Original article ABSTRACT Background
advertisement

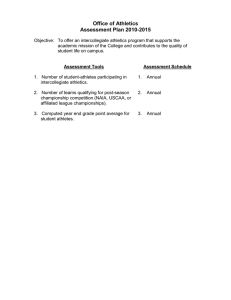
Downloaded from bjsm.bmj.com on September 6, 2014 - Published by group.bmj.com Original article Design of a protocol for large-scale epidemiological studies in individual sports: the Swedish Athletics injury study Jenny Jacobsson,1 Toomas Timpka,1 Joakim Ekberg,1 Jan Kowalski,1 Sverker Nilsson,1 Per Renström2 1Section of Social Medicine and Public Health, Department of Medical and Health Sciences, Linköping University, Linköping, Sweden 2Section of Sports Orthopedic Surgery, Department of Surgical Sciences, Karolinska Institute, Stockholm, Sweden Correspondence to Jenny Jacobsson, PT MSc, Section of Social Medicine and Public Health, Department of Medical and Health Sciences, Linköping University, Linköping SE-581 83, Sweden; jenny.jacobsson@liu.se Accepted 18 February 2010 Published Online First 19 May 2010 1106 ABSTRACT Background Epidemiological studies have mainly been performed on team sports. The authors set out to develop a protocol for large-scale epidemiological studies of injuries among elite athletics athletes. Methods An argument-based method for investigation of complex design problems was used to structure the collection and analysis of data. Specification of the protocol was preceded by an examination of requirements on injury surveillance in individual sports and iterated drafting of protocol specifications, and followed by formative evaluations. Results The requirements analysis shows that the central demand on the protocol is to allow for detailed epidemiological analyses of overuse injuries, which subsequently requires regular collection of self-reported data from athletes. The resulting study protocol is centred on a web-based weekly athlete e-diary enabling continual collection of individual-level data on exposure and injuries. To be able to interpret the self-reported data on injury events, collection of a wide range of personal baseline data from the athlete, including a psychological profile, is included in the protocol. Conclusions The resulting protocol can be employed in intervention programmes that can prevent suffering among both adult elite and youth talent athletes who have made considerable life investments in their sport. However, the contexts for injury surveillance in team sports and in individual sports such as athletics differ in several important aspects (table 1). For example, there are important differences between team and individual sports regarding everyday access to physicians and physiotherapists. In team sports, such as cricket and soccer, the majority of the elite clubs have medical staff employed.15 It is therefore necessary to reflect on the main characteristics of team and individual sports to distinguish the components of injury surveillance in team sports that are useful for the study of an individual sport. The aim of this study is to develop a protocol for large-scale epidemiological studies of injuries among elite athletics athletes. The protocol is to be used in planning of intervention programmes among adult and youth athletes. METHODS An argument-based method for investigation of complex design problems16 17 was used to structure the collection and analysis of the data. Examination of requirements on injury surveillance in athletics was followed by iterated drafting of protocol specifications and formative evaluations. The protocol is exemplified by implementation in a national-level study in Sweden. INTRODUCTION Data collection A frequent sighting in the media coverage of the 2008 Beijing Olympics was an injured athlete. The agony of these injured sportspersons became matters of national concern in many countries, such as Sweden and China. A secondary effect was a public questioning of the training methods and the quality of injury prevention in the particular sport. In hindsight, the events and the debate raise questions about whether the practice schedules and loads are safe and not directly or indirectly hazardous for the athletes. Epidemiological studies of injury prevalence, incidence and patterns in athletics are scarce,1–6 and the studies available lack the uniformity in methods and data defi nitions that would allow observed injury patterns to be generalised among populations. In comparison, systematic injury surveillance has been implemented at the elite level in several team sports.7–10 In many team sports, injury consensus groups have also formulated guidelines on how studies of injury epidemiology should be performed to allow between-study comparisons.11–14 A nominal group method18 was used for the requirements analysis. Two expert panels examined requirements on the data to be collected by the study protocol and the study implementation process, respectively (figure 1A). Individual expert’s