advertisement
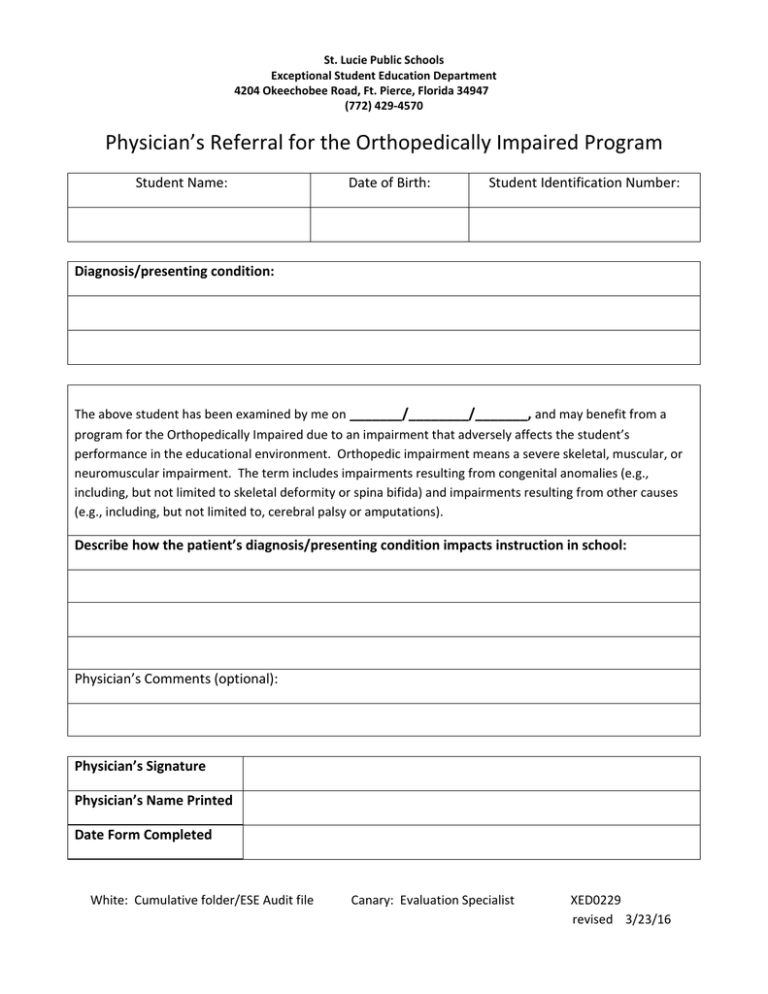
St. Lucie Public Schools Exceptional Student Education Department 4204 Okeechobee Road, Ft. Pierce, Florida 34947 (772) 429‐4570 Physician’s Referral for the Orthopedically Impaired Program Student Name: Date of Birth: Student Identification Number: Diagnosis/presenting condition: The above student has been examined by me on _______/________/_______, and may benefit from a program for the Orthopedically Impaired due to an impairment that adversely affects the student’s performance in the educational environment. Orthopedic impairment means a severe skeletal, muscular, or neuromuscular impairment. The term includes impairments resulting from congenital anomalies (e.g., including, but not limited to skeletal deformity or spina bifida) and impairments resulting from other causes (e.g., including, but not limited to, cerebral palsy or amputations). Describe how the patient’s diagnosis/presenting condition impacts instruction in school: Physician’s Comments (optional): Physician’s Signature Physician’s Name Printed Date Form Completed White: Cumulative folder/ESE Audit file Canary: Evaluation Specialist XED0229 revised 3/23/16