2010 / 2011 Quality Account Improving patient experiences
advertisement

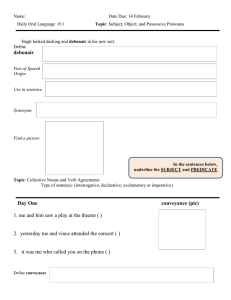
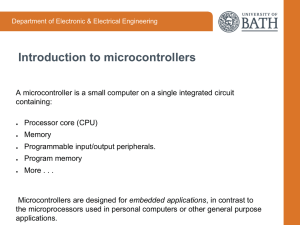
2010 / 2011 Quality Account Improving patient experiences Contents Introduction Partnerships in Care – Who are we? Section 1 Statements from PiC Group Chief Executive and Group Medical Director/Director of Nursing Section 2 Priorities for improvement – Looking forward 2011 / 2012 Section 3 Progress against 2010 / 2011 priorities: 1. Further improve the patient experience 2. Further develop a culture of risk management across PiC 3. Continue to improve clinical outcomes for patients 4. Deliver the Recovery Model in all PiC hospitals 5. Continue to improve on overall quality, whilst reducing rather than increasing costs where possible 6. Continue to review patterns of demand and, where necessary, adjust clinical offerings 7. Continue to develop information management and technology systems Who was involved? 2 Introduction Partnerships in Care – Who are we? Partnerships in Care (PiC) is the largest independent provider of secure mental health facilities across the UK. We have 25 years of experience in caring for men and women with complex mental health needs. Our services focus on the care and treatment of people with mental illness, personality disorder, learning disability and brain injury. We have more than 1,200 beds in 23 facilities, within which our multidisciplinary teams provide assessment, treatment and rehabilitation for patients in low and medium security and specialised rehabilitation units. Our services focus on the care and treatment of people with mental illness, personality disorder, learning disability and brain injury Through the delivery of integrated care pathways, we are able to consistently achieve our aim of meeting the patient’s needs, in the least restrictive conditions and as close as possible to the patient’s home. London & South East Eastern North East 0■ Partnerships in Care Head Office Borehamwood Hertfordshire 06 Burston House Diss, Norfolk/Suffolk 17 Stockton Hall Stockton-on-the-Forest, York 07 St John’s House Diss, Norfolk/Suffolk North West 01 Kneesworth House Royston, Cambridgeshire 08 Lombard House and Richmond House Harleston, Norfolk/Suffolk 02 The North London Clinic Edmonton, London 03 Suttons Manor Romford, Essex 04 The Dene Hassocks, West Sussex 05 Pelham Woods Dorking, Surrey 09 Oaktree Manor Tendring, Essex 10 Brain Injury Services Essex Colchester, Essex Midlands 11 Abbey House, Malvern Wells, Worcestershire 12 Hazelwood House Chesterfield, Derbyshire 13 The Willows Newark, Nottinghamshire 14 Annesley House Annesley, Nottinghamshire 15 Calverton Hill Arnold, Nottinghamshire PiC facilities Head Office 16 Brain Injury Services Northamptonshire Grafton Regis, Northampton 18 Kemple View Blackburn, Lancashire 19 Arbury Court Warrington, Cheshire 23 20 The Spinney Atherton, Manchester Wales 21 Llanarth Court Abergavenny, Monmouthshire 18 20 19 22 Aderyn Nr Pontypool, Monmouthshire 17 12 13 15 14 Scotland 23 The Ayr Clinic Ayr, Ayrshire 21 22 11 16 7 1 2 3 10 8 6 9 5 4 3 Section 1 Statements from PiC Group Chief Executive and Group Medical Director/ Director of Nursing In this section… …we take a look at statements from the Group Chief Executive, the Group Medical Director and the Director of Nursing 4 Section 1 Statement from Group Chief Executive It gives me great pleasure to present the 2010 / 2011 Quality Account for Partnerships in Care (PiC). Our second Quality Account report reflects our own internal quality standards and the expectations that our patients, carers, commissioners and regulators have of our services. In putting together this report, we have sought feedback and input from patients and staff across all our hospitals and other stakeholders. I would like to take this opportunity to thank our Corporate Director of Nursing, Group Medical Director, Clinical Governance Commitee, information and communication teams for pulling all the material together for this report in such a clear and concise way. The vast majority of PiC services are commissioned exclusively by the NHS – either by individual PCTs or through specialised commissioning groups on behalf of their host PCTs. We believe the needs of patients can be more safely and efficiently met where there is a seamless relationship between independent and NHS providers. These are times for collaboration and cooperation, and it remains the ambition of PiC to become fully integrated into the developing provider landscape. In a year in which we have fully adapted our reporting requirements to meet the needs of the NHS standard contract, I am proud that we have achieved all our CQUIN targets In a year in which we have fully adapted our reporting requirements to meet the needs of the NHS standard contract, I am proud that we have achieved all our CQUIN targets. The delivery of secure psychiatry is a very complex endeavour – the achievement of CQUIN goes far beyond a modest financial adjustment and reflects the capacity of our staff to deliver a consistently high quality service to an occasionally challenging and often unpredictable patient group. PiC will only remain at the forefront of secure psychiatric treatment through sustained and honest evaluation of all aspects of our work and, where necessary, we must promptly respond to any identified shortfalls. Like many organisations we have on occasion had concerns with regard to staff sickness and the monitoring of sickness levels across the organisation. We have successfully introduced the third party management of staff sickness reporting and occupational health. Across all our hospitals staff sickness was a very commendable annualised mean of 2.65% for 2010. Improved monitoring of and responding to staff sickness has allowed us to further reduce our use of agency staff to an annualised mean of 0.99%. This very low usage of agency staff has clear benefits for continuity of