SIMVASTATIN REDUCES S. AUREUS-STIMULATED EXPRESSION OF C5AR ON MACROPHAGES A RESEARCH PAPER
advertisement

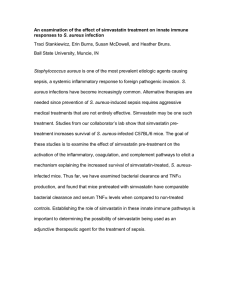
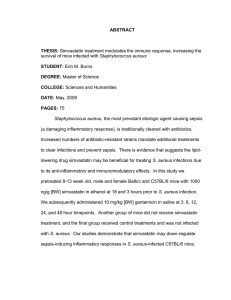
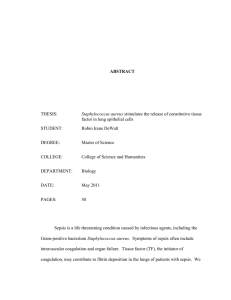
SIMVASTATIN REDUCES S. AUREUS-STIMULATED EXPRESSION OF C5AR ON MACROPHAGES A RESEARCH PAPER SUBMITTED TO THE GRADUATE SCHOOL IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE MASTER OF ARTS IN BIOLOGY BY MICHAEL V. KUSHDILIAN DR. HEATHER A. BRUNS - ADVISOR BALL STATE UNIVERSITY MUNCIE, INDIANA MAY 2012 INTRODUCTION Sepsis is a progressive hyper-inflammatory immune response that can lead to shock, multi-organ failure, or death. Each year in the United States there are approximately 700,000 cases of sepsis, resulting in about 210,000 deaths annually (1, 2). In intensive care units, patient mortality rates from sepsis can be as high as 50% (3). Sepsis is broadly classified as an inappropriate immune response to an invasive pathogen. Normally this response is contained within the affected area to prevent further spread of pathogens without harm to the host. However, without proper regulatory mechanisms, the result is systemic inflammation that escalates to a pathological state known as sepsis (4). An important innate immune response that contributes to a septic pathology is the complement system. The complement cleavage product C5a has an especially potent role in sepsis progression and prognosis. Serum C5a concentration is a strong indicator of sepsis severity due to its marked ability to initiate systemic inflammation and enhance sepsis (5). C5a exerts its effects upon binding to its receptor (C5aR), a G-protein coupled receptor with seven transmembrane domains (6). Importantly, C5aR surface expression is upregulated during sepsis and blockade of C5aR confers protection from sepsis lethality (7). Staphylococcus aureus, a gram-positive opportunistic bacterium, is the most common etiologic agent of sepsis in US hospitals and second leading cause of bacterial infections in outpatients (8, 9). This pervasive opportunistic pathogen can cause a variety of diseases from minor skin infections to 2 pneumonia and meningitis. The alarming frequency of S. aureus infections can be attributed to a vast array of virulence factors, including its ability to evade the immune system and develop resistance to antibiotics (9). The alarming frequency of S. aureus-induced sepsis and decreased effectiveness of current treatments highlight the need for alternative or adjunctive therapeutic strategies. In recent years, statins (HMG-CoA reductase inhibitors) have exhibited beneficial immunomodulatory effects, independent of their lipid-lowering ability (10). Murine models of sepsis have shown cerivastatin to be protective from sepsis-related death when administered 24 hours before bacterial infection (11) and up to 72 hours post (12). Additionally, mice pretreated with simvastatin exhibit nearly 4 times the mean survival time from sepsis compared to untreated control animals with preservation of cardiovascular function (13). In humans the clinical effectiveness of statin therapy is emphasized by reduced mortality rates and hospitalizations in septic patients undergoing a statin regimen (14). These studies demonstrate compelling support for statin use as an effective adjuvant treatment for sepsis. Of particular importance in bacterial sepsis progression is activation of macrophages in body tissues. Once activated, these cells increase surface marker expression, enhance phagocytic abilities, and mediate inflammatory responses to contain and eliminate the pathogen (4). However, during sepsis, macrophages respond to C5a by releasing powerful inflammatory cytokines, such as TNF-α, that can facilitate sepsis progression (15). Therefore, the 3 macrophage C5a-C5aR interaction is a “double-edged sword” that is beneficial when appropriate, but harmful during sepsis. Macrophages treated with statins show reduced surface expression of activation markers MHC Class II and CD40 via intracellular sequestration (16, 17). These findings suggest simvastatin may reduce the harmful effects of sepsis by altering levels of specific surface proteins. Because macrophages