Quality Account Report 2010 / 2011

Quality Account Report
2010 / 2011
Contents
1.0 Introduction and statement on quality from Managing Director
2.0 2011 / 2012 Quality Objectives
2.1 Statements of assurance from the Board
2.1.1 National Audits
2.1.2 Local Audits
2.2 Clinical Audits – National and Local
2.3 Research
2.4 Goals agreed with commissioners
2.5 What others say about us – Care Quality Commission
2.6 Data Quality Statement
3.0 Review of Quality Performance
3.1 Priority 1 – Ensuring patient and staff safety
3.2 Priority 2 – Ensuring efficient and effective clinical services
3.3 Priority 3 – Ensuring a Positive Patient Experience
3.4 Complaints
4.0 Statements from Local Involvement Network, HOSC and PCT
Page No.
3
5
21
30
2
1.0 Introduction and Statement on Quality from
the Managing Director
Delivering the right service, with the best staff, closer to home, first time, every time underpins our vision to become the leading provider of community health service in the South East and by 2014 becoming:
• The Service of Choice
• The Employer of Choice
• The Partner of Choice.
It gives me great pleasure to introduce West Kent Community Health’s first and last Quality Account as part of our achievement is that we now move forward as Kent Community Health NHS Trust.
Quality Accounts are aimed at assuring our patients, commissioners, and local population that we are focused not only on providing the highest level of clinical care, but also on continuously seeking ways of doing better. They are our opportunity to showcase where we are performing well, but also highlight areas in which we know we need to improve.
During 2010 / 2011 we can point to many achievements that demonstrate our commitment to high quality clinical care.
At Sevenoaks hospital, we have built a new Minor Injury Unit ensuring residents receive 21st Century care.
Our New Born Hearing Screening Service which was struggling to meet the most basic standards now fully complies with key national guidance and this has been externally validated by the Department of Health New Born Hearing Screening Programme National Quality Assurance Team.
Our Paediatric Audiology services have brand new accommodation at Sevenoaks, Gravesend and
Hawkhurst, to match the high clinical standards delivered by our audiology team.
The two improvements above were further recognised in our services being receiving an award from the Deaf Children’s Society for the outstanding care these services deliver to local residents.
Across our six community hospitals there were no breaches in delivering same sex accommodation.
At a time when other parts of the safeguarding children systems were in crisis our Children’s
Safeguarding teams were audited by South Coast Audit and found to provide significant assurance of compliance with national standards.
99% of our staff working in Child Protection receive supervision every 4 months. 100% of staff requiring an enhanced Criminal Record Bureau check had this undertaken.
Whilst we are proud of our successes we wish to do better; we have outlined in this Quality Account those areas we will be prioritising for improvement in the coming year.
These priority areas (detailed in part 2 of this report) are linked to the three domains of quality; patient safety, clinical effectiveness and patient experience.
3
We hope you will agree that our Quality Account provides many examples of where we are already providing the highest quality clinical care. We are confident that during 2011 / 2012 we will continue to work with our patients, staff and commissioners to do even better.
Finally, I confirm, in accordance with my statutory duty, that to the best of my knowledge the information in these Quality Accounts is accurate. I would like to thank our staff, who continuously strive to improve the care they deliver and patients for giving of their time to tell us when we got it right or helping us improve where we could do better.
Mark Shepperd
Managing Director
West Kent Community Health
NB: West Kent Community Health is the provider arm of WKPCT. This means that it provides the community services but is managed at arms length from the statutory body, West Kent PCT. West
Kent Community Health integrated with Eastern and Coastal Kent NHS Trust on 1st April 2011 to create Kent Community Health NHS Trust.
4
2.0 2011 / 2012 Quality Objectives
2011 / 2012 is an exciting but challenging year and the key focus of attention, as Kent Community
Health NHS Trust, will continue to be on three quality goals and associated pledges and actions as shown in the table below:
Ambition (quality goal) Related Pledge
Patient Safety
We will continuously develop our clinical practice so we can deliver evidenced based, appropriate and resilient care to our patients and services users
No one will contract Clostridium
Difficile or MRSA infections in any of our community hospitals
Actions to Achieve Quality
Goals 2011 / 2012
• Continue to sustain Infection
Prevention and Control
Management compliance
• Maintain standards of
cleanliness.
Clinical Effectiveness
(continuous improvement)
We will embed quality and performance at all levels of the organisation
Embed and measure quality improvement in services
Patient Experience
We will care for people and treat them kindly, professionally, with dignity and with respect
Ensure patients report a positive experience
• Introduction of care bundles
across high risk areas
• Clinical Quality and Safety in
Practice implementation
• Implementation of the service/
team level quality and safety
indicators
• Continue to complete actions
in relation to the single
equality scheme, research
project and work with trans
gender population
• Implement patient report
outcome measures (PROMs)
• Implement revised clinical
audit process
• Implement revised CQC
assurance process.
• Implement revised approach
to gaining views on patient
experience
• Implement personalisation
work.
•
•
•
•
•
Care bundles are monitoring tools that are applied at team level from the current active service caseload and is known as prospective monitoring (real time). This approach allows immediate corrective action to be taken by staff to risks that are highlighted it also serves to engage the staff in the quality agenda and allow them to own the improvement. Areas covered by care bundles include:
Pressure Ulcers
Nutrition
Medication Administration
Prevention from Infection
Falls.
5
Support in clinical practice will be via clinical practice coaches who will provide targeted support and education at team and service level to help with the continuous improvement of quality and safety of care delivery.
