The Utility of Ultrasound in Detecting Anterior
advertisement

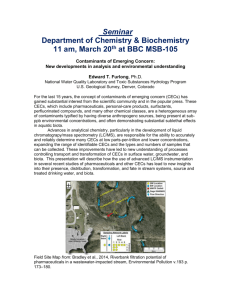
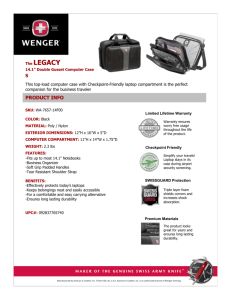
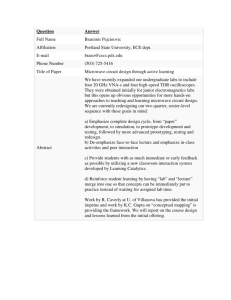
ORIGINAL RESEARCH The Utility of Ultrasound in Detecting Anterior Compartment Thickness Changes in Chronic Exertional Compartment Syndrome: A Pilot Study Sathish Rajasekaran, MD,* Cole Beavis, MD,† Abdel-Rahman Aly, MD,* and Dave Leswick, MD‡ Objective: To test the hypothesis that patients with chronic exertional Key Words: ultrasonography, sports medicine, anterior compartment syndrome compartment syndrome (CECS) of the anterior leg compartment have an increased anterior compartment thickness (ACT) compared with control subjects after exertion using ultrasound. (Clin J Sport Med 2013;23:305–311) Design: Prospective comparison study. Setting: Diagnostic imaging department of a tertiary care hospital. Patients: Four patients with CECS and 9 control subjects. Interventions: Patients with CECS and control subjects ran on a treadmill for up to 10 minutes. Anterior compartment thickness (both groups) and anterior compartment pressure (CECS patients) were measured before exertion and at scheduled intervals after exertion. Main Outcome Measures: Anterior compartment thickness, percentage change in ACT from rest, and compartment pressure. Results: Anterior compartment pressures were diagnostic of CECS using the modified Pedowitz criteria in patients with CECS. Mean percentage change in ACT from rest in patients with CECS versus control subjects at 0.5 minutes was 21.3% versus 6.32% [95% confidence interval (CI), 6.92-35.6 and 0.094-12.5, respectively; P = 0.011]; at 2.5 minutes, it was 24.6% versus 4.22% (95% CI, 10.738.5 and 21.85-10.3, respectively; P = 0.003); and at 4.5 minutes, it was 24.9% versus 5.08% (95% CI, 14.3-35.5 and 20.813-11.0, respectively; P = 0.003). Mean ACT in patients with CECS versus control subjects significantly increased after exertion (P = 0.003) at 0.5 minutes, 2.5 minutes, and 4.5 minutes. Conclusions: Ultrasonography reveals a significant increase in ACT in patients with CECS of the anterior leg compartment. Further studies are warranted to validate these findings with the goal of developing anterior leg compartment CECS ultrasound diagnostic criteria and exploring the role of using ultrasound to diagnose CECS in other compartments. Submitted for publication August 15, 2012; accepted December 29, 2012. From the *Department of Physical Medicine and Rehabilitation, University of Saskatchewan, Saskatoon, Canada; and †Division of Orthopaedic Surgery, Department of Surgery, University of Saskatchewan, Saskatoon, Canada; and ‡Department of Diagnostic Imaging, University of Saskatchewan, Saskatoon, Canada. The authors report no conflicts of interest. Corresponding Author: Sathish Rajasekaran, MD, Physical Medicine and Rehabilitation, 7th Floor, Saskatoon City Hospital, 701 Queen St, Saskatoon, SK SYK 0M7, Canada (sathish.k.rajasekaran@gmail.com). Copyright © 2013 by Lippincott Williams & Wilkins Clin J Sport Med Volume 23, Number 4, July 2013 INTRODUCTION Chronic exertional compartment syndrome (CECS) is reported to occur in 14% to 27% of patients with undiagnosed exertional leg pain.1,2 The incidence is equal between men and women, with a median age of 20 years.2 This condition often occurs in athletes, with running being the most common precipitating activity.3 The majority of CECS cases have been reported in the lower leg, with the anterior compartment being most often affected and bilateral leg involvement in up to 82% of cases.4,5 After a specific amount of exertion, patients with CECS typically report pain in the affected compartment.2,6 Patients report a dull aching fullness that worsens with prolonged activity and resolves with rest.7 The physical examination is typically normal at rest. Reported findings after exertion include muscle hernias, pain with passive stretching of the involved muscles, and abnormal neurological findings in the distribution of the affected