical settings. The monitoring equipment involved is
relatively simple: a small wearable device containing a light sensor and a pair of light sources, which
is then applied to the skin. With regards to self-tracking, modified versions of the same technology
can be (and have been) integrated into commercial wearable devices for monitoring heart rate
throughout the day. With regards to interactive architecture, we could easily imagine information
from light-based medical or self-tracking devices being transmitted to building environmental
11
control systems to modulate some relevant condition in a space - be it light, temperature, airflow, or
some other phenomenon. Thus, the deployment of light as a medical device has advantages due to
the relative simplicity of the equipment that may be involved.
In contrast, the connotations of light in architectural discourse are deep, complex, and
profound; they quickly launch off into lofty philosophical, phenomenological, psychological, and
(eventually) practical considerations that are fundamental to architectural theory and practice. No
beginning architecture student goes for long without hearing one of their professors deliver a
lengthy exegetical lecture on what the revered
2 0 th
century architect Louis Kahn meant when he
said: "All material in nature [is] made of Light which has been spent, and this crumpled mass called
material casts a shadow, and the shadow belongs to Light."' If not Kahn, then perhaps we could
substitute one of his contemporaries, Le Corbusier: "Architecture is the learned game, correct and
magnificent, of forms assembled in the light." 2 And if not Le Corbusier, we can substitute one of any
number of influential architectural theorists and philosophers going all the way back to Vitruvius.
On the other hand, the practical considerations are somewhat more explicit and concrete. There are
required illumination levels required for various spaces, depending on function; there are building
orientation and daylight factors to consider; there are lighting fixture types, quantities,
configurations, and so on. It would be impossible to adequately give voice here to the full variety of
perspectives on the role of light in architecture, but these examples may give a hint at the larger
picture. It seems fair to say that the discipline of architecture is deeply concerned with how the
selective deployment of light may add both subjective and objective value to space, and there is little
reason to think that the deployment of light in the form of interactive phototherapy cannot align with
those motivations.
1.3 Previous Work
Medical knowledge of the potentially therapeutic properties of light is actually quite old, but there
have been a number of technological improvements over time. Phototherapy using natural sunlight,
also known as heliotherapy, is said to have been practiced in ancient Egypt, Greece, and Rome,
among others. Research into modern phototherapy, however, did not develop until the late
19th
century. The Faroese physician Niels Finsen is considered to be the father of modern phototherapy.
In 1903, he received the Nobel Prize in Physiology or Medicine for his work on the use of artificial
light to treat conditions such as lupus vulgaris and smallpox. Over the following century, numerous
methods and applications of phototherapy have been developed; various techniques may include
(Lobdell,
2
2008)
(Le Corbusier, 2007)
12
multi-spectrum therapy, monochromatic therapy, or low-level laser therapy. Another technique,
photodynamic therapy, uses phototherapy in combination with photoactive compounds. In addition
to the visible light spectrum, ultraviolet and near infrared light may be used, depending on the
application. The conditions that may be treated with phototherapy cover a broad range and includes
(but is not limited to) circadian rhythm disorders, hair growth (or removal), skin conditions, pain
management, and accelerated wound healing.
Challenges with phototherapy as a medical tool largely involve user and/or device compliance.
First, phototherapy lamps are designed to deliver a specific level of illumination at a fixed distance.
Head or body movements may take the user out of the therapeutic range of the light, thus reducing
the effectiveness of treatment. This problem is exacerbated with the use of smaller lamps, which in
turn have tighter therapeutic ranges. Second, the user may not use the phototherapy lamp for the
appropriate amount of time; if the user gets up too soon, the necessary fluence or dosage may not yet
have been achieved. On the other hand, longer exposure times are not necessarily better. Many
conditions are known to exhibit a biphasic dose response to phototherapy; past a certain point,
prolonged exposure may generate diminished or even negative effects. Thus, the user must use the
phototherapy lamp at the right distance for precisely the right amount of time. Third, variations in
the performance of the lamp may also potentially negatively impact phototherapy effectiveness.
Some artificial light sources may undergo a non-negligible decline in output over months or years of
use. In response, some lamps may incorporate sensors and systems that self-monitor light output and
increase power accordingly. Finally, there is still room for design innovations that make
phototherapy usage in general more convenient. An example of such innovation in a clinical setting
is the Firefly phototherapy lamp (Fig. i.),I a "cost-effective, intuitive phototherapy device designed
Fig. 1.1: Firefly phototherapy lamp.
3 (Design
that Matters, 2014)
13
to treat newborns with mild to severe jaundice in low-resource settings." By making a lamp compact
enough to install in a mother's recovery room, the lamp proposes to promote in-hospital
breastfeeding by the mother, as well as reduce staff workload associated with bringing a mother to a
neonatal intensive care unit or monitoring a mother and newborn in separate locations. In short,
there is room for improving the actual implementation of phototherapy in addition to further
developing the underlying science.
With regards to the quantified self and the larger "user wellness" paradigm, there have been a
number of applications and devices that operate on principles related to phototherapy. For example,
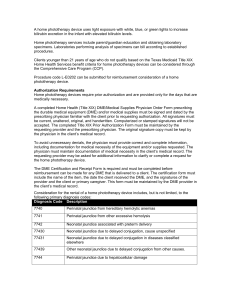
flux (Fig.
1.2a)
4
is a computer application that adjusts the color and brightness of a computer screen
according to the time of day and location. In doing so, the application aims to reduce eye strain and
circadian rhythm or sleep disruption during evening hours. A more speculative art/architecture
project, i-weather (Fig.
I.2b)5
is a website and computer-based application that uses the computer
screen as an "artificial sun" that oscillates between alertness-stimulating blue and non-stimulating
orange light over a
25
hour, 7 minutes, and 40 seconds period. This, in turn, aims to allow users to
synchronize their circadian rhythms to an artificial cycle that is independent of their geographic
location, a useful feature for overcoming sleep disruptions due to airplane travel and "extra-
Fig. 1.2: flux (a), i-weather (b), iluMask(c), and SunSprite (d).
4
5
(Herf & Herf, 2009)
(Philippe Rahm Architects & fabric I ch,
2001)
14
terrestrial trips and holidays." Based on phototherapy used by dermatologists in clinical settings,
illuMask (Fig. I.2c) 6 aims to allow users to eliminate facial acne at home by wearing a light therapy
mask for 15-minutes per day. illuMask uses LEDs to radiate red and blue light, wavelengths known in
the medical literature to have some effectiveness in reducing acne. SunSprite (Fig.
7
I.2d)
is a
wearable monitor and corresponding application that monitors the amount of sunlight (visible and
ultraviolet) a user receives over the course of a day. By tracking and informing users about their light
exposure relative to a daily goal, the tools aims to help users improve light-related conditions such as
circadian rhythm disorders and some forms of depression.
Although all of the aforementioned applications have merit and may be potentially helpful, it is
also possible to imagine potential room for improvement upon each tool. First, the effectiveness of
flux in adjusting the color temperature of a computer screen for promoting sleep hygiene is
potentially irrelevant if ambient light in the room is still disruptive. Indeed, there is some common
sense on the part of a user that is expected - if the user cares enough about circadian rhythm
disruptions to download a program to minimize them, then they will probably also care enough not
to keep all the lights on at full blast in the evening hours. In short, it would be interesting to see
operation principles similar to flux applied not only to computers, but integrated into all of the
other lamps in an interior environment - i.e., "smart lights." Second, the interoperability of iweatheracross different devices (indeed, any device that has an internet connection) raises questions
about its effectiveness in regulating circadian rhythm - in particular, with stimulating alertness
within a given exposure time. Specifics about the screen size and brightness of the device running iweather are not known to the application, nor are specifics about the user's distance from that screen
known. Without these parameters, how is it possible to know if the application is providing sufficient
stimulation to promote alertness within a given time frame? In defense, we do know that the
brightness of a smartphone screen in the evening is sufficient enough to disrupt sleep. Even so, it
would be interesting if more nuanced information about dosage parameters could be integrated into
the application. Third, the anti-acne version of illuMask has been shown to be at least as effective in
FDA studies as a certain "predicate device." An alternate anti-aging version of the mask, however, is
completely opaque and lacks a viewport - a decision that prohibits carrying out other activities
during the therapy session and potentially discourages user compliance. Of course, the apparent
concern is the need for eye protection from LEDs in close proximity to the eye. Even so, one is still
left to wonder whether there are ways to accommodate this need in a way that isn't as disruptive.
Finally, presuming SunSprite carries out sunlight monitoring to a reasonable level of accuracy, there
is a question of the interoperability of the data collected. One concern that may or may not apply to
6
(La Lumiere, LLC)
7 (GoodLux Technology, 2014)
15
SunSprite that has been noted across many self-tracking devices and applications is that the
information collected is stored in a format proprietary to that application. Thus, data from one
application becomes difficult to cross-compare to data from another application to generate more
nuanced, holistic information about user health. Although it is not clear from the available literature
whether SunSprite stores data in a proprietary format, a concern going forward for similar
applications would be promoting the accessibility of collected data to other applications.
06
00
(b 24
12
0
20
(b)
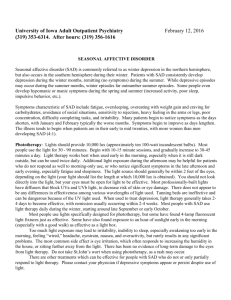
Fig. 1.3: Paimio Sanatorium by Alvar Aalto (a), "sombrero" plot visualization (b).
Specific contributions from the paradigm of interactive architecture to phototherapy are not
completely clear yet; there is, however, evidence of concern for the health benefits of light in the
larger discipline of architecture. In fact, there was once an entire category of architecture dedicated
to the pursuit of plentiful sunlight and clean air to improve occupant health: the sanatorium. In the
early 2oth century before the development of antibiotics, medical rationale dictated that plenty of
sunlight, fresh air, rest, and good nutrition could be used to jumpstart a patient's immune system in
overcoming pulmonary tuberculosis - a rationale that still makes sense, opposed to alternative
conditions of the time. One of the most notable examples of sanatoria would be the Paimio
Sanatorium in Finland (Fig. I-3a), designed by Finnish architect Alvar Aalto and completed in 1932.
The facility featured long roof terraces for sunbathing, as well as custom fixtures and furniture
specifically geared toward user health and comfort during stays which could last as long as several
years. In more recent times, the Center for the Built Environment (CBE) at the University of
California - Berkley has conducted extensive research to evaluating how occupants respond to the
indoor environmental quality of buildings." Much of this research has involved daylighting
performance in commercial buildings, and has yielded direct correlations between access to daylight
and worker satisfaction and productivity: more (controlled) daylight, happier employees. Building
on this trajectory of thought, others have sought to quantify the effects of lighting in spaces on
8 (Center For the Built Environment)
16
regulating biological functions. 9 A "sombrero" plot may be used to characterize the cumulative
effects of ambient light at a certain point on regulating circadian rhythm (Fig. i. 3 b). A series of
concentric rings are divided into quadrants, with each quadrant representing a particular view
direction; inner rings correspond to earlier parts of the day. The shading of each ring quadrant
corresponds with the relative potential of light from a particular direction and time of day to affect
circadian rhythm. Another paradigm for analyzing space in terms of health impact is that of
evidence-based design (EBD). Evidence-based design emphasizes the use of research and postoccupancy evaluations to influence design decisions. This has become a particularly popular with
regards to healthcare design, and much of the evidence confirms research and approaches to lighting
design from the other categories discussed. In summary, it is important to emphasize the fact that
the research with regard to architectural lighting and health is (i) still ongoing and therefore
incomplete to a certain extent, and (2) can only serve as guidelines to design, as opposed to explicit,
prescriptive rules.
1.4 Proposal
This thesis will explore the potential for interactive phototherapy, the convergence of
phototherapy and interactive architecture; in order to do so, we will first need to explicitly define
some terms. The Oxford English Dictionary defines phototherapy quite succinctly as: "The use of
light in the treatment of physical and mental illness." Given that the field of phototherapy is
relatively well-established in the medical discipline, this definition will suffice for our purposes. On
the other hand, interactive architecture is a relatively new paradigm in the context of architecture, a
paradigm that is heavily linked to the proliferation of computing technology. Michael Fox and Miles
Kemp, in their book InteractiveArchitecture,describe it as "built upon the convergence of embedded
computation (intelligence) and a physical counterpart (kinetics) that satisfies adaptation within the
contextual framework of human and environmental interaction."'
To clarify, physical mechanisms
devoid of an underlying form of "intelligence" cannot be described as interactive architectural
systems. Conversely, digital media projects that happen to use physical display devices are not
sufficient for this definition, either. Next, Fox and Kemp goes on to echo Usman Hasque in
emphasizing that interactive architecture must by definition be a two-way exchange with regards to
user interaction: "A truly interactive system is a multiple-loop system in which one enters into a
conversation: a continual and constructive information exchange."" Thus, we will define interactive
phototherapy as a system that (i) uses light,
Mardaljevic, & Lockley,
(Fox & Kemp, 2009, p. 12)
"(Fox & Kemp, 2009, p. 13)
9 (Andersen,
2012)
(2)
treats physical and/or mental illness, (3) is a physical
mechanism, (4) has embedded "intelligence", (5) is in continuous interaction with a human user,
and (6) operates within an environmental context.
With these definitions in place, we can define the structure of this thesis. In Chapter 2, we will
explore to some of the basic principles of light as they may apply to phototherapy. Physical units of
measurement, physiological effects of light on the body, andvarious methods of phototherapy will be
discussed. In Chapter 3, we will examine the CityHome, a project of the Changing Places group in
the MIT Media Laboratory, as a physical platform for interactive phototherapy. In the process of
developing this thesis, I had the opportunity to collaborate with a team of researchers within the
Changing Places group as an architectural designer for the project. This provided an opportunity to
demonstrate that the physical systems necessary for interactive phototherapy are feasible with
current technologies, as will be explored further. In Chapter 4, we will develop methods for
calculating the effectiveness of interactive phototherapy, using information about an existing
phototherapy lamp as a reference case. The result will be an explicit set of equations for calculating
the phototherapy dosage given off by a lamp with respect to a user's location in space and time
elapsed. In Chapter 5, we will propose a phototherapy installation scheme as an "add-on" for the
CityHome project and analyze the performance of this scheme under various hypothetical user
interaction scenarios. The performance and possible adjustments to the lighting scheme for each
scenario will also be discussed. In Chapter 6, we will conclude with a summary and discuss potential
directions for further development of interactive phototherapy.
The contributions of this thesis will be twofold: the demonstration of a physical prototype as a
platform, and the development of calculation methods for design and analysis purposes. We should
clarify that none of the supporting material for these contributions, whether they be physical
technology or mathematical equations, is actually new. What is (hopefully) new, however, is the realignment of this material in a new context: a vision of phototherapy (and healthcare, by extension)
serving a passive, intelligent, and continuous role in our day-to-day lives.
Works Cited
Andersen, M., Mardaljevic, J., & Lockley, S. W.
(2012).
A framework for predicting the non-visual effects of
daylight - Part I: photobiology-based model. Lighting Research & Technology, 44, 37-52.
Center For the Built Environment. (n. d.). Centerforthe Built Environment. Retrieved December 2014, from
Center for the Built Environment: http://www.cbe.berkeley.edu/
Design that Matters. (2014). Firefly- Design that Matters. Retrieved December 2014, from Design that
Matters: http://www.designthatmatters.org/firefly/
Fox, M., & Kemp, M. (2009). Interactive Architecture. New York: Princeton Architectural Press.
GoodLux Technology. (2014). Wearable Sun & Light Tracker. Retrieved December 2014, from SunSprite:
https://www.sunsprite.com/tracklight/
Herf, M., & Herf, L.
(2009,
Februrary).
f lux. Retrieved
February 2014, from f.Hux: software to make your life
better: https://justgetflux.com/
La Lumiere, LLC. (n.d.). Light Therapy Mask I Anti-Wrinkle & Acne Treatment
I illuMask. Retrieved
December 2014, from illuMask: http://www.illumask.com/
Le Corbusier. (2007). Towards A New Architecture. (J. Goodman, Trans.) Los Angeles: Getty Research
Institute.
Lobdell,
J. (20o8). Between Silence and Light: Spiritin the Architecture ofLouis I.
Kahn (2nd ed.). Boston:
Shambhala.
Philippe Rahm Architects & fabric
I ch. (2001, October 26). i-weather.org - artificialclimate based on human
physiology. Retrieved December 2014, from i-weather: http://www.i-weather.org/
19
20
2 I LIGHT AND MEDICINE
2.1 Overview
The goal of this chapter will be to explain some (but certainly not all) of the guiding principles and
terminology regarding phototherapy. First, we will examine light in terms of its more independent
physical properties: wavelength, various units of measurement, and source-dependent emission
properties. Next, we will examine light in terms of how it affects the human body. This will include
discussion of both various visual and non-visual responses and mechanisms. Finally, we will discuss
basic categories and principles regarding the implementation of phototherapy, along with some of
its challenges.
2.2 Wavelength
+-
1024
1022
Y rays
I
I
io-' 4
10-'6
1020
I
10-12
1018
1016
io[4
XI rays
IUV
I
io~
0-1~I0
--- ~ - -
10'
1012
IR
:10~6
I
Increasin g Frequency (v)
108
FM
Microwave
I
104
I
106
100
102
I
v(Hz)
Long radio waves
A
RoA.o waves
10 2
le
102
100
Increasing
I
I
I
1o 4
106
108
Wavelength (k)
X(m)
-+
Visible spectrum
1
V
B
G
R
iy~ Yeoe
o
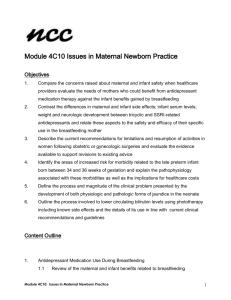
Figure 2.1: Electromagnetic spectrum with visible light highlighted.
We know that "light" refers to relatively narrow subset of electromagnetic radiation that is being
emitted at frequencies that are visible to the human eye (Fig. 2.1).' It is typically characterized as
having a wavelength within the range of 400 to 7oo nanometers (nm), but this is not considered to
be the absolute range of human vision. Some sources define the visible band to be as narrow as 420 to
'(Ronan & Gringer, 2013)
21
68o nm, 2 while others have observed it to be as short as 310 nm 3 or as long as
controlled laboratory
conditions.
The International
1050
nm 4 under
Commission on Illumination (typically
abbreviated as CIE for CommissionInternationalede l'Eclairage,its French name) defines the visible
light spectrum to be from 380 to 78o nm by way of its luminosity function, which will be discussed
later. The International Standards Organization (ISO) has also published standards on various
spectral categories for electromagnetic radiation in general. An important distinction to be made is
that these categories do not always correspondwith the perceived 'color' of an object or light source,
due to reasons involving the human eyes. For the purposes of this thesis, we will adopt the ISO 21348
definition (Table 2.1) for visible light spectral categories, but perform analyses over the CIE standard
visible spectrum.