Patient experience has been, and will continue to be, a key focus for the trust. Going forward the focus will be on the personalisation agenda which has shown increased satisfaction for both patients and staff. We will also expand our options for collecting patient and carer feedback for example via an email link, through electronic devices and comment cards. Patient reported outcome measures will also be introduced.
2.1 Statements of assurance from the Board
During 2010 / 2011, West Kent Community Health provided / sub contracted 26 NHS services.
West Kent Community Health has reviewed all the data available to them on the quality of care in all
26 of these NHS services.
The income generated by the NHS services reviewed in 2010 / 2011 represents 100% of the total income generated from the provision of NHS services by West Kent Community Health for 2010 /
2011.
2.2 Clinical Audits – National and Local
2.2.1 National Audits
For the purposes of the quality account report, West Kent Community Health is required to review its
2010 / 2011 Clinical Audit Programme against National Clinical Audits for the same period of time.
During 2010 / 2011, there were 55 national clinical audits. West Kent Community Health participated in one audit. The remainder focused on services provided within acute hospital settings.
West Kent Community Health participated in the following National Clinical Audit:
• National Falls and Bone Health Audit: The patient sample received from the two partner acute trusts amounted to only one patient identified as being discharged to the community services.
Results and action planning is due to take place in June 2011.
During the period 2010 / 2011 West Kent Community Health participated in 100% of the national confidential enquiries which it was eligible to participate in as follows:
• Cardiac Arrest procedures: West Kent Community Health reported no cardiac arrests during the study period. The findings of the full study will be published in late 2012.
6
2.2.2 Local Audits
There were 108 local clinical audits/surveys registered in the period 2010 / 2011. As the table below shows there were 52 projects completed by year end 2010 / 2011. The remainder continue into
2011 / 2012. Completed audits include 2 national (1 audit and 1 national confidential enquiry) and 15
Essence of Care rolling programme of audits. The reports of the 52 completed projects have been reported via the West Kent Community Health governance committee structure.
Clinical Audit Programme Activity
Total projects registered 2010 / 2011: 108
Closed Projects: 52
Reasons & project type:
Project Abandoned
Completed & Action Plans in place
Completed & Best Practice Achieved
Essence of Care Audits
National
No Action Plan in place (no longer relevant due to service redesign)
Other
Total
Audits (34)
2
13
1
15
2
1
34
Surveys: (18)
PS (patient) SS (staff)
3
12 2
1
16 2
Essence of Care
West Kent Community Health is committed to ensuring best practice is adopted by all clinical staff when delivering patient care. Essence of Care (EoC) benchmarking (DH 2001) provides a tool to help practitioners take a patient focused and structural approach to sharing and comparing practice. It has enabled health and care personnel to work with patients to identify best practice and to develop action plans to improve care.
Year on year improvements are shown in the comparison graphs over the page.
These reports were also used to evidence improvements for Commissioning for Quality and
Innovation (CQUIN) (see section 2.4) indicators agreed with Commissioners.
7
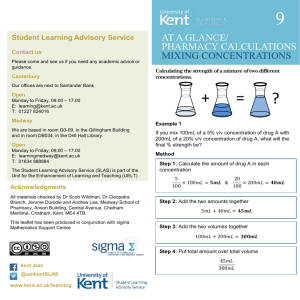
CQUIN comparison 2009 / 2010 and 2010 / 2011 common data Essence of Care summary report
Essence of Care comparison
100%
83%
96%
82%
100%
95%
85%
78%
Food and
Nutrition 09-10
Food and
Drink 10-11
100% 100%
100%
88%
81%
Bladder &
Bow el Care
09-10
91%
93%
86%
Bladder &
Bow el Care
10-11
93%
89%
84%
89%
75%
Record
Keeping
Jun09
97%
96%
82%
95%
100%
94%
88%
94%
90%
Record
Keeping Jul10
Personal &
Oral Hygiene
09-10
Community Hospitals Community Nursing Rapid Response MIU Neuro Rehab
100%
97%
94%
94%
Personal
Hygiene
10-11
100%
100%
88%
81%
48%
Privacy &
Dignity 09-10
100%
100%
88%
93%
94%
Respect
10-11
Essence of Care comparison
100%
85%
87%
88%
96%
99%
87%
71%
93%
93%
90%
81%
97%
97%
Self Care Sep
09
Self Care Oct
10
Pressure
Ulcers 09-10
Pressure
Ulcers 10-11
92%
89%
Care
Environment
09-10
100%
81%
92%
98%
100%
97%
95%
100%
96%
95%
89%
84%
92%
98%
87%
74%
95%
83%
Care
Environment
10-11
Promoting
Health 09-10
Promoting
Health 10-11
Safety 09-10 Safety 10-11
Community Hospitals Community Nursing Rapid Response MIU Neuro Rehab
Please note: The process for auditing Neuro Rehab and Minor Injury Units (MIU) changed during the year so comparable scoring is not available for all domains
8
Surveys and Audits
To enable prioritisation when developing the clinical audit programme, WHCH considers any national and local priority topics, as well as areas of concern and/ or risk. The following table categorises audits by priority area.
Audit/survey priority.
Total
NICE
4
General Audit
3
Clinical Practice
Guidelines
Development of
Guidelines
Clinical Gov/risk
3 1 7
CQC
2
Local
Protocols / guidelines
11
Actions identified and taken as a result of the local audits and surveys highlighted in the above table include the following:
• Medicines policy modified in line with NICE guidance CG76
• Family needs assessment tool in place and staff trained in its use.
• School nurses offering to take part in school assemblies to provide education about Chlamydia
• Improved use of the Newborn Hearing Screening equipment by retraining and reassessment
• Staff to record NHS number on the Child Health Record
• Tissue Viability nurses developed a new wound formulary
• Access time for first appointments to children services improved
• Provision of personalised care plan and hand held record for heart failure patients
• Heart failure protocol to be updated, rewritten and implemented.
