Application for Enrollment USA Health & Dental Plan
advertisement

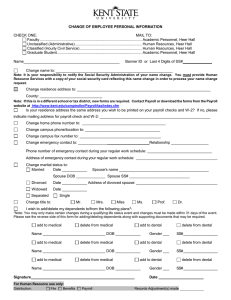
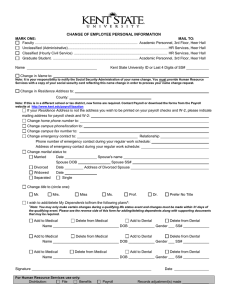
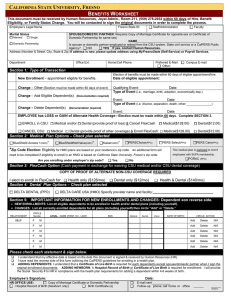
Application for Enrollment USA Health & Dental Plan PLEASE PRINT CLEARLY AND BE SURE TO SIGN AND DATE THIS FORM EMPLOYEE INFORMATION - PLEASE PRINT CLEARLY EMPLOYEE NAME (LAST): (FIRST): STREET ADDRESS: CHECK ONE: MALE FEMALE (INITIAL): CITY: CHECK ONE: SINGLE MARRIED DIVORCED WIDOWED STATE: CHECK ONE: Dr. Mr. TYPE OF COVERAGE SELECTED: ZIP: EMPLOYEE DATE OF BIRTH: GROUP NUMBER: PHONE NUMBER: EMPLOYEE SOCIAL SECURITY NUMBER: Mrs. Ms./Miss EMPLOYEE (J) NUMBER: J INDIVIDUAL FAMILY NATURE OF APPLICATION – CHECK THE APPROPRIATE BOX FOR THE ACTION DESIRED: NEW CONTRACT APPLICATION CHANGE CONTRACT CANCEL CONTRACT ADD/REMOVE DEPENDENT NAME CHANGE ADD SPOUSE ADDRESS CHANGE ADD DEPENDENT CHILD TYPE OF COVERAGE CHANGE REMOVE SPOUSE CHANGE COB INFORMATION REMOVE DEPENDENT CHILD DATE EVENT OCCURRED (Example: Date of marriage, birth date of child, date of death, etc.): LIST ALL DEPENDENTS ELIGIBLE UNDER THIS CONTRACT AND PROVIDE SOCIAL SECURITY NUMBER AND/OR MEDICARE NUMBER (HICN) The Social Security Number for the employee and ALL dependents must be provided in order for this application to be processed. SOCIAL SECURITY NUMBER DATE OF BIRTH LAST NAME FIRST NAME INITIAL RELATIONSHIP AND/OR HIC NUMBER MONTH DAY YEAR SPOUSE Male Female SON DAUGHTER SON DAUGHTER SON DAUGHTER SON DAUGHTER COORDINATION OF BENEFITS – MANDATORY INFORMATION If you, your spouse, or dependents are covered by any other group health insurance, you are required to provide the following information: NAME OF CONTRACT HOLDER: POLICY, ID, CONTRACT OR CERTIFICATE TYPE OF COVERAGE: NAME OF INSURANCE COMPANY NUMBER: INDIVIDUAL FAMILY EMPLOYER’S NAME: EMPLOYER’S STREET ADDRESS, CITY, STATE, & ZIP: GROUP NUMBER: COVERAGE EFFECTIVE DATE: NAME OF MEMBER ENTITLED TO MEDICARE BENEFITS: MEDICARE NUMBER (HICN): PART A PART B Page 1 of 2 EMPLOYEE CERTIFICATION – CHECK ONE I waive my rights to health and dental benefits and do not wish to enroll. I am requesting cancellation of my existing benefits as indicated. I am applying for coverage under the USA Health & Dental Plan (Plan). I understand that my application is subject to the terms and conditions of the Plan and that coverage is subject to the eligibility rules and plan of benefits as stated in the USA Health and Dental Plan Member Handbook. I understand that any misrepresentation is fraud and will be pursued to the fullest extent allowed by law. I understand that coverage under the Plan will not become effective until my application is accepted by evidence of issuing an identification card or other written notice. I agree to notify the USA Human Resources Department if an eligible dependent has a change-in-status, especially if a dependent is no longer a dependent due to divorce. I authorize my doctor, hospital or anyone else to give all medical records for anyone covered under my coverage to the claims administrator for the operation of the Plan including determination of eligibility and benefits. I agree to cooperate with the claims administrator and provide information required to administer the Plan, pay claims, coordinate benefits with other coverage, subrogate against another responsible party or recover benefits paid in error. I agree that benefits may be paid directly to providers of service and such payment will release the Plan of its benefit obligation. TOBACCO USE CERTIFICATION The USA Health & Dental Plan is committed to helping you achieve your best health. The Wellness Incentive is available to all employees. If you think you might be unable to meet the standard under this Wellness Program, you may qualify for an opportunity to earn the same reward by different means. Contact the USA Human Resources Department for additional information. HAVE YOU OR YOUR SPOUSE USED TOBACCO PRODUCTS WITHIN THE LAST SIX (6) MONTHS? : Yes No Further, I attest that everything in the application is true. Signature of Employee Date Signed Beginning in 2014, the Affordable Care Act (ACA) prohibits pre-existing condition waiting periods. In compliance with the Affordable Care Act (ACA), effective January 1, 2014, the USA Health & Dental Plan no longer utilizes a pre-existing condition waiting period. Departing employees or dependents no longer eligible will be provided a Certificate of Creditable Coverage from this Plan that can be submitted to possibly offset the waiting period for coverage of pre-existing conditions under a new health plan which may not be subject to the ACA mandates. Departing employees and dependents no longer eligible for coverage will be entitled to COBRA coverage, and may be eligible to purchase coverage through the Health Insurance Marketplace. STOP – TO BE COMPLETED BY A UNIVERSITY OF SOUTH ALABAMA HUMAN RESOURCES DEPARTMENT REPRESENTATIVE All the information appears to be complete and correct. Signature of HR Representative Date Signed University of South Alabama Human Resources Department 650 Clinic Drive Technology & Research Park, Building 3 – Suite 2200 Mobile, AL 36688 Phone: (251) 460-6133 Page 2 of 2