are integral components of the innate immune system but also initiate adaptive immune responses, they are a logical cell choice for further investigation of the precise immunocellular responses to simvastatin. Previous work in our lab demonstrated that simvastatin pretreatment increases survival of mice infected with S. aureus (Figure 1). Additionally, serum levels of C5a between infected simvastatin and control mice that were both infected by S. aureus were nearly identical (Figure 2). These initial findings suggest that simvastatin alters the cellular response to C5a but not the concentration of C5a itself. Therefore, I infected simvastatin-treated macrophages with S. aureus to study alterations in C5aR expression to further investigate the immunomodulatory mechanisms of simvastatin. I hypothesized that simvastatin treatment dampens macrophage activation to invading pathogens by altering surface protein expression, thus decreasing harmful inflammatory reactions and potentially increasing survival to S.aureus-induced sepsis. 4 Figure 1. Simvastatin pretreatment increases survival of mice infected with S. aureus. Male and female mice were pretreated with simvastatin (+Simva) or vehicle control (-Simva) 18 and 3 hours prior to infection with S. aureus, treated with gentamicin 3, 6, 12, 24, and 48 hours post-infection and observed for 14 days. The graph represents individual data points combined from 3 replicate studies (n=13-14/group). * p < 0.05 by Kaplan-Meier Log Rank analysis. 5 Figure 2. Serum levels of C5a induced by S. aureus infection are comparable between simvastatin and control-treated mice. Mice were pretreated with simvastatin (+Simva) or vehicle control (-Simva) 18 and 3 hours prior to infection with S. aureus. Serum was isolated at 24 hours post-infection and analyzed by ELISA. Data were pooled from 2 replicate studies (n=8/group) and analyzed using Student’s t-test. MATERIALS AND METHODS Cell culture RAW 264.7 macrophages (American Type Culture Collection, Manassas, VA) were grown in filter-sterilized DMEM (Lonza, Allendale, NJ ) antibiotic-free media supplemented with 1% v/v L-glutamine (BioWhittaker) and 10% v/v FBS (Atlanta Biologicals, Lawrenceville, GA) or RPMI-1640 (BioWhittaker) supplemented with 1% v/v L-glutamine (BioWhittaker) and 10% v/v FBS (Atlanta Biologicals) at 37°C in 5% CO2. S. aureus preparation. 6 Methicillin-sensitive Staphylococcus aureus (MSSA) (#29213, ATCC) were cultured in tryptic soy broth (TSB) (Sigma-Aldrich, St. Louis, MO) at 37°C shaking at 200 rpm. Bacteria were washed and diluted to 3x108 bacteria/mL. This bacterial strain was selected based upon extensive characterization of the inhibition of invasiveness by simvastatin (18). S. aureus infection of RAW macrophages RAW cells were plated onto 35mm plates at 2.5 X 105 cells/ml in supplemented RPMI (BioWhittaker). Cells were pre-treated with 1 µM simvastatin (Calbiochem [EMD Chemicals]) or DMSO (Thermo Fisher Scientific) for 18-24 hours prior to infection. Each plate received either 1 X 108 bacteria (MOI 400) or an equal volume of 0.85% saline and incubated at 37°C and 5% CO2. After one hour, media from each plate was replaced with media containing 50 µg/ml Gentamicin (Sigma-Aldrich) and 20 µg/ml Lysostaphin (Sigma-Aldrich) and incubated for 12-24 hours before analysis of cell surface marker expression by flow cytometry (described below). Flow cytometry. RAW macrophages (2.5x105 cells per sample) were infected with S. aureus as described above, were washed and stained in FACS buffer (PBS containing 2% BSA and 0.1% NaN3). Cells were first incubated with diluted normal rat serum (Jackson ImmunoResearch, West Grove, PA) for 5 minutes at 7 4 °C then washed once in FACS buffer. Samples were stained with antibodies (MHC Class II, CD80, CD86, CD40, and C5aR) conjugated to FITC, PE, CyChrome, or allophycocyanin (eBioscience, San Diego, CA). Staining was performed at 4°C for 15 minutes. Cells were washed and then fixed in FACS buffer containing 0.5% formaldehyde. Samples were analyzed using an Accuri C6 flow cytometer. Mean fluorescence intensity (MFI) was recorded and normalized to the background fluorescence intensity of the negative control. RESULTS The