Table 2.1: ISO 21348 Spectral Categories
Sub-Category
Category
Ultraviolet (UV)
Visible (VIS)
UVC
100 -280
UVB
280 -315
UVA
315 -400
Violet
380 -450
Blue
450 -500
Green
500 -570
Yellow
570 -591
Orange
591 - 610
Red
610-760
Near Infrared (NIR)
Infrared (IR)
Wavelen gth range (nm)
Middle Infrared (MIR)
Far Infrared (FIR)
760
-1
400
1 400 -3 000
3 000 -1 000 000
2.3 Units of measurement
Light is typically quantified in two alternative sets of SI (abbreviated SI from French: le Systeme
International d'unitis) units: photometric and radiometric. Photometric measurements quantify
light in terms of a human observer's ability to see it, whereas radiometric units operate in more
general terms. It is possible to convert measurements between analogous measurements with the aid
2
(Laufer, 1996, p.
ii)
3 (Miyawa & Schulman, 2001, p. 187)
4 (Sliney, Wangemann, Franks, & Wolbarsht, 1976)
22
of a standardized function that models the human brightness sensitivity to different wavelengths,
which will be discussed later. Some of the most common units are summarized in the included tables
(Tables
& 2-3). To provide some point of reference for the photometry units - specifically
2.2
illuminance in lux (lx), as we will be using this quite frequently in later chapters - common outdoor
and indoor illuminance levels are included in the appendix (Tables A- 3 and A.4, p. 1o5)Table 2.2: SI Photometry Units
Quantity
Unit
Name
Symbol
Name
Symbol
Im . s
QV
lumen-second
Luminous flux
0t)V
lumen (= cd - sr)
Im
Luminous intensity
H,
candela (= lm/sr)
cd
Luminance
candela per square metre
Illuminance
lux (=lm/m
)
Luminous energy
Luminous emittance
lux(= m/m
2
cd/m2
2
)
lx
Luminous exposure
(1,
lux second
Luminous energy density
cop
lumen second per metre
Luminous efficacy
q
lumen per watt
Luminous efficiency
V
(unitless)
lx- s
lm -ms- m
3
Im/W
(unitless)
Table 2.3: SI Radiometry Units
Unit
Quantity
Name
Sym bol
Radiant energy
Qe
Oe
Radiant flux
Spectral power
oe;
Radiant intensity
I,
Name
Symbol
J
joule
W
watt
watt per metre
W/m
watt per steradian
W/sr
Spectral intensity
'e
watt per steradian per metre
W-sr-1.m-1
Radiance
Le
watt per steradian per square metre
W-sr-1-m-2
Spectral radiance
Le2 or Lev
Irradiance
Ee
Spectral irradiance
/
Radiant exitance
Radiant emittancc
Spectral radiant
exitance / Spectral
radiant emittance
watt per steradian per metre3 or
watt per steradian per square metre per hertz
watt per square metre
watt per metre3 or
watt per square metre per hertz
EeA or
Me
MeA or M.
watt per square metre
watt per metre3 or
watt per square metre per hertz
23
W/m3 or
W-m22-Hz-1
2
_Wi
W/m 2
W/M
W-m
or
-Hz
W/M
2
W/m3 or
W-m 2 -Hz 1
Quantity
Name
Unit
Symbol
Radiosity
J
Name
Symbol
watt per square metre
W/m 2
W/m
Spectral radiosity
Je,
watt per metre3
Radiant exposure
Radiant energy density
He
joule per square metre
J/m 2
0),
joule per metre3
J/m 3
3
2.4 Emission Properties
With the (partial) exception of lasers, most light sources cannot produce light at a single specific
wavelength; instead, output occurs over a range of wavelengths. We need some method of accurately
describing the compound wavelength characteristics of this light source. One way to do this is to plot
out each wavelength that is being emitted by a light source along with some definition of the strength
of each wavelength. We call this a spectral power distribution (SPD) curve: a plot of the absolute or
relative power of light at a given wavelength for all of the wavelengths in a light source. This is a
useful tool for characterizing additional information about the light source itself, especially when
comparing two light sources that are considered to be "white" in coloration.
What we consider to be a "white" light is another interesting topic to consider, since there are
many ways to define it. One way would be to say that an ideal white light source emits equal amounts
of power at all wavelengths over the visible spectrum. Indeed, it is possible for some specialized light
sources to very closely approximate this via filtering and a combination of light sources with known
SPDs, but this definition by and large is only theoretical when describing real-world light sources.
Another way is to concede that light is not emitted perfectly evenly by natural sources, but to still
describe a given light source in comparison to some equivalent "ideal" emitter. This idealized
emitter is known as a "black body" emitter (for reasons that are beyond the scope of this thesis), and
emits known spectral power distributions when such a body is heated to known temperatures. This is
where we get the term "color temperature" when referring to white light sources; generally
speaking, light sources with higher temperatures appear to be more "blue", and sources with lower
temperatures appear to be more "red." The CIE has also established a series of "standard
illuminants" that attempt to model commonly encountered sources of white light. Finally, we can
also attempt to quantify how accurately light tends to render the colors of various objects. A color
rendering index (CRI) for a light source attempts to do exactly this. A CRI value of ioo represents
sunlight (for sources with a color temperature of 5,ooo K - 21,ooo K) or a blackbody emitter (<5000
K), whereas light sources that reveal colors less effectively may even have negative values.
24
Light propagates in the form of transverse electro-magneticwaves; polarization describes the
orientation of the magnetic and electric field components of a particular light wave. Most light
sources tend to be completely non-polarized; all of the light waves from the source have a more or
less equal probability of propagating in any orientation. Linearly polarized light has its electric and
magnetic wave components oscillating in phase with one another. Circularly polarized light has the
two planes oscillating go
out of phase with one another. Elliptically polarized light has its two
component planes somewhere in-between being o -go out of phase. For circularly and elliptically
polarized light, the phase shift direction (forward or backward) of the waves (relative to linearly
polarized light) determines the spin direction, clockwise or counter-clockwise.
Coherence is a category of properties that describe the pattern of constructive and destructive
interferences that occur as light waves propagate. Temporal coherence describes the degree to which
light rays of the same wavelength oscillate "in-sync" with one another. In other words, the waves of
two light sources are temporally coherent if they have a constantphasedifference and have the same
frequency. Spatial coherence describes the degree of cross-correlation between two waves from a
light source at different points (in two dimensions). Spatially coherent light will have all of the waves
in a given plane oscillating at the same rate, over a large or (ideally) infinite span. Polarization
coherence is the degree to which the polarization angles of various light waves are synchronous.
Spectral coherence is the degree to which light rays of different wavelengths synchronize with each
other with respect to time. Spectrally coherent white light will produce distinct "pulses" as various
component wavelengths constructively and destructively interfere. Spectrally incoherent light will
produce a relatively uniform "noise" with respect to amplitude and time.
Finally, we should make a brief note on the property of collimation. Collimation describes the
degree to which rays from a light source are parallel to one another. A laser beam has a high degree of
collimation; conversely, a typical ceiling light has a very low degree of collimation.
2.5 Eye Sensitivity to Light
It is known that the retina of the human eye is composed of rod-like cells and three different types of
cone-like cells. It is also known that these cells have differing sensitivities to light. The rod cells have
a peak sensitivity of around 5o7nm. The three cone cell types - short- (S), medium- (M) and longwavelengths (L) - have peak sensitivities of approximately 420-440 nm, 534-545 nm and 564-580
nm, respectively.5'6 These sensitivity of the cone cells to light as a function of wavelength has been
used to define several mathematical models for quantifying human color perception. In addition, the
5 (Wyszecki
& Stiles,
6 (Hunt, 2004)
1982)
25
varying sensitivities of the rod and cone cells to light have been used by the CIE (and other
organizations) to define two primary modes for brightness perception (luminosity), phototopic and
scotopic. The scotopic luminosity function is a normalized curve that best corresponds to the
response of the eye under very low light levels. The sensitivity of the eye at the peak of this curve is
lm/W.7 The phototopic luminosity function best approximates the eye under "normal"
lighting levels. The peak sensitivity of the eye under these conditions occurs at 555 nm (green1700
yellow) is 683 lm/W.8
Given this information, the eye's overall perception of a light source's brightness is a weighted
sum of all of the wavelengths present in that source. The luminous flux and radiant spectral power
distribution of a light source are related based on the following equation:
F = 683 lm/W
f y(A)J(A)d
1t
(2.1)
0
where F is the luminous flux in lumens, J(A) is the spectral power distribution of the radiation
(power per unit wavelength) given in W/nm, y(A) is the phototopic luminosity function, normalized
(o-i) and dimensionless, and A is the wavelength in meters (m). This is the mathematically accurate
version of the conversion, but in reality Y(A) and J(A) are not continuous mathematical functions, but
a recorded table of values at predetermined wavelengths from experiments. More often, we may use
the following form of the equation:
780
F = 683 lm/W -
yG)J(A)
(2.2)
A = 380
The CIE
1931
phototopic luminosity function, the most commonly used standard for these
conversions, is only actually defined for wavelengths between 380 and 78o nm. Thus, we can set our
summation to be over that specific range.
2.6 Physiological Responses to Light
As we discussed briefly in Chapter i, the use of light exposure for medicinal purposes has quite a
lengthy history dating back to ancient civilizations such as Egypt, Greece and Rome.9 However, it
has not been until relatively recently that scientific research has validated many of these claims.
7 (DeCusatis,
8
1998)
(Stroebel & Zakia, 1993)
9 (Ellinger, 1957)
26
Since the turn of the
2 0 th
century, there has been a substantial amount of medical research
documenting the body's various photochemical, endocrine, and other physiological responses to
light at various wavelengths and exposure amounts. Many of the various biochemical chain reactions
that occur within cells, and their resultant macro-effects, have been documented; a few examples are
listed in the following paragraphs:
VIOLET
LIGHT (400-450
NM).
Although the color is often referred to as "blue", light from what we
would consider to be the violet portion of the spectrum has been used for a number of dermatological
purposes, with varying degrees of success. Some studies seem to indicate that violet light may be
effective for reducing acne.' 0 Propionibacteriumacnes (P. Acnes), the bacterium responsible for the
skin condition acne vulgaris, has an endogenic porphyrin-coporphyrin III that has a peak sensitivity
to light in the 415 nm range." At this time, however, there is not enough evidence yet to conclusively
recommend it as treatment for acne." There is also some research indicating that 420 nm light may
be a potential treatment for psoriasis, in combination with the use of the photosensitizing agent
salicylic acid in petrolatum." Violet and near-ultraviolet light may also be a treatment option for
atopic dermatitis (AD), also known as eczema. 4
BLUE LIGHT
(450-500
NM).
5
Blue light has a very broad range of documented physiological effects. A
key component in the body's non-visual responses to blue light are intrinsically-photosensitive
retinal ganglion cells (ipRGCs). ipRGCs are sensitive to blue light due to the presence of the
photopigment melanopsin.' 6 ipRGCs are not involved in vision, but they are connected via the
retinohypothalamic tract (RHT) to the body's "master" circadian clock, the suprachiasmatic nuclei
(SCN). In turn, the SCN regulates other circadian "clocks" throughout the brain, including those
associated with sleep-wake cycles, alertness, melatonin (the "go-to-sleep" hormone), cortisol and
core body temperature.' Both ipRGCs and rod and cone cells are involved in regulation of the SCN;
however, rod and cone cells are primarily involved in the onset of exposure to blue light, whereas
ipRGCs are responsible for a sustained signal to the SCN.' 8 In short, this means that prolonged visual
exposure to blue light results in reduced fatigue, increased alertness and increased cognitive
function.' 9 In addition, there is research that suggests that due to this increased cognitive function,
(Gold, Sensing, & Biron,
2011)
" (Arakane, et al., 1996)
12 (Titus & Hodge,
2012)
(Kleinpenning, Otero, van Erp, Gerritsen, & van de Kerkhof, 2011)
1(Becker, et al., 2011)
15 (Meduri, Vandergriff, Rasmussen, & Jacobe, 2007)
16 (Brainard, et al.,
2001)
(Hastings, O'Neill, & Maywood, 2007)
18 (Gooley, et al., 2010)
'3
'7
'9
(Rahman, et al., 2014)
27
blue light may influence areas of the brain involved in processing emotion and language.2 " Skin
exposure to blue light may start a series of biochemical reactions that result in the production of
nitric oxide (NO), a vasodilator and powerful pain reliever, and anti-inflammatory agent." In
addition, blue light irradiation therapy has become common practice for reduction of bilirubin levels
in infants with neonatal jaundice." These various non-visual physiological responses mean that blue
light - in moderation - may be used in a wide variety of conditions. A few include: seasonal affective
disorder (SAD), delayed sleep-phase syndrome (DSPS), other circadian disorders, minor pain relief,
and (when used appropriately) restoring overall "sleep hygiene."
GREEN LIGHT
(500-570
NM).
There is research indicating that green light may also be a potential
treatment for various circadian disorders, " particularly in older adults. This is due in part to the fact
that transmission of blue light to the retina becomes attenuated in older adults by the yellowing of
the lens;2 4 therefore, blue light therapy may be less effective. Further, if ipRGCs in the retina are
weak or sparse - as occurs in individuals with SAD - and blue light is being attenuated, then green
light may be used as a substitute for stimulating the retinohypothalamic tract via the rod and cone
cells. Since the eye has a greater sensitivity to green light than blue, adequate stimulation may still be
possible. At higher intensities, 532 nm light might have an effect on reducing cellulite (adipose
tissue) as an alternative to cosmetic surgery,
YELLOw
LIGHT
(570-591
NM).
25
At higher
but medical research is still ongoing.
(laser) intensities,
yellow light
- among other
colors/wavelengths - may be used for the selective destruction of vascular malformations, such as
spider veins.2 Oxyhemoglobin, the oxygenated form of hemoglobin found in red blood cells, absorbs
yellow light via photocoagulation.2 7 This allows for the selective destruction of vascular tissue and
prevents excessive damage or vaporization of other tissue.
ORANGE
LIGHT (591 -610 NM). Orange light and longer visible wavelengths (i.e., red light) may be used
for circadian maintenance in the evening hours. Unlike blue or green light, orange light does not
suppress the production of melatonin. Studies in permanent night-shift workers have shown that
wearing orange-tinted (blue-blocking) glasses or goggles at sunrise significantly improved the
20 (Vandewalle,
et al., 2010)
21 (Oplinder,
et al., 2013)
2
23
24
25
26
27
(Management of Hyperbilirubinemia in the Newborn Infant 35 or More Weeks of Gestation, 2004)
(Gooley, et al., 2010)
(Spector, 1982)
(Jackson, Roche, & Shanks,
2013)
(Anderson & Parrish, 1981)
(H6hmann, Waner, & Schwager, 1993)
28
quality of daytime sleep for these workers.,29 For healthy circadian cycles, this helps minimize the
chance of delaying or disrupting appropriate sleep onset times.
RED LIGHT
(61o - 760
NM).
Red light stimulates the compound cytochrome c oxidase, or CCO, a
"proton pump" in the mitochondria of cells.3 CCO has peak excitation wavelengths of 620 nm, 68o
nm, 76o nm, and 820 nm (infrared).31 32 Upon stimulation, CCO proton pumps become agents in a
chain reaction that produces the compound adenosine triphosphate (ATP), a form of "chemical
energy" for intracellular activity.33ATP, in turn, becomes the fuel for damaged cells to use in making
repairs. Red light may also stimulate the production of NO from CCO, meaning it has some
applicability in minor pain relief as well.'4
NEAR INFRARED LIGHT
(760-1400
NM).
Near infrared light has many of the benefits of red light, but its
longer wavelength allows for deeper tissue penetration.",'"' Various applications include pain
8 '9 stimulating cell repair,4 and increasing localized blood flow. 4 1,42 In addition to therapeutic
relief,31
purposes, near infrared light may also be used for a number of imaging/monitoring purposes. This is
due to the presence of a hemodynamic imaging "window" between the 70o and goo nm
wavelengths, in which it becomes relatively easy for far red and near infrared light to pass through
skin, bones, and a number of other tissues. 43
WHITE LIGHT
(400-760
NM).
White light, by definition, has the potential to provide all of the
therapeutic benefits of its constituent wavelengths. The source, however may often to be several
times more powerful to achieve the dosages necessary for these individual therapeutic effects, or the
exposure time must be several times longer. This may pose potentially harmful consequences, or not
28
29
30
(Sasseville, Benhaberou-Brun, Fontaine, Charon, & Hebert, 2009)
(Boivin, Boudreau, & Tremblay, 2012)
(Karu, 1988)
31 (Karu, Pyatibrat, Kalendo, & Esenaliev,
32
1996)
(Karu & Kolyakov, 2005)
33 (Hashmi, et al.,
2010)
(Poyton & Ball, 2011)
3s (Lister, Wright, & Chappell,
34
2012)
36 (Krawiecki, Cysewska-Sobusiak, Wiczynski, & Odon,
37 (Jacques, 2013)
38
(Whelan, et al.,
2001)
39 (Panhoca, et al., 2015)
40 (Whelan, et al., 2001)
41 (Nawashiro, Wada, Nakai, & Sato,
42 (Poyton & Ball, 2011)
43 (Weissleder, 2001)
2012)
29
2008)
be effective at all; thus, some moderation is needed. There is, however, research specific to white
light indicating that it may have a role to play in modulating immune system activity.44
2.7 Implementation
The range of phototherapeutic techniques may be grouped into four primary categories. First,
broad-spectrum phototherapy is a combination of light from multiple spectral categories (or
"colors"). This may include white light therapy, or a combination of two or more spectrums. Second,
narrow-spectrum phototherapy operates with light within a relatively narrow spectrum of light, such
as blue light therapy for SAD. Third, low-level laser therapy (LLLT) operates within a spectrum
consisting primarily of a single wavelength, emitted by a laser. Finally, photodynamic therapy may
(in theory) consist of any of the three previously mentioned forms of phototherapy in combination
with a photoactive agent for targeted treatment of malignant cells.