service and direct patient care. In a time of tumultuous change in healthcare, PiC has responded positively to the new Health and Social Care Bill. Through our own offices and those of the Independent Mental Health Services Alliance (IMHSA), we have contributed extensively to the consultation exercises encouraged by the Health White Paper. We hope that the Act when it receives Royal Assent will reflect those contributions. We know that a ‘liberated NHS’ that fully engages with the independent sector can produce all the outcomes to which the NHS rightly aspires. This Quality Account for Partnerships in Care is testimony to our ability to learn and develop alongside our NHS colleagues. We look forward to reporting the continued development of our services in 2012. Fred Sinclair-Brown Group Chief Executive 5 Section 1 Statement from Group Medical Director and Corporate Director of Nursing We believe that our patients and their families deserve the highest quality care possible. This is essential from a business and clinical governance perspective. While the definition of quality can be hard to pin down, we know intuitively that quality is fundamentally about ensuring that those who use our services receive care and treatment appropriate to their needs. A good service is one that goes above and beyond doing things right. We would wish our care to be at a standard that we would expect for ourselves or our relatives A good service is one that goes above and beyond doing things right. We would wish our care to be at a standard that we would expect for ourselves or our relatives. It is important that the management of PiC is coordinated in a way that focuses on overall quality improvement and the effective functioning of the underpinning operational systems. Quality requires a strategy, which describes clearly the context and outlines in detail the priorities for the Company. These priorities provide the framework for the production of the Quality Account. Quality also requires an assurance framework, which ensures that services are delivered to agreed standards. Policy, procedure, clinical guidelines and care pathways define the relevant standards. There are two key drivers in place to ensure these standards are applied in practice. These are: • Quality monitoring • Review of service areas Quality monitoring involves capturing, compiling and analysing data on quality and where possible benchmarking against local and national standards. This requires regular systematic reviews and independent inspections of the services. Finally, practice improvement is necessary in the management of quality and involves activities to ensure services meet standards and constantly improve. This involves an area working to develop practice based on feedback regarding their performance as part of the Quality Improvement philosophy. At PiC we strive to continually improve the quality of all aspects of service throughout the organisation. The PiC Clinical Governance Committee is the key body responsible for driving quality improvements across all our hospitals and their strategy is informed where appropriate by emerging national policy initiatives, our internal arrangements for ensuring regulatory compliance as well as Quality Account priorities. This committee also ensures the alignment of our performance with the Commissioning for Quality and Innovation (CQUIN) standards and payment framework. All PiC hospitals endeavour to continuously improve the patient experience through their clinical governance systems, patient forums, ward planning and development teams, quality improvement initiatives and commitments to ever more patient involvement within all aspects of the individual service. We are proud to be leading the quality and clinical strategy for PiC and will endeavour to ensure that in 2011/12 and beyond, standards are maintained and enhanced wherever possible. John Taylor Group Medical Director (up to June 2011) Doreen McCollin Corporate Director of Nursing 6 Section 1 Quality Account Statement from Group Medical Director (from June 2011) I am delighted to endorse the Partnerships in Care (PiC) 2010 / 2011 Quality Account. The information in this report is based on extensive quantitative data and there is a strong commitment to expand our evidence base to include a move towards more comprehensive levels of clinical outcome reporting from our hospitals. This report sets out evidence that the organisation is well governed and that patients are provided with safe services that are effective and associated with a positive experience. There are high levels of compliance with CQC regulations across the organisation and our services are committed to regular peer review benchmarking through the Royal College of Psychiatrists Quality Network for Forensic Mental Health Services. I look forward to supporting the objectives for the year ahead to ensure that PiC consistently provides a high quality recovery-focused service that maximises the potential of patients and our workforce. Dr Quazi Haque Group Medical Director (from June 2011) I look forward to supporting the objectives for the year ahead to ensure that PiC consistently provides a high quality recovery-focused service that maximises the potential of patients and our workforce 7 Section 1 PiC registration under the Health and Social Care Act 2008 PiC was required to register its services in England with the CQC under the Health and Social Care Act 2008 from 1 October 2010. PiC developed a provider compliance assessment based on CQC guidance which enables each service to have up-todate information showing compliance against each of the CQC outcomes This required a process of self-assessment against the new regulations and outcomes set out in Essential Standards of Quality and Safety (CQC 2010) prior to submission of an application for registration during a 28 day time slot allocated by the CQC. The process of registration was overseen by the PiC Director