reviews of working documents were followed by telephone conferences. Requirements on the data to be collected were defi ned by a panel consisting of scientists and practitioners (n=8) with backgrounds in athletics coaching, sports medicine, epidemiology, biostatistics and medical psychology. To answer specific questions, international experts were consulted during a working seminar at the 2nd World Congress on Sports Injury Prevention in Tromsö, Norway 2008, and by personal communications. The panel examining requirements on implementation of the study in practice consisted of scientists (n=5) with backgrounds in sports medicine, statistics, health informatics and cognitive science. All experts provided a fi rst round of comments to the study coordinator, who assembled these into a case-study Br J Sports Med 2010;44:1106–1111. doi:10.1136/bjsm.2009.067678 Downloaded from bjsm.bmj.com on September 6, 2014 - Published by group.bmj.com Original article assessment document. When subsequent turns did not return with significant changes in the document, the requirements were considered fi nalised. Data analysis Data from the two-step requirements analysis processes were transferred to a study protocol specification procedure. Members of the two panels were merged into one design specification group (figure 1B). The task communicated to the group was to formulate a preliminary study protocol using the requirements, their personal expertise and the published literature. The experts fi rst provided their individual comments, which were collected by a design process coordinator. Formulation of study protocol suggestions was performed independently by experts. Comments on each version of the working study design document were circulated to the entire expert group, and a consensus document was established. In the third and fi nal step, the document was approved as the preliminary study design protocol. Formative evaluations A cognitive walkthrough19 review of the injury surveillance part of the preliminary protocol was performed. Six athletes and coaches individually reviewed the weekly surveillance section of the protocol. The instructions were to ‘walk through’ six weekly report scenarios, where the respondent: (1) had been injured but had recovered; (2) had been fit and Table 1 Conditions for elite athletes in selected team sports and athletics with relevance for the design of large-scale epidemiological studies Soccer8 11 Conditions for elite athletes Practice in teams Individual training Set league schedule Individual competition schedule Coaches employed by club Medical staff employed by club Full professionals √ – √ – √ √ √ Cricket14 Rugby12 √ – √ – √ √ √ Athletics* √ – √ – √ √ √ – √ – √ (√) – (√) *Conditions for Swedish elite athletes. (√ ), hardly any. was still fit; (3) had been injured and was still injured; (4) had been fit but was now injured; (5) had been injured but was now recovering with adjusted practice load; and (6) had entered the study with a previous injury. The reviewers were instructed to report if they noted any ambiguities or vague formulations, lack of suitable alternatives, or risk of misinterpretation and what the consequences of these observations would be. The reviewers’ reports were analysed and the preliminary protocol revised into a prototype protocol. The fi nal evaluation of the prototype injury surveillance protocol was performed in a pilot study, which was carried out among adult and youth athletes (n=22). The survey data were used to revise the protocol into its fi nal version. RESULTS Requirements on a study protocol in athletics The primary requirement on the protocol was a correct defi nition of athletics injury at the borderline between functional over-reaching leading to improved accomplishments and overtraining leading to overuse injuries. 20 21 Athletics athletes have been shown to sustain a large proportion of overuse injuries,1 2 4 5 22–24 which implies that this injury category in particular has to be exactly defi ned and covered in epidemiological studies. Second, to reflect the complexity of the sport, epidemiological data have to be collected directly from the individual athletics athletes. For instance, the training schedules can diverge substantially among individuals within a subdiscipline. 25 It is therefore important to both extract individual data on exposure to practice and competition, and to include psychological and behavioural variables in the analyses. Coping strategies and different behavioural traits have been found to be associated with sports injury rates. 