purpose of this study was to demonstrate a novel mechanism by which simvastatin alters the inflammatory response to C5a by down-regulating its receptor, C5aR, during S. aureus-induced sepsis. Simvastatin reduces the basal and S. aureus-induced surface expression of C5aR on macrophages. To determine whether simvastatin alters C5aR expression during sepsis, macrophages were used to setup an infection model in vitro. Macrophage cells were chosen because of their unique ability to enhance the inflammatory response and further sepsis progression (5). Half of the macrophages were pretreated with simvastatin or a control solution of dimethyl sulfoxide (DMSO) to assess changes in basal expression of C5aR. Two additional groups of 8 macrophages were also pretreated with either simvastatin or DMSO and then infected by S. aureus as a model for sepsis progression. After antibiotic treatment, C5aR expression was determined by flow cytometry analysis. The results showed lower levels of C5aR expressed on simvastatin treated macrophages compared to the DMSO control group. Since neither of these groups was infected with bacteria, these results show that simvastatin reduces basal expression of C5aR. Additionally, the S. aureusinfected control macrophages displayed higher levels of C5aR compared to noninfected controls, which indicates that infection alone was sufficient to increase expression of C5aR. Simvastatin pretreated macrophages that were infected by S. aureus demonstrated significantly reduced expression of C5aR compared to infected controls. These results collectively suggest that simvastatin reduces both basal and infection-induced levels of C5aR (Figure 3). 9 Figure 3. C5aR expression on macrophages is decreased due to simvastatin treatment. RAW macrophages were treated with 1 µM simvastatin (SIMVA) or dimethyl sulfoxide (DMSO) 18-20 hours prior to infection with S. aureus for 1 hour (SA+DMSO and SA+ SIMVA). The infection was stopped and cells were analyzed 18 hours post-infection for expression of C5aR by comparison of Mean Fluorescence Intensity (MFI). Normalized MFI was pooled from all experiments and analyzed by one-way ANOVA followed by Student Neuman-Keuls post-hoc analysis. *p < 0.05 compared to DMSO. **p < 0.05 compared to SA+DMSO. Simvastatin does not alter the basal or S. aureus-induced expression of activation markers To investigate the changes in gene expression induced by simvastatin, the expression of activation makers CD40, CD80, CD86, and MHC Class II surface proteins were also analyzed. No significant changes in activation marker expression on simvastatin or control-treated macrophages were observed by flow cytometry analysis (Figure 4). Pretreatment with simvastatin did not reduce the 10 basal expression of activation markers on macrophages nor did it reduce the S. aureus-stimulated expression of these surface proteins. In summary, these data demonstrate that simvastatin does not alter expression of surface proteins that are indicative of macrophage activation. 11 Figure 4. Simvastatin does not alter the basal or S. aureus-induced expression of surface proteins CD40, CD80, CD86, and MHC Class II on macrophages. RAW macrophages were treated with 1 µM simvastatin (SIMVA) or dimethyl sulfoxide (DMSO) 18-20 hours prior to infection with S. aureus for 1 hour (SA+DMSO and SA+ SIMVA). The infection was stopped and cells were analyzed 18 hours post-infection for expression of MHC Class II, CD40, CD80, and CD86. Normalized MFI was pooled from all experiments and analyzed by one-way ANOVA followed by Student Neuman-Keuls post-hoc analysis. 