nerve.8 The modified Pedowitz criteria is the most commonly used method to diagnose CECS in the lower leg using preexertional and postexertional intracompartmental pressure testing.5,7,9 However, several weaknesses have been reported in the design of their study, and the criteria has been found to have overlapping confidence intervals between healthy subjects and patients with CECS.10 Furthermore, a recent systematic review found conflicting and poor evidence for the methods used for intracompartmental pressure testing.11 Increased signal intensity changes on magnetic resonance imaging (MRI) in patients with CECS after exertion are reported in the literature.12–17 However, MRI is not widely used as a validated technique to diagnose CECS and has only been reported in 2 studies, with this technique being exclusively used at the Mayo Clinic (Rochester, Minnesota) to diagnose CECS of the anterior leg compartment.16,17 Functional imaging studies have not proven to aid in the diagnosis of CECS.18–23 Near-infrared spectroscopy is reported to approach the accuracy of intracompartmental pressure testing for the diagnosis of CECS, but further research is needed to validate this imaging modality for clinical use.24–27 The role of using ultrasound in the diagnosis of CECS of the anterior leg compartment was first described by Gershuni et al28 and subsequently a technique has been validated to measure www.cjsportmed.com | 305 Clin J Sport Med Volume 23, Number 4, July 2013 Rajasekaran et al anterior compartment thickness (ACT) by another group.29 This technique was used in 2 studies to measure the change in ACT after isometric and eccentric exercises in patients with CECS of the anterior leg compartment and control subjects, finding no significant differences between the groups.30,31 The objective of our study was to measure ACT with ultrasound before and after exertion on a treadmill in patients with CECS of the anterior leg compartment and control subjects and analyze if ACT and percentage change in ACT from rest was significantly different after exertion. We hypothesized that ACT would be significantly increased in patients with CECS compared with that in control subjects after exertion. MATERIALS AND METHODS All subjects gave written informed consent to participate in the study, which was approved by the Institutional Review Board of the University of Saskatchewan. TABLE 2. Inclusion Criteria for Patients With CECS 1. Pain (burning, aching, sharp, fullness, dull or pressure) in the anterior compartment after lower extremity exertion? 2. Pain worsened with prolonged lower extremity exertion? 3. Majority of pain relieved within #30 minutes of rest? 4. Able to run for $5 minutes? 5. No clinical or electrodiagnostic findings of peroneal neuropathy? 6. No clinical or Doppler ultrasonographic findings of popliteal artery syndrome? 7. No clinical or positive bone scans confirming the presence of tibial or fibular fractures? 8. No previous fasciotomy in the leg? YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO A response of “yes” is required for questions 1 to 8 to meet inclusion criteria. Patients and Control Subjects Ten control subjects were recruited through the department of diagnostic imaging (medical residents and technicians) and screened (Table 1) for the precision phase of this study. A letter outlining the study and requesting patients presenting with symptoms suggestive of CECS be referred to us was sent to physicians practicing sports medicine within the health region. Over a 1-year period, 8 patients were referred and screened with our inclusion criteria (Table 2), leading to 4 patients (3 men and 1 woman) meeting the clinical criteria to participate in the study (Figure 1). Intracompartmental pressures were not measured in patients suspected of CECS before the study. Nine control subjects were TABLE 1. Exclusion Criteria for Precision Phase and Study Control Subjects 1. Pain (burning, aching, sharp, fullness, dull, or pressure) after lower extremity exertion in the leg? 2. After lower extremity exertion, pain with palpation of lower leg muscle(s)? 