• Single assessment form for the Podiatry services.
9
2.3 Research
The number of participants receiving NHS services provided or sub-contracted by West Kent
Community Health in 2010 / 2011 that were recruited during that period to participate in research approved by a research ethics committee was 30.
Participation in clinical research demonstrates West Kent Community Health’s commitment to improving the quality of care we offer and to making our contribution to wider health improvement.
Our clinical staff stay abreast of the latest possible treatment possibilities and active participation in research leads to successful patient outcomes.
West Kent Community Health was involved in conducting ten clinical research studies in various clinical areas during 2010 / 2011. The improvement in patient health outcomes in West Kent
Community Health NHS Trust demonstrates that a commitment to clinical research leads to better treatments for patients.
There were three clinical staff participating in research approved by a research ethics committee at
West Kent Community Health during 2010 / 2011. These staff participated in research covering three specialities.
As well, in the last three years, three final report publications have resulted from our involvement in NIHR research, which shows our commitment to transparency and desire to improve patient outcomes and experience across the NHS. Our engagement with clinical research also demonstrates
West Kent Community Health’s commitment to testing and offering the latest medical treatments and techniques.
2.4 Goals agreed with Commissioners
Use of the Commissioning for Quality and Innovation (CQUIN) payment framework
A proportion of West Kent Community Health’s income in 2010 / 2011 was conditional on achieving quality improvement and innovation goals agreed between West Kent PCT and any person or body they entered into a contract, agreement or arrangement with for the provision of NHS services, through the CQUIN payment framework. The CQUINs have been linked to the three domains of quality; patient safety, clinical effectiveness and patient experience.
CQUINs agreed with commissioners and the level of achievement for each is as follows:
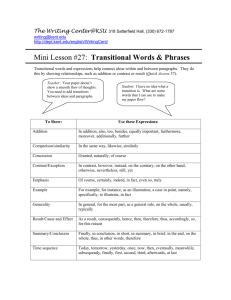
CQUIN 1a
Indicator: To improve patient safety and ensure high quality nursing care through improvements in the Essence of Care audits (see section 2.2.2).
Quality Domain: Safety and Patient Experience
Goal: 5% improvement across 75% of the 10 domains. Minimum achievement of 80% per service.
Achievement: The following graph shows 8 out of 10 domains improved, 6 of which by more than
5%. Just one service in one month (May) failed to achieve 80%.
10
Essence of Care
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
Foo d a nd
drin k
Bla dde
Re r an d b cord ow
Ke epin g el c are
Per son
Pre al a nd o ssu re U
Self
Ca re ral h lce rs ygie ne
Re spe ct
Ca re E nvir onm
He alth
Saf
an ent d w ety ellb ein g
2009/10
2010/11
CQUIN 1b
Indicator: Essence of Care record-keeping audit.
Quality Domain: Safety and Experience
Goal
Improvement to 90%
No service to be below 85%
Achievement
1 service below 85% (82%)
11
CQUIN 2a
Indicator: Mixed and/or venous leg ulcer healing rates within community settings.
Quality Domain: Safety
Goal: 5% improvement (ie to 24.81%) in healing rates by April 2011
Achievement: The following graph shows an actual improvement in healing rate of 28.81% (target indicated by red line).
35.00%
30.00%
25.00%
20.00%
15.00%
10.00%
5.00%
0.00%
23.63%
Leg ulcer healing rate
28.81%
Percentage achieved
Quarter 2 Quarter 4
CQUIN 2b
Indicator: Adherence to West Kent’s dressings formulary.
Quality Domain: Safety
Goal: 90% adherence to dressing’s formulary by April 2011
Achievement: The red line on the graph shows target achieved
92%
90%
70%
50%
30%
10%
Quarter 2
94.50%
Quarter 4
Percentage on formulary
12
CQUIN 3a
Indicator: Percentage of patients receiving all relevant community stroke indicator interventions.
Quality Domain: Clinical Effectiveness
Goal: 60% of new stroke patients having full compliance with all 9 stroke quality indicators.
Achievement: This indicator has been an area of focussed development over the last year.
CQUIN 3b
Indicator: Reduction in community therapy waiting times.
Quality Domain: Clinical Effectiveness
Goal: Reduce by 20% by end of March 2011.
Achievement: There is currently variable performance against this target. This has been an area of focussed development over the last year.
CQUIN 4a
Indicator: Number of first time mother contacts within 28 days of delivery.
Quality Domain: Clinical Effectiveness
Goal: 100% first time mothers contacted within 28 days of delivery from July 2010
Achievement: Red line on graph below shows target achieved.
100%
100%
Percentage of new mothers accounted for
100% 100% 100% 100% 100% 100% 100% 100%
95%
90%
85%
80%
86%
88%
75%
Ma y
Jun e
Jul y
Au gus t
Se pte mb er
Oc tob er
No vem be r
De cem be r
Jan ua ry
Fe bru ary
Ma rch
13
CQUIN 4b
Indicator: Percentage of new birth contacts taking place within 10-14 days
Quality Domain: Clinical effectiveness
Goal: 40% by April 2011
Achievement: Red line on graph below shows target achieved.
90.00%
80.00%
70.00%
60.00%
50.00%
40.00%
30.00%
20.00%
10.00%
0.00%
Ma y
Ju ne
Ju ly
Au gu st
Se pte mb er
Oc tob er
No ve mb er
De ce mb er
Ja nu ar y
Fe br ua ry
Ma rch
Percentage of new birth contacts taking place within 10 - 14 days
CQUIN 5a
Indicator: Percentage of basic wheelchairs triaged within 5 days from receipt of referral.