26 Definition of athletics injury: protocol choice and arguments The injury defi nition used for the protocol follows, with some alterations, the defi nitions previously used in athletics.4 24 A reportable athletics injury is any new musculoskeletal pain, feeling or injury that results from athletic training or competition and further leads to one or both of the following alternatives: (A) causes alterations in normal training and competition in mode, duration, intensity or frequency from the current A. Requirements analysis Coordinator Expert panel Study protocol requirements Data to be collected Expert panel Study procedures Study protocol design Pilot tests B. Study protocol design and testing Coordinator Expert panel Figure 1 Display of associations between the (A) analysis of requirements and (B) study protocol specification. Br J Sports Med 2010;44:1106–1111. doi:10.1136/bjsm.2009.067678 1107 Downloaded from bjsm.bmj.com on September 6, 2014 - Published by group.bmj.com Original article or subsequent training and competition sessions (partial time loss injury) (B) requires total removal from current or subsequent training and competition sessions (time loss injury). The argument for using this defi nition is threefold. First, the athletes will be handling surveillance reports themselves, and the injury recording will be performed from the athlete’s subjective perspective, their experience of pain and/or feeling. Second, practice in athletics consists of several different components—for example, training with barbell and discipline-specific technique training. When athletes are unable to follow the original schedule due to injury or feeling, they routinely modify their practice schedule by exchanging elements. The concept of partial time-loss injury supports the search for identifying complex background patterns for overuse injuries. Third, to allow for comparisons with previous studies in athletics and other sports, injuries will primarily be identified by time loss, and at a secondary level the analysis will be complemented by investigations of tissue damage and the functional level of the athlete. Means for athlete-level data collection: protocol choice and arguments A majority of the adult athletics athletes, regardless of level of performance, perform their training sessions using a set programme and without immediate supervision. For this reason, we ruled out using coaches to assist with data collection. An alternative considered was to involve local physicians and physiotherapists, but this was not feasible due to the irregularity in individual practice schedules and was difficult in practice, since athletes live at various geographic locations. We chose a combination of web-based injury surveillance system and postal mail survey to facilitate athlete self-report of data on exposure and injury events. We introduced the concept of a web-based ‘weekly e-diary’ to overcome difficulties in collecting the continuous information needed, that is, hours of training per week. Web-based survey methods have been reported to be reliable, in particular among young adults. 27 28 Study protocol specification The core of the protocol is deployed on an internet website for athlete self-report of data on exposure to athletic training and competition as well as injury surveillance (fi gure 2). The athlete enters the primary surveillance data themself on the website (for those under the age of 18 years with support from parents). Due to the wide geographical spread of athletics athletes, standardised physical examinations are difficult to administrate. No data on clinical biomechanical examinations are therefore included in the basic level of the protocol. Data on the athlete’s psychological profi le are collected using paper questionnaires by a postal survey, mainly because visual analogue scales have not been completely validated for use in electronic instruments/tools (for online surveys). Baseline questionnaires Baseline data are collected in two sets. First, data are collected using a web questionnaire (online appendix 1) asking for demographic data and subject characteristics, ie, sex, age, height, weight, experiences from participation in athletics, main event/discipline and previous injuries. Second, data for the psychological profi le are collected using a paper-based 1108 form created from a combination of validated instruments, measuring private and public body consciousness (BSC), 29 psychological commitment to exercise, 30 coping (BRIEF COPE), 31 perceived motivational climate (Perceived Motivational Clittiate in Sport Questionnaire) 32 and general health-related quality of life (EQ-5D). 