3. After lower extremity exertion, pain with passive stretch of lower leg muscle(s) 4. After lower extremity exertion, lower leg muscle herniation? 5. After lower extremity exertion, dorsiflexion weakness? 6. After lower extremity exertion, eversion weakness? 7. After lower extremity exertion, numbness of the first web space? 8. After lower extremity exertion, numbness of the dorsum of the foot? 9. After lower extremity exertion, plantar flexion weakness? 10. After lower extremity exertion, numbness of the lateral foot? 11. After lower extremity exertion, numbness of the distal calf? 12. After lower extremity exertion, numbness of the sole of the foot? 13. Previous diagnosis of CECS? YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO A response of “yes” to any of the questions (1-13) excludes the individual from participating in the precision phase or as a control subject in the study. 306 | www.cjsportmed.com FIGURE 1. Schematic overview of patient inclusion and exclusion criteria. ELP, exertional leg pain; PAES, popliteal artery entrapment syndrome. Ó 2013 Lippincott Williams & Wilkins Clin J Sport Med Volume 23, Number 4, July 2013 recruited through the department of diagnostic imaging (medical residents and technicians) for the study and screened for exertional leg pain symptoms (Table 1). Equipment Ultrasound images were obtained using a Philips iU22 (Philips Ultrasound Systems, Bothell, Washington) with a 12-5 MHz linear array transducer by the diagnostic medical sonographer (N.K.). Standard ultrasound gel was used for all scans. The general musculoskeletal settings of the ultrasound machine were used for image optimization, and the ultrasound machine received routine maintenance based on the manufacturer’s recommendations. The Stryker Intracompartmental Pressure Monitor System with a side-ported 18-gauge needle (Stryker Surgical, Kalamazoo, Michigan) was used for pressure testing. Ultrasound Technique The ACT was measured at 20% of the distance from the head of the fibula to the lateral tip of the lateral malleolus, where the ACT was found to correlate with the crosssectional area of the anterior compartment.29 This landmark was located while the subjects lied supine. Using ultrasound coupling gel, the probe was placed on the landmark at an approximated 90-degree angle to the anterior tibial muscle group to minimize anisotropy and parallel to the interosseous membrane.29 Real-time images of the anterior tibial muscle group were captured (Figure 2).29 The thickness of the anterior tibial muscle group was measured by placing one caliper on the border of the interosseous membrane facing the anterior compartment and the second caliper on the interior border of the fascia adjacent to the subcutaneous fat measuring the shortest distance between the borders (Figure 2). All ACT measurements were made by the same diagnostic medical sonographer (N.K.). Ultrasound Findings in CECS Precision Phase The diagnostic medical sonographer’s (N.K.) technique was validated with a precision phase before scanning study patients using 10 control subjects who were screened for exertional leg pain symptoms (Table 1). Resting ACT was measured after lying supine for 10 minutes and again after 3 sets of 10 calf raises. The same exercise protocol and ultrasound recordings were repeated after 10 minutes of rest in each control subject. Study Phase Patients (n = 4) were asked to refrain from exercising on the day before testing. The point of needle insertion for pressure testing in the dominant leg (all patients had bilateral symptoms) was localized by marking a point 10 cm distal to the tibial tubercle and 1.5 cm lateral to the anterior tibial crest.32 The ankle was placed in a neutral position and the knee placed in 10 degrees of flexion (confirmed with goniometer) to minimize the effect of joint position on intracompartmental pressure.32 Patients then laid supine for 20 minutes to ensure the