One of the basic principles of photochemistry is that light must be absorbed by a compound
before light-sensitive chemical reactions may occur. Further, light of various wavelengths may not
be absorbed equally or at all by a given compound. Two tools for characterizing the absorption and
chemical reactions of a compound relative to light wavelength are absorption spectra and action
spectra. As the name implies, an absorption spectrum plots the relative absorption of light by a
compound with respect to wavelength. Conversely, an action spectrum plots the chemical reaction
of a given compound with respect to wavelength. Ideally, the absorption and action spectra of a
photosensitive compound should be identical. Finding matching spectra, however, may be a
challenge in practice; it may well be possible that other compounds are affecting the rate of
photochemical reactions as well. Example graphs of the action spectra of the compounds bilirubin,
melanopsin, and cytochrome c oxidase (CCO) are provided in appendix, along with the luminosity
function of the eye (CIE 1931) as a reference (Fig. A.2, p.101). 45,46,47
Another principle commonly encountered in phototherapy is that chemical and cellular
reactions may exhibit a biphasic response with respect to phototherapy dosage.4 8 In other words,
there is an interval of time over which longer exposure results in more desired reactions, followed by
a period of reaction decline or even inhibition. This classic relationship is characterized by what is
known as the Arndt-Schulz curve. Occasionally, there may be a degree of flexibility in the
44
(Roberts, 2ooo)
4s
(Hankins, Peirson, & Foster, 2008)
(Lamola, Bhutani, Wong, Stevenson, & McDonagh,
2013)
(Karu & Kolyakov, 2005)
(Huang, Chen, Carroll, & Hamblin, 2009)
46
47
48
30
relationship between exposure time and intensity for phototherapy dosages. The same total fluence
of phototherapy may be achieved at higher irradiances and shorter exposure times, or lower
irradiances and longer exposure times. This flexibility however, is not infinite; for excessively long
exposure times, the desired phototherapeutic effects may never be achieved. Conversely, excessively
high irradiances may result in reaction inhibition or cellular damage - particularly when shorter
wavelengths are involved. The damaging effects of ultraviolet light are well-known, but there is also a
phenomenon known as "blue light hazard", which may result in damage to eyesight or other
'
problems if phototherapy irradiances are too high.4 9'5 "'5
As noted in Chapter i, one of the biggest challenges with the implementation of phototherapy is
with patient compliance.5 '
53
The patient may be required to be positioned in front of a phototherapy
device that delivers a predetermined dosage at a predetermined distance, over a predetermined
amount of time. This may be the source of some discomfort, inconvenience, and boredom for the
user; however, if the user does not remain in the phototherapeutic range of the device for an
appropriate amount of time, the treatment is compromised. In addition to proper education of
patients on the operation of their phototherapy device, systems that take into account a more
nuanced understanding of user needs and behavior are needed. This echoes back to our overall cause
for developing interactive phototherapy, a way to maintain the position of the user and
phototherapeutic device output in a "dynamic equilibrium" assisted by embedded computing
technologies.
2.8 Discussion
Over the course of this chapter we have set up some of the basic principles surrounding light and
biological mechanisms that may influence our development of interactive phototherapy. First, we
discussed light in terms of some of its physical properties: the significance of wavelength, units of
measurement, and emission properties. Next, we discussed light in terms of its relation to the human
body. This included commentary on human vision's varying sensitivities to light of different
wavelengths, as well as a few of the body's non-visual responses to light with respect to wavelength.
Finally, we discussed some of the basic categories and principles regarding the implementation of
phototherapy, along with particular challenges that may arise in doing so. The goal of these
investigations has been to establish guiding principles to phototherapy that any proposed system or
49
(Walker, Vollmer-Snarr, & Eberting,
50
(Olih, T6th-Molnir, Kemeny, & Csoma, 2013)
2012)
(Cesarini, 2009)
(Yelverton, Balkrishnan, & Feldman, 2006)
s3 (Kandaswamy, Akhtar, Ravindran, Prabhu, & Shenoi, 2013)
5'
52
31
platform will have to address. The ability for embedded computing technologies to support these
criteria will be evaluated in our discussion of the CityHome project in the following chapter.
Works Cited
Anderson, R. R., & Parrish, J. R. (1981). Microvasculature Can Be Selectively Damaged Using Dye Lasers: A
Basic Theory and Experimental Evidence in Human Skin. Lasers in Surgery & Medicine, '(3), 263-276.
Arakane, K., Ryu, A., Hayashi, C., Masunaga, T., Shinmoto, K., Mashiko, S., . . . Hirobe, M. (1996). Singlet
Oxygen (iAg) Generation from Coproporphyrin in Propionibacterium acnes on Irradiation.
Biochemical and Biophysical Research Communications, 223(3), 578-582.
Becker, D., Langer, E., Seemann, M., Seemann, G., Fell, I., Saloga, J., . . . von Stebut, E.
(2011,
June). Clinical
Efficacy of Blue Light Full Body Irradiation as Treatment Option for Severe Atopic Dermatitis. PLoS
One, 6(6), 1-9.
Boivin, D. B., Boudreau, P., & Tremblay, G. M.
(2012,
June). Phototherapy and orange-tinted goggles for
night-shift adaptation of police officers on patrol. ChronobiologyInternational, 29(5), 629-640.
Brainard, G. C., Hanifin, J. P., Greeson, J. M., Byrne, B., Glickman, G., Gerner, E., & Rollag, M. D.
(2001,
August 15). Action Spectrum for Melatonin Regulation in Humans: Evidence for a Novel Circadian
Photoreceptor. The JournalofNeuroscience, 21(16), 6405-6412.
Cesarini, J.-P. (2009, October-December). Blue light hazards for ocular lesions. Radioprotection, 44(4), 463478.
DeCusatis, C. (1998). Handbook ofApplied Photometry. New York: Springer.
Ellinger, F. (1957). MedicalRadiationBiology. Springfield, IL: Thomas.
Gold, M. H., Sensing, W., & Biron, J. A.
(2011,
December). Clinical efficacy of home-use blue-light therapy for
mild-to moderate acne. Journalof Cosmetic & Laser Therapy, q3(6), 308-314.
Gooley, J. J., Rajaratnam, S. M., Brainard, G. C., Kronauer, R. E., A, C. C., & Lockley, S. W.
(2010,
May
12).
Spectral responses of the human circadian system depend on the irradiance and duration of exposure
to light. Science TranslationalMedicine, 2(31)-
Hankins, M. W., Peirson, S. N., & Foster, R. G. (2008, January 31). Melanopsin: an exciting photopigment.
Trends in Neurosciences, 31(), 27-36.
32
Hashmi, J. T., Huang, Y. Y., Osmani, B. Z., Sharma, S. K., Naeser, M. A., & Hamblin, M. R.
(2010,
December).
Role of low-level laser therapy in neurorehabilitation. PM & R: The Journal OfInjury, Function, And
Hastings, M., O'Neill,
2),
S2 9
2- 3 o 5
J. S., & Maywood, E. S.
-
Rehabilitation,2(12, Suppl.
(2007). Circadian clocks: regulators of endocrine and metabolic
rhythms. JournalofEndocrinology, 195, 187-198.
H6hmann, D., Waner, M., & Schwager, K. (1993, April). [Yellow light laser photocoagulation of vascular
malformations in the head and neck area] (German article). HNO, 41(4), 173-178.
Huang, Y.-Y., Chen, A. C.-H., Carroll, J. D., & Hamblin, M. R. (2009, September i). Biphasic Dose Response
in Low Level Light Therapy. Dose Response,
7(4), 358-383-
Hunt, R. W. (2004). The Reproduction ofColour (6th ed.). Chichester, United Kingdom: Wiley - IS&T Series
in Imaging Science and Technology.
Jackson, R. F., Roche, G. C., & Shanks, S. C. (2013, March). A double-blind, placebo-controlled randomized
trial evaluating the ability of low-level laser therapy to improve the appearance of cellulite. Lasers in
Surgery andMedicine, 45(3), 141-147-
Jacques, S. L. (2013, June 7). Optical properties of biological tissues: a review. Physics in Medicine and
Biology,
58(11), R37-R61.
Kandaswamy, S., Akhtar, N., Ravindran, S., Prabhu, S., & Shenoi, S. D.
(2013,
July/August). Phototherapy in
Vitiligo: Assessing the Compliance, Response and Patient's Perception about Disease and Treatment.
Indian JournalofDermatology, 58(4), 324-328.
Karu, T. I. (1988). Molecular Mechanism of the Therapeutic Effect of Low-Intensity Laser Radiation. Lasers in
the Life Sciences, 2(1), 53-74.
Karu, T. I., & Kolyakov, S. F. (2005). Exact Action Spectra for Cellular Responses Relevant to Phototherapy.
Photomedicineand Laser Surgery, 23, 355-361.
Karu, T. I., Pyatibrat, L. V., Kalendo, G. S., & Esenaliev, R. 0. (1996). Effects of monochromatic low-intensity
light and laser irradiation on adhesion of HeLa cells in vitro. Lasers in Surgery and Medicine, 18(2),
171-177.
Kleinpenning, M. M., Otero, M. E., van Erp, P. E., Gerritsen, M. J., & van de Kerkhof, P. C. (2011). Efficacy of
blue light vs. red light in the treatment of psoriasis: a double-blind, randomized comparative study.
Journalofthe European Academy ofDermatologyand Venereology, 26,
33
219-225-
Krawiecki, Z., Cysewska-Sobusiak, A., Wiczynski, G., & Odon, A. (2008). Modeling and measurements of light
transmission through human tissues. Bulletin ofthe PolishAcademy ofSciences: Technical Sciences,
56(2), 147-154.
Lamola, A. A., Bhutani, V. K., Wong, R. J., Stevenson, D. K., & McDonagh, A. F. (2013, July). The effect of
hematocrit on the efficacy of phototherapy. PediatricResearch, 74(l), 54-60.
Laufer, G. (1996). Introduction to Optics andLasers in Engineering. Cambridge: Cambridge University Press.
Lister, T., Wright, P. A., & Chappell, P. H.
(2012,
September
17).
Optical properties of human skin. Journalof
Biomedical Optics, 17(9), 090901-1 - 090901-15.
Management of Hyperbilirubinemia in the Newborn Infant 35 or More Weeks of Gestation.
(2004,
July).
Pediatrics, 114(I), 297-316.
Meduri, N. B., Vandergriff, T., Rasmussen, H., & Jacobe, H. (2007). Phototherapy in the management of
atopic dermatitis: a systematic review. Photodermatology, Photoimmunology & Photomedicine, 23(4),
106-112.
Miyawa, J. H., & Schulman, S. G.
(2001).
Ultraviolet-Visible Spectrophotometry. In L. Ohannesian, & A.
Streeter (Eds.), Handbook ofPharmaceuticalAnalysis (pp.187-224). New York: Marcel Dekker, Inc.
Nawashiro, H., Wada, K., Nakai, K., & Sato, S.
(2012,
April). Focal increase in cerebral blood flow after
treatment with near-infrared light to the forehead in a patient in a persistent vegetative state.
Photomedicine and Laser Surgery, 30(4), 231-233Olih, J., T6th-Molndr, E., Kem6ny, L., & Csoma, Z.
(2013,
August). Long-term hazards of neonatal blue-light
phototherapy. British JournalofDermatology, 169(2), 243-249.
Oplinder, C., Deck, A., Volkman, C. M., Kirsch, M., Liebmann, J., Born, M.,
Suschek, C. V. (2013,
December). Mechanism and biological relevance of blue-light (420-453 nm)-induced nonenzymatic
nitric oxide generation from photolabile nitric oxide derivates in human skin in vitro and in vivo. Free
Radical Biology and Medicine, 65, 1363-1377Panhoca, V. H., Nunez, S. C., Pizzo, R. C., Grecco, C., Paolillo, F. R., & Bagnato, V. S. (2015, February).
Comparative clinical study of light analgesic effect on temporomandibular disorder (TMD) using red
and infrared led therapy. Lasers In Medical Science, 30(2), 815-822.
Poyton, R. 0., & Ball, K. A.
(2011,
February). Therapeutic photobiomodulation: nitric oxide and a novel
function of mitochondrial cytochrome c oxidase. Discovery Medicine, 11(57), 154-159-
34
Rahman, S. A., Flynn-Evans, E. E., Aeschbach, D., Brainard, G. C., Czeisler, C. A., & Lockley, S. W. (2014,
February i). Diurnal spectral sensitivity of the acute alerting effects of light. Sleep, 37(2), 271-281.
Roberts,
J. E.
(2000).
Light and Immunomodulation. Neuroimmunomodulation, 917, 435-445-
Ronan, P., & Gringer. (2013, Februrary 19). EM Spectrum. Wikimedia Commons. Retrieved May 1, 2014, from
http://commons.wikimedia.org/wiki/File:EM-spectrumrevised.png
Sasseville, A., Benhaberou-Brun, D., Fontaine, C., Charon, M. C., & Hebert, M. (2009, July). Wearing blueblockers in the morning could improve sleep of workers on a permanent night schedule: a pilot study.
ChronobiologyInternational,26(5), 913-925Sliney, D. H., Wangemann, R. T., Franks,
J. K., & Wolbarsht, M. L. (1976). Visual sensitivity of the eye to
infrared laser radiation. Journalofthe Optical Society ofAmerica, 66(4), 339-341.
Spector, A. (1982). Aging of the lens and cataract formation. In R. Sekuler, D. Kline, & K. Dismukes (Eds.),
Aging and human visualfunction (pp. 30-43). New York: Alan R. Liss, Inc.
Stroebel, L. D., & Zakia, R. K. (Eds.). (1993). The FocalEncyclopedia ofPhotography (3rd ed.). Boston: Focal
Press.
Titus, S., & Hodge,
J. (2012, October 15). Diagnosis and treatment of acne. American FamilyPhysician, 86(8),
734-740.
Vandewalle, G., Schwartz, S., Wuillaume, C., Balteau, E., Degueldre, C., Schabus, M., . . . Maquet, P. (2010,
November 9). Spectral quality of light modulates emotional brain responses in humans. Proceedings of
the NationalAcademy of Sciences ofthe United States ofAmerica, 107 (45), 19549-19554.
Walker, D. P., Vollmer-Snarr, H. R., & Eberting, C. L.
(2012,
January). Ocular hazards of blue-light therapy in
dermatology. Journalofthe American Academy ofDermatology, 66(1), 130-135.
Weissleder, R. (2001, April). A clearer vision for in vivo imaging. Nature Biotechnology, 19(4), 316-317.
Whelan, H. T., Smits, R. L., Buchman, E. V., Whelan, N. T., Turner, S. G., Margolis, D. A.,
(2001,
Caviness, J.
December). Effect of NASA light-emitting diode irradiation on wound healing. Journalof
ClinicalLaserMedicine & Surgery, 19 (6), 305-314.
Wyszecki, G., & Stiles, W.
S. (1982). ColorScience: Concepts and Methods, Quantitative Data andFormulae
(2nd ed.). New York: Wiley - Series in Pure and Applied Optics.
35
Yelverton, C. B., Balkrishnan, R., & Feldman, S. R. (2006, October). The utility of a data-logging device for
&
measuring adherence to home phototherapy. Photodermatology, Photoimmunology
Photomedicine, 22(5),
270-272.
36
37
38
3 / THE CITYHOME PROJECT
3.1 Overview
This chapter will explore the CityHome, a project of the Changing Places group in the MIT Media
Lab, as a platform for implementing interactive phototherapy. Here, the goal is not to provide a
comprehensive description of the CityHome's features, a task that may best be done in other
literature. Instead, we will focus on core features that are most relevant. Before doing this, we will
make note of the CityHome project's primary contributors, as well as the background problems and
motivations supporting the project. Next, we will discuss the CityHome's (i) spatial configurations,
(2)
structural/mechanical configurations, (3) user interfaces, and (4) additional hardware/software
configurations. This will then be followed by a brief discussion of how these features may fit with the
goal of implementing interactive phototherapy in a domestic environment.
3.2 Contributors
Under the supervision of Changing Places group principal investigator Kent Larson, the following
graduate students were lead researchers for the project: Hasier Larrea (MAS '15, Changing Places
group); Daniel Goodman (MAS '15, Changing Places group); Oier Arinto (visiting student, Changing
Places group); Phillip Ewing (SMArchS '15, Design and Computation group). In addition, the
following undergraduate students contributed as research assistants: Carlos Rubio, Matthew Daiter,
Kelly McGee, Hyunjoon Song, Hannah Ahlblad, Kabir Abiose, States Lee. As the architectural lead
for the project, I was primarily responsible for: architectural design of the wall unit, apartment
space, some of the more visible pieces of mechanical hardware, and coordination with the designs for
the internal mechatronic frame.
3.3 Background
The CityHome project was motivated by the need to find high-quality, affordable solutions to urban
housing. Increasing demand and limited real estate have driven cities to become increasingly
complex and often prohibitively expensive. In the United States, one only need to attempt to find an
apartment in cities such as New York City or San Francisco to see that this is the case. This is to say
nothing of other cities internationally, such as Tokyo, Shanghai, or Moscow, with even greater
populations and challenges. If cities are to remain accessible or even relevant in the long term,
solutions to problems of affordable urban housing are needed.
39
Multiple approaches to solving this problem have emerged in recent years. One approach is to
aggressively optimize the limited space that may be available in a given housing unit, resulting in
"micro-apartments." While commendable, there are obviously upper limits to this method. Second,
modular and prefabricated housing modules may attempt to reduce overall cost by minimizing onsite labor. In theory, this is a productive approach; in practice, however, prefabricated structures
may frequently cost as much as an equivalent "one-off" structure, often because the resulting
production volume is not enough to offset the cost of specialized fabrication equipment. Third,
transformable furniture - such as the classic fold-away Murphy bed - are another solution to fitting
more functionality into limited space. Such furniture, however, may often require manual actuation
to transition between configurations. This may not always be convenient if multiple spaces are
needed by the user in rapid or repetitive succession - or even possible, as in the case of some
physically-handicapped individuals.
The CityHome aims to build upon the advantages of these existing approaches, but extend them
with the aid of embedded computing technology. At 200 ft2 , the apartment has a small footprint, not
unlike many more affordable micro-apartments. The ability, however, to transform spatial
configurations enables the CityHome to have the functionality of a conventional apartment three
times its size. Its primary component comes in the form of a single, 6o"
x 100" x
96" robotic core
with modular, prefabricated components. Thus it is able to be installed in new and pre-existing
-
spaces with relative ease, and may be customized by a particular user in a "mix-and-match" manner
all at significantly reduced cost compared to an equivalent custom-made element. It is
transformable, but embedded computing technology allows for a variety of control methods,
including touch, voice, and gesture/position interfaces. Thus, the CityHome is an approach that
acknowledges previous work and challenges, but opens up new possibilities for how architecture
may actively adapt to the needs of its occupants.
3.4 Spatial Configuration
The basic CityHome apartment unit allows for five primary spatial configurations. First, the Living
configuration (Fig 3.1) is the CityHome default; all of the internal elements remain retracted; the
wall remains in its default position, flush against the bathroom area. Access is available to the
bathroom toilet and sink, but not to the shower area. As an option, a bench panel may be lifted to
allow for seating in front of the wall unit. Second, in the Dining configuration (Fig 3.2), the table
mechanism has been fully deployed; the bench panel has been lifted to allow for seating in front of
40
I~III~I-
-II-
I
I
Fig. 3.1: CityHome living configuration.
41
I
fi
I
(p
K
-I-
F-71-
I
*L
I
Fig. 3.2: CityHome dining configuration.
42
I~III~i-
-II-
7th
/~
~Th
i
--- ---- ------I
Fig. 3.3: CityHome working configuration
43
I~III~I-
-I-
7
-7
rz#
'p
I
I
I
Fig. 3.4: CityHome sleeping configuration.
44
I-Ill-I
YL
I
r
I
I
I
Fig. 3.5: CityHome bathing configuration.
45
I
the wall unit; free-standing chairs (not included in the wall unit) may be added on the window side of
the apartment to allow for seating of up to 8 people. Third, in the Working configuration (Fig 3-3),
the table mechanism has been partially deployed, leaving three tabletop edges exposed and one edge
concealed. A free-standing chair may be pulled up to the table, enabling functionality akin to that of
an extra-wide desk. Fourth, in the Sleeping configuration (Fig 3.4), the bed unit has been deployed;
the panel originally concealing the bed swings down, exposing the upper edge of the bedding and
mattress. Finally, in the Bathing configuration (Fig 3-5), the wall unit shifts over
42";
all other
elements remain retracted; access to the shower and adjacent closet is now possible.