of Policy and Regulation, who is the Nominated Individual. Process followed 1. Each service completed a PiC developed Declaration of Compliance, which set out our compliance with each of the new outcomes and any action required to ensure compliance by October 2010 2. The application was made within the allocated time slot in July 2010 3. A Statement of Purpose was completed prior to the October registration date 4. Confirmation of registration of all services without conditions was received in late September and the Certificate of Registration in December 2010 Preparation for the transfer to registration under the Health and Social Care Act 2008 1. All CQC guidance documentation was made available to PiC staff via the internal intranet 2. Patients / residents were briefed on the change in regulation and how this may affect them 3. Staff were briefed on the change in regulation and the implications of this and each ward / house has a copy available of the Summary of Regulations, Outcomes and Judgement Framework 4. The process of reviewing and updating PiC and local policies was commenced On-going monitoring of compliance To monitor the on-going compliance with the new outcomes, PiC developed a format for provider compliance assessment visits where the Nominated Individual or his representative would visit and assess compliance at each hospital on a six-monthly basis and care homes on a monthly basis (but at least once a year by the Nominated Individual). These visits commenced in October and reports are reviewed by the PiC Corporate Management Group and copies sent to the CQC. PiC developed a provider compliance assessment based on CQC guidance which enables each service to have up-to-date information showing compliance against each of the CQC outcomes. This all remains under continual review through feedback on its implementation within PiC and from the CQC. 8 Section 2 Priorities for improvement looking forward 2011/2012 In this section… …we take a look at our priorities for improvement in 2011/2012 9 Section 2 – Priorities for improvement Looking forward 2011/2012 Following consultation with patients, staff and other stakeholders, the Clinical Governance Committee has set the following priorities for 2011/2012 focused in three key areas, patient experience, safety and effectiveness. Patient experience: we aim to 1. ensure all elements of care are patient focused (e.g engagement in the CPA process / further develop patient surveys) – ‘no decision about me without me’ 2. encourage patient involvement through workshops and patient conferences 3. further increase meaningful engagement 4. provide high quality information for patients as well as relatives and carers 5. continue to carry out patient-focused audits as appropriate to encourage the use of the recovery principles and the Recovery Star Safety: we aim to Improve infection control within all patient environments through training and audits 10 1. improve relational security by the utilisation of the DH guide – See, Think, Act 2. improve medicine management processes through audits and training 3. improve infection control within all patient environments through training and audits 4. further develop patient environments through conducting EssenCES surveys and make changes as appropriate in response to the findings Section 2 – Priorities for improvement Effectiveness: our goal is to 1. further develop the Recovery approach and embed the Recovery Star within the CPA process 2. continuously review and improve clinical outcomes 3. continue to work with internal and external stakeholders to further improve the care pathway* 4. improve consistency of clinical processes across the Company 5. improve the standard of record keeping and communication with partners by: a. installing and implementing N3 connection b. enhancing the Electronic Patient Record system Further develop the Recovery approach and embed the Recovery Star within the CPA process * Several PiC hospitals have been selected by commissioners to take part in pilots of the new ‘My Shared Pathway’. We look forward to feeding back on this work. Engagement and feedback PiC considers that meaningful feedback is essential to help us understand our actual rather than aspired to levels of service and quality. The reported and measured experience of patients, staff, relatives and carers, as well as commissioners, is essential to support a sustained programme of improvement. We have sought feedback from staff, patients and external parties on our approach to quality and service development with emphasis on our 2010/11 priorities and we are working to further improve our methods of gaining feedback from all stakeholders (internal and external). A draft of this report was circulated to a representative section of our key customers for their review and feedback prior to publication. 11 Section 3 Our 2010 / 2011 priorities In this section… …we look at our progress against our 2010 / 2011 priorities 12 Section 3 – Our 2010 / 2011 priorities Progress against our objectives In our 2009 / 2010 Quality Account we stated our priorities for further service development. At the end of Q1 of 2010 we reviewed those priorities to produce the following schedule of work for 2010 / 2011: 1. Further improve the patient experience 2. Further develop a culture of risk management across PiC 3. Continue to improve clinical outcomes for patients 4. Deliver the recovery model in all PiC hospitals 5. Continue to improve on overall quality, whilst reducing rather than increasing costs where possible 6. Continue to review patterns of demand and, where necessary, adjust clinical offerings 7. Continue to develop information management and technology systems Patient engagement and involvement activities are considered as integral to priority number 1. This report therefore reports on our progress against these seven priorities. Audits relevant to each priority are mentioned throughout the report. We