Quality Domain: Clinical Effectiveness and Patient Experience.
Goal: 95% of basic wheelchairs triaged within 5 days from receipt of referral by April 2010 This indicator was finalised with Commissioners in December 2010.
Achievement: The red line on the graph shows target achieved.
100.00%
90.00%
80.00%
70.00%
60.00%
50.00%
40.00%
30.00%
20.00%
10.00%
95.60%
97.60%
Percentage of w heelchairs triaged 5 days from receipt of referral
Quarter 3 Quarter 4
14
CQUIN 5b
Indicator: Average waiting time for three streams of wheelchair.
Quality Domain: Clinical Effectiveness and Patient Experience.
Goal: Trajectory not confirmed by Commissioners.
Achievement: This has been an area of focussed development over the last year.
CQUIN 6a
Indicator: Patient experience survey responses to question about involvement in care.
Quality Domain: Patient Experience.
Goal: To improve ‘yes definitely’ score to at least 89% by April 2011.
Achievement: The following graph shows an improvement of over 5% (83% to 88.1%). Less than
1% below target.
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
Percentage of patients giving response of yes definitely felt involved in decisions about their care
88.10%
83%
Quarter 1&2 Quarter 3&4
CQUIN 6b
Indicator: Composite score for responses to two survey questions focused on privacy and dignity.
Quality Domain: Patient Experience.
Goal: Maintain always score at 95.5%, with no drop below 91% at April 2011
Achievement: The following graph (over the page) shows an improvement of over 2% (93% to
95.27%). Less than 0.25% below target (95.5%)
15
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
Composite score for 2 survey questions focussed on privacy and dignity
Quarter 1 &2 Quarter 3&4
CQUIN 6c
Indicator: Implementation of wider community patient experience survey.
Quality Domain: Patient Experience.
Goal: Extend survey and respond to patient feedback.
Achievement: Patient experience survey has been extended to include all community services and made as a result of feedback (see section 3.3).
CQUIN 7
Indicator: Number of referrals to smoking cessation service.
Quality Domain: Clinical Effectiveness.
Goal: 580 referrals by April 2011.
Achievement: Red line on graph below shows target achieved.
Graph to show accumulation of monthly referrals to stop smoking service
700
600
500
400
300
200
100
0
Ju ne
Ju ly
Au gu st
Se pte mb er
Oc tob er
No ve mb er
De ce mb er
Ja nu ary
Fe bru ary
Ma rch
Number of referrals
16
CQUIN 8a
Indicator: Engagement in delivery of Diabetes strategy .
Quality Domain: Clinical Effectiveness.
Goal
West Kent Community Health involvement in
West Kent Diabetes Clinical Advisory Group and
Diabetes Network Board to support delivery of
Diabetes strategy
Achievement
CQUIN 8b
Indicator: Percentage of eligible staff trained in Diabetes awareness and care.
Quality Domain: Clinical Effectiveness.
Goal
Diabetes awareness: 10% eligible staff to attend face to face training
Achievement
Diabetes Medicines Management: 30% eligible staff to undertake e learning training
CQUIN 9a
Indicator: Percentage eligible staff trained in Dementia awareness and care.
Quality Domain: Clinical Effectiveness.
Goal
10% of eligible staff trained in Dementia awareness and care
Achievement
17
CQUIN 9b
Indicator: Provider commitment to local health economy implementation of the West Kent Dementia
Strategy.
Quality Domain: Clinical Effectiveness.
Goal
West Kent Community Health involvement in
West Kent Dementia Forum meetings to support delivery of Dementia strategy
Achievement
CQUIN 10
Indicator: Enhancing Quality Programme.
Goal: Achieve all programme milestones.
Achievement: Red line on graph below shows target achieved.
Enhancing Quality all milestones met
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
Ap ril
Ma y
Ju ne July
Au gu st
Se pte mb er
Oc tob er
No ve mb er
De ce mb er
Ja nu ary
Fe bru ary
Ma rch
Enhancing Quality Programmeimprove the quality of patient care by delivering the process defined measures and success for heart failure as part of the
EQP (Percentage of process milestones achieved)
18
2.5 What others say about us - Care Quality Commission
West Kent Community Health has put in place a process for monitoring compliance with the Care
Quality Commissions (CQC) registration standards. For this coming year we have developed a new approach to ensure understanding of the outcomes at service level. This will involve compliance support visits to teams and services to ask a series of questions relating to the outcomes and action plans being developed where there are identified learning needs. In addition, there will be observations in care in the same way as the CQC would undertake should they visit the Trust.
West Kent Community Health is required to register with the CQC (as West Kent PCT) and has been registered since 1 April 2010. West Kent Community Health has no conditions placed against its registration status.
The CQC performed the first unannounced inspection of four of West Kent Community Health’s six community hospitals on 7th June 2010 to assess whether West Kent Primary Care Trust is adequately protecting patients, workers and others from healthcare-associated infection. Of the 14 measures inspected, the CQC had no areas for concern about 13 and found areas for improvement in the remaining one.
West Kent Community Health took immediate remedial action following the visit.
In addition, an audit was carried out by South Coast Audit (SCA) in January 2011 to provide assurance of the implementation of actions and the adequacy and effectiveness of those actions taken to address the CQC’s concerns. SCA was able to declare “significant assurance” as a result of their audit. The final report is awaited at the time of writing this report.