3.5 Structural/Mechanical Configuration
The CityHome wall module consists of a lower mechatronic chassis and modular upper units (Fig.
3.6). The mechatronic chassis (countertop height and below) contains all of the motors and drive
systems that enable the wall and its various elements to move. This portion of the module would be
standard for all CityHome units. The upper portion of the unit may allow for "plug-and-play"
customization of the wall module. Bookshelf units may be installed instead of some of the cabinets,
for example (Fig. 3-7a-c). The configurability of the upper portion also allows for the CityHome wall
module to be installed in a variety of apartment retrofit scenarios (Fig 3.8). In addition to the wall
module, auxiliary elements in an apartment, such as window blinds or ceiling lights, may be
connected and controlled via the same interfaces as the CityHome wall module.
3.6 User Interfaces
Users may control various components and features within the CityHome via touch, voice
commands, or gestures. Force sensitive resistor pads at the corners of the components in the
mechatronic base (wall, table, bed) may be easily deployed or retracted with a light, but firm, touch.
A simple "tap" at a corner, for example, moves the entire wall system several inches (Fig 3-9a-c).
Voice command mode allows the user to control the state of any component in the apartment. In an
effort to avoid unintentional activation, voice commands are prefaced by the name "CityHome". In
addition, the user may select a custom "name" for the apartment, if preferred.
A Microsoft Kinect for Windows sensor enables gesture control of various components in the
apartment (Fig 3.ioa-d). To avoid unintentional activation of components, the user raises his/her
right hand for approximately 2-3 seconds to enter gesture mode. The ambient lighting flashes on
with a slow pulsing, pattern to prompt the user to select an object for control. As the user points at an
46
Fig. 3.6: Exploded isometric diagram
of early version of CityHome module.
Fig. 3.7:
CityHome wall
module
variations.
Fig. 3.8: CityHome wall module in an existing
apartment scenario.
47
Fig. 3.9a-c: Sequence of images showing wall
module before (a), during (b), and after (c)
movement via touch interface.
Fig. 3.10a-d: Sequence of images
demonstrating gesture interface for ambient
lighting. Side-to-side gestures control hue (a
and b); vertical gestures control brightness (c);
placing both hands forward confirms the user
selection.
48
Fig. 3.11 a-b: An overhead projector enables visual media to be displayed on a variety of surfaces
in the CityHome apartment, including the table (a) and wall (b).
object with his/her right hand and pauses, the gesture interface program uses the extracted 3 D body
skeleton of the user to construct a "selection" ray. The head of the body skeleton constitutes the
ray's base, and the pointing hand determines the ray direction. The selection program already has
preset information about the coordinate ranges of moveable elements in the apartment. Based on
this information, the ray-coordinate-range intersection determines the user selection. After a
selection has been made, the selected object remains lit while all other ambient lights turn off. The
user may then make gestures to determine the component's position or state. After making the
desired changes, bringing both hands forward locks the selection into place, and the program
returns to user prompt mode. The user may make another selection, or raise his/her left hand to exit
gesture mode. The lighting flashes red to confirm the mode cancellation.
Apico projector, mounted on a servo-controlled arm with two degrees of freedom, enables the
display of visual media on any surface in the main living space of the apartment (Fig. 3.IIa-b).
Although not implemented in this version of the project, potential further developments could
implement computer vision to recognize user selections of projected media.
3.7 Software/Hardware
Details
Similar to the physical hardware of the wall module, the software configuration of the CityHome has
a base "operating system" and optional add-on applications (or "apps"). The base package of
programs consists of a database for storing user data and apartment settings, a main loop for event
control, and core set of applications for controlling the wall module. These applications, in turn,
allow for the continuous incorporation of new functionalities, or access to various media. For
example, a user may command the CityHome to retrieve the latest news, or display the weather
forecast for the coming week. The main event loop program determines the port location of each of
the subsystems. The main event loop, user database, and user applications may all send and receive
49
information from each other. In turn, user applications may communicate directly with the
subsystems once the port location has been set and received from the main event loop. In most cases,
communication between subsystems and programs are facilitated by integer flags. Object-oriented
system architecture enables modular construction or substitution of CityHome subsystems. Most
subsystems, such as the ambient lighting and mechatronics - consist of an ArduinoMega board and a
USB interface to the main CityHome computer. The projector is controlled via a Raspberry Pi board
and an Ethernet interface.
3.8 Discussion
In order to effectively implement interactive phototherapy, we need: (i) phototherapy fixtures with
variable intensity/output,
(2)
the ability to determine the position of a user in relation to the given
lamp(s), (3), an interface for specifying the type and amount of phototherapy that is needed, and (4) a
system that takes into account all of these variables in continuously evaluated current dosage in
relation to the specified dosage goal. Given these criteria, the features of the CityHome project
discussed thus far are capable of implementing a form of interactive phototherapy. First, the
modular nature of the hardware and software provides the possibility of adding one or several
phototherapy lamps onto the wall module and/or throughout the apartment. Moreover, it is possible
software-wise to adjust the output properties of these lamps continuously, as demonstrated by
gesture control of ambient lighting. Second, if information about the location of each lamp is known,
then it should also be possible to determine the location of a user in relation to a lamp using the
CityHome's Kinect sensor. For areas that may fall outside the range of the Kinect sensor, each
phototherapy lamp could be equipped with location/proximity sensors for determining (in a
somewhat less specific way) user location. Third, any of the CityHome's touch voice or gesture
interfaces could be deployed as a means of specifying information to a specific software application
about the type and duration of phototherapy needed. Finally, it would also be feasible for this same
software application to continuously evaluate all of the relevant variables in determining dosage
accumulated over time in relation to a dosage goal.
In order to have some further proof of this last statement, we will need to establish some
methods for calculating dosage properties under changing conditions. The next chapter will attempt
to set forward equations describing output, using information from an existing photother apy lamp as
a test case. From these equations, we will then be able to more precisely evaluate interactive
phototherapy in the CityHome.
50
51
52
4 / CALCULATING PHOTOTHERAPY
4.1 Overview
In this chapter we will develop a process for analyzing lighting in terms of phototherapeutic dosage
in real-life scenarios. First, starting with basic optical equations and distributions, we will describe
the illuminance of an existing fluorescent phototherapy lamp as an equivalent representation of
point sources. Second, we will convert the illuminance of this lamp representation into irradiance.
Third, we will convert the irradiance into an estimated active therapeutic dosage for the specific
condition being treated. Finally, we will review the implications of this experiment and discuss
further directions for development.
4.2 Background
Before going any further, some explanation must be made for why we are constructing an analysis
method practically from scratch - as opposed to utilizing any of several lighting programs available
to architectural designers. Indeed, some examples of such programs may include (but are not limited
to): Autodesk® Ecotect® Analysis,' Radiance,' IES* VE for Architects®,l DIVA-for-Rhino, 4 the
Lighting Analysis Assistant in Autodesk® 3ds Max Design*,' Ladybug + Honeybee for
Grasshopper®,6 and GECO for Grasshopper*,7 among others. In my own attempts to utilize these
applications, however, it proved cumbersome - if not impossible - to (easily) parametrically control
the number, positioning, and/or orientation of light sources in a lighting array. Problems also often
arose when attempting to define and/or control the illumination distribution pattern of artificial
light sources.
In particular, one workflow obstacle that emerged has to do with the fact that many of the
aforementioned applications rely on hidden command-line prompts to the Radiance software
program for generating lighting analysis information. Radiance is a program that does not actually
have a graphical user interface (GUI). Therefore, Radiance can only be directly accessed via a
command prompt interface. Radiance's analysis features are invoked on files that are written in a
(Autodesk, Inc.)
(Radiance WWW Server)
3 (Integrated Environmental Solutions Limited)
/ (Solemma, LLC)
5 (Autodesk, Inc.)
6 (Roudsari)
7 ([uto])
2
53
specialized RADIANCE scene description language. As a result, many developers have come up with
more user-friendly applications for accessing Radiance's lighting analysis features; with the
exception of the Lighting Analysis Assistant in Autodesk®
3 ds
Max Design®, all of the
aforementioned programs rely either completely or partially on Radiance for lighting analysis. If any
of the scene description files being input from these programs are invalid, the Radiance lighting
analysis will fail and return a blank screen. Since communication to/from Radiance occurs in the
background, however, it becomes difficult to debug where an error may have occurred. Even if it is
possible to identify where the error occurs, fixing the problem may require knowledge of the
RADIANCE scene description language - if the problem file is even human-readable at all.
Another workflow obstacle has to do with the management of illumination distribution pattern
data of light sources. One of the most commonly-supported file formats for this data is the IES
standard (*.ies) file format, an ASCII delimited text file standard first defined by the Illuminating
Engineering Society of NorthAmerica (IES) in 1986 (LM-6 3 -86) and updated in 1995 (LM-6 3- 9 5 ) and
2002
(LM-6 3 -02). In attempting to make use of this photometric data, there are multiple potential
problems that may emerge. First, Radiance cannot directly read an IES file (at least, not at the time
of this writing); it must first be converted to a file in the RADIANCE scene description language
before it can be used for lighting analysis. In theory, this is not a problem, since there is a specific
Radiance command ("ies2rad") for doing this; however, errors related to differing IES file standard
versions can (and do) occur. Second, The IES file description by default specifies the origin of the
light source at the world origin (o,o,o) and orients the "axis" of a light source in a "cardinal"
direction (i.e. "up", "down", "left", etc.). In order to move or rotate the light into a different
position/orientation for the lighting analysis, the IES file must be converted to the RADIANCE
scene description language ("ies2rad") and a command ("xform") must be invoked in order to make
the transformation before the lighting analysis occurs. Anomalies in the file formatting from the
conversion command ("ies2rad"), if not addressed, may cause problems with the transformation
("xform") command. Finally, it is also possible that lighting manufacturers may not provide data in
the IES format - or any similar format, such as EULUMDAT or TM-14 . Instead, photometric data
may only be available in a format that can only be opened by specialized optical design programs such
as ASAP*," LightTools®,9 or Zemax*®
- programs that, for any of various reasons, are typically
beyond the reach of architectural designers. In fact, this is exactly the case regarding photometric
information for a particular LED model we will be using later in this chapter, as well as the following
(Breault Research Organization, Inc.)
9 (Synopsys Optical Solutions Group)
8
'0 (Zemax, LLC)
54
chapter. Thus, it falls to the user to reconstruct an IES (or equivalent) file from the graphs and other
information in a light source's datasheets - a process which may not be immediately clear.
Even if both of these workflow obstacles can be resolved, there are still other problems that
make creating a custom system more appealing. First, photometric units must be converted to
radiometric units, a task which relies on more data than is typically specified in most photometric
data files. Second, we must then convert radiometric units into an actual phototherapy dosage. None
of the aforementioned programs support these tasks - nor were they designed to do so. In light of all
of these various reasons, we will be creating our own system for analyzing interactive phototherapy.
In this thesis, we will be using Grasshopper® (v. 0.9.0014)," a "graphical algorithm editor" for the
modelling program Rhinoceros® (v. 4.0, SR9 )," as our analysis environment. Analysis equations,
however, will be written out in standard mathematical notation for implementation in any
3D
appropriate analysis/programming environment.
4.3 Existing Lamp
In Chapter 2: Light and Medicine, we discussed the broad range of phototherapy light sources and
techniques. In all cases, a phototherapy lamp has an (i) illuminance rating, (2) phototherapeutic
range, (3) spectral power distribution (SPD), and (4) dosage time.
The Bio-Light Ultra® (Fig. 4.1), produced by Enviro-Med*,
is an example of a broad-spectrum
phototherapy lamp. It is a 12" X 24" unit that produces (i) io,ooo lux at a distance of (2) 24" away,
with a SPD characteristic of a (3) fluorescent lamp, and (4) has a dosage time of 20-30 minutes (we
will use 25 minutes for the purpose of our analysis). The goal of analysis will be to reconstruct an
Fig. 4.1: Bio-Light Ultra* lamp.
"(Robert McNeel & Associates)
1 (Robert McNeel &Associates)
13 (Enviro-Med, 1997)
55
equivalent mathematical model of the Bio-Light Ultra® unit that is capable of producing a similar
phototherapy dosage output. For the sake of simplicity, and due to the lack of more specific
information about the lamp, our analysis will include a few assumptions and simplifications.
First, the analysis of finite linear light sources inside the unit presents some initial challenges.
An equation governing the falloff - the attenuation rate of illuminance with respect to distance from
a light source - from finite linear light sources is a complex topic that is beyond the scope of this
thesis. Instead, we will construct a representation for linear and area lighting as a series of point light
sources. This is a commonly accepted method used by optical engineers for approximating the falloff
from such sources. Further, we do not have published information regarding the geometric
configuration of fluorescent lamps inside the Bio-Light Ultra® unit. Therefore, for our calculation
purposes we will take the 12" x 24" luminous opening as a starting point and attempt to construct an
array of phototherapy light sources that satisfies the same illuminance rating.
Second, we do not know the luminous intensity falloff with respect to angle of emission, or how
the intensity of the light varies as we move away from the imaginary "axis" of the lamp. The falloff
with respect to angle of emission is a function of the (i) distribution pattern of the fluorescent lamps,
(2) geometry of the reflector inside the phototherapy unit, and (3) the refraction pattern of the
diffuser. Specific information on any of these properties is not available to us. Therefore, we will
assume that our light sources have a bell-curve or Gaussian distribution pattern, a pattern that is not
uncommon in lighting analyses.
Third, the absorption spectra of the lamp's reflector and diffuser might have the potential to
alter the SPD of the light emitted from the lamp. As light is reflected off of the internal reflector or
refracted through the diffuser, certain wavelengths of light may be attenuated based on the
properties of the materials involved. This, in turn, may alter the effective phototherapy dosage.
Therefore, we will simply assume that the diffuser and reflector components evenly absorb a
combined io% of the light emitted from the internal light sources, resulting in a transmission
efficiency of 90%.
Finally, having made all of these assumptions about the characteristics of the light sources for
our analytical model, we still must specify the luminous flux or intensity of each point light. We will
make a (somewhat arbitrary) decision of modelling our point light sources off of a selection of a
Philips® LUXEON Rebel® LEDs produced by Philips. This decision is primarily motivated by the
increased flexibility (compared to fluorescent lamps) in creating lighting configurations for the
CityHome, which will become evident in subsequent sections. To be more specific, we will use the
luminous flux of an example LED model as a starting point for this analysis. This will be useful in
calculating the luminous intensity distribution pattern, which we will assume to be Gaussian in
56
nature, as mentioned earlier. However, for this analysis we will still rely on the typical SPD of a
fluorescent lamp in calculating the effective phototherapy dosage. The actual SPDs of the LEDs will
be used in calculations
for the CityHome lighting configurations. With these and the
aforementioned assumptions and simplifications, we can begin construction of our analytical model.
4.4 Calculating Illuminance
Calculating the illuminance from a light at a given point in space will be done in three stages. First,
we must characterize the illumination falloff rate with respect to distance from the lamp. Second, we
must account for the fact that light may not be radiated uniformly in all directions from a light
source; thus, a function describing the luminous intensity with respect to angle of emission must be
defined. Third, we must also account for how the angle of incidence of light rays relative to the
(implied) analysis surface affects illumination. Having accounted for these three principal
components, it will then be possible to calculate illuminance for a point and - by repetition - an
entire analysis grid. Finally, we will demonstrate how this illuminance calculation can be
implemented in Grasshopper*.
4.4.1 Falloff
We know that there are basic equations governing the falloff of illuminance from a light source with
respect to distance. First, we know that an infinitely large area light source has a constant
illumination with respect to distance; no matter how far you move away from the source, the
illumination at a given analysis point will always be the same. This can be described by the equation
EV = I,/k, where E, is illuminance specified in lux (lx), 1, is luminous intensity specified in
candelas (cd), and k is a constant value. Second, we know that an infinitely long linear light source
has a linear falloff with respect to distance. This can be described by the equation E, = I,/d , where
d is distance specified in meters (m). Third, we know that an infinitesimally small point light source
.
has a quadratic falloff with respect to distance. This can be described by the equation E, = Iv/d2
No light source in the real world has an infinite area, infinite length, or is infinitesimally small,
but it can sometimes be useful to model a light source as a combination of these falloff equations in
varying degrees. A generalized version of this equation that is used in some ray-tracing programs has
the format:' 4
'4
Adapted from (Foley, van Dam, Feiner, & Hughes, 1996, p. 726)
57
EV =
IV
kc + k 1d + kqd 2
(4.1)
where k, is the constant attenuation factor, k I is the linear attenuation factor, and k q is the quadratic
attenuation factor. We will not be using nor needing constant or linear falloff components for our
analysis, but these considerations are useful to keep in mind when specifying a more generalized
model for analyzing illuminance. Since we are assuming our light sources can be best modelled as
point lights, we can simply assume that, k c and k 1 are equal to o, and k q is equal to
i.
4.4.2 Angle of Emission
For a point source that radiates light uniformly, we can readily convert between luminous flux in
lumens (lm) and luminous intensity in candelas (cd) with the equation:
I =
(4.2)
v
where I, is luminous intensity specified in candelas (cd),
v, is the luminous flux of the point source
specified in lumens (lm), and f2 is the solid angle through which light is being emitted, specified in
steradians (sr). We know this to be correct simply by unit definition (see Table 2.1 in Chapter 2): cd
=
(cd - sr) / sr. If light were being emitted from a single point into all directions, then f2 would be
equal to 4n steradians.
However, we know that our light is, in fact, not radiating light uniformly in all directions. In
fact, we are making the assumption (based on observation of comparable light sources) that the light
is being radiated in a bell-curve-like or Gaussian pattern. Therefore, we need a more sophisticated
way of specifying the luminous intensities for every angle of emission in such a way that everything
sums to a known luminous flux.
Before we tackle that problem, we should first state in mathematical terms exactlywhat we mean
by the term "Gaussian." The Gaussian function (named after mathematician Carl Friedrich Gauss)
has the general format:
g(x) = a exp ((x2 -
2
+ d
(4.3)
where a is a constant describing the height of the curve's peak (relative to the value the curve
asymptotically approaches), b is a constant that describes the position of the center of the curve's
peak, c is a constant describing the "standard deviation" or width of the "bell", and d is a constant
describing the "offset" of the curve (from zero).
A useful way to understanding the value of c is in its relation to the function'sfull width at half
maximum (FWHM) andfull width at tenth maximum (FWTM). Full width at half maximum (FWHM)
can be expressed as:"
FWHM = 2M In 2 c ~ 2.35482c
(4.4)
Similarly, full width at tenth maximum (FWTM) can be expressed as:
FWTM = 2M 2n 10 c - 4.29193c
(4.5)
With this formula in mind, we can mathematically describe the distribution pattern of our point light
source.
One way to accomplish this task would be to specify the peak (i.e., "on-axis") luminous intensity
of the light source as the constant a in the Gaussian function, and all other angles of emission from
our light source would be some fraction of this peak luminous intensity. This is a nice idea, but we
still need to figure out what exactly the peak luminous intensity would be with respect to our
Gaussian distribution. There are two ways of going about this, an exact conversion and a "quick"
conversion. Both methods will define the peak intensity of a light by asking how we can compute a
solid angle feq through which light would be radiated uniformly at peak intensity that is equivalent
to the luminous flux of our actual distribution pattern.