33 Athlete weekly e-diary Data on athletic training and competition as well as injury surveillance are collected using an e-diary which is to be fi lled in weekly (online appendix 2). Each week, an alert is automatically sent out to participants’ email addresses, inviting them to complete a questionnaire about amount of training and competition hours, and occurrence or absence of injury. In addition, the diary collects information on each athlete’s training level, that is, whether the training is performed at full capacity or not, the number of practice sessions, medical contacts and general well-being. If the athlete reports any injury, they are requested to report modification of training, and numbers of missed training sessions in relation to that injury. The study coordinator monitors the injury data reported in the weekly reports. If an athlete is absent from training due to a reported, but not diagnosed, injury event which has lasted longer than 3 weeks, the event is followed up by email or telephone interviews. Injury-related problems, as defi ned above that prevent the athlete from returning to full training, are requested to be examined by a sports physician or sports physiotherapist at the site to affi rm a full clinical diagnosis. Injury report form The occurrence of a perceived injury event is fi rst reported in the weekly e-diary. When an injury is reported, the athlete is provided with a link to an injury report form (online appendix 3) where additional questions on the current injury are to be reported. The form used for injury surveillance is a modified version of the injury report form reported by the soccer consensus and International Olympic Committee (IOC) groups. 34 This injury report form has been shown to be feasible for the collection of injury data during athletic competitions. 24 The original form34 was translated into Swedish using a back-translation procedure, 35 and adjusted for online recording. All original items were included in our web injury report form, while questions were added regarding (A) injury event context (training/competition; indoors/outdoors), (B) specification of training method performed at time of injury (endurance, weight, sprint, etc), (C) anatomical site of the injury (left/right, back/front), (D) individual who made the preliminary diagnosis (trainer, medical profession, parent, etc) and (E) recurrence of earlier injury. Injury closure form When the injured athletes report in the e-diary that they have returned to normal athletic training, they are asked to complete a web-based injury closure form (online appendix 4) which asks for information regarding (A) time duration off full athletics training, (B) fi nal diagnosis of the injury, (C) individual who made the diagnosis and (D) treatment received. There is also the possibility to provide personal remarks about the injury reported. Protocol implementation: the Swedish athletics injury study The web-based system for injury surveillance in the Swedish athletics injury study is based on a commercial product for Br J Sports Med 2010;44:1106–1111. doi:10.1136/bjsm.2009.067678 Downloaded from bjsm.bmj.com on September 6, 2014 - Published by group.bmj.com Original article ATHLETICS Limited coach supervision Individual practice Individual training programmes behaviour Wide geographical spread Limited access to medical staff Over-reach/ overuse Requirements Self report of data Adjusted exposure definition Adjusted injury event definition Psychological profile e-diary Questionnaires Protocol e-diary Web system for data collection and storage Figure 2 Display of associations underlying the study protocol specification. collection of survey data over the internet (SiteVision V.2.5; Senselogic AB, Örebro, Sweden). The product enables definition of personal usernames and passwords to protect data from unauthorised use. Ethics Ethical approval was obtained for the study from the Research Ethics Committee in Linköping, Sweden in November 2008 (registration number M-201-08). Informed written consent was collected from all study participants. For those under the age of 18 years, approval was collected from their parents. Informed written consent was also collected from all participants in the pilot studies. Subject recruitment We aimed to recruit ‘unique’ top-10 athletes in each discipline (19 disciplines for adults, 18 disciplines for youths), age group (adult and youths (under-18)) and sex. Four top-10 lists (two adult and two youth) for each discipline were thus compiled by the Swedish Athletic Association (SAA). The SAA maintains statistics for the top-25 adult and top-20 adolescent Br J Sports Med 2010;44:1106–1111. doi:10.1136/bjsm.2009.067678 athletes in each discipline (http://www.friidrott.se). If an athlete was ranked among the top 10 in more than one discipline, the athlete was only included in their self-reported main discipline, and number 11 on the top 25 was upgraded to the top-10 list. If an adult athlete’s address was not recorded at the SAA, it was tracked and obtained from their athletics club. No such central record exists at the SAA for youth athletes. The addresses were instead collected from a website listing contact information