12 DISCUSSION Excessive activation of the innate immune system, specifically the complement cascade, has been correlated with poor prognosis in numerous inflammatory diseases including sepsis (19), respiratory disorders (20), and arthritis (21). One of the most potent activators of the complement cascade, C5a, is produced in excess by the immune system during sepsis caused by the uncontrolled spread of a pathogen. However, preliminary data showed no difference in C5a levels following simvastatin treatment despite improved survival outcomes from bacterial sepsis (Figures 1 & 2). Therefore, the aim of this study was to elucidate the immunocellular mechanism by which simvastatin exerts its beneficial effect without altering serum C5a levels during sepsis. Statins have demonstrated beneficial effects in humans by altering complement activation. For example, patients taking simvastatin or atorvastatin exhibited reduced serum levels of complement proteins C3 and C3c (22-24). Given that excessive C5a leads to sepsis, the fact that simvastatin-treated and control mice displayed no difference in serum C5a concentrations (Figure 2) but did show improved survivability from sepsis (Figure 1) suggests that simvastatin may reduce cellular responses to C5a by down-regulating expression of its receptor on immune cells. This is plausible given that simvastatin treatment has been reported to alter actin dynamics at the cell surface, suggesting simvastatin may also alter surface receptor recycling via endocytosis (25). The data shown in Figure 3 support this mechanism of action, since basal and S. aureus-induced 13 expression of C5aR was reduced on macrophages pretreated with simvastatin. This down-regulation of C5aR surface expression may serve to dampen the harmful over-activation of macrophages by preventing C5a from interacting with its receptor during sepsis. Additional surface proteins were assessed for changes in expression levels to study the effects of simvastatin on macrophage activation. When exposed to pathogen, macrophages are activated and expression of CD40, CD80, CD86, and MHC Class II proteins at the cell surface is increased (26). These proteins facilitate macrophage functions including presentation of antigen and activation of T cells involved in the adaptive immune response. However, simvastatin pretreatment did not significantly alter basal or S. aureus-induced expression of these activation markers as shown in Figure 4. This suggests that simvastatin does not interfere with activation of macrophages during sepsis nor does it impede their ability to activate other immune cells, which function collectively to eliminate and contain invasive pathogens. This investigation highlighted a novel mechanism by which simvastatin attenuates hyper-inflammatory responses by down-regulating C5aR levels that lead to sepsis pathology without affecting other macrophage surface proteins. This specific and selective ability of simvastatin to down-regulate expression of complement receptors allows for precise modulation of complement activity during immune challenge by S. aureus. This mechanism may also explain the beneficial effects of simvastatin during bacterial sepsis and provide explanation for numerous reports of improved survival in animal models of sepsis while 14 undergoing a statin regimen (11, 27, 28). Furthermore, these findings may also elucidate the underlying mechanism behind the beneficial effect of statin use in humans. Many observational studies have associated statin use with fewer hospitalizations and decreased mortality from septic patients (14, 29). Therefore, these data provide compelling support for statin use as a potential adjuvant treatment for sepsis via alteration of immunocellular processes. ACKNOWLEDGEMENTS I would like to thank Dr. Heather Bruns for giving me the opportunity to complete this project in her lab, showing me the ropes, and mentoring me along the way. Additionally I would like to thank Dr. Susan McDowell for her patience in guiding me through the research process. This research was funded by a grant through the Indiana Academy of Science. 15 REFERENCES 1. D. Angus et al., Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Critical Care Medicine 29, 1303 (2001). 2. G. S. Martin, D. M. Mannino, S. Eaton, M. Moss, The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med 348, 1546 (Apr 17, 2003). 3. C. Alberti et al., Epidemiology of sepsis and infection in ICU patients from an international multicentre cohort study. Intensive Care Medicine 28, 108 (2002). 4. D. J. Stearns‐Kurosawa, M. F. Osuchowski, C. Valentine, S. Kurosawa, D. G. Remick, The pathogenesis of sepsis. Annu Rev Pathol 6, 19 (2011). 5. P. A. Ward, The harmful role of C5a on innate immunity in sepsis. J Innate Immun 2, 439 (2010). 