(The CQC full inspection report is available on their website www.cqc.org.uk/)
The CQC’s Quality and Risk Profile for the Trust has been provided to the Trust on a monthly basis since October 2010, and the profile is reviewed each month to ensure that any risks identified are addressed.
2.6 Data Quality Statement
Effective delivery of patient care relies on good quality information and is essential if improvements in quality of care are to be made. West Kent Community Health will be taking the following actions to improve data quality.
• Outline our obligations in relation to data quality and raise the profile of the importance of good information to support both clinical and non clinical decision making
• Ensure that the basic principles of data quality are understood and implemented across the Trust
• Improve the Trust’s rating with regard to the Information Maturity Assessment matrix tool developed to support the Transforming Community Services programme
• Encourage service and system leads to introduce and maintain robust change control processes for all key information systems
• Provide guidance for internal data quality audits.
The implementation of a new Community Information System within the Trust during 2011 / 2012 will also have a positive impact on data quality as it will provide a single integrated electronic patient record.
19
NHS Number and General Medical Practice Code Validity
West Kent Community Health did not submit records during 2010 / 2011 to the Secondary Uses service for inclusion in the Hospital Episode Statistics which are included in the latest published data.
Information Governance Toolkit Attainment Levels
West Kent Community Health’s Information Governance Toolkit Assessment score was 67% and rated Green.
Clinical Coding Error Rate
West Kent Community Health was not subject to the Payment by Results clinical coding audit during
2010 / 2011 by the Audit Commission.
20
3.0 Review of Quality Performance
West Kent Community Health made impressive progress in 2010 / 2011 towards providing high quality care, thanks to the excellent work of our staff. We continue to be a high performing community arms length provider and have developed a wide range of initiatives to improve quality of care and patient experience.
In 2010 / 2011 we set 3 key quality objectives:
Priority 1 – Ensuring patient and staff safety
Priority 2 – Ensuring efficient and effective services
Priority 3 – Ensuring a positive patient experience
3.1 Priority 1 – Ensuring patient and staff safety
Central to this priority is Infection Prevention & Control
Training
An annual update in Infection Prevention and Control (IPC) is part of the statutory and mandatory training for all staff.
Commissioning contract IPC staff training requirement
75%
Total number of staff who received IPC training during
2010 / 2011
84%
Total number of staff working in in-patient areas who received
IPC training during 2010 / 2011
(in response to CQC visit)
100%
Clinical Practice
Inpatient areas undertake hand hygiene and dress code compliance (“Bare Below the Elbows”) audits monthly. Any non-compliance with standards is immediately addressed with the relevant member of staff.
Scores for 2010 / 2011 were as follows:
Hand Hygiene Compliance for Inpatient Staff
%
100
95
90
85
80
75
70
65
60
55
50
Ap r-1
0
Ma y-1
0
Ju n-1
0
Ju l-1
0
Au g-1
0
Se p-1
0
Oc t-1
0
No v-1
0
De c-1
0
Ja n-1
1
Fe b-1
1
Ma r-1
1
Percentage staff compliant
21
Dress Code Compliance for Inpatient Staff
%
100
95
90
85
80
75
70
65
60
55
50
Ap r-1
0
Ma y-1
0
Ju n-1
0
Ju l-1
0
Au g-1
0
Se p-1
0
Oc t-1
0
No v-1
0
De c-1
0
Ja n-1
1
Fe b-1
1
Ma r-1
1
Percentage staff compliant
Healthcare Associated Infections
In setting targets for the reduction for Healthcare Associated Infections (HCAIs), the Department of
Health has recognised that these are present in community as well as hospital settings. As such, it has set limits on numbers of infections identified from specimens either sent from community settings, or taken within a defined period after acute hospital admission.
Currently, the only HCAIs required to be investigated in community settings are Methicillin-resistant
Staphylococcus aureus (MRSA) bacteraemias (blood-stream infections) and Clostridium difficile infections (CDI).
MRSA bacteraemia is attributed to community settings if the specimen is taken within the first 48 hours of acute hospital admission (pre 48 hours) or in a community hospital (post 48 hours).
Clostridium difficile Infection (CDI) is attributed to community settings if the specimen is taken in the community or within the first 72 hours of acute hospital admission.
Figures for infections attributable to West Kent Community Health services are only available, for
Community Hospital inpatients.
Number of cases of infection in WKCH Community Hospitals: 2010 / 2011
MRSA bacteraemia NIL (none since December 2008)
Clostridium difficile
Norovirus outbreaks
2 (3 in 2009 / 2010)
3
22
All CDI and MRSA bacteraemia infections acquired in West Kent Community Health community hospitals are subject to internal Root Cause Analysis, as are all outbreaks. The purpose of these investigations is to identify any lessons and take remedial action to reduce the risk of recurrence.
Environment and Cleanliness
As a result of falling cleaning audit scores in some of the community hospitals, additional focus and actions were taken with a view to improving the environment.
The ability to keep the environments clean is exacerbated by old buildings and the requirement for refurbishment of some of the buildings by the landlord.
Improvement in the cleaning audit scores towards the end of the year has been seen due to
implementation of remedial action including:
• investment in additional cleaning staff,
• senior management focus on cleaning audits
• Deep Clean Programme in October and November 2010
• refurbishment building work.
It is interesting to note, however, that 97% of patients who were treated in West Kent Community
Health community hospitals and clinics and surveyed by the patient experience telephone survey stated that the overall level of cleanliness was very good or quite good.
%
100
Average Weighted Cleaning Scores- Community
Hospitals
80
60
40
20
0
Ap r-1
0
Ma y-1
0
Ju n-1
0
Ju l-1
0
Au g-1
0
Se p-1
0
Oc t-1
0
No v-1
0
De c-1
0
Ja n-1
1
Fe b-1
1
Ma r-1
1
Average weighted score Minimum Standard
NB: No audits were undertaken during September and October 2010 due to technology issues.