An exact formula for calculating d2eq for light sources with a symmetrical radiation pattern is as
follows:'6,17
deq = 27T
I'(6) sin(9) dO
(4.6)
0
where 0 is the angle of emission expressed in radians, and I'(0) is the radiation distribution pattern
normalizedin amplitude - i.e., the largest value of I'(0) is equal to i.
15 (Weisstein)
6 (Giangrandi, 2013) provides an explicit definition of this equation.
17
(Smith, 1966, p. 186) discusses radiation through an incremental dO ring area of a hemisphere.
59
If we assume, however, that our radiation distribution pattern is Gaussian, we can approximate
9
eq as the full width at half maximum (FWHM) angle of the light. This angle is frequently given
explicitly in light fixture datasheets. We can relate this angle (given as 260.5 for the full angle, or
simply 60.5, for half of the angle) to the equivalent solid angle in steradians using the following
equation:' 8
Deq = 27r(1
-
(4.7)
cos60 .5 )
This paper will not develop a specific proof for why the integral of a Gaussian curve over a specified
interval (which is basically what we are trying to do) can be estimated as a rectangle with FWHM for
its width and peak intensity for its height. However, the intuition of this method becomes clear if we
plot out both distributions and compare differing areas (Fig. 4.2). In this thesis, we will use this latter
method for calculating
feq,
though general methods for arriving at this value should be noted.
-- g(x)
-teq
0.8
0.6
0.4
0.2
-2
-4
0
2
Fig. 4.2: Plot of Gaussian function g(x) alongside C.eq estimation. Note that the shaded areas
between the two plots are approximately equal in area.
Once we have determined 12q, the peak luminous intensity Innax can be computed using the
following equation:
18
(Giangrandi,
2013)
66
(4.8)
~eq
-
ivmax
where P, is the luminous flux expressed in lumens (lm).
Before proceeding to the general equation of our luminous intensity distribution, we should
consider that our light may not necessarily be transmitted into space with ioo% efficiency. It is
probable that any number of intermediate optical diffusers, reflectors, etc. may reduce the intensity
of our light by a certain non-negligible factor. We will account for these losses due to any
intermediate optical devices/filters with the normalized factor k, which at a value of i indicates
ioo% transmission efficiency and at a value of o indicates o% transmission efficiency.
Having made considerations for all of these parameters, we can now construct a general
relationship between the Gaussian distribution pattern of our light source and its luminous flux.
Expanding and substituting for our original Gaussian equation:
g(x) = a exp
=
(x - b)2
2C2
+d
(
ke Ivmax exp
0-0b) 2
I,(0) = keIvmax exp
2 ( FWHM
\2421n 2/
I(0) = ke (
+d
)
(0 - b) 2
(
Iv(0)
(
(0 - b)2
expy
neq)
+d
2
d
2
2( 20
2V2 -n2/
(4.9)
)+
If we further assume that the peak intensity of our light source will always occur on axis (as we have
in both versions calculations for Deq, and will always approach zero, we can eliminate the variables b
and d. We then arrive at the following equation:
(
\eq/
(2 - (0))2
exp|
)
Iv(0) = k e
-
(
2 0.
2, 2 In 2/
61
2
)+
(O)
I,(0) = ke
(
2
(
- COS05)
exp
(2
K
o2\
2005
2
2 ,2 In2/
I(0) = ke
I(0) = k e
(\21(1
(@,
(
)
exp I o~)B.5
2
00o
K( n2)2
exp
ov
27r(1 - cos0.)
2)02
(In 0.sp
(4.10)
where 0 is the angle of emission expressed in radians (rad), ke is the normalized transmission
efficiency factor (unitless, o-i), (P, is the luminous flux of the light source in lumens (1m), and 00.s is
the ha/fwidth at half maximum expressed in radians (rad).
We have arrived at a function, I, (0), that can describe luminous intensity (I,) with respect to an
angle of emission (0). To calculate illuminance (E,) as a function of distance (d) and angle of
emission (0), we may simply combine Eq. 4.10 with the constant-linear-quadratic falloff equation we
discussed earlier (Eq. 4.1):
E, (0, d) =k
e
OVexp
(2w(1 -cos 0.))
( -I
)0 )
0.52
kc+ kd + kqd2
(4.11)
4.4.3 Angle of Incidence
Eq. 4.11 applies if our analysis surface is always oriented directly towards the light (i.e., is spherical),
but we can assume that this is not always the case. Therefore, we will need another term in our
equation that handles varying angles of incidence for our light rays. Fortunately, Lambert's cosine
law handles this condition quite succinctly.'" It states that the illuminance falling on any surface
depends on the cosine of the light's angle of incidence, expressed as p:
E, = Ecosqi
(4.12)
We can simply add this term onto our working equation to arrive at the following expression that
calculates illuminance as a function of angle of emission, distance, and angle of incidence:
19 (Smith, 1966, p.
185)
62
Ev(6, d, T)
= [ke
(27r( - COS 0.5))
exp
(
2)
00.5 2)
[
kc+ kid1 + kqd 2
[cos p]
(4.13)
Eq. 4.13 works nicely for describing illuminance from one point source, but our analysis will involve
multiple light sources. More specifically, it will involve a two-dimensional array of light sources. The
illuminance of any point in space will be the sum of the contributions of every light source in the
array - each source with its own angle of emission, distance, and angle of incidence relative to the
point in space being analyzed.
To account for all of the illuminance contributions from an m x n array of light sources, we
could restate our equation in the following way:
Ev(0,d, p)=
m-i n-1
E
(
_
ke
2(1 -COS)0.s)
exp
2_
2)!2)1
-(n26
60.s
(4.14)
~
12
kc+ kld 4 + kqd[
[COS vpi,j)
where m and n denote the size of the array in each direction, i and j are indices for denoting which
particular angle of emission, distance, and angle of incidence is being used at each step in the double
summation. A visualization of calculation of this may be as follows (Fig 4.3):
0
d
E (0,d,(p)
Fig. 4.3: To calculate total E,
m x n array must be summed.
d, (P) at a single analysis point, all of the light sources (i J) in an
It would be possible to continue expanding this equation to account for scenarios in which every
light source in the array has a different luminous flux, beam width, transmission efficiency, etc. For
the sake of our analyses, however, we will assume that these properties remain identical for every
light source in our array.
4.4.4 Implementation
Implementation of Eq. 4.14 into Grasshopper® can be described as a five-part process. First, we must
parametrically (or manually) define geometry representing light sources and an analysis grid.
Second, the geometric conditions between the light sources and analysis grid must be translated into
variables (0, d, p) for all of the light sources relative to each analysis point. Third, we must perform
the actual illuminance calculations for each point in the analysis grid, using variables (0, d, W) and
other constants specified in Eq. 4.14. Fourth, the illumination calculation results must be mapped to
the analysis grid to evaluate whether desired performance criteria for the lamp have been met.
Finally, if the desired performance criteria have been met, then a fixture solution has been found; if
not, adjust the lighting parameters and repeat parts
1-4.
Screenshot images of implementation in
Grasshopper® are as follows (Fig. 4.4-5).
Three 3 m
x
3 m analysis grids, containing ioo
x
ioo faces (or
10,201
analysis points) were
defined in order to analyze our reconstructed phototherapy lamp with regard to its XY, XZ, and YZ
planes. The intersection of these three grids denotes an analysis point 24" (o.61o m) away from the
phototherapy lamp and co-linear with the lamp's central axis. Luminous flux (0,), full beam angle
(200.5), and (applying Eqs. 4.7 and 4.8) peak luminous intensity ('vmax) were derived from a Philips®
LUXEON Rebel® 30oo K LED (part no. LXM 3 -PW7 i); additional data for this and other LEDs to be
used in this and the following chapter may be found in the appendix (Tables A.I-2).
20
'"Illumination
falloff parameters (kc,k,,kq) were set to (0,0,1). For sake of simplicity, here the transmission
efficiency factor (ke) assumes no intervening optics, and is set to (1).
Through trial and error, it was determined that an evenly spaced array 16
x
io array of light
sources would result in an illuminance of 10,661-9437 lux at an analysis point 24" (o.61o m) away
from the phototherapy lamp and co-linear with the lamp's central axis. Analysis results are plotted in
the following figure (Fig. 4.6a-d).
2
" (Philips Lumileds Lighting Company,
(Philips Lumileds Lighting Company,
21
2014)
2014)
for white LEDs.
for color LEDs.
64
a
a
I
t
:1
a
--
I.-.I
~-4~b
Ii
I-'-J
L: :::1
C,
WWWmE
.
..........
Fig. 4.4: Main level diagram of illuminance calculation in Grasshopper@.
Fig. 4.5: Screenshot of illuminance values being mapped back to the Rhinoceros@ modelling
environment from Grasshopper@.
65
-1.0
0
1.0
2.0
2.0
1.0
1.0
xz
xz
-1.0
1.0
-1.0
1.0
0
0
XZ
1.0
2.0
1.0
1.0
1.0
0 -- - - -
- - - -
- - - - - - - -0
- -
Y
-1.0
-1.0
-1.0
-1.0
0
0
1.0
XZ
1.0
2.0
lux (lx)
0
5000
10000+
Fig. 4.6a-d: Illuminance calculation results for reconstructed model of phototherapy lamp.
66
4.5 Illuminance to Irradiance
We now have a way of calculating the illuminance in lux at a particular analysis point, but the actual
irradiance in W/m2 is still not known. If we are to figure out the effective dosage for our
phototherapy lamp, we need to know the irradiance of our lamp at every wavelength of light.
As discussed in earlier chapters, we know that the visibility of light is a function of the eye's
varying sensitivity to varying wavelengths. In order to convert illuminance to irradiance, we will
need to know the SPD of our light source, P (A) (defined in any arbitrary units - we will handle this
shortly), and the wavelength sensitivity of the eye or luminosity function, Y(A).
The units provided for a spectral power distribution are not necessarily provided in datasheets
for a given light source, P(A); frequently, SPD data may only be provided on a relative scale.
Therefore, it becomes helpful to define a new function P'(A) based on P(A) that is normalized in
surface and unitless. In other words, the integral of P'(1) should be equal to 1:
0
dA - 0fo CP(A)
P( A)d A
0
0
1
(4.15)
Next, we can use P'(A) to calculate an illuminance conversion factor i, This factor, 77, will describe
the relative visibilityof our light source to the human eye:
780
683 lm/W
i,=
f
P'(A)Y(A) dA
(4.16)
380
We can relate illuminance E, (lx or lm/m 2 ), irradiance E (W/m 2 ), and our illuminance conversion
factor 77, with the following equation:
E
E = -V
(4.17)
7V
Substituting and expanding our equations, we can arrive at a more complete formula for converting
illuminance to irradiance in our application:
E =
683
780 v
f380 P'(A)y(A) dA
(4.18)
Returning to our phototherapy lamp calculations, we have enough information to convert
illuminance to irradiance. The concept of the eye's luminosity function was introduced in Chapter 2:
67
Light and Medicine, and a graph of this function is available in the appendix (Fig. A.i). The
phototherapy lamp manufacturer Enviro-Med* does not explicitly provide information about which
specific light bulbs are being used - let alone the SPD. Since the Enviro-Medowebsite describes the
phototherapy lamp as having "3 double tubes," we will assume the lamp uses some form of
fluorescent lighting. A typical SPD for a 650o K compact fluorescent is also provided in the appendix
(Fig. A.2).
Starting with Eq. 4.18, we can get the following value for irradiance (E). Calculations were
performed in Grasshopper, but the substitutions of values can be followed here:
E =
780
683 - f380 P'(A)y(A) d2
E
10661.9437
683 - (0.5184)
10661.9437
354.0672
E = 30. 1128 W/m 2
It is critical to remember that this level of irradiance would not be constant over a given surface if we
were to place an actual i m2 target at our analysis point. This value for irradiance is only indicating
that light is being radiated at that particular point at a rate of 30.128 W/m , which may very well
2
change drastically as we move away from that particular point. In any case, we may now proceed to
the next step, which is that of calculating phototherapeutic dosages.
4.6 Irradiance to Dosage
We now know the total irradiance of our light source across the wavelengths of the visible
spectrum in W/M 2 , but describing the phototherapeutic dosage or fluence for a targeted condition is
not necessarily straightforward. It is true that - by unit definition - simply multiplying irradiance in
W/m2 by time in seconds (s) will yield a value in J/m2 ; it is also true that summation of practically any
SPD in W/m 2 of equal power could yield the same quantity in J/m 2 . What is not true, however, is that
equal amounts of irradiance from light sources with differing SPDs will necessarily catalyze the
photoactive agent we wish to target at equal rates. Further, the specific SPD of the light sources
deployed in the medical literature for phototherapy are not always explicitly reported. Thus, it
68
becomes difficult to accurately compare the phototherapeutic performance of a light source with a
somewhat different (but still similar) SPD, given the same irradiance. The confusion of the situation,
however, is further compounded by the fact that total dosages are - in fact - not the same across
medical literature that may be experimenting with the same mode of phototherapy. One paper may
arrive at an optimal fluence of 2 J/cm2 for treatment, whereas another paper may conclude that 5
J/cm 2 is best. Thus, the only true way to accurately evaluate the performance of a light with a given
SPD is to recreate all of the other conditions in the experiment that was conducted in a medical
-
paper. Such an investigation is beyond the scope of this thesis. We will need to find another metric
even if it is a largely academic one - for describing the effectiveness of a light source's SPD in
catalyzing the therapeutic mode we may desire.
A few hints at the steps to figuring out an answer to this need are embedded in the question.
First, we need to figure out how much of the irradiated light is being absorbed by the photoactive
agent(s) we wish to catalyze. Second, we need to relate the rate of this estimated active irradiance
expressed in W/m 2 , to an actual phototherapeutic dosage, typically expressed in J/cm 2 . Besides the
obvious change of area units, this is where the variable of time comes into play. Finally, we should
give some consideration for the abilityto modulate the dosage rate with respect to time. Indeed, even
if we are able to achieve the necessary fluence for a specific phototherapeutic mode, it is possible that
too high an active irradiance rate within too short a time period may be harmful. Conversely, too low
an irradiance rate across too long a time period may not induce the reactions necessary for a
particular therapeutic application.
To address the first step, we will need a spectral distribution of the relative effectiveness of each
wavelength in producing change. I propose that we call this a phototherapeutic action spectrum
A(A), with values normalized between o and i. Relative values for this action spectrum are
determined in medical and photochemical literature, and we will make reference to the appropriate
action spectra in calculating our estimated active phototherapeutic dosage.
Using A (A), one way of determining the active irradiance, which we will call Ea, would be to
weight each value of our light's spectral power distribution by the action spectrum of our
photoactive agent. This would result in the following equation:
780
Ea=E
f
P'(A)A( A) dA
(4.19)
380
The implications of this equation are that light sources with the bulk of their power in less
effective spectra will result in a lower values for Ea Conversely, light sources with SPDs that more
closely match the phototherapeutic action spectrum A (A) will result in higher values for Ea69
Now that we know the estimated active irradiance, we will need to determine how long it will take to
achieve the estimated active phototherapeutic fluence Ja. Since one joule is equal to one watt of
power transmitted for one second (J = W -s), the equation is simple:
Ja = Eat
(4.20)
where Ja is the estimated active fluence expressed in joules per meter squared (J/m2 ), Ea is the
estimated active irradiance expressed in watts per meter squared (W/m2 ), and t is time expressed in
.
seconds (s). Conversion to J/cm 2 only requires division by io,ooo cm 2 /m 2
Our calculations thus far have implied that irradiance is fixed and continuous, but this may not
always be desirable. To handle scenarios in which we may wish to pulse-width-modulate (PWM) our
light (if the light fixture allows it, as with LEDs), we will introduce the duty cycle factor kd, which
may be calculated from the on-time (ton) and off-time (toff) of our lamp's pulse structure:
kd-=ton
(4.21)
ton + toff
As a point of clarity, it is implied that the on-time and off-time intervals are significantly smaller than
the dosage time:
(ton + toff).
Substituting and expanding our equations, we can arrive at a more complete formula for
converting irradiance to dosage in our application:
Ja = kdEat
a
a
ton
ton+ to f
(E - J3'80
(4.22)
) CA~
2
10,000 cm /M2
t
(4.23)
where Ja is the estimated active fluence in joules per centimeter squared (J/cm2 ), ton and toff is the
on-time and off-time respectively for pulse-width modulation expressed in seconds (s), E is the
irradiance expressed in watts per meter squared (W/m2 ), P'(A) is the surface-normalized spectral
power distribution of our lamp, A (A) is the action spectrum for our phototherapy agent(s), and t is
the phototherapy session time expressed in seconds (s).
Of course, if our goal is to calculate the total fluence from a given phototherapy lamp, we need
only make a small change:
70
(10,000 CM2M
ton+ toff
(4.24)
)t
E
(tonton
To return to our ongoing phototherapy lamp analysis, we can describe the output of the lamp in
both total ()
1,500
and estimated active (/a) therapeutic dosages over a time period of
seconds. We will assume that the lamp is constantly on: kd
=
25
minutes, or
1. Starting with Eq. 4.24, we
arrive at the following dosage:
ton
(ton
=
Et
10,000 Cm2/m2
+toff
30.1128 W/m 2
(1) (10,000 cm2/m2) (1500 s)
J = 4.5169j/cm 2
We can also calculate the estimated active therapeutic fluence. In this calculation, the function
A (A) will represent the action spectrum of melanopsin. We may recall from Chapter 2: Light and
Medicine that melanopsin photopigment in intrinsically-photosensitive retinal ganglion cells
(ipRGCs) that contributes to the alertness response. Starting with Eq. 4.23:
780 P'A)A(A)dA
/E
Ia
=
ton.
=ton+ toff-)
ha= (1)
- f380
2'~A~
10,000 cm 2 /m 2
((30.1128 W/m 2 ) . (0.3651)(
1,0cm/ CM2 /m22
10,000
Ia =
dAt
)(1500
s)
1. 6491 J/cm 2
4.7 Discussion
This chapter has established some basic methods for analyzing the effectiveness of phototherapy
with regards to spatial and temporal conditions. First, in three parts, we formulated an equation for
calculating illuminance from an array of point sources with Gaussian radiation patterns. Second, we
explored conversion from illuminance to irradiance, especially with regard to a light source's
spectral power distribution. Third, we developed two ways of describing the phototherapeutic
71
dosage from a lamp: one method considers the total irradiance over a spectral power distribution,
while another attempts to take into account the action spectra for photoactive agents. These
equations also attempt to allow for modulation of dosage rates by varying the source's pulse
structure. Throughout this investigation, we used these equations to reconstruct some of the
performance information of an existing phototherapy lamp.
The next chapter will explore what the results of these analysis methods mean for hypothetical
everyday user scenarios. Since the medical literature may often suggest varying phototherapeutic
dosages - even for treating the same condition - it will not be the purpose of this thesis to definitively
establish firm dosage goals. Such a task would be best suited to a more comprehensive survey of the
medical literature. Instead, the next chapter will focus on the process of working with the equations
set forth in this chapter, as well as how they may help inform broader design choices and
considerations in a project.