for Swedish citizens (http://www. upplysning.se; Berlock Information AB, Enköping, Sweden). Letters of invitation were distributed by postal mail to all athletes targeted for the study and for whom addresses could be found in December 2008. The athletes received information about the forthcoming study, a consent form for participation, a request for a contact email address and a prepaid return envelope. Six hundred and forty-seven athletes (369 adults and 278 youths) were informed about the study by letter and invited to participate. Seventy-one per cent (n=459) 1109 Downloaded from bjsm.bmj.com on September 6, 2014 - Published by group.bmj.com Original article responded to the invitation, among whom 70% (n=321) consented to participate in the study. Twenty athletes withdrew from the study after a fi rst consent due to retirement from athletics. The fi nal study population thus consisted of 301 athletes. Ninty-one per cent (n=278) of the fi nal population contributed data over the web-based system the fi rst study week. Thereafter, on average 74–83% of the athletes contributed reports each week, some athletes fi ling their reports and submitting them each second or third week. DISCUSSION We have presented a protocol for epidemiological injury surveillance in athletics, provided arguments for its design and reported preliminary experiences from a fi rst implementation. To maintain compatibility with previous studies, the ambition was that as many features as possible from existing guidelines for team sports are transferred to the athletics protocol. We found in the requirements analysis that the central demand on the protocol was that it had to allow for detailed epidemiological analyses of overuse injuries, which subsequently requires regular collection of self-reported data from athletes. These conclusions had several consequences for the detailed protocol design. First, the self-reported injury events had to be defi ned broad enough to cover conditions resulting from loads at the borderline between over-reaching and overuse. Nevertheless, the defi nition still had to be sufficiently exact to admit rigorous recording of what medically, by coaches and from the perception of individual athletes, are considered to be an injury. In addition, we found that in order to be able to interpret the self-reported data on injury events epidemiologically, a wide range of personal baseline data, including a psychological profi le, needed to be collected from each athlete. To cope with this task, the traditional infrastructure for data collection and analysis had to be extended. One motivation for large-scale epidemiological studies in athletics is the need to be able to tailor preventive interventions to subgroups of athletes, taking into account, for example, age group, sex and type of event. A particular need for prevention concerns the association between the physical and behavioural maturation of children and injury occurrence, taking into account injury risks both in the near future and later on in their sporting career. Competing with the best athletes at both national and international levels is today not only a goal for adult athletics athletes but also a part of the ambitions of youth athletes. For example, the world championships in athletics for the age group 17 years is today organised by the International Association of Athletic Federations every second year. In order to fi nd safe ways to train elite children effectively, the IOC emphasises that international sports federations and national sports governing bodies must make use of scientific research methods to identify safe training volumes and develop injury- surveillance programmes also for this group of athletes. 36 The elite youth athlete should not be encouraged to invest years of training in a sport where a promising career can be abruptly ended due to a preventable injury indirectly caused by lack of scientific knowledge. It is possible that only novel infrastructural means, such as the use of internet-based information technology, can make it feasible to offer these age groups in an individual sport, such as athletics, injury-prevention services. This is because systematic injury surveillance requires the collection of individual-level data over long periods of time 1110 and the performance of compound computations on these data sets. In conclusion, the need for epidemiological evidence as a foundation for planning of preventive interventions in sports is today well established. 