23
Patient Environment Action Team (PEAT)
PEAT is a national programme of annual assessment of inpatient healthcare sites in England with more than 10 beds
PEAT Inspections were carried out in all six West Kent Community Health community hospitals over
January and February 2011. The site assessments were carried out by representatives from the
Quality and Performance Team of Kent and Medway Shared Services, Non Executive Directors,
Modern Matrons, Cleaning Supervisors and members of the Infection Prevention and Control Team.
The following table shows PEAT scores for 2011 compared with the previous assessment:
Site
Sevenoaks
Hospital
2010
2011
Acceptable
Acceptable
Good
Good
Excellent
Good
Sevenoaks Hospital is still undertaking building works and has been for well over a year now and unfortunately this is having an impact on general cleanliness and environment throughout the unit.
Hawkhurst
Hospital
2010
2011
Acceptable
Good
Good
Excellent
Excellent
Good
86%
96%
Tonbridge
Hospital
Edenbridge
Hospital
Year
2010
2011
2010
2011
Environment
Score
Acceptable
Acceptable
Good
Acceptable
Food Score
Good
Excellent
Good
Excellent
Privacy and
Dignity
Excellent
Excellent
Excellent
Excellent
Aggregated
Cleaning
Score
77%
74%
93%
79%
96%
82%
Livingstone
Hospital
2010
2011
Acceptable
Good
Excellent
Good
Excellent
Good
84%
95%
Food service and protected meal times need to be refined to gain full the full score needed.
Needless marks were lost due to Livingstone not having a private treatment room for the ward patients.
Gravesham
Community
Hospital
2010
2011
Good
Good
Good
Excellent
Excellent
Excellent
87%
91%
Gravesham improved its score in Food service and maintained the same scores as last year for environment and Privacy and Dignity. There were a few issues with the flooring throughout the building and also the alcohol and soap dispensers were dirty underneath.
Scores have fallen since 2010
Scores have stayed the same since 2010
Scores have risen or remain at the top since 2010
24
Additional initiatives and work to improve IPC and prevent avoidable infection include:
• installation of additional hand wash basins
• conversion of open two-bedded bays to isolation rooms
• unannounced infection control visits and commode inspections.
• cleanyourhands campaign (this initiative was fully rolled out prior to its cessation by the
Department of Health)
• Essential Steps for Clean, Safe, Care: This national IPC audit programme has been implemented in all West Kent Community Hospitals, and Minor Injuries Units, with leads expected to submit monthly returns of observations. Roll out continues in Community Nursing Teams.
• Infection Control Audit Programme: a rolling programme of audit for all community inpatient and outpatient services. Inpatient services are subject to yearly audit and outpatient services three-yearly audit.
• Programme of site visits by Executive and Non-executive Directors.
3.2 Priority 2 – Ensuring efficient and effective clinical services
Lean / 6 Sigma methodology in the NHS is nothing new and it underpins the roll out of the Community
‘Productive series’. In West Kent Community Health we decided to build a new “Lean Culture” that would contribute to both improving quality outputs and removing waste.
The main objective is to develop an internal capability of front line staff, to identify; scope and deliver improvement projects of various complexities to help underpin the quality agenda. Through embracing this initiative we have already seen some impressive results, in training over 20 ‘Green Belts’ and
150 ‘Yellow belts’. (Green and Yellow belt refers to various levels of training in the Lean / 6 Sigma methodology).
Throughout the year there have always been over a dozen improvement projects ongoing and the yellow belts are delivering many more local ‘Just Do It’ (mini projects).
Modern Matron Sherrie Ryder: ‘I thought this Lean programme was another Management fad, but I can honestly say it has completely changed the way I look at what I do’
Responding to a three day yellow belt programme a Charge Nurse stated ’20 years of nursing and this is the best programme I have attended’
Hard results are also visible which combined with staff enthusiasm is a powerful combination, when using well established techniques such as cross functional ‘Rapid Improvement Events’; Stakeholder workshops or problem solving teams.
Our Children’s Audiology service was at risk of collapse; we have now quadrupled productivity in 12 months, and are regularly delivering the national standards for this service.
A project completely redesigned how we carry out the Flu immunisation programme, during two weeks in October 2010, we delivered 150% more vaccinations to housebound patients than we did over five months during 2009.
Within the Productive Community Services programme we have launched our showcase wave:
Four teams selected for Showcase Wave:
- Community Neuro-Rehab, Sevenoaks
- Health Visitors, Snodland
- Children’s Therapies, CRC DVH
- Community Nursing, TW2 Tunbridge Wells.
25
3.3 Priority 3 – Ensuring a Positive Patient Experience
Patient experience allows us to assess the quality of our services from the eye of the user. Along with patient safety and clinical outcomes it enables us to know what we are doing right and what we need to do better.
During the past year West Kent Community Health has focused on extending the survey of patients discharged from its community hospitals (as undertaken in previous years) to include patients receiving care from all its services.
To this end, West Kent Community Health undertook a two phase piece of user research. The aim of the qualitative part , phase one, of the project, was to ensure we survey what matters to patients, to determine the best approach to surveying patients in order to elicit the optimum response rate and to understand staff perceptions of what may affect the patient’s experience.
Phase two (quantitative phase) of the project was a rolling programme of telephone interviews of patients; the interview questions having been developed from the information obtained in phase one.
Quarterly evaluations across services form a picture of patient experience and satisfaction within the community services setting. These quarterly evaluations gradually build up long-term evidence of experience and satisfaction.