are very pleased to have met 100% of our Commissioning for Quality and Innovation (CQUIN) targets which focused on the areas of Safety, Innovation, Patient Experience and Effectiveness, set by our commissioners. We are very pleased to have met 100% of our Commissioning for Quality and Innovation (CQUIN) targets 13 Section 3 – Our 2010 / 2011 priorities 1. Further improve the patient experience All PiC hospitals are focused on continually improving the patient experience. This is looked at and reviewed in many different ways including regular patient surveys, evaluated patient involvement and effective complaint handling audits. A patient perspective “I have been a patients’ rep for two years and have achieved many things for the patients. Some of these things are small issues, some bigger, but 90% of the time we get a result” Key achievements • Where appropriate 100% of PiC patients had HCR-20 assessments prior to any leave being granted • 100% of PiC patients were offered a physical examination in this reference period • 100% of patients had been offered a schedule of meaningful activity for 25 hours or more; 93% of patients actually engaged in 25 hours or more of meaningful activity • Four PiC-wide patient surveys were completed and recommendations and action plans progressed • A PiC-wide patient exit interview was initiated in early 2011 Patient involvement and empowerment All PiC hospitals have active patient councils / user involvement groups that engage with local senior management teams and underpin patient empowerment and involvement. Proper consultation and effectiveness at these groups is monitored by the Corporate Director of Nursing. Provider compliance reports are reviewed as part of corporate governance. All PiC hospitals completed schedules of identified service improvements by the end of March 2011. 14 A patient perspective Patients involved in meaningful activity “The Patient’s Council is where lads from all wards come together and talk about their issues about the hospital. I’ve been a rep for six months and it’s been most enjoyable” By the end of March 2011, 100% of eligible patients had a scheduled timetable of activity for 25 hours or more per week and 93% of patients actually undertook 25 hours or more of actual activity. Activities generally fall into one of the following categories (as recommended by the Quality Network for Forensic Mental Health Services): Daily living skills Physical health care OT groups/sessions Psychological therapies Nurse led therapies Education Leave Other groups activities/leisure Work Ward based activities/ Residential services leisure Sports and leisure One-to-one sessions with clinicians Substance misuse therapies Service wide events Activity not attached to a programme Section 3 – Our 2010 / 2011 priorities In 2011 / 2012 we aim to increase the level of engagement in line with patient needs and commissioner expectations. Monitored by the PiC Corporate Management Group, each hospital will be expected to produce an action plan to achieve the necessary increases in activity. That action plan will include: • A weekly audit of activity levels monitored by hospital Senior Management Teams • Evidence of engagement with patients to establish a meaningful choice of activity • A cycle of feedback to patients and staff of activity levels on a monthly basis Patient surveys Across all PiC hospitals we engage in a series of audits that consider the patient experience and create appropriate action plans. As mentioned in our 2009/2010 Quality Account report, during that year we introduced a new ‘PiC-wide’ model for patient surveys to help standardise practice across the group and to generate the first corporate patient audit report. In the period 2010 / 2011 the following surveys have been carried out: i. Figure 1 – “The Ward and Rooms I use”. Graph of one PiC hospital, Arbury Court, which serves as an example, to show key responses from patients on ‘What I think of where I live’ survey. Patient Survey ‘What I think of where I live?’ Agree Strongly Disagree ii. Patient Survey ‘What I think of what I am told?’ Strongly agree Disagree iii. The whole dining experience No response Not sure iv. EssenCES ward atmosphere survey 100 i. Patient Survey ‘What I think of where I live?’ – key findings and recommendations An impressive figure of almost 50% of patients across PiC took part in this survey (research suggests an average response rate of 30% for most similar surveys). Below is a summary of key findings: Response distribution % The 2010 survey ‘What I think of Where I Live’, used a structured questionnaire to obtain and examine information relevant to the quality of living environments experienced by patients across PiC. The inaugural report (Nov 2010) focused on the feedback obtained from the survey and covered services in England, Wales and Scotland. (Figure 1) 80 60 40 20 0 The ward rooms I use 1 2 3 4 5 Questions • Overall the majority of respondents reported satisfaction about the rooms that they use and the general ward environment. The majority were happy with their bedrooms and most of the communal living areas on the wards 1. I am happy with my bedroom 2. I enjoy spending time in the main lounge 3. I like eating in the dining room • Respondents raised concerns in some units over the lack of privacy when making private telephone calls as well as the cleanliness of some shared toilets / bathrooms. • Some patients made a request for increased bedroom access 4. The bathroom and the toilets are always clean 5. The visitors’ room is a nice room 15 Section 3 – Our 2010 / 2011 priorities 1. Further improve the patient experience (cont) Food • Across the group the majority of patients agreed or strongly agreed that they were happy with the food choice available. Some units performed better than others in this domain. Action plans have been developed to improve satisfaction at these sites. It should also be noted that the majority of