37 38 However, in several individual sports, including athletics, this body of basic research is still missing. The protocol presented in this paper should be regarded as one means to overcome this shortcoming. However, before wide dissemination of the protocol, it is necessary to analyse and evaluate the international variations within the organisation and performance of athletics as an elite and community sport. For instance, an e-diary was included as a central part in the surveillance process. Introduction of the e-dairy demands a certain level of technological infrastructure and additional investments, which may not be available in other regions of the world. The implementation procedure must, before introducing web-based injury surveillance methods on a broad scale in athletics, be adapted to the conditions in the setting where the surveillance will be conducted. Acknowledgements The study was supported by research grants from the Swedish Centre for Sports Research, the SAA and Linköping University. Funding Swedish Centre for Sports Research and SAA. Competing interests None. Patient consent Obtained. Ethics approval Ethics approval was provided by the Ethical Board at Linköping University. Provenance and peer review Not commissioned; not externally peer reviewed. Contributors JJ, JK, SN, JE, PR and TT contributed to the analyses reported in the study. JJ, JE and TT drafted the first version of the paper. All authors provided comments on subsequent versions and have read and approved the final manuscript. JJ, JK and TT act as coordinators of the Swedish athletics study. TT is the guarantor of the study. Demonstration versions of the online questionnaires (online appendices 1–4) are available for download (http://www.imh.liu.se/samhallsmedicin/socialmedicin/ injury_epidemiology_individual_sports?l=en). What is already known on this topic ▶ ▶ Systematic injury surveillance has been implemented at the elite level in team sports but seldom in individual sports. Surveillance of injury prevalence and incidence in athletics has been scarce and lacked the uniformity in methods and data definitions that would allow observed injury patterns to be generalised among populations. What this study adds ▶ ▶ ▶ A formatively evaluated protocol for injury surveillance in athletics is reported. Injury surveillance in individual sports requires collection of individual-level data over long periods of time. Novel infrastructural means, such as internet-based information technology, makes it feasible to offer also individual sports injury-prevention services. Br J Sports Med 2010;44:1106–1111. doi:10.1136/bjsm.2009.067678 Downloaded from bjsm.bmj.com on September 6, 2014 - Published by group.bmj.com Original article REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. Watson MD, DiMartino PP. Incidence of injuries in high school track and field athletes and its relation to performance ability. Am J Sports Med 1987;15:251– 4. D’Souza D. Track and field athletics injuries—a one-year survey. Br J Sports Med 1994;28:197–202. Bennell KL, Malcolm SA, Thomas SA, et al. Risk factors for stress fractures in track and field athletes. A twelve-month prospective study. Am J Sports Med 1996;24:810 –18. Bennell KL, Crossley K. Musculoskeletal injuries in track and field: incidence, distribution and risk factors. Aust J Sci Med Sport 1996;28:69 –75. Lysholm J, Wiklander J. Injuries in runners. Am J Sports Med 1987;15:168 –71. Rebella GS, Edwards JO, Greene JJ, et al. A prospective study of injury patterns in high school pole vaulters. Am J Sports Med 2008;36:913 –20. Lorentzon R, Wedrèn H, Pietilä T. Incidence, nature, and causes of ice hockey injuries. A three-year prospective study of a Swedish elite ice hockey team. Am J Sports Med 1988;16:392– 6. Waldén M, Hägglund M, Ekstrand J. Injuries in Swedish elite football—a prospective study on injury definitions, risk for injury and injury pattern during 2001. Scand J Med Sci Sports 2005;15:118 –25. Hägglund M, Waldén M, Ekstrand J. Exposure and injury risk in Swedish elite football: a comparison between seasons 1982 and 2001. Scand J Med Sci Sports 2003;13:364 –70. Timpka T, Risto O, Borg K, et al. Injury incidence in a men’s elite bandy league: an epidemiological study of a full regular season. Scand J Med Sci Sports 2007;17:636 – 40. Fuller CW, Ekstrand J, Junge A, et al. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Clin J Sport Med 2006;16:97–106. Fuller CW, Molloy MG, Bagate C, et al. Consensus statement on injury definitions and data collection procedures for studies of injuries in rugby union. Clin J Sport Med 2007;17:177– 81. Hägglund M, Waldén M, Bahr R, et al. Methods for epidemiological study of injuries to professional football players: developing the UEFA model. Br J Sports Med 2005;39:340 – 6. Orchard JW, Newman D, Stretch R, et al. Methods for injury surveillance in international cricket. Br J Sports Med 2005;39:e22. Orchard J, Hoskins W. For debate: consensus injury definitions in team sports should focus on missed playing time. Clin J Sport Med 2007;17:192– 6. Rittel HJW, Webber MM. Dilemmas in a general theory of