6. N. P. Gerard, C. Gerard, The chemotactic receptor for human C5a anaphylatoxin. Nature 349, 614 (1991). 7. N. C. Riedemann, Increased C5a receptor expression in sepsis. Journal of Clinical Investigation 110, 101 (2002). 8. D. Diekema et al., Survey of infections due to Staphylococcus species: frequency of occurrence and antimicrobial susceptibility of isolates collected in the United States, Canada, Latin America, Europe, and the Western Pacific region for the SENTRY Antimicrobial Surveillance Program, 1997‐1999. Clinical Infectious Diseases 32, S114 (2001). 16 9. D. Styers, D. J. Sheehan, P. Hogan, D. F. Sahm, Laboratory‐based surveillance of current antimicrobial resistance patterns and trends among Staphylococcus aureus: 2005 status in the United States. Ann Clin Microbiol Antimicrob 5, 2 (2006). 10. B. Kwak, F. Mulhaupt, S. Myit, F. Mach, Statins as a newly recognized type of immunomodulator. Nature Medicine 6, 1399 (2000). 11. H. Ando, T. Takamura, T. Ota, Y. Nagai, K. Kobayashi, Cerivastatin improves survival of mice with lipopolysaccharide‐induced sepsis. The Journal of Pharmacology and Experimental Therapeutics 294, 1043 (2000). 12. M. Z. Chaudhry, J. H. Wang, S. Blankson, H. P. Redmond, Statin (cerivastatin) protects mice against sepsis‐related death via reduced proinflammatory cytokines and enhanced bacterial clearance. Surgical Infections 9, 183 (2008). 13. M. W. Merx et al., HMG‐CoA Reductase Inhibitor Simvastatin Profoundly Improves Survival in a Murine Model of Sepsis. Circulation 109, 2560 (June 1, 2004, 2004). 14. H. Schmidt et al., Association of statin therapy and increased survival in patients with multiple organ dysfunction syndrome. Intensive Care Medicine 32, 1248 (2006). 15. N. C. Riedemann et al., Regulation by C5a of neutrophil activation during sepsis. Immunity 19, 193 (2003). 17 16. H. F. Kuipers et al., Statins affect cell‐surface expression of major histocompatibility complex class II molecules by disrupting cholesterol‐ containing microdomains. Hum Immunol 66, 653 (2005). 17. K. P. Townsend et al., Lovastatin modulation of microglial activation via suppression of functional CD40 expression. J Neurosci Res 78, 167 (2004). 18. M. Horn et al., Simvastatin inhibits Staphylococcus aureus host cell invasion through modulation of isoprenoid intermediates. Journal of Pharmacology and Experimental Therapeutics 326, 135 (2008). 19. P. A. Ward, The dark side of C5a in sepsis. Nat Rev Immunol 4, 133 (2004). 20. R. A. Robbins, W. D. Russ, J. K. Rasmussen, M. M. Clayton, Activation of the complement system in the adult respiratory distress syndrome. The American review of respiratory disease 135, 651 (1987). 21. S. M. Linton, B. P. Morgan, Complement activation and inhibition in experimental models of arthritis. Molecular Immunology 36, 905 (1999). 22. C. J. Halkes et al., Postprandial increase of complement component 3 in normolipidemic patients with coronary artery disease: effects of expanded‐dose simvastatin. Arterioscler Thromb Vasc Biol 21, 1526 (Sep, 2001). 23. A. Muscari et al., Short term effect of atorvastatin and vitamin E on serum levels of C3, a sensitive marker of the risk of myocardial infarction in men. Cardiovasc Drugs Ther 15, 453 (Sep, 2001). 18 24. C. Verseyden, S. Meijssen, H. van Dijk, H. Jansen, M. Castro Cabezas, Effects of atorvastatin on fasting and postprandial complement component 3 response in familial combined hyperlipidemia. J Lipid Res 44, 2100 (Nov, 2003). 25. T. E. Stankiewicz et al., GTPase activating protein function of p85 facilitates uptake and recycling of the β1 integrin. Biochemical and Biophysical Research Communications 391, 443 (2010). 26. D. M. Mosser, The many faces of macrophage activation. Journal of Leukocyte Biology 73, 209 (February 1, 2003, 2003). 27. U. Buerke et al., Apoptosis Contributes to Septic Cardiomyopathy and Is Improved By Simvastatin Therapy. Shock 29, 497 (2008). 28. M. W. Merx et al., Statin Treatment After Onset of Sepsis in a Murine Model Improves Survival. Circulation 112, 117 (July 5, 2005, 2005). 29. R. Gupta et al., Statin Use and Hospitalization for Sepsis in Patients With Chronic Kidney Disease. JAMA: The Journal of the American Medical Association 297, 1455 (April 4, 2007, 2007). 19