respondents reported that their personal dietary needs were being met and that they were happy with accessibility to drinks as well as the variety of meals available. Living conditions • The majority of respondents stated that they could approach staff and talk to them about any issue of concern Across the group the majority of patients were satisfied with their general living conditions. The majority of respondents stated that they could approach staff and talk to them about any issue of concern. However some patients found their ward both noisy and stressful. In some hospitals respondents also raised concerns about lack of access to fresh air as well as opportunities to practice their religion. These issues are addressed in individual and hospital action plans. Recommendations 1. To continue with the EssenCES Climate Scale and associated action plans 2. To implement the patient dining experience project 3. To share audit findings and implement action plans with patient groups 4. To discuss noise and associated environment as a standing agenda item for community meetings / patients councils in all wards 5. To submit regular updates on progress within the action plan as a key element of annual clinical governance report for all services The information gathered and action plans developed as a result of this survey are reviewed at a local level by governance committees. ii. Patient Survey ‘What I think of what I am told?’ – key findings and recommendations 44% of patients across PiC participated in this survey. The majority of respondents across the group reported that they were happy with both the quality and content of the information they received about the hospital and the services provided. However, a small number of patients were consistently dissatisfied with the quality and quantity of information that they have received. All services provide information booklets and leaflets to patients on admission and this distribution is recorded in the patient’s clinical record. Hospitals are now reviewing the quality, content and format of information for patients with patient councils, user groups and advocacy services. A common theme in the majority of responses was the paucity of written information describing side effects of commonly prescribed psychiatric medication. 16 Section 3 – Our 2010 / 2011 priorities Recommendations 1. Review all patient satisfaction questionnaires locally (as well as centrally) 2. Review of content of questionnaires by patient councils / user groups 3. Develop PiC information leaflet on ‘How to access the Health Record’ 4. Source best practice medication information leaflets and roll out across PiC iii. Patient survey ‘The whole dining experience’ – key findings and recommendations PiC hospitals aim to meet both the nutritional and social requirements of the dining experience. All PiC hospitals carried out a dining experience survey. Responses from the hospitals were varied, with both positive and negative feedback. Local action plans were developed with patients and led to improvements, such as: • Some extended meal times to prevent patients feeling rushed when dining • Dining tables being laid prior to meal times, which has led to a more relaxed and social atmosphere at meal times Patient councils across PiC will continue to inform practice in relation to the dining experience. iv. EssenCES ward atmosphere survey The Essen Climate Evaluation Schema – EssenCES - is a questionnaire, originally developed for assessing essential traits of the social and therapeutic atmosphere of forensic psychiatric wards. Social climate refers to the interaction of aspects of the material, social, and emotional conditions of an environment, which may – over time – influence the mood, behaviour, and self-concept of the persons in that environment (Schalast, Redies, Collins, and Howells, 2008). The ward atmosphere scale is thought to be linked to treatment outcomes and was developed in Germany by Schalast et al. (2008). As part of our commitment to the Standard NHS Contract for Mental Health Services, we conduct Essen Climate Evaluation Scale (EssenCES) ward atmosphere surveys across all PiC psychiatric hospitals. In conjunction with our patients we have developed innovative action plans that reflect the findings of those surveys. A total of 907 questionnaires were completed and returned, of which 407 (45%) were patients and 500 (55%) were ward based staff All patients and clinical staff across PiC were offered the opportunity to participate in the EssenCES Survey and all completed questionnaires were included in the analysis using the following three subscales: 1. Therapeutic Hold (the extent to which the climate is perceived as supportive of patients’ therapeutic needs); 2. Experienced Safety (the level of perceived tension and threat of aggression and violence) 3. Patients’ Cohesion and Mutual Support (whether mutual support of a kind typically seen as characteristic of therapeutic communities is present). A total of 907 questionnaires were completed and returned, of which 407 (45%) were patients and 500 (55%) were ward based staff. 