planning. Policy Sci 1973;4:55 –169. Ackoff RL. Resurrecting the future of operational research. J Oper Res Soc 1979;30:189 – 99. Jones J, Hunter D. Consensus methods for medical and health services research. BMJ 1995;311:376 – 80. Polson PG, Lewis C, Rieman J, et al. Cognitive walkthroughs: a method for theory-based evaluation of user interfaces. Int J Man Mach Stud 1992;36:741–73. Peluso MA, Guerra de Andrade LH. Physical activity and mental health: the association between exercise and mood. Clinics (São Paulo) 2005;60:61–70. Br J Sports Med 2010;44:1106–1111. doi:10.1136/bjsm.2009.067678 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. Small EW, Bernhardt DT, Brenner JS, et al. Overuse injuries, overtraining, and burnout in child and adolescent athletes. Pediatrics 2007;119:1242– 5. Orava S, Saarela J. Exertion injuries to young athletes: a follow-up research of orthopaedic problems of young track and field athletes. Am J Sports Med 1978;6:68 –74. Bennell KL, Malcolm SA, Thomas SA, et al. The incidence and distribution of stress fractures in competitive track and field athletes. A twelve-month prospective study. Am J Sports Med 1996;24:211–17. Alonso JM, Junge A, Renström P, et al. Sports injuries surveillance during the 2007 IAAF world athletics championships. Clin J Sport Med 2009;19 :26 – 32 . Zemper ED. Track and field injuries. Med Sport Sci 2005;48:138 – 51. Junge A, Dvorak J, Rösch D, et al. Psychological and sport-specific characteristics of football players. Am J Sports Med 2000;28:S22– 8. Ekman A, Dickman PW, Klint A, et al. Feasibility of using web-based questionnaires in large population-based epidemiological studies. Eur J Epidemiol 2006;21:103 –11. Ekman A, Klint A, Dickman PW, et al. Optimizing the design of web-based questionnaires – experience from a population-based study among 50,000 women. Eur J Epidemiol 2007;22:293 – 300. Miller LC, Murphy R, Buss AH. Consciousness of body—private and public. J Pers Soc Psychol 1981;41:397– 406. Davis C, Brewer H, Ratusny D. Behavioral frequency and psychological commitment: necessary concepts in the study of excessive exercising. J Behav Med 1993;16:611–28. Steffen K, Pensgaard AM, Bahr R. Self-reported psychological characteristics as risk factors for injuries in female youth football. Scand J Med Sci Sports 2008;19:442– 51. Seifriz JJ, Duda JL, Chi LK. The relationship of perceived motivational climate to intrinsic motivation and beliefs about success in basketball. J Sport Exerc Psychol 1992;14:375 – 91. Lawrence WF, Fleishman JA. Predicting EuroQoL EQ-5D preference scores from the SF-12 Health Survey in a nationally representative sample. Med Decis Making 2004;24:160 – 9. Junge A, Engebretsen L, Alonso JM, et al. Injury surveillance in multi-sport events: the International Olympic Committee approach. Br J Sports Med 2008;42:413 –21. Nilsson P, Baigi A, Marklund B, et al. Cross-cultural adaptation and determination of the reliability and validity of PRTEE-S (Patientskattad Utvärdering av Tennisarmbåge), a questionnaire for patients with lateral epicondylalgia, in a Swedish population. BMC Musculoskelet Disord 2008;9:79. Mountjoy M, Armstrong N, Bizzini L, et al. IOC consensus statement: ‘training the elite child athlete.’ Br J Sports Med 2008;42:163 – 4. Ljungqvist A, Jenoure PJ, Engebretsen L, et al. The International Olympic Committee (IOC) consensus statement on periodic health evaluation of elite athletes, March 2009. Clin J Sport Med 2009;19:347– 65. Orchard JW, Seward H. Decreased incidence of knee posterior cruciate ligament injury in Australian Football League after ruck rule change. Br J Sports Med 2009;43:1026 – 30. 1111 Downloaded from bjsm.bmj.com on September 6, 2014 - Published by group.bmj.com Design of a protocol for large-scale epidemiological studies in individual sports: the Swedish Athletics injury study Jenny Jacobsson, Toomas Timpka, Joakim Ekberg, et al. Br J Sports Med 2010 44: 1106-1111 originally published online May 19, 2010 doi: 10.1136/bjsm.2009.067678 Updated information and services can be found at: http://bjsm.bmj.com/content/44/15/1106.full.html These include: References This article cites 38 articles, 16 of which can be accessed free at: http://bjsm.bmj.com/content/44/15/1106.full.html#ref-list-1 Article cited in: http://bjsm.bmj.com/content/44/15/1106.full.html#related-urls Email alerting service Topic Collections Receive free email alerts when new articles cite this article. Sign up in the box at the top right corner of the online article. Articles on similar topics can be found in the following collections Epidemiology (130 articles) Notes To request permissions go to: http://group.bmj.com/group/rights-licensing/permissions To order reprints go to: http://journals.bmj.com/cgi/reprintform To subscribe to BMJ go to: http://group.bmj.com/subscribe/