intracompartmental pressure normalized. The insertion site was prepped with antiseptic and anesthetized with 1 mL of 1% lidocaine. The needle was inserted at the previously localized point to a depth of 2.5 cm at a 45-degree angle to the skin surface.32 The pressure was allowed to stabilize and then recorded. Anterior compartment thickness was then measured and recorded. Patients were asked to exercise on a treadmill beginning at 3 mph and a 0% grade of incline. After 2 minutes, the running speed was increased gradually up to 7 mph (1 mph/1 minute) and a 20% grade of incline (5% grade/1 minute). Patients were instructed to run for at least 5 minutes and to increase the speed and incline (within the exercise protocol) as tolerated to maximize their symptoms. The duration of exertion was recorded, and the timer was restarted once the patient stopped running. Patients were instructed to lie supine with the previous configuration of the dominant leg once they stopped running. Compartment pressures were obtained at 1 minute, 3 minutes, and 5 minutes after exercise. Anterior compartment thickness was measured at 30 seconds, 2.5 minutes, and 4.5 minutes after exercise. Anterior compartment pressure was used to confirm the diagnosis of CECS using the modified Pedowitz criteria.5 Control Phase The same ultrasound measurements were taken without corresponding compartment pressures in control subjects (n = 9). All control subjects ran for 10 minutes and reached 7 mph and a 20% grade of incline (1 mph/1 minute and 5% grade/1 minute) after warming up at 3 mph and a 0% grade of incline for 2 minutes. Statistical Analysis FIGURE 2. Ultrasound marker placement for ACT measurement using ultrasound in patients at rest. Line represents interosseous membrane, dotted line represents fascial border with subcutaneous fat, crosshairs denote calipers, and double-headed arrow denotes ACT. ATMG, anterior tibial muscle group; Fib, fibula; TP, tibialis posterior; Tib, tibia. Ó 2013 Lippincott Williams & Wilkins Intraclass correlation coefficient equations were used to examine the repeatability of the preexercise and postexercise ACT data in the precision phase.33 Confidence intervals (95%) for means were calculated using the 1-sample t test. The Wilcoxon signed rank test was used to compare postexertion pressure and ACT within each group from resting values. The Wilcoxon www.cjsportmed.com | 307 Clin J Sport Med Volume 23, Number 4, July 2013 Rajasekaran et al rank sum test was used to compare ACT and percentage change in ACT from rest between patients with CECS and control subjects. All data analysis was completed using SAS 9.3 for Windows software (SAS Institute, Inc, Cary, North Carolina). 2.12-2.45; P = 0.086) (Figure 3). Statistical significance was not found in mean ACT in patients with CECS versus control subjects at rest (P = 0.05) but was significant (P = 0.003) at 0.5 minutes, 2.5 minutes, and at 4.5 minutes after exertion. Percentage Change in ACT RESULTS Precision Phase Preexertional and postexertional ACT repeatability was high, and intraclass correlation coefficients (1,1) for both measurements was 0.96 [95% confidence interval (CI), 0.860.99 and 0.85-0.99, respectively]. Patient and Control Demographics Mean age of patients with CECS (3 men and 1 woman) and control subjects (5 men and 4 women) was 35.3 years and 32.6 years, respectively (95% CI, 28.0-42.5 and 27.8-37.3, respectively). Mean running time in patients with CECS was 6.0 minutes (95% CI, 3.8-8.3), and control subjects ran for 10 minutes. Compartment Pressure Compartment pressure in patients with CECS was 21.5 mm Hg at rest (95% CI, 17.3-25.7), 38.3 mm Hg at 1 minute (95% CI, 30.3-46.2; P = 0.068), 34.5 mm Hg at 3 minutes (95% CI, 27.4-41.6; P = 0.068), and 38.8 mm Hg at 5 minutes (95% CI, 18.9-58.6; P = 0.068). Pressures in all 4 patients were diagnostic of CECS using the modified Pedowitz criteria.5 Anterior Compartment Thickness Mean ACT in patients with CECS was 2.63 cm at rest (95% CI, 2.11-3.15), 3.17 cm at 0.5 minutes (95% CI, 2.733.61; P = 0.068), 3.26 at 2.5 minutes (95% CI, 2.92-3.59; P = 0.068), and 3.26 at 4.5 minutes (95% CI, 2.82-3.69; P = 0.068) (Figure 3). Anterior compartment thickness in control subjects was 2.18 cm at rest (95% CI, 2.06-2.30), 2.32 at 0.5 minutes (95% CI, 2.13-2.50; P = 0.086), 2.27 cm at 2.5 minutes (95% CI, 2.10-2.43; P = 0.173), and 2.29 cm at 4.5 minutes (95% CI, FIGURE 3. Mean ACT in patients with CECS and control subjects. Statistical significance was found in between-group comparisons (P = 0.05 at rest, P = 0.003 at 0.5 minutes, 2.5 minutes, and 4.5 minutes). Statistical significance was not found in within-group comparisons (P . 0.05). Vertical lines represent 95% CIs. 308 | www.cjsportmed.com Mean percentage change in ACT from rest in patients with CECS was 21.3% at 0.5 minutes (95% CI, 6.92-35.6), 24.6% at 2.5 minutes (95% CI, 10.7-38.5), and 24.9% at 4.5 minutes (95% CI, 14.3-35.5) (Figure 4). Mean percentage change in ACT from rest in control subjects was 6.32% at 0.5 minutes (95% CI, 0.094-12.5), 4.22% at 2.5 minutes (95% CI, 21.85-10.3), and 5.08% at 4.5 minutes (95% CI, 20.813-11.0) (Figure 4). Statistical significance was found in mean percentage change in ACT from rest in patients with CECS versus control subjects at 0.5 minutes (P = 0.011), 2.5 minutes, and 4.5 minutes (P = 0.003) after exertion. DISCUSSION Our study is the first to describe statistically significant findings (ACT, percentage change in ACT from rest) between patients with CECS of the anterior leg compartment and control subjects after exertion using ultrasound. Two studies have used ultrasound to measure ACT in patients with CECS of the anterior leg compartment, performing eccentric or isometric exercises and found no statistical difference between patients with CECS and control subjects after exertion.30,31 In the isometric exercise study, patients with CECS reported a median pain score of 6 with a range between 1 and 9 after 20 minutes of exercise compared with a median pain score of 1.5 (range, 0-6) in control subjects.31 In the eccentric exercise study, there was no statistical difference in pain scores between patients with CECS and control subjects during exercise or recovery.30 The varied severity of symptoms in patients with CECS after exercise in the isometric exercise study and lack of significant differences in symptoms between patients with CECS and control subjects in the eccentric exercise study may have contributed to the lack of significant findings on ultrasound in both studies.30,31 FIGURE 4. Mean percentage change in ACT from rest in patients with CECS and control subjects. Statistical significance was found in between-group comparisons (P = 0.011 at 0.5 minutes and P = 0.003 at 2.5 and 4.5 minutes). Vertical lines represent 95% CIs. Ó 2013 Lippincott Williams & Wilkins Clin J Sport Med Volume 23, Number 4, July 2013 Additionally, in the isometric exercise study, percentage change in ACT was measured at rest, 20 minutes, 22.5 minutes, 25 minutes, 27.5 minutes, and 30 minutes after exercise.31 These delayed postexercise measurements may have also contributed to the lack of significant findings on ultrasound in the isometric exercise study.31 In our study, we refrained from having a set duration and intensity of exercise but allowed patients with CECS to titrate this using a standardized protocol to ensure that they were symptomatic after exercise. Our validated technique revealed a significant difference in ACT and percentage change in ACT from rest in patients with CECS compared with control subjects at all time points after exertion. Statistical significance was not found when comparing ACT after exertion with resting values within patients with CECS. The 95% CIs for mean ACT compared with mean percentage change in ACT from rest in patients with CECS versus control subjects were more distinct for mean ACT after exertion. Furthermore, the statistical significance was greater for ACT at 0.5 minutes than percentage change in ACT from rest in patients with