Works Cited
[uto]. (n.d.). Geco I Grasshopper. Retrieved June 2014, from Food 4 Rhino I Apps for Rhino and Grasshopper:
http://www.food4rhino.com/project/geco?ufh
Autodesk, Inc. (n.d.). 3 D Design & Visualization Software | 3 ds Max Design IAutodesk. Retrieved June 2014,
from Autodesk: http://www.autodesk.com/products/3ds-max-design/overview
Autodesk, Inc. (n.d.). Ecotect Analysis - SustainableBuilding DesignSoftware - Autodesk. Retrieved 2014
June, from Autodesk: http://usa.autodesk.com/ecotect-analysis/
Breault Research Organization, Inc. (n.d.). Key FeaturesofASAP; the Optical Software by BreaultResearch
(BRO). Retrieved June 2014, from Optical Software, Engineering, and Training by Breault Research
(BRO): http://www.breault.com/software/asap-features
Enviro-Med. (1997). Enviro-MedBio-Light Ultra io,ooo LUX light therapy system. Retrieved June 2014, from
http://www.bio-light.com/ultra. html
Foley, J. D., van Dam, A., Feiner, S. K., & Hughes, J. F. (1996). Computer Graphics:Principlesand Practice in
C (2nd ed.). Reading, MA: Addison-Wesley.
Giangrandi,
1.
(2013,
December). Luminous intensity and luminousflux converter. Retrieved August 2014,
from giangrandi.ch: http://www.giangrandi.ch/optics/lmcdcalc/lmcdcalc.shtml
72
Integrated Environmental Solutions Limited. (n. d.). VEfor Architects I Architecturalanalysispackage.
Retrieved June 2014, from Integrated Environmental Solutions: http://www.iesve.com/software/vefor-architects
Philips Lumileds Lighting Company. (2014, May 27). LUXEON Rebel ColorLEDs[datasheet]. Retrieved from
Philips Lumileds Lighting Company: http://www.philipslumileds.com/uplo ads/265/DS68 -pdf
Philips Lumileds Lighting Company.
(2014,
November 3). LUXEON Rebel White LEDs [datasheet]. Retrieved
from Philips Lumileds Lighting Company: http://www.philipslumileds.com/uploads/2o/DS63-pdf
Radiance WWWServer. (n.d.). Retrieved June 2014, from http://radsite.lbl.gov/radiance/
Robert McNeel & Associates. (n.d.). Grasshopper- algorithmic modelingfor Rhino. Retrieved June 2014, from
http://www.grasshopper3d.com/
Robert McNeel & Associates. (n.d.). Rhinoceros. Retrieved June 2014, from https://www.rhino3d.com/
Roudsari, M. S. (n.d.). Ladybug + Honeybee I Grasshopper. Retrieved June 2014, from Food4Rhino I Apps for
Rhino and Grasshopper: http://www.food4rhino.com/proj ect/ladybug-honeybee?ufh
Smith, W.
J. (1966). Modern OpticalEngineering - The Design ofOpticalSystems
(1st ed.). New York: McGraw-
Hill.
Solemma, LLC. (n.d.). DIVA ForRhino. Retrieved June 2014, from http://diva4rhino.com/
Synopsys Optical Solutions Group. (n.d.). LightTools -Synopsys OpticalSolutions. Retrieved June 2014, from
Synopsys.com: http://optics.synopsys.com/lighttools/
Weisstein, E. W. (n.d.). Gaussian Function. Retrieved August 2014, from MathWorld -- AWolfram Web
Resource: http://mathworld.wolfram.com/GaussianFunction.html
Zemax, LLC. (n.d.). Zemax - OpticStudio
I Zemax. Retrieved June 2014, from Zemax - Optical and
Illumination Design Software I Zemax: https://www.zemax.com/products /opticstudio
73
74
5 I DESIGNING PHOTOTHERAPY
5.1 Overview
The purpose of this chapter is to explore the application of our analysis methods to various user
interaction scenarios in the CityHome apartment. In order to do so, we will first propose a lighting
configuration that can provide adequate illumination under some of the most common user
occupancy conditions. A few preliminary fixture concepts will be given consideration before settling
on the scheme to be used for the rest of the chapter. Second, we will explore the potential
performance of this lighting scheme under different user interaction scenarios. In addition to
differing spatial contexts, each of the scenarios will be staged to demonstrate changes in spectral
power distributions (SPDs), irradiance rates, and other variables in a way that may require a less
"linear" approach than the methodology discussed in Chapter 4. Finally, we will review the results of
our exercises with regard to design choices. We will not conclusively claim that the dosages achieved
in our interaction scenarios are (or are not) adequate for phototherapeutic purposes - in order to do
so, it would take a more comprehensive survey of the medical literature, as well as physical
experiments/testing. In summation, these interaction studies simply aim to lay the groundwork for
more refined design exploration and development.
5.2 Design Development
With an understanding of our analysis methodology in place, we can now go about developing a
lighting scheme for the CityHome apartment. The scheme must (i) provide sufficient irradiance at
comfortable distances and positions in the apartment,
(2)
keep glare to a minimum, (3) fit the
tectonic and aesthetic modularity of the CityHome system, and (4) minimize occupation of storage
space or other passive utilities in the CityHome.
5.2.1 Linear Array
In order to keep the lamps' form factor to a minimal size, initial lighting schemes focused on
developing a linear array module with a relatively narrow beam spread. By leveraging information
from the CityHome's Kinect sensor concerning the location of a user in space, the appropriate array
could, in turn, be continuously aimed at the user during a phototherapy session. Three schemes were
developed with this approach in mind; we will call them Linear A, Linear B, and Linear C (Figs 5-1-3)-
75
We will briefly summarize the implications of these studies for developing the proposed lighting
scheme for this thesis.
In an attempt to balance concerns for minimizing glare with maintaining a narrow beam spread,
the Linear A scheme (Fig. 5-1) utilizes a row of LEDs aimed at an extruded parabolic reflector. In
turn, the light transmitted to the user would be reflected light with a moderately diffuse quality,
depending on the surface of the reflector. While Linear A maintains a tight beam width-wise, the
extruded geometry of the array would result in considerable beam-spread length-wise. Further, the
dimensions of the Linear A proved to be both tectonically and aesthetically cumbersome to
incorporate in tighter areas of the CityHome apartment, such as the kitchen.
Linear B (Fig.
5.2)
consists of a compact, modular strip that can be interchanged with the
CityHome's ambient lighting strips in appropriate areas. Like Linear A, Linear B relies on parabolic
reflectors to transmit light from LEDs, but with a key difference. Each LED is aimed at a section of a
hyperbolic paraboloid, resulting in completely parallel rays (depending on the quality of the
reflector). While a major setback of Linear A was too wide a beam-spread, Linear B erred in the
opposite direction - too narrow. The tightly collimated beams would be efficient at transmitting the
most illumination to longer distances, but the coverage area would likely remain too small. Further,
the discontinuous pattern of reflectors would likely create a zebra-like pattern, exacerbating any
problems with glare.
Linear C (Fig- 5-3) shares a similar form factor to Linear B, but most of the transmitted light is
radiated directly from the LEDs. Reflector cells for each LED are used to re-direct only wide-angle
rays, instead of all or most of the radiated light. Each reflector cell has a parabolic profile in plan and
a freeform profile in section. Like the previous two linear systems, the parabolic profile collimates
rays with a wide-angle in plan. However, the freeform profile in section "folds" increasingly
divergent rays in section back towards the center of the beam. Although the approach to reflector
design is more nuanced in the Linear C scheme, it still seems unlikely to overcome the issue of glare
caused by the high contrast ratio between the lamp module and adjacent surfaces. Also, the moving
parts involved with the concept of pivoting linear array introduce potential for mechanical failure
and/or the need for routine maintenance.
Further design iterations may or may not be able to resolve these issues, but for the purpose of
this thesis - developing an analytical model for dynamic phototherapy - dynamic linear lighting
schemes were set aside in favor of static area arrays.
76
I
I
Fig. 5.1: Drawings of Linear A lamp module.
I I(
I 26 II 16 I I(
Fig. 5.2: Drawings of Linear B lamp module.
I 16 I
Fig. 5.3: Drawings of Linear C lamp module.
5.2.2 Area Array
The area array scheme trades some of the flexibility and nearly universal coverage of the linear
lighting schemes in favor of user comfort and cleaner implementation. Each area array takes the
form of a fixed panel that provides a more diffuse light and large coverage area within a somewhat
limited range. The dimensions and mounting of each panel are tailored to its specific location in the
apartment. A panel may be equipped with multiple arrays of LEDs in varying colors, with each color
in response to a specific phototherapeutic mode. Further, each panel may be equipped with a
proximity sensor for evaluating the distance of the user from the panel. Along with the CityHome
Kinect sensor, information about the location of the user in space maybe used to continuously adjust
the appropriate panel's duty cycle and/or required phototherapy session time.
With these principles in mind, a lighting scheme consisting of six locations throughout the
apartment is proposed (Figs. 5.4-6), with each installation having its own designated abbreviation:
(Ov), an 8" x ioo" array serving as an overheadlight; (So), an 18" x 37" array adjacent to the sofa;
(Fr),a 25" x 30" array mounted to thefront of the CityHome module and doubling as a cabinet door;
(Ki), a 21" x 33" array mounted in the kitchen area and doubling as a custom refrigerator cabinet
panel; (Va), a pair of 6" x 29" arrays mounted in the vanity area of the bathroom; (Sh), a 8" x 69"
array mounted in the shower area.
78
71
Sh
ii
1-a
Fig. 5.4 Plan view of area phototherapy lighting scheme.
SSo
Fig. 5.5: Longitudinal section perspective of area phototherapy lighting scheme.
79
Fig. 5.6: Transverse section perspective of area lighting scheme.
5.3 Scenario A: Waking
It is 6:30 AM Monday morning. Over the course of 20 minutes, panel (Ov) initiates a "wake-up"
mode. An array of blue LEDs increases in brightness at a constant linear rate, starting with a duty
cycle o.o (therefore, o lux) and ramping up to a duty cycle that is equivalent to the dosage rate of 450
lux shining continuously. The user does not wake up until 5 minutes into the cycle. S/he, however,
(stubbornly) chooses to remain in bed for another
15
minutes, until the lamp reaches the end of the
wake-up cycle. Afterwards, s/he chooses to sit on the sofa near panel (So). An array of white LEDs
switches on, with a duty cycle equivalent to a continuous dosage rate of io,ooo lux. The user remains
on the sofa, reading a book until the phototherapy session is complete. What is the active fluence for
the time that the user is in bed, and what (minimum) additional time is required on the sofa for the
user to receive a totalfluence of 3 J/cm2 ? (See Figs. 5.7-8 for illuminance patterns.)
8o
lux
(Ix)
500
0
100
Fig. 5.7: Illuminance pattern for (Ov) at 24" above ground level. Target point is marked (+).
lux (Ix)
0
5000
10 00
Fig. 5.8: llluminance pattern for (So) at 54" above ground level. Target point is marked (+).
5.3.1 Setup parameters
Setup parameters for the analysis are given in the following table (Table 5-1):
Table 5.1: Scenario A Setup Parameters
Symbol
Name
(So)
(Ov)
LED Color
-
LED Model No.
- LXML-PB02
Blue
White (3000 K)
LXM3-PW71
'l
83
94
0O.5
a/4
;r/4
Optics Transmission Efficiency (0-1)
ke
0.9
0.9
Constant Attenuation Factor (0-1)
kc
0
0
Linear Attenuation Factor (0-1)
k
0
0
Quadratic Attenuation Factor (0-1)
kq
1
1
No. of Rows (#)
m
25
18
No. of Columns (#)
n 4
Luminous Flux (lm)
Half Width at Half Maximum, w/added optics (rad)
5.3.2 Lying in Bed
Solving for Eq. 4.14 at the target point 24" above ground level yields the following value:
E,(0, d, V) = 814 lux
Solving for irradiance is as follows, starting with Eq. 4.18:
E =
683 - f
0
P(A)y A) d1I
814
683 - (0.707107)
E
814
482.9541
E = 1. 6855 W/m 2
82
9
In order to determine a duty cycle kd for our lamp (from Eq.
4.21)
equivalent to 450 lux, we may
notice that in Eq. 4.18 there is a direct relationship between the illuminance value E, and the
irradiance value E. With all other variables remaining constant, we can simply divide our desired
equivalent illuminance value by the calculated illuminance value:
450 lux
= 0.5528
814 lux
kd=
In order to calculate total phototherapeutic fluence, we may take advantage of the convenient detail
that lamp (Ov) ramps up at a constant linear rate to the desired duty cycle over the course of 15
minutes (or goo seconds). First, let us temporarily consider what the total fluence would be if the
lamp were operating at the peak duty cycle (0.5528) for the entire length of time that it is on. Starting
with Eq. 4.24:
E
ton
(ton + toff
t
10,000 cm2/m2
(1.685
5 W/m
10,000 m/m2
2
j = (0.5528)
(10,000 CM2/M2
j = 0. 1118J/cm
(1200 s)
2
Of course, we do know that the lamp (Ov) is constantly ramping up its duty cycle over this course of
time from o.o to 0.5528. This makes calculation of the total fluence of the lamp somewhat akin to
calculating the area of a bisecting right triangle compared to our first calculation, so we may simply
cut the earlier calculation in half:
j = (0.5)(0.1118 J/cm2 ) = 0.0559J/cm
2
Next, we must also consider that the user is asleep for the first five minutes of the wake-up cycle. If
we assume that the fluence achieved during this time does not contribute to our total dosage (i.e., the
user' s eyes are closed), then we may calculate the amount achieved during that time and subtract it
ton
ton +toff
E
)
from the overall fluence to get the final value. Starting again with Eq. 4.24:
10,000 CM2/M2
j = (0.5528 - 0.25)
(1.6855
2
W/m
1.,85cm
/2 2
/m
(10,000
(300s)
/M
j = 0.0070 j/cm 2
j = 0.1118j/cm
2
0.0070 j1/cm 2 = 0.1048 J1/cm 2
-
5.3.3 Sitting on Sofa
Solving for Eq. 4.14 at the target point 24" above ground level yields the following value:
Ev(O, d, qp) = 17,020 lux
Solving for irradiance is as follows, starting with Eq. 4.18:
780 E
E =-
683 - f380 P'(1)Y(11) dA
E
17,020
683 - (0.670503)
=
17,020
E
=457.9535
E = 37.1653 W/m 2
In order to calculate the time that the user needs to sit on the couch to achieve a total fluence of 3
J/cm2 may be calculated by inserting this and our previously calculated dosage into Eq. 4.24:
(
ton
\con+ to014
(
Et
10,000 cm2/m2)
/
!
3j/CM2 =0.1048 j/cm2 + (1)
3j1/cm
2
37.1653 W/m2 t
(10,000 CM2/M2)
= 0.1048J/cm2 + (1)(0.0037 W/cm 2 )t
84
3j/cm 2 - 0.1048 J/cm 2 = (1)(0.0037 W/cm 2 )t
2.8952 J1/cm 2 = (1)(0.0037 W/cm 2 )t
2.8952 J/cm 2 =
0.0037 W/cm 2
t = 783 s
Thus, the user must remain by panel (So) for an additional 783 seconds (or 13 minutes, three
.
seconds) to achieve a total fluence of 3 J/cm2
5.4 Scenario B: Washing
The user proceeds to wash-up for the day, and wishes to relieve some minor upper body
bruises/abrasions from a rough weekend of skiing. S/he spends a total of 8.2 minutes in the shower
(the typical shower time for the average American), and proceeds to brush teeth for the American
Dental Association's recommended minimum of
2
minutes. During this time, the red LED arrays of
panels (Sh) and (Va) operate at full power. Disregarding any incidental turning around/away from
the light, what is the estimated activefluence achieved over this time period? (See Figs- 5.9-10 for
illuminance patterns.) Assume that the photoactive agent we are targeting is cytochrome c oxidase
(see the action spectra for CCO in the appendix, Fig A.i, p.103).
I
2
II
II
II
II
lux (lx)
0
10000
20000
Fig. 5.9: Illuminance pattern for (Sh) at 54" above ground level. Target point is marked (+).
I
I
EU
-aI
lux (Ix)
0
5000
10000
Fig. 5.10: Illuminance pattern for (Va) at 54" above ground level. Target point is marked (+).
86
5.4.1 Setup Parameters
Setup parameters for the analysis are given in the following table (Table 5.2):
Table 5.2: Scenario B Setup Parameters
Symbol
(Sh)
(Va)
LED Color
- Red
Red
LED Model No.
-
Name
0,
LXM2-PD01-0060
LXM2-PD01-0060
83
94
005
:T/4
a/4
Optics Transmission Efficiency (0-1)
ke
0.9
0.9
Constant Attenuation Factor (0-1)
k,
0
0
Linear Attenuation Factor (0-1)
k
0
0
Quadratic Attenuation Factor (0-1)
kq
1
1
No. of Rows (#)
m
23
15(x2)
n
4
3(x2)
Luminous Flux (1m)
Half Width at Half Maximum, w/added optics (rad)
No. of Columns (#)
5.4.2 Showering
Solving for Eq. 4.14 at the target point 54" above ground level yields the following value:
Ev(0, d, qp) = 13,804 lux
Solving for irradiance is as follows, starting with Eq. 4.18:
E =
780
683 -380
E
=
P'(A)y(A) d2
13,804
683 - (0.707107)
13,804
482.954081
2
E = 28.5824 W/m
87
Solving for estimated active dosage over the course of 8.2 minutes (492 s) and at a duty cycle of i.o is
as follows, starting with Eq. 4.23:
Ia
7 80
E
ton
10,000 cm2/m2
ton + toff
~(28.5824
Ia Ja
= (1)
((85
a10,000
Ja =
P' A)A(A)dA
W/M2)
2
m/ - (0.5581)
CM 2/M 2
)(492
(9s
s
0.7848 1/cm 2
5.4.3 Brushing Teeth
Solving for Eq. 4.14 at the target point 66" above ground level yields the following value:
Ev(0, d, T) = 7,837 lux
Solving for irradiance is as follows, starting with Eq. 4.18:
E=
780
,683 -f38 0 P'(A)y(A) dA
E
=
7,837
683 - (0.707107)
7,837
482.954081
E = 16.2272 W/m 2
Solving for estimated active dosage over the course of 2 minutes
(120 s)
and at a duty cycle of i.o is as
follows, starting with Eq. 4.23:
Ia
Ja
=
ton
( ton + toff
Jk
/E
780
E
*f38 0
P'(A)A(A)dA
P'tAtct2
10,000 cm /m
(16.2272 W/m 2 )2 . (0.5581)
2
10,000 cm / m
88
2
(120s)
Ja = 0.1087 J/cm 2
Thus, the total estimated active fluence for the user while washing up is as follows:
Ja = 0.7848 J/cm 2 + 0.1087 J/cm 2
=
0.8935 J/cm 2
5.5 Scenario C: Working
The user proceeds to set about the work for the day (writing a thesis, coincidentally). While sitting at
the table in desk mode, the white LED array of panel (Fr) operates at a duty cycle equivalent to a
continuous dosage rate of approximately io,ooo lux. After 15 minutes, the user paces around, then
moves to the sofa to read a research paper. In turn the white LED array of panel (Fr)switches off, and
the blue LED array switches on, operating at a duty cycle equivalent to a continuous dosage rate of
350 lux. What is the active fluence achieved in the time period in which the user is sitting at the desk,
and how much additional time will it take for the user to receive an estimated active fluence of 3
J/cm2 while sitting on the sofa? (See Figs. 5.11-12 for radiation patterns.) Assume that the
photoactive agent we are targeting is melanopsin (see the action spectra for melanopsin in the
appendix, Fig A.i, p.103)-
89
lux (Ix)
0
5000
10000
Fig. 5.11: lluminance pattern for (Fr) at 54" above ground level. Target point is marked (+).
lux (lx)
0
2500
5000
Fig. 5.12: Illuminance pattern for (Fr) at 54" above ground level. Target point is marked (+).