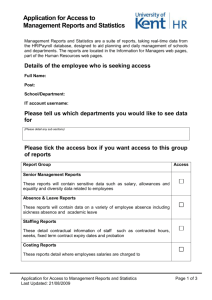
The table below shows overall satisfaction with treatment / care received by service (services all grouped into 12 categories). The overall satisfaction rate is 93%.
13% 13%
13%
10% 10%
18%
17% 20%
29%
20% 27%
40%
75%
97%
87% 87% 84% 83% 83%
72% 70% 68%
60% 57%
53%
TO
TA
L
MI
U
Co mm
N urs ing
He alt h V isit ors
Po dia try
Ne wb orn
H ea rin g
OP
Ph ys io
Wh ee lch air
Se rvi ce s
Co mm
P ae ds
Co mm
H os pit als
Very satisfied Quite satisfied
AM
PS
Ne uro
R eh ab
Ch ild ren
's
Th rap ies
During 2010 / 2011 over 700 patients will have been telephone surveyed with an even spread across the 12 service groups.
NB: At the time of writing the report end of year data was not available.
26
In addition, individual service focused surveys are undertaken (see section 2.2.2). This enables services to gain more specific and detailed feedback from patients, for example, in response to service redesign.
Examples of changes made as a result of patient feedback include:-
Service
Community Nursing
Issue
Patients requesting times that nurses will visit
Change/Action
Morning and afternoon time slots now provided to patients
Advanced Musculoskeletal
Physiotherapy Service (AMPS)
Patient expectations regarding referral for diagnostics do not always match clinical need
Revision of service information leaflets to explain appropriate referrals
Newborn Hearing Screening
Programme
Neurological Rehabilitation
Podiatry
Some patients were not given appropriate information
Need to improve communication within team
Appointment booking processes
Weekly quality check by Senior
Screener to ensure appropriate information is being given
Weekly business meeting commenced on the Unit and in each of the 3 Community
Neurological Rehabilitation
Teams.
Project underway to review and streamline booking processes.
Children’s Therapies Patients dissatisfaction with time they had to wait from initial referral to commencement of treatment
Robust access policy to meet
18 week target
27
3.4 Complaints
Complaints Policy
Our complaints policy adheres to the national regulations, guidance and principles contained within the following documents:
• Local Authority Social Services and National Health Service Complaints (England) Regulations
2009 Statutory Instrument 309
• The NHS Constitution
• The Health Service Ombudsmen Publications:
- Principles of Good Complaint Handling
- Principles of Good Administration
- Principles for Remedy.
Our Commitment to Complaints Handling
When complaints are made, we commit to:
• Inviting the complainant to have a say in how the case is handled and how things will be put right
• Providing an honest and open response to all the concerns raised
• Providing a through and detailed explanation about the events which led to the complaint
• Providing an apology where something has gone wrong
• Informing the complainant what we doing to learn from the experience, together with an assurance that other patients will have a better outcome as a result
• Where possible, provide or contract to provide care or treatment to reinstate the patient to the condition they would have been if the error had not been made
• Consider making a financial contribution to the complainant if they have suffered financial loss as a direct consequence.
Joint Investigations
NHS and Social Care Organisations in Kent, including West Kent Community Health, have signed up to a joint working protocol. Its aim, with the understanding and acceptance of the patient or client, is to undertake joint investigations where necessary, provide a single joint response from all agencies involved in providing the care, share outcomes and disseminate good practice where appropriate.
Themes and Trends in Complaints
Trends and patterns of concern in complaints, which may indicate problems in the delivery or quality of services, are reported to governance groups, and ultimately the Board.
In addition, trends and themes in complaints are analysed alongside trends and themes in incidents and activity within each service to identify ‘hot spots’ on a monthly basis which reviews and scrutinises the responses and subsequent actions.
A total of 97 complaints were received during the year 1 April 2010 to 31 March 2011.
28
The top five complaint areas related to:
• Treatment (40 or 41% of complaints received). These complaints relate to lack of treatment, errors in treatment or complaints where the treatment is questioned.
• Communication (18 or 19% of complaints received). These complaints relate to breakdowns in communication with patients, relatives or between professional teams, difficulties in making contact with services, or inappropriateness of communication.
• Lack of Services (13 or 13% of complaints received). These complaints relate to access to services or changes to the eligibility criteria of services.
• Staff Attitude (7 or 7% of complaints received). These complaints relate to rudeness or disinterest shown by staff.
• Waiting Times (6 or 6% of complaints received). These complaints relate to the length of time it can take to access services.
Performance in complaints handling
The table below shows the number of cases closed during the period 1 April 2010 to 31 March 2011, and the number of complaints that were responded to within the timescales set out in the Complaints
Policy.
No of cases closed
No of cases responded to within agreed timescale
No of cases which did not meet agreed timescale for reply
All complaints closed between 1 April 2010 and
31 March
93 (4 received on 31 March
2011 are still ongoing)
97
0
29
4.0 Statements From Local Involvement Network,
HOSC and PCT
30
31
32
Your LINk for improving health and social care
Your future local HealthWatch
2 June 2011
Kent LINk Commentary on West Kent
Community Health Quality Account
The Kent LINk would like to thank West Kent Community Health (WKCH) for the opportunity to comment on their Quality Account prior to publication. We have worked with Canterbury Christ
Church University, developing a process for commenting on Quality Accounts and have used a variety of methods to collect data regarding the quality of services at Community Hospitals, including patient experience questionnaires. Kent LINk Project Development Workers also engaged with patients in Community Hospitals about the Trust’s priorities for 2011 / 2012.