17 Section 3 – Our 2010 / 2011 priorities 1. Further improve the patient experience (cont) Patients and staff responded to a list of statements, which included: ‘This ward has a homely atmosphere’; ‘The patients care for each other’; ‘Really threatening situations can occur here’; ‘On this ward, patients can openly talk to staff about all their problems’. Figure 2 – Patient Cohesion Patient (%) 17 Staff (%) 7 16 34 36 High Moderate 36 Implementation of EssenCES will enable PiC to: 13 44 Low Very Low • Provide on-going service evaluation and development • Monitor social climate generally and in a timely way to assess the impact of specific service changes • Comply with CQUIN 6 of the NHS Contract Patient Cohesion These findings (Figure 2) reflect that the majority of patients saw patient cohesion as moderate (33%), with 17% as high, 34% low and 16% very low. This equates to a 50% split between moderate and high and low and very low. Figure 3 – Experienced Safety Patient (%) 22 15 29 34 High Forty four percent of staff felt that cohesion was low, with 13% very low, 7% high and 36% moderate equating to >50 feeling that cohesion is low or very low and only 43% believing that cohesion is high and very high. Staff (%) Moderate 12 19 38 31 Low Experienced Safety The findings (Figure 3) reflect that patients across PiC experience the wards as safe with 22% believing safety is high and 34% as moderate giving a combined score of 56% moderate to high, with 15% feeling that safety is very low and 29% saying that safety is low giving a combined total of 44% for low and very low. Very Low With respect to staff, the picture is slightly different with 19% of staff feeling that safety on the wards is very low and 31% saying safety is low, giving a combined 50:50 staff believing that safety is moderate to high and low to very low. Figure 4 – Therapeutic Hold Patient (%) Therapeutic Hold Staff (%) 4 5 18 38 40 High 18 Moderate 57 Low 38 In respect of therapeutic hold, (i.e. climate is perceived supportive for therapeutic need), the findings (Figure 4) reflect 40% of patients believed that therapeutic hold is moderate, and 38% believed that it was high, giving a combined total of 78%. However, 18% said that therapeutic hold was low and 4% said it was very low. With regard to the staff, 57% said that therapeutic hold is very good (high), 38% moderate and 5% saying that it is low and no staff saying that it is very low in this area. Very Low Section 3 – Our 2010 / 2011 priorities Recommendations 1. Feed back results to staff and patients at appropriate meetings 2. Facilitate focus groups for patients on all wards to look at: • Therapeutic hold; patient cohesion; mutual support / experienced safety • What patients think might help improve the ward atmosphere • Patients’ understanding of the questions and how to complete the survey 3. Ensure that ward community meetings happen with: • Appropriate peer support • An ongoing record of issues as they arise and audit trail 4. Encourage more communal events to help foster a community feel on all the wards 5. Feed back lessons learnt to the Corporate Clinical Governance Committee Patient exit interview form PiC has implemented a company-wide Patient exit interview (My stay at PiC – have your say). This interview will elicit a patient’s view of their total experience in a PiC hospital very close to the point of discharge. The format of the survey is very similar to the patient satisfaction survey, with the easy to understand scale and graphics that have been well received by patients (Figure 5). The survey has space for additional comments in free text. The completed interview data will form the basis of a report and action plan. Figure 5 – Simple scale used in patient surveys and patient exit interview forms Strongly Disagree Disagree Not Sure Agree Strongly Agree Patient information leaflets In April 2010, we produced additional patient information leaflets to help patients better understand certain aspects of their care. Patients were involved in the development of leaflets ‘Enhanced Observations – what do they mean for me?’ and ‘Alternatives to Self Injury’. In early 2011, further information leaflets for patients on the themes of ‘Clinical governance’ and ‘Access to health records’ were produced by our in house team and distributed to all hospitals. Complaints In 2010 the number of complaints by occupied bed day decreased by 22% in 2010 (compared to the year prior). (Figure 6) Figure 6 – Complaints 0.15 No. of complaints Complaints audits confirm that generally the complaints resolution process operates effectively and in accordance with company policy and relevant statutory guidance. 0.12 0.09 0.06 0.03 0.00 Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month 2008 2009 2010 19 Section 3 – Our 2010 / 2011 priorities 2. Further develop a culture of risk management across PiC Our clinical risk management strategy provides the overarching quality and clinical governance framework for all patient safety initiatives. The corporate Health and Safety Committee meets on a quarterly basis to discuss and review best practice for risk and safety management within PiC. The Corporate Clinical Governance Manager also sits on this committee to ensure that clinical governance is integrated into the health and safety agenda. Key objectives of this group include: A full and proper understanding of patterns and triggers for accidents and incidents can help develop harm reduction and safety strategies • review of all Corporate Health and Safety Policies to ensure legal compliance and best practice is achieved throughout PiC • review of all incident and accident related data to identify trends and patterns of behaviour, which indicate the need for further investigation or change • review and amendment of the Corporate (Health and Safety) Audit Tool to ensure it reflects the new POSHH standards (Partnership for Occupational Safety and Health in Healthcare) and HSG 65 (HSE-Successful Health and Safety Management) • review and updates to the corporate stress policy and risk assessment tool • review and regular update of health and safety inspection checklists to ensure consistency throughout PiC Accidents and incidents reporting We continue to monitor all accidents and incidents across PiC. A full and proper understanding of patterns and triggers for accidents and incidents can help develop harm reduction and safety strategies. All health and safety reporting should be considered within the context of bed days, approximately 90,000 per quarter. Figure 7 – Trend in incidents per bed over a quarter The accidents and incidents report (Q1 2010-Q1 2011) highlighted several themes, including: (Q2 2010 – Q1 2011) 8.0 Incidents per bed 7.5 7.0 6.5 6.0 Q2/2010 Q3/2010 Q4/2010 Quarter/Year 20 Q1/2011 • The