CECS versus control subjects (P = 0.003 vs P = 0.011, respectively) but identical at 2.5 and 4.5 minutes (P = 0.003). However, we hypothesize that percentage change in ACT may prove to be more beneficial Ultrasound Findings in CECS because it corrects for differences in leg size in the general population. Larger studies need to be undertaken to more confidently assess the benefit of one over the other with the goal of constructing a criteria for anterior leg compartment CECS diagnosis using ultrasound. A convexity in the anterior compartment fascia was seen in the ultrasound images of patients with CECS after exertion (Figure 5). We did not attempt to quantify this convexity, as the entire width of the fascia of the anterior compartment was not imaged. The combination of bowing of the fascia and a statistically significant increase in the ACT in patients with CECS compared with control subjects argues against the decreased compliance theory as the underlying pathophysiology of CECS.34,35 Furthermore, a recent study found no significant difference in the compliance of fascial tissue samples of patients with CECS of the anterior leg compartment compared with control subjects, which contradicts previous findings.34–36 Quantifying the changes in anterior compartment volume versus pressure of patients with CECS and control subjects would help clarify the role compliance plays in CECS. A more practical approach may be to use ACT to estimate volume because it has been found to correlate with the anterior compartment cross-sectional area.29 FIGURE 5. Anterior compartment thickness visualized with ultrasound. A, CECS patient at rest. B, CECS patient at 30 seconds after exertion. C, Control at rest. D, Control at 30 seconds after exertion. Ó 2013 Lippincott Williams & Wilkins www.cjsportmed.com | 309 Rajasekaran et al Clin J Sport Med Volume 23, Number 4, July 2013 FIGURE 6. Mean ACT plotted against corresponding (30-second delay) mean anterior compartment pressure in patients with CECS. Time 1 = 0.5minute ACT/1-minute compartment pressure; Time 2 = 2.5-minute ACT/ 3-minute compartment pressure; Time 3 = 4.5-minute ACT/5-minute compartment pressure. Correlating the relationship between ACT and pressure may prove to be a means of estimating compliance in patients with CECS of the anterior leg compartment (Figure 6). Comparing the estimated compliance curves between patients with CECS of the anterior leg compartment and control subjects may lead to a better understanding of the pathophysiology of CECS. Several study limitations are noteworthy. First, our sample size of patients with CECS (n = 4) and control subjects (n = 9) was very small and would need to be expanded to properly assess the role of using ultrasound to diagnose CECS of the anterior leg compartment. As this is a relatively uncommon condition, a multicenter trial or conducting this project at a larger referral center would help recruit more patients in future studies. Second, we did not standardize the discomfort perceived by patients with CECS or control subjects after exertion using a validated scale (Visual Analog Scale). However, we instructed patients with CECS to run until they could not tolerate the discomfort, and all the 9 control subjects reported no symptoms after exertion. Third, our control subjects were not age matched to patients with CECS. Fourth, the length and intensity of exercise was not identical between the groups or within patients with CECS. In an attempt to compensate for the difference between patients with CECS and control subjects, all control subjects ran for a longer duration (10 minutes) than patients with CECS and reached the full incline and speed defined in our exercise protocol. Even though duration, incline, and speed of the treadmill sessions were different among patients with CECS, all patients ran to the point where they could no longer tolerate the discomfort in their legs. Fifth, compartment pressure was not recorded at the same time ACT was measured. However, to do this, a