90
5.5.1 Setup Parameters
Setup parameters for the analysis are given in the following table (Table 5-3):
Table 5.3: Scenario C Setup Parameters
Symbol
Name
(Fr) @ Desk
LED Color
- White (3000 K)
LED Model No.
-
Luminous Flux (lm)
0,
Half Width at Half Maximum, w/added optics (rad)
LXM3-PW71
94
(Fr) @ Sofa
Blue
LXML-PB02
83
QO.5 n/4
g/4
0.9
Optics Transmission Efficiency (0-1)
ke
0.9
Constant Attenuation Factor (0-1)
k,
0
0
Linear Attenuation Factor (0-1)
ki 0
0
Quadratic Attenuation Factor (0-1)
kq
1
1
No. of Rows (#)
m
12
15
No. of Columns (#)
n
12
15
5.5.2 Sitting at Desk
Solving for Eq. 4.14 at the target point 54" above ground level yields the following value:
Ev(O, d,p) = 10, 331 lux
Solving for irradiance is as follows, starting with Eq. 4.18:
E =
780
683 -f 380 P'(A)y(A) dA
13,804
683 - (0.670503)
E =13,804
457.953549
E = 30.1428 W/m 2
91
Since the illuminance value of
lux is relatively close to the initial goal of io,ooo lux in our
10,331
scenario description, we will leave the duty cycle factor kd at 1.0. Solving for estimated active dosage
over the course of
15
minutes (492 s) and at a duty cycle of i.o is as follows, starting with Eq. 4.23:
Ia
E -f3'
1ton P'(A)A(A)dA
10,000 cm2/m2
a
ton + toff)
=(1)
((30.1428 W/m2)
(0.1871)
(900s)
10,000 CM2/M2
Ja = 0.50761/cm 2
5.5.3 Reading on Sofa
Solving for Eq. 4.14 at the target point 54" above ground level yields the following value:
E(O, d,qp) = 1, 267 lux
Solving for irradiance is as follows, starting with Eq. 4.18:
E =
7807
683 - f380 P'(A)y(A) dA
E
=
1,267
683 - (0.670503)
1,267
457.953549
E = 28. 5824 W/m 2
As demonstrated in interaction scenario A, we may readily determine the appropriate duty cycle of
our lamp needed to emulate 350 lux by dividing our desired equivalent illuminance value by the
calculated illuminance value:
k
350 lux
= 1,267 lux
= 0.2762
92
In order to calculate the time that the user needs to sit on the couch to achieve an estimated active
fluence of 3 J/cm2 may be calculated by inserting this and our previously calculated dosage into Eq.
4.23:
(a
ton
( ton+ tof )
3 j/cm
2
d2
2())A(2
f387800 PP'A)A(A)dA
/E
'\(
10,000 cm 2 /m 2
28.5824 W/m 2 -0.947312\
2
2
2
= 0.5076J/cm + (0.2762)
3 J/cm 2
-
J
1000
cm
94m
10,000 CM 2/M 2
t
0.5076 J1/cm 2 = (0.2762)(0.0027 W/cm 2 )t
2.4924j1/cm
2
)
(0.2762)(0.0027 W/cm 2
t = 3,343 s
Thus, the user must remain by panel (So) for an additional 3,343 seconds (or 55 minutes, 43 seconds)
2
.
to achieve a total estimated active fluence of 3 J/cm
5.6 Discussion
We have demonstrated methods of determining whether and/or how interactive phototherapy may
be effective in the context of interior spaces and user activities. It is possible to see how geometry,
spatial conditions, user activities, and time may all affect the performance of a phototherapy system.
Conversely, it is also possible to see ways in which the design and performance parameters of the
phototherapy system may have to be adjusted. In scenario A, for example, it might very well be the
case that fewer LEDs are needed in lamp (Ov) if it is never intended for the lamp to perform beyond a
level equivalent to 450 lux. In scenario B, it might also end up being the case that it is simply
unsuitable to implement phototherapy for minor pain relief because the fluences are too low and the
irradiation times are too short. Or, in scenario C, it's possible that the irradiation time required
while the user is on the sofa is too long; another lamp might provide better coverage, or the duty
cycle of the existing lamp (Fr) may have to be increased. This dynamic way of understanding how
user behavior may guide phototherapy system design would be an improvement over existing
phototherapy techniques, which do not allow for changes in user position during phototherapy
93
sessions. It is true that we have not explicitly referenced actual phototherapy fluences documented in
the medical literature, due to the fact that (a) dosages for even the same condition may vary by a
significant order of magnitude, and (b) parameters for determining dosages are more complex than
the scope of this thesis will allow. If dosage goals were to be made more explicit in further studies,
then our current methods should be able to accommodate them with some success. For the current
time, however, we have established the groundwork for how interactive phototherapy may be used to
inform interior architecture - and vice versa.
94
95
96
6 I CONCLUSION
6.1 Summary
This thesis has sought to demonstrate only one of potentially many ways in which the paradigm of
interactive architecture (IA) is uniquely poised to address issues concerning user health in relation
to the built environment.
In Chapter i, we noted emerging interests in (i) healthcare innovation,
(2)
the "quantified self"
paradigm, and (3) interactive architecture all converging on the notion of continuously monitoring
and/or adapting to information about a user's health or well-being. For healthcare innovation, this
would offer the possibility for acquiring continuous patient information in the context of everyday
life, potentially providing insight on health conditions that are difficult to diagnose or treat. For the
"quantified self" paradigm, information about how a person's day-to-day activities affect his/her
health may be useful for pursuing a sense of wellness in more general terms. For interactive
architecture, accessible information about user health could augment the functioning of buildings
and spaces while enhancing user comfort and well-being. Having established underlying motivations
and previous work within this research context, we identified light, particularly for phototherapy, as
a modality for further exploration.
In Chapter 2, we explored some basic concepts of light as they may apply to phototherapy. First,
we discussed light in terms of its independent physical properties (with the exception of photometric
units, which are based on the human eye). Second, we surveyed a few of the physiological effects light
may have on the body via both visual and non-visual pathways. For non-visual pathways, we discussed
some of the physiological responses according to wavelength. Third, we discussed four broad
categories of phototherapeutic methods, as well as where there is still room for improvement for the
implementation of phototherapy. In response to the further goals for phototherapy implementation,
we proposed the concept of "dynamic phototherapy." This passive, continuous form of therapy
would be able to take into account user information about (i) what phototherapeutic method is
desired, (2) where the user is in relation to phototherapeutic devices, (3) how the phototherapy is to
be implemented, which in turn is a function of the user's activity at the time of therapy.
In Chapter 3, we examined the CityHome project as a platform for supporting interactive
phototherapy. The CityHome's spatial configurability, tectonic configurability, user interfaces, and
hardware/software architecture were discussed. In illustrating the configuration and functionalities
of the CityHome across these areas, we are able to find a fit between the project and our conception
97
of dynamic phototherapy. First, touch, gesture and voice commands become methods by which the
user can specify what mode of phototherapy is desired. Second, the CityHome's Kinect sensor, and
the hardware/software architecture's ability to incorporate additional sensor systems in ad hoc
manner, become methods for establishing where the user is in relation to phototherapeutic devices.
Third, the combination of spatial configuration, user commands, and user location may provide
insight on the user's activity at the time of therapy, which in turn may provide information for how
the phototherapy is to be implemented.
In Chapter 4, we constructed a methodology for designing and analyzing dynamic phototherapy.
As a proof of concept, we sought to reconstruct an analytical model of an existing commercial
phototherapy lamp. First, we derived an equation for describing the lamp's illumination field, taking
into account angle of emission, distance, and angle of incidence relative to the light sources within
the lamp. Second, we derived an equation for determining irradiance, taking into account
illuminance and the lamp's spectral power distribution. Third, we derived an equation for
determining active dosage, taking into account irradiance,the action spectra of the photoactive
agents, irradiationtime, and the lamp's duty cycle. With these three equations we were able to arrive
at an analytical model for our commercial lamp case study.
In Chapter 5, we applied our methodology to the design and analysis of three interaction
scenarios in the CityHome apartment. First, we analyzed a scenario in which the user is waking up,
and involved varying illuminances, different lamps, and different phototherapeutic spectra. Second,
we analyzed a scenario in which the user is bathing, and involved similar illuminances, different
lamps, and the same phototherapeutic spectra. Third, we analyzed a scenario in which the user is
working, and involved different illuminances, the same lamp, and different phototherapeutic
spectra.
The contributions of this study, in conclusion, are twofold. The first is that of a physical
prototype capable of serving as a platform for dynamic phototherapy, the CityHome project. The
second is that of an analytical prototype for designing and analyzing phototherapy, which comes in
three parts: equations for calculating illuminance, converting illuminance to irradiance, and
converting irradiance to an active dosage. A corollary of this latter contribution is a rudimentary
implementation of these equations in a 3D/parametric modelling context, as has been demonstrated
in the previous two chapters.
98
6.2 Further Research
There are plenty of additional areas that could not be covered in the scope of this study. We will give
consideration to the following, each with increasingly broad scope and implications: (i) the limits of
the analytical model;
(2)
further design refinement via physical prototyping and experiments; (3) the
incorporation of direct physiological feedback; (4) Computer applications for simulating dynamic
phototherapy, particularly ones that may be accessible to architectural designers; (5) Physical
tools/devices for designers; (6) other/additional therapeutic modes that may be implemented in
interactive architectural systems; (7) dynamic therapeutic methods in the larger "internet of things"
(loT) and the built environment.
ANALYTICAL
LIMITS.
There are a number of physiological variables that still remain to be incorporated
into an analytical model. Skin complexion, for example, may have an effect on dosage as differing
levels of pigmentation may allow more or less light to penetrate the skin. There has been research
done on this, but the categories analyzed are still rather broad. Further, it is known that different
wavelengths of light do not penetrate the skin at an even rate; typically, longer wavelengths of light
are able to penetrate deeper into the body. This is an important factor to consider when calculating
irradiance for sub-dermal target sites. We should also keep in mind that other non-visual, userspecific information, (e.g., genetics, skin conditions, etc.) may affect the phototherapeutic dosage
appropriate for an individual user/patient.
This study also made some conscious assumptions about optical variables that may influence the
effectiveness of phototherapy. With the exception of broad-spectrum (white) light, we did not go into
the potential for compound phototherapy, i.e. attempting to conduct two distinctly different
phototherapeutic modes at the same time. This has to do with unknowns regarding interference
effects between various photoactive agents. Further, it is not always clear whether other optical
properties such as coherence, polarization, or collimation have any effect on phototherapy
effectiveness. The working assumption, however, is that due to the heterogeneous nature of the
dermal layers, any such order that may be inherent in the light is quickly scattered into differing
coherences, polarities, and directions as it penetrates through the skin.
PHYSICAL PROTOTYPING AND TESTING. The transition from an analytical model of dynamic phototherapy
to an operational physical prototype brings with it another category of variables and challenges. For
one, there would have to be a way of monitoring the output of the light sources to ensure that they
are operating at the expected brightness. Some phototherapy lamps already come equipped with
closed-loop monitoring mechanisms, as the performance of a lamp is known to drift to a nonnegligible extent over time. The performance of the electronic components, the effects of diffusers,
reflectors, lenses, or other intervening optical hardware would also have to be taken into
99
consideration in both analyzing the lamp design and evaluating the built prototype's performance.
This is also to say nothing of evaluating the significance of other light sources in the room in or the
individual characteristics
of human subjects in evaluating the appropriate dosage. These
considerations, too, will have to be left for later investigation.
BiOLOGICAL FEEDBACK. If dynamic phototherapy is to be truly interactive, then some consideration
may have to be given to the concept of biofeedback. Indeed, at the time of this writing, the latest SDK
for the Windows Kinect sensor incorporates computer vision algorithms for detecting a person's
pulse from video capture. Such algorithms also exist independently outside of the Kinect system.
Further, more nuanced information may be given to physiological data simultaneously monitored by
external apps or wearable devices: blood glucose levels, pulse oximetry, photoactive agent levels, or
similar data. A novel trajectory for later research could be whether vital signs or other physiological
data can be used in real-time for setting or evaluating phototherapeutic dosage parameters.
SIMULATION
TOOLS. Although this study has derived analytical equations for evaluating dynamic
phototherapy and demonstrated their applicability with rudimentary parametric definitions, a
comprehensive, accessible analysis tool would be useful. This could take the form of a plugin for an
existing modelling program used by architectural designers, such as for Rhino or Autodesk Revit.
Alternatively, we could envision a standalone application with interoperability between other design
and analysis programs. Further consideration might also lead to an online, cloud-based application
could be foreseeable for analyzing particularly complex models or easily sharing information
between multiple design collaborators.
PHYsICAL TOOLKITS FOR DESIGNERS.
The reciprocal of more comprehensive software tools for
evaluating dynamic phototherapy would be physical toolkits accessible to architectural designers.
For example, it would not be difficult to imagine a smartphone-based add-on module that
incorporates the necessary sensors for producing spectral power distributions. There are devices
that have implemented this in a way that involves a diffracting prism, smartphone's camera, and a
corresponding application; however, there is reason to wonder whether the color filters over the
camera's image sensors may have some effects on the accuracy of the spectrum reading. We could
further imagine Arduino or other microcontroller hobby electronics kits that specifically for
measuring irradiance or mapping a lamp's spatial radiation pattern. This would be useful in
evaluating the effectiveness of physical models or prototypes in the design process. Both
smartphone- and microcontroller-based devices would, in turn, would have interoperability with
corresponding desktop applications in order for measured physical data to re-inform digital designs.
OTHER THERAPEUTIC MODES.
The potential for other environmental modalities to be deployed in ways
analogous to dynamic phototherapy should also be considered. For example, Julian Treasure has
100
written and spoken about how ambient sound or noise may effects on our health; a natural extension
of this trajectory could be the selective deployment (or suppression) of ambient sound to promote
user health. The development of modern HVAC systems - as documented by Reyner Banham's
seminal book, The Architecture of the Well-Tempered Environment - was largely driven out of
concerns for building occupants' health. In turn, application of interior heat and/or cooling in a
therapeutic mode would be a novel contribution to the field of environmental controls.
BEYOND THE
CITYHOME. Finally, a long-term goal for dynamic phototherapy could be to extend its
implementation beyond domestic environments and into the larger built environment. One vehicle
for this goal lies in wearable phototherapeutic devices, some of which already do exist. We can
further imagine dynamic phototherapy devices being implemented in places where users may spend
a significant portion of time, such as at work or school. At the highest level, the potential or support
for dynamic phototherapy could become another criterion against which architecture is evaluated.
Threads of this thought, such as circadian potential, are already being discussed; dynamic
phototherapy would propose to explicitly quantify, track, and control the properties of the light
around us with regard to circadian rhythm.
6.3 Concluding Remarks
There are a substantial number of trajectories for further research for dynamic phototherapy, as
illustrated in the preceding paragraphs. There is demonstrable merit, specifically the promotion of
people's health, in pursuing these trajectories. As healthcare innovation and the IoT paradigms
show increasing interest in connecting information about our health with the environment around
us, architects - as designers of the built environment - should have a leading role to play in shaping
further investigations into the impact of the built environment on our health.
101
102
APPENDIX
Figures
-CIE
1931 (a)
melanopsin (b)
1-
--
ilirbin (c)
-CCO (d)
0.8
0.6
------.9
0.4
0
400
450
500
600
550
650
700
750
wavelength (nrn)
Fig. A.1: Relative action spectra of various photoactive agents, including melanopsin (b),
bilirubin, and cytochrome c oxidase or CCO (b). The luminosity function of the human eye, CIE
1931, is included for reference (a).
-CFL
0.8
0.6
0.4
02
01
400
450
500
550
600
650
700
750
Fig. A.2: Typical spectral power distribution for a 6500 K compact fluorescent light bulb.
103
6500K
-
I
-
0.8-
-
Blue (a)
Green (b)
Lime (e)
PC Amber (d)
Red-Orange (e)
Red (f)
0.6
0.4
I
400
450
500
750
700
650
600
550
wavelength (nm)
Fig. A.3: Spectral power distributions for Philips' LUXEON Rebel ES' LEDs in blue (a), green (b),
lime, PC amber (d), red-orange (e), and red (f).
-
1-
0.6
S0.4
02
0
400
450
500
550
600
650
700
750
wavelength (nm)
Fig. A.4: Spectral power distribution of Philips' LUXEON Rebel * LED in white, 3000K.