total number of incidents across PiC has decreased over the last three quarters, (Figure 7) • 15 of the units showed an overall decrease in incidents over the last three quarters • Incidents per bed have decreased every quarter for the last year • Physical assault by a patient is the most common cause of staff injury • Patient incidents and injuries have both decreased when compared to the previous quarter • Self-harm remains the most common cause of patient injury Section 3 – Our 2010 / 2011 priorities Serious untoward incidents We report and record serious untoward incidents (SUIs) according to our commissioner’s specific requirements. Currently different commissioners class different incidents as SUIs. All reports are sent to PiC’s Director of Policy and Regulation for comment and to ensure suitable action has (or will) take place. SUI reports are completed each quarter for discussion at the various contract meetings, they are also reviewed by the Corporate Clinical Governance Committee. Each SUI report contains an action plan with recommendations. It is these recommendations that are discussed at the Corporate Clinical Governance Committee and lessons learnt are cascaded across the company. Between April 2010 and March 2011, across all commissioner classifications there were between 3 and 18 incidents each month, with the least number of incidents in December 2010. All reports are sent to PiC’s Director of Policy and Regulation for comment and to ensure suitable action has (or will) take place There were no ‘never events’ during the period of this report. Recommendations • Discussion with the new national commissioning board about standardising the SUI categories to ensure that all commissioners use the same categorisation when requesting information • The Corporate Clinical Governance Committee continues to review all SUIs and ensure that each hospital provides feedback on the actions they take in cascading down the learning from these incidents Medicines management Within PiC there is a comprehensive procedure for the safe administration of medication. The medicines management audit has been revised to reflect the Essential Standards of Quality and Safety (CQC 2010). There is a Service Level Agreement with Lloyds Pharmacy, incorporating a quarterly medication audit, which is subject to annual review. Monthly medicine card audits include proper prescription, signature compliance, Section 62 compliance and use of PRN medication. In addition we carry out annual Consent to Treatment audits. Looking forward we will continue to evaluate all aspects of medication management. 21 Section 3 – Our 2010 / 2011 priorities 2. Further develop a culture of risk management across PiC (cont) Infection control PiC supports the principle that infections should be prevented wherever possible and that effective arrangements for the surveillance, prevention and control of infection are provided throughout the organisation. It is PiC’s policy to encourage the individual responsibility of every member of staff to participate in the prevention and control of infection and to comply with Health and Safety, Control of Substances Hazardous to Health (COSHH) and other legislation and regulations applying to the safe provision of health and social care. PiC has trained all local infection control leads in delivering infection control training and has set up a system for the surveillance and reporting of occurrences of infection PiC takes its responsibility seriously and therefore appointed the Corporate Director of Nursing as the Director of Infection Prevention and Control (DIPC) who takes the lead for infection control across the company. Any adjustments to infection prevention and control arrangements and policy must be approved and assessed by the DIPC. All hospital sites across the organisation have a nominated IPC lead who drives IPC activity within their hospital. All staff have clear responsibilities to support the IPC programme and aims. The Group Chief Executive and Corporate Management Group (CMG) have overall accountability for the provision of high standards of infection prevention and control. Within PiC, infection prevention and control has a key role to play in the clinical governance framework. Over the last year we have developed an annual IPC programme and aim to produce its first full annual report in 2011. PiC has also produced a policy manual and has been working to implement the policies. It has trained all local infection control leads in delivering infection control training and has set up a system for the surveillance and reporting of occurrences of infection. We enhanced the way we carried out audits in the latter part of 2010 and launched three PiC-wide infection control audits focused on hand hygiene, environment, and kitchen areas, where compliance (> 85%) partial compliance (76 – 84%) or minimal compliance (< 75%) were measured (as per the Infection Control Nursing Association (ICNA) standards). Following the audits, the following actions have been developed: 1. Review action plans for non/partial compliant areas 2. Re-audit all areas on an annual basis 3. Continue sharing information across all services through the meetings of the infection control leads 4. Continue infection control training and updates across all sites 22 Section 3 – Our 2010 / 2011 priorities Security within PiC All aspects of proper security contribute greatly to the effective conduct of our secure hospital operations. Security is a broad descriptor that embraces a wide range of activities relating to patients/residents, buildings, property, staff and visitors. With such a diversity of operations and patient groups across PiC’s facilities there are inevitably local variations and requirements in regard to security. Local security policies informed by the corporate security strategies are in place for all units. PiC works with all national guidance and good practice. All MSUs participate in Quality