different method (ie, slit catheter) would need to be used, and a further precision phase completed to ensure that pressure recordings were not affected by sonopalpation. Sixth, interrater reliability was not assessed in our precision phase. Seventh, repetitive dorsiflexion would have activated the anterior compartment muscles to a greater degree in the precision phase rather than calf raises. Eight, we did not blind the diagnostic medical 310 | www.cjsportmed.com sonographer, which undoubtedly decreased the quality of the study. However, this was attempted but complicated by the clearly apparent discomfort that patients with CECS had with transferring onto the bed, ankle positioning, and sonopalpation. Despite the limitations mentioned above, our study shows a promising role for using ultrasound, a noninvasive, readily available, and cost-effective method of imaging patients with suspected CECS of the anterior leg compartment. Further studies are warranted to validate the findings of this study in an attempt to develop an anterior leg compartment CECS ultrasound diagnostic criteria using ACT or percentage change in ACT from rest. If this is accomplished, further studies investigating the role of using ultrasound to diagnose CECS in other compartments is warranted. Furthermore, our novel description of estimating compliance may lead to a better understanding of the pathophysiology of CECS. ACKNOWLEDGMENTS The authors thank Nadine Kanigan for scanning study patients and recruiting controls. REFERENCES 1. Qvarfordt P, Christenson JT, Eklof B, et al. Intramuscular pressure, muscle blood flow, and skeletal muscle metabolism in chronic anterior tibial compartment syndrome. Clin Orthop Relat Res. 1983;179:284–290. 2. Shah SN, Miller BS, Kuhn JE. Chronic exertional compartment syndrome. Am J Orthop. 2004;33:335–341. 3. Taunton JE, Ryan MB, Clement DB, et al. A prospective study of running injuries: the Vancouver Sun Run "In Training" clinics. Br J Sports Med. 2003;37:239–244. 4. Detmer DE, Sharpe K, Sufit RL, et al. Chronic compartment syndrome: diagnosis, management, and outcomes. Am J Sports Med. 1985;13:162–170. 5. Pedowitz RA, Hargens AR, Mubarak SJ, et al. Modified criteria for the objective diagnosis of chronic compartment syndrome of the leg. Am J Sports Med. 1990;18:35–40. 6. Fraipont MJ, Adamson GJ. Chronic exertional compartment syndrome. J Am Acad Orthop Surg. 2003;11:268–276. 7. Tucker AK. Chronic exertional compartment syndrome of the leg. Curr Rev Musculoskelet Med. 2010;3:32–37. Ó 2013 Lippincott Williams & Wilkins Clin J Sport Med Volume 23, Number 4, July 2013 8. Bong MR, Polatsch DB, Jazrawi LM, et al. Chronic exertional compartment syndrome: diagnosis and management. Bull Hosp Jt Dis. 2005;62:77–84. 9. Hislop M, Tierney P. Intracompartmental pressure testing: results of an international survey of current clinical practice, highlighting the need for standardised protocols. Br J Sports Med. 2011;45:956–958. 10. Roberts A, Franklyn-Miller A. The validity of the diagnostic criteria used in chronic exertional compartment syndrome: a systematic review. Scand J Med Sci Sports. 2012;22:585–595. 11. Aweid O, Del Buono A, Malliaras P, et al. Systematic review and recommendations for intracompartmental pressure monitoring in diagnosing chronic exertional compartment syndrome of the leg. Clin J Sport Med. 2012;22:356–370. 12. Eskelin MK, Lotjonen JM, Mantysaari MJ. Chronic exertional compartment syndrome: MR imaging at 0.1 T compared with tissue pressure measurement. Radiology. 1998;206:333–337. 13. Lauder TD, Stuart MJ, Amrami KK, et al. Exertional compartment syndrome and the role of magnetic resonance imaging. Am J Phys Med Rehabil. 2002;81:315–319. 14. Verleisdonk EJ, van Gils A, van der Werken C. The diagnostic value of MRI scans for the diagnosis of chronic exertional compartment syndrome of the lower leg. Skeletal Radiol. 2001;30:321–325. 15. Amendola A, Rorabeck CH, Vellett D, et al. The use of magnetic resonance imaging in exertional compartment syndromes. Am J Sports Med. 1990;18:29–34. 