104
3000 K
Tables
Table A.1: Selected Photometric LED Data for Analyses
Philips' LUXEON Rebel/ES*
Blue
Green
Lime
PC Amber
LXML-PB02
LXML-PMO1-0100
LXML-PX02-0000
LXM2-PL01-0000
Typical Luminous Flux
(Im)
83
161
361
198
FWHM, w/o lens (deg)
125
125
125
120
FWHM, w/lens (deg)
90
90
90
90
Lens efficiency factor
(0-1)
0.9
0.9
0.9
0.9
Est. Peak Intensity, w/o
lens (cd)
24.5
47.6
107
63
Est. Peak Intensity,
w/lens (cd)
40.6
78.7
176.4
97.2
Peak Wavelength (nm)
470
530
567.5
591
20
30
100
80
Part Number
Spectral FWHM (nm)
Table A.2: Selected Photometric LED Data for Analyses (continued)
Red-Orange
Red
White
LXM2-PH01-0070
LXM2-PD01-0060
LXM3-PW71
Typical Luminous Flux
(Im)
134
119
94
FWHM, w/o lens (deg)
125
125
120
FWHM, w/lens (deg)
90
90
90
Lens efficiency factor
(0-1)
0.9
0.9
0.9
Est. Peak Intensity, w/o
lens (cd)
39.6
35.2
29.9
Est. Peak Intensity,
w/lens (cd)
65.5
58.2
46
617
627
-
Philips LUXEON Rebel/ES
20
20
Part Number
Peak Wavelength (nm)
Spectral FWHM (nm)
105
Table A.3: Common Outdoor Illuminance Levels
Condition
Illuminance (lux)
Sunlight
107,527
Full daylight
10,752
Overcast day
1,075
Very dark day
107
Twilight
10.8
Deep twilight
1.08
Full moon
0.108
Quarter moon
0.0108
Starlight
0.0011
Overcast night
0.0001
Table A.4: Common Indoor Illuminance Levels
Activity
Illuminance (lux)
Public areas with dark surroundings
20-50
Simple orientation for short visits
50- 100
Working areas where visual tasks are only occasionally performed
100 -150
Warehouses, homes, theatres, archives
150
Easy office work, classes
250
Normal office work, PC work, library study, groceries, show rooms, laboratories
500
Supermarkets, mechanical workshops, office landscapes
750
Normal drawing work, detailed mechanical workshops, operation theatres
1,000
Detailed drawing work, very detailed mechanical work
1,500 - 2,000
Performance of visual tasks of low contrast and very small size for prolonged periods of time
2,000 - 5,000
Performance of very prolonged and exacting visual tasks
Performance of very special visual tasks of extremely low contrast and small size
io6
5,000 - 10,000
10,000 - 20,000
107
io8
FIGURE REFERENCES
Fig 1.1: (Design that Matters, 2014)
Fig. 1.2a: (Herf & Herf,
2009)
Fig. 1 .2b: (Philippe Rahm Architects & fabric I ch,
2001)
Fig. 1 .2c: (La Lumiere, LLC)
Fig. 1.2d: (GoodLux Technology,
2014)
Fig. 1.3a: from (Aalvar Aalto Foundation)
Fig. 1.3b: (Andersen, Mardaljevic, & Lockley, 2012)
Fig. 2.1: (Ronan & Gringer, 2013)
Figs. 3.1 - 3.11: Changing Places group archives, MIT Media Laboratory
Fig. 4.1: (Enviro-Med, 1997)
Figs. 4.2 - 4.6: Personal archives
Figs. 5.1 - 5.12: Personal archives
Fig. A.1: Data based on (Hankins, Peirson, & Foster,
2008),
(Hankins, Peirson, & Foster,
and (Karu & Kolyakov, 2005)
Fig. A.2: Data based on (GE Lighting, 2014)
Fig. A.3: Data based on (Philips Lumileds Lighting Company,
2014)
Fig. A.4: Data based on (Philips Lumileds Lighting Company,
2014)
109
2008),
110
BIBLIOGRAPHY
[uto]. (n.d.). Geco I Grasshopper.RetrievedJune 2014, from Food4Rhino I Apps for Rhino and
Grasshopper: http://www.food4rhino.com/project/geco?ufh
Aalvar Aalto Foundation. (n.d.). paimio. Retrieved December 2014, from
http://www.alvaraalto.fi/net/paimio/paimio.html
Andersen, M., Mardaljevic,
J., & Lockley,
S.W.
(2012).
A framework for predicting the non-visual
effects of daylight - Part I: photobiology-based model. LightingResearch& Technology, 44,
37-52.
Anderson, R. R., & Parrish,
J. R. (1981). Microvasculature
Can Be Selectively Damaged Using Dye
Lasers: A Basic Theory and Experimental Evidence in Human Skin. Lasersin Surgery&
Medicine, 1(3), 263-276.
Arakane, K., Ryu, A., Hayashi, C., Masunaga, T., Shinmoto, K., Mashiko, S.,. . . Hirobe, M. (1996).
Singlet Oxygen (iAg) Generation from Coproporphyrin in Propionibacterium acnes on
Irradiation. BiochemicalandBiophysicalResearch Communications, 223(3), 578-582.
Autodesk, Inc. (n.d.)- 3 D Design & VisualizationSoftware | 3ds Max Design I Autodesk. Retrieved
June 2014, from Autodesk: http://www.autodesk.com/products/3ds-max-design/overview
Autodesk, Inc. (n.d.). EcotectAnalysis- SustainableBuildingDesign Software -Autodesk. Retrieved
2014
June, from Autodesk: http://usa.autodesk.com/ecotect-analysis/
Becker, D., Langer, E., Seemann, M., Seemann, G., Fell, I., Saloga, J., . . . von Stebut, E.
(2011,
June). Clinical Efficacy of Blue Light Full Body Irradiation as Treatment Option for Severe
Atopic Dermatitis. PLoS One, 6(6), i-9.
Boivin, D. B., Boudreau, P., &Tremblay, G. M.
(2012,
June). Phototherapy and orange-tinted
goggles for night-shift adaptation of police officers on patrol. ChronobiologyInternational,
29(5),
629-640.
Brainard, G. C., Hanifin,
(2001,
J. P., Greeson, J. M., Byrne, B., Glickman,
G., Gerner, E., & Rollag, M. D.
August 15). Action Spectrum for Melatonin Regulation in Humans: Evidence for a
Novel Circadian Photoreceptor. TheJournalofNeuroscience,21(i6), 6405-6412.
111
Breault Research Organiz ation, I nc. (n.d.). Key FeaturesofASAP; the OpticalSoftware byBreault
Research (BRO). Retrieved June 2014, from Optical Software, Engineering, and Training by
Breault Research (BRO): http://www.breault.com/software/asap-features
Center For the Built Environment. (n.d.). CenterfortheBuiltEnvironment.Retrieved December
2014,
from Center for the Built Environment: http://www.cbe.berkeley.edu/
Cesarini, J.-P.
(2009,
October-December). Blue light hazards for ocular lesions. Radioprotection,
44(4), 463-478.
DeCusatis, C. (1998). HandbookofAppliedPhotometry. NewYork: Springer.
Design that Matters. (2014). Firefly -Design thatMatters. Retrieved December
2014,
from Design
that Matters: http://www.designthatmatters.org/firefly/
Ellinger, F. (1957)- Medical RadiationBiology. Springfield, IL: Thomas.
Enviro-Med. (1997). Enviro-MedBio-LightUltra1o,oooLUXlghttherapysystem. Retrieved June
2014,
Foley,
from http://www.bio-light.com/ultra.html
J. D., van Dam, A., Feiner,
S. K., & Hughes, J. F. (1996). ComputerGraphics:Principlesand
Practicein C(2nd ed.). Reading, MA: Addison-Wesley.
Fox, M., & Kemp, M. (2009). InteractiveArchitecture.New York: Princeton Architectural Press.
GE Lighting. (2014). Commercial&IndustrialLighting I ProfessionalSolutionsI GELightingNorth
America. Retrieved from http://www.gelighting.com/LightingWeb/na/
Giangrandi, I. (2013, December). Luminous intensity andluminousflux converter.Retrieved August
2014, from giangrandi.ch: http://www.giangrandi.ch/optics/lmcdcalc/lmcdcalc.shtml
Gold, M. H., Sensing, W., & Biron, J. A.
(2011,
December). Clinical efficacy of home-use blue-light
therapy for mild-to moderate acne. JournalofCosmetic & Laser Therapy, 13(6), 308-314.
GoodLux Technology. (2014). Wearable Sun & Light Tracker. Retrieved December
2014,
from
SunSprite: https://www.sunsprite.com/tracklight/
Gooley, J. J., Rajaratnam, S. M., Brainard, G. C., Kronauer, R. E., A, C. C., & Lockley, S.W. (2010,
May12). Spectral responses of the human circadian system depend on the irradiance and
duration of exposure to light. Science TranslationalMedicine,2(31).
Hankins, M. W., Peirson, S. N., & Foster, R. G. (2008, January 31). Melanopsin: an exciting
photopigment. Trends in Neurosciences,31(1), 27-36.
112
Hashmi, J. T., Huang, Y. Y., Osmani, B. Z., Sharma, S. K., Naeser, M. A., & Hamblin, M. R.
(2010,
December). Role of low-level laser therapy in neurorehabilitation. PM& R: The JournalOf
2), S2 9 2- 3 o 5
.
Injury, Function, AndRehabilitation, 2(12, Suppi.
Hastings, M., O'Neill, J. S., & Maywood, E. S. (2007). Circadian clocks: regulators of endocrine and
metabolic rhythms. JournalofEndo crinology, 195,187-198.
Herf, M., & Herf, L.
(2009,
Februrary).flux. Retrieved February
2014,
from f.lux: software to make
your life better: https://justgetflux.com/
H6hmann, D., Waner, M., & Schwager, K. (1993, April). [Yellow light laser photocoagulation of
vascular malformations in the head and neck area] (German article). HNO, 41(4),
173-178.
Huang, Y.-Y., Chen, A. C.-H., Carroll, J. D., & Hamblin, M. R. (2009, September i). Biphasic Dose
Response in Low Level Light Therapy. Dose Response, 7( 4 ), 358-383.
-
Hunt, R. W. (2004). The Reproductionof Colour(6th ed.). Chichester, United Kingdom: Wiley
IS&T Series in Imaging Science and Technology.
Integrated Environmental Solutions Limited. (n.d.). VEforArchitects I Architecturalanalysis
package. Retrieved June
2014,
from Integrated Environmental Solutions:
http://www.iesve.com/software/ve-for-architects
Jackson, R. F., Roche, G. C., & Shanks, S. C.
(2013,
March). A double-blind, placebo-controlled
randomized trial evaluating the ability of low-level laser therapy to improve the appearance
of cellulite. Lasers in Surgery andMedicine, 45(3),141-147.
Jacques, S. L. (2013, June 7). Optical properties of biological tissues: a review. Physics in Medicine
andBiology, 58(11), R3 7 -R6i.
Kandaswamy, S., Akhtar, N., Ravindran, S., Prabhu, S., & Shenoi, S. D. (2013, July/August).
Phototherapy in Vitiligo: Assessing the Compliance, Response and Patient's Perception
about Disease and Treatment. IndianJournalofDermatology, 58(4), 324-328.
Karu, T. I. (1988). Molecular Mechanism of the Therapeutic Effect of Low-Intensity Laser Radiation.
Lasersin the Life Sciences,
2(I),
53-74.
Karu, T. I., & Kolyakov, S. F. (2005). Exact Action Spectra for Cellular Responses Relevant to
Phototherapy.PhotomedicineandLaserSurgery,23,355-361.
113
Karu, T. I., Pyatibrat, L. V., Kalendo, G. S., & Esenaliev, R. 0. (1996). Effects of monochromatic
low-intensity light and laser irradiation on adhesion of HeLa cells in vitro. Lasers in Surgery
andMedicine, 18(2), 171-177.
Kleinpenning, M. M., Otero, M. E., van Erp, P. E., Gerritsen, M. J., & van de Kerkhof, P. C. (2o1).
Efficacy of blue light vs. red light in the treatment of psoriasis: a double-blind, randomized
comparative study. Journalofthe EuropeanAcademy ofDermatologyandVenereology,
26,
219-225-
Krawiecki, Z., Cysewska-Sobusiak, A., Wiczynski, G., & Odon, A. (2008). Modeling and
measurements of light transmission through human tissues. Bulletin ofthe PolishAcademy
ofSciences: TechnicalSciences, 56(2),147-154.
La Lumi re, LLC. (n.d.). Light Therapy Mask I Anti-Wrinkle & Acne Treatment I illuMask.
Retrieved December 2014, from illuMask: http://www.illumask.com/
Lamola, A. A., Bhutani, V. K., Wong, R. J., Stevenson, D. K., & McDonagh, A. F. (2013, July). The
effect of hematocrit on the efficacy of phototherapy. PediatricResearch, 74(1), 54-60.
Laufer, G. (1996). Introductionto Optics andLasersin Engineering. Cambridge: Cambridge
University Press.
Le Corbusier. (2007). TowardsA New Architecture. (J. Goodman, Trans.) Los Angeles: Getty
Research Institute.
Lister, T., Wright, P. A., & Chappell, P. H. (2012, September 17). Optical properties of human skin.
JournalofBiomedical Optics, 17(9), 090901-1 - 090901-15Lobdell,
J. (2008). Between Silence and Light: Spiritin theArchitectureofLo uisl
Kahn (2nd ed.).
Boston: Shambhala.
Management of Hyperbilirubinemia in the Newborn Infant 35 or More Weeks of Gestation.
(2004,
July). Pediatrics,114(1), 297-316.
Meduri, N. B., Vandergriff, T., Rasmussen, H., & Jacobe, H.
(2007).
Phototherapy in the
management of atopic dermatitis: a systematic review. Photodermatology,
Photoimmunology& Photomedicine, 23(4),
Miyawa,
J. H., & Schulman,
106-112.
S. G. (2001). Ultraviolet-Visible Spectrophotometry. In L. Ohannesian,
& A. Streeter (Eds.), HandbookofPharmaceuticalAnalysis(pp. 187-224). New York: Marcel
Dekker, Inc.
114
Nawashiro, H., Wada, K., Nakai, K., & Sato, S. (2012, April). Focal increase in cerebral blood flow
after treatment with near-infrared light to the forehead in a patient in a persistent vegetative
state. PhotomedicineandLaserSurgery,30(4), 231-233.
Olih, J., T6th-Molnir, E., Kemeny, L., & Csoma, Z. (2013, August). Long-termhazards of neonatal
blue-light phototherapy. BritishJournalofDermatology, 169(2),
243-249.
Ophinder, C., Deck, A., Volkman, C. M., Kirsch, M., Liebmann, J., Born, M.,.. . Suschek, C. V.
(2013, December). Mechanism and biological relevance of blue-light (420-453 nm)-induced
nonenzymatic nitric oxide generation from photolabile nitric oxide derivates in human skin
in vitro and in vivo. FreeRadicalBiology andMedicine, 65,
1363-1377.
Panhoca, V. H., Nunez, S. C., Pizzo, R. C., Grecco, C., Paolillo, F. R., & Bagnato, V. S.
(2015,
February). Comparative clinical study of light analgesic effect on temporomandibular
disorder (TMD) using red and infrared led therapy. LasersInMedicalScience, 30(2), 815-822.
Philippe Rahm Architects & fabric I ch. (2001, October 26). i-weather.org- artificialclimate based
on humanphysiology. Retrieved December
2014,
from i-weather: http://www.i-
weather.org/
Philips Lumileds Lighting Company. (2014, May 27). L UXEONRebel ColorLEDs[datasheet.
Retrieved from Philips Lumileds Lighting Company:
http://www.philipslumileds.com/uploads/265/DS68-pdf
Philips Lumileds Lighting Company.
(2014,
November 3). L UXEONRebel WhiteLEDs [datasheetj.
Retrieved from Philips Lumileds Lighting Company:
http://www.philipslumileds.com/uploads/2o/DS63-pdf
Poyton, R. 0., & Ball, K. A.
(2011,
February). Therapeutic photobiomodulation: nitric oxide and a
novel function of mitochondrial cytochrome c oxidase. DiscoveryMedicine, 1(57),154-159Radiance VWWVServer. (n.d.). Retrieved June 2014, from http://radsite.lbl.gov/radiance/
Rahman, S. A., Flynn-Evans, E. E., Aeschbach, D., Brainard, G. C., Czeisler, C. A., & Lockley, S. W.
(2014,
Februaryi). Diurnal spectral sensitivity of the acute alerting effects of light. Sleep,
37(2), 271-281.
Robert McNeel & Associates. (n.d.). Grasshopper- algorithmicmodelingforRhino. Retrieved June
2014,
from http://www.grasshopper3d.com/
115
Robert McNeel& Associates. (n.d.). Rhinoceros. Retrieved June 2014, from
https://www.rhino3d.com/
Roberts,
J. E.
Light and Immunomodulation. Neuroimmunomodulation, 917, 435-445.
(2000).
Ronan, P., & Gringer.
Februrary 19). EM Spectrum. Wikimedia Commons. Retrieved Mayi,
2014, from http://commons.wikimedia.org/wiki/File:EM-spectrumrevised.png
(2013,
Roudsari, M. S. (n.d.). Ladybug + Honeybee I Grasshopper.Retrieved June
2014,
from Food4Rhino
IApps for Rhino and Grasshopper: http://www.food4rhino.com/project/ladybughoneybee?ufh
Sasseville, A., Benhaberou-Brun, D., Fontaine, C., Charon, M. C., & H ebert, M. (2009,
July).
Wearing blue-blockers in the morning could improve sleep of workers on a permanent night
schedule: a pilot study. ChronobiologyInternational,26(5), 913-925-
Sliney, D. H., Wangemann, R. T., Franks,
J. K., & Wolbarsht, M. L.
(1976). Visual sensitivity of the
eye to infrared laser radiation. Journalofthe OpticalSociety ofAmerica, 66(4), 339-341.
Smith, W. J. (1966). Modern OpticalEngineering- The Design of OpticalSystems (ist ed.). NewYork:
McGraw-Hill.
Solemma, LLC. (n.d.). DIVA ForRhino. Retrieved June 2014, from http://diva4rhino.com/
Spector, A. (1982). Aging of the lens and cataract formation. In R. Sekuler, D. Kline, & K. Dismukes
(Eds.), Aging and human visualfunction(pP- 30-43). NewYork: Alan R. Liss, Inc.
Stroebel, L. D., & Zakia, R. K. (Eds.). (1993). The FocalEncyclopediaofPhotography(3rd ed.).
Boston: FocalPress.
Synopsys Optical Solutions Group. (n.d.). LightTools -Synopsys OpticalSolutions. Retrieved June
2014, from Synopsys.com: http://optics.synopsys.com/lighttools/
Titus, S., & Hodge,
J. (2012, October 15).
Diagnosis and treatment of acne. American Family
Physician, 86(8), 734-740Vandewalle, G., Schwartz, S., Wuillaume, C., Balteau, E., Degueldre, C., Schabus, M., . . . Maque t,
P.
(2010,
November 9). Spectral quality of light modulates emotional brain responses in
humans. Proceedingsofthe NationalAcademy ofSciences ofthe UnitedStates ofAmerica,
107(45),19549-19554.
116
Walker, D. P., Vollmer-Snarr, H. R., & Eberting, C. L.
(2012,
January). Ocular hazards of blue-light
therapy in dermatology. JournaloftheAmerican Academy ofDermatology, 66(1), 130-135Weissleder, R.
(2001,
April). A clearer vision for in vivo imaging. NatureBiotechnology, 19(4), 316-
317.
Weisstein, E. W. (n.d.). GaussianFunction.Retrieved August2014, from MathWorld -- A Wolfram
Web Resource: http://mathworld.wolfram.com/GaussianFunction.html
.
Whelan, H. T., Smits, R. L., Buchman, E. V., Whelan, N. T., Turner, S. G., Margolis, D. A., . .
Caviness,
J. (2001, December). Effect of NASAlight-emitting diode irradiation on wound
healing. Journalof ClinicalLaserMedicine& Surgery, 19(6), 305-314.
Wyszecki, G., & Stiles, W. S. (1982). ColorScience: Concepts and Methods, QuantitativeDataand
Formulae(2nd ed.). New York: Wiley - Series in Pure and Applied Optics.
Yelverton, C. B., Balkrishnan, R., & Feldman, S. R. (2006, October). The utility of a data-logging
device for measuring adherence to home phototherapy. Photodermatology,
Photoimmunology & Photomedicine,22(5), 270-272.
Zemax, LLC. (n.d.). Zemax - OpticStudio I Zemax. Retrieved June 2014, from Zemax - Optical and
Illumination Design Software I Zemax: https://www.zemax.com/products/opticstudio
117