The LINk focused on the three aspects of ‘quality’ described within the Quality Account and outlined below. LINk participants were also asked to comment on the presentation and layout of the Account. This commentary is based on the responses received by the LINk in relation to the following:
1. Patient Safety
2. Clinical Effectiveness / Effectiveness of Care
3. Patient Experience.
4. Quality Account Presentation and Layout
5. Priorities laid out in the Quality Account.
1. Patient Safety
The LINk received no concerns about safety and those surveyed indicated that safety should continue to be a high priority. We received feedback from participants relating to difficulties in identifying information about patient safety throughout the account. The LINk suggests that this information be grouped together to aid public understanding. The diagrams in Section 2 of the account were difficult to interpret and the explanations provided were not suitable for nonhealth professionals.
KMN, Unit 24 Folkestone Enterprise Centre,
Shearway Road, Folkestone, Kent, CT19 4RH
Tel: 01303 297050
E-mail: info@kentlink.org
Page 1 of 3
Office Hours: Monday – Friday 8.30am - 4.00pm (Answerphone available out of office hours)
The LINk was pleased to note that WKCH had good standards of staff hand hygiene and dress code compliance. We were also satisfied that the staff Infection Prevention and Control training target had been exceeded in the year 2010 / 2011. Whilst there had been low levels of
Clostridium Difficile infection and Norovirus outbreaks, we would encourage WKCH to maintain standards of hygiene to maintain the current low ra tes.
The levels of cleanliness recorded in Section 3.1 are commendable, and WKCH clearly has many initiatives raising levels of cleanliness and improving infection rates. The LINk would like further explanation on Patient Environment Action Team (PEAT) assessments, and details of assessments to help public understanding. It would also recommend that patients and carers are involved in these assessments. The LINk recommends that a description of measures showing improvement standards that have been recorded as falling from the previous year be included within the section.
2. Clinical Effectiveness / Effectiveness of Care
Participants agreed that WKCH should place high priority on clinical effectiveness and the measurement of quality improvement in services. However, those interviewed struggled to interpret the actions assigned to this priority, and a glossary would benefit public understanding. Section 3.2 within the Account would benefit from clearer explanations of terms such as ‘Lean / 6 Sigma’ and ‘Green Belts’. WKCH should be commended for the improvements made to Children’s Audiology services and also the success of the Flu immunisation programme.
Explanations relating to the CQUIN achievements in Section 2 were difficult to comprehend, and the LINk would suggest that WKCH looks at alternative ways of displaying these results.
3. Patient Experience
The Trust has demonstrated clearly in the Account the extent to which they engage with patients to gather feedback on quality of experience. Section 3.3 demonstrates that WKCH is engaging with patients receiving care from all of its services, and the results demonstrate a high patient satisfaction. WKCH has demonstrated that complaints were responded to within agreed timescales, but the figures provided would be more meaningful if statistics relating to numbers of patients treated in 2010 / 2011 were provided.
The LINk hopes that WKCH continues to involve patients and carers throughout 2011 / 2012.
The Kent LINk, as it becomes Local HealthWatch, looks forward to maintaining existing professional relationships at Board and other levels with the new Kent Community Health NHS
Trust.
Page 2 of 3
33
4. Quality Account Presentation and Layout
The feedback we received regarding the presentation and layout was mixed. The document length was considered reasonable, but it was noted that it contained many graphs and diagrams without adequate plain English explanations. In particular, section 2.4 was considered to be unapproachable and irrelevant to the public. Some indication of context is needed for many of the graphs, and in general throughout the Account. Therefore it would be beneficial if at the beginning the Account demonstrated the types of services provided by
WKCH and the number of patients seen in 2010 / 2011. Without these details, the Account is not accessible to the public and has little relevance for the average reader.
A glossary would benefit the Quality Account and less jargon and professional terminology would aid public understanding. The LINk also received feedback that the Account was not accessible to the public and that it contains no clear indication of where WKCH sits within the local structure or its geographical area. A map of the area covered by WKCH would help the public understand the context of WKCH. There were noticeable amounts of spelling errors and the LINk hopes that these are remedied before publication. The LINk would find more detail relating to Care of the Elderly and End of Life Care to be of benefit in next year’s Account.
5. Priorities laid out in the Quality accounts
The LINk carried out one to one interviews at Community Hospitals with patients about the three quality goals and associated pledges. Patients agreed with the priorities for Patient
Safety, Effectiveness and Patient Experience without exception. The LINk were pleased that priorities and their actions were set out clearly. We received comments that the priorities actions contained ‘jargon’ and further description would improve public understanding. WKCH have clearly addressed the priorities for the year 2010 / 2011 and information on progress of these priorities was easy to find within the document. However, it is noted that there are several places within the Account where data or audit reports are not available. This undermines the indication that progress has been made on key objectives.
The LINk would like to commend West Kent Community Health for its progress over the past year and looks forward to working with them as Kent Community Health NHS Trust.
--- End ---
Page 3 of 3
As mentioned in the LINks commentary, not all of the end of year data was available at the time the draft report was sent to them. However, this final version now has it all included.
34
35
36
Quality Report Production
The Trust welcomes any comment and asks you to shape next year’s quality report by sharing your views and contacting the Communication and Engagement Team:
Telephone: 01233 667812
Email: commsteam@kentcht.nhs.uk
Address: Trinity House, 110-120 Upper Pemberton, Eureka Park, Ashford, Kent, TN25 4AZ
Quality Report Availability
The Quality Report is available in Braille, large print, audio tape, CD and translated into foreign language. To request one of these version please telephone 01233 667812
Or download a copy from the Trust website www.kentcht.nhs.uk