16. Ringler MD, Litwiller DV, Felmlee JP, et al. MRI accurately detects chronic exertional compartment syndrome: a validation study. Skeletal Radiol. 2013;42:385–392. 17. Litwiller DV, Amrami KK, Dahm DL, et al. Chronic exertional compartment syndrome of the lower extremities: improved screening using a novel dual birdcage coil and in-scanner exercise protocol. Skeletal Radiol. 2007;36:1067–1075. 18. Takebayashi S, Takazawa H, Sasaki R, et al. Chronic exertional compartment syndrome in lower legs: localization and follow-up with thallium-201 SPECT imaging. J Nucl Med. 1997;38:972–976. 19. Hayes AA, Bower GD, Pitstock KL. Chronic (exertional) compartment syndrome of the legs diagnosed with thallous chloride scintigraphy. J Nucl Med. 1995;36:1618–1624. 20. Trease L, van Every B, Bennell K, et al. A prospective blinded evaluation of exercise thallium-201 SPET in patients with suspected chronic exertional compartment syndrome of the leg. Eur J Nucl Med. 2001;28:688–695. 21. Edwards PD, Miles KA, Owens SJ, et al. A new non-invasive test for the detection of compartment syndromes. Nucl Med Commun. 1999;20:215–218. 22. Oturai PS, Lorenzen T, Norregaard J, et al. Evaluation of Tc-99m-tetrofosmin single-photon emission computed tomography for detection of chronic exer- Ó 2013 Lippincott Williams & Wilkins Ultrasound Findings in CECS 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. tional compartment syndrome of the leg. Scand J Med Sci Sports. 2006;16: 282–286. Andreisek G, White LM, Sussman MS, et al. T2*-weighted and arterial spin labeling MRI of calf muscles in healthy volunteers and patients with chronic exertional compartment syndrome: preliminary experience. AJR Am J Roentgenol. 2009;193:W327–W333. McDonald S, Bearcroft P. Compartment syndromes. Semin Musculoskelet Radiol. 2010;14:236–244. van den Brand JG, Nelson T, Verleisdonk EJ, et al. The diagnostic value of intracompartmental pressure measurement, magnetic resonance imaging, and near-infrared spectroscopy in chronic exertional compartment syndrome: a prospective study in 50 patients. Am J Sports Med. 2005;33:699–704. Mohler LR, Styf JR, Pedowitz RA, et al. Intramuscular deoxygenation during exercise in patients who have chronic anterior compartment syndrome of the leg. J Bone Joint Surg Am. 1997;79:844–849. van den Brand JG, Verleisdonk EJ, van der Werken C. Near infrared spectroscopy in the diagnosis of chronic exertional compartment syndrome. Am J Sports Med. 2004;32:452–456. Gershuni DH, Gosink BB, Hargens AR, et al. Ultrasound evaluation of the anterior musculofascial compartment of the leg following exercise. Clin Orthop Relat Res. 1982;167:185–190. Martinson H, Stokes MJ. Measurement of anterior tibial muscle size using real-time ultrasound imaging. Eur J Appl Physiol Occup Physiol. 1991;63:250–254. Birtles DB, Rayson MP, Jones DA, et al. Effect of eccentric exercise on patients with chronic exertional compartment syndrome. Eur J Appl Physiol. 2003;88:565–571. Birtles DB, Minden D, Wickes SJ, et al. Chronic exertional compartment syndrome: muscle changes with isometric exercise. Med Sci Sports Exerc. 2002;34:1900–1906. Gershuni DH, Yaru NC, Hargens AR, et al. Ankle and knee position as a factor modifying intracompartmental pressure in the human leg. J Bone Joint Surg Am. 1984;66:1415–1420. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:307–310. Turnipseed WD, Hurschler C, Vanderby R Jr. The effects of elevated compartment pressure on tibial arteriovenous flow and relationship of mechanical and biochemical characteristics of fascia to genesis of chronic anterior compartment syndrome. J Vasc Surg. 1995;21:810–816. Hurschler C, Vanderby R Jr, Martinez DA, et al. Mechanical and biochemical analyses of tibial compartment fascia in chronic compartment syndrome. Ann Biomed Eng. 1994;22:272–279. Dahl M, Hansen P, Stal P, et al. Stiffness and thickness of fascia do not explain chronic exertional compartment syndrome. Clin Orthop Relat Res. 2011;469:3495–3500. www.cjsportmed.com | 311