Network for Forensic Mental Health Services peer review system. The Quality Network review system has a significant focus on all aspects of security in medium secure hospitals. Local security policies informed by the corporate security strategies are in place for all units In 2010 / 2011, a number of new security related polices were developed and include: • The Group Security Strategy (GSS) • The Patient Escort Baseline Risk Assessment • The Control and Management of High Risk Items The level of compliance achieved is measured through an audit process using the Group Security baseline document sheets. Audits may be conducted locally by means of mutual support between sites and externally by the Group Security Officer. To date baselines have been created for: • The Physical Security Document (PSD) • The Procedural Security Index Document (PSID) • The Security Committee • Access to secure gardens and courtyards • The MoJ Person Escort Record (PER) • Control and management of high risk items • Escort Baseline Risk Assessment • Security training • Secure management of keys • Site security lead • Shared mailbox and briefings • Search policy All secure sites within the Group were audited against the Group Security Strategy baselines followed by an action plan creation and implementation processes. 23 Section 3 – Our 2010 / 2011 priorities 2. Further develop a culture of risk management across PiC (cont) Additional initiatives in 2010 / 2011 The following initiatives were implemented through the year: • Training packages (Security Awareness; Person Escort Record; First on Scene) • Security briefing system • Security mailbox system • Contingency planning – desk top exercises Following the roll-out of the corporate security awareness training in March 2010, there has been an emphasis across PiC on implementation of the Department of Health (DH) relational security guidelines. Security notice boards, where information on relational security is displayed alongside DH posters, have been installed in all our secure hospitals 24 Security notice boards, where information on relational security is displayed alongside DH posters, have been installed in all our secure hospitals. All staff have access to the DH document Your Guide to Relational Security: See, Think, Act. It is presented during the annual security awareness training and available on each ward. Staff are also directed to the relevant pages of the DH website and have started using the ‘Relational Security Explorer’ in staff meetings, handovers and reflective practice groups. Further security workshops for all staff will take place on a regular basis. Security policies and procedures are under constant review through the Group Security Officer and Director of Policy and Regulation. Section 3 – Our 2010 / 2011 priorities 3. Continue to improve clinical outcomes for patients Figure 8 – HONoS Improvement Summary Report Category PiC constantly strives to maximise performance through focus on measurable outcomes. At the end of 2010 we developed a workstream to specifically focus on outcomes data across PiC. We routinely review and collate our length of stay data to meet our CQUIN requirements. It is now routine practice for all hospitals to give a clear indicative length of stay expectation at initial assessment – this expectation is reviewed at the first care programme approach (CPA) meeting. In discussion with the patient and external stakeholders all patients have an agreed treatment pathway with timelines. 78.90% 72.05% 0 20 40 60 80 100 % Improvement % improvement in secure item score That pathway will indicate treatment interventions, reducing levels of security and probable onward placement. % improvement in 12 item score Clinical teams at all PiC regions work together to help streamline, standardise and ensure a continuous pathway of care for all patient journeys. A patient’s pathway is not determined by us as a provider, nor solely the commissioner – it is a ‘shared pathway’ with a common understanding between all stakeholders, with the patient at the very centre. Figure 9 – HCR-20 Summary Report HONoS 2 In 2010 / 2011, 94% of PiC patients met the criteria for a HONoS Secure assessment and HONoS 12 item score. Of those eligible* 91.7% of patients cooperated sufficiently with the tester to produce valid scores. Figure 8 shows the number of patients (as a percentage) who have showed improvements on their scores (78.9% for HONoS Secure; 72.05% for HONoS 12 item score). 18 *Eligibility for HONoS score is when patients have been at a PiC unit for at least three months; as per the contract requirements, data was collected from Q3 2010). HCR 20 80 In the period 2010 / 2011, 92% patients were eligible for HCR-20, and 80% of patients had a score, and 18% were awaiting assessment (Figure 9). Data was collected from August 2010 as per contract requirements. % of eligible patients with HCR-20 score % of eligible patients under assessment % of eligible patients awaiting assessment 25 Section 3 – Our 2010 / 2011 priorities 3. Continue to improve clinical outcomes for patients (cont) Physical health PiC recognises the importance of providing a holistic care package to patients addressing their physical and mental healthcare needs through individual care planning PiC recognises the importance of providing a holistic care package to patients addressing their physical and mental healthcare needs through individual care planning. All patients have a physical assessment on admission to PiC hospitals and an annual physical. They have access to resources and facilities that support their physical well-being to ensure that their physical healthcare needs are not compromised by their stay within PiC services. Whilst each region has a medical lead who is accountable for the standards of physical healthcare, the actual physical healthcare will be under the direction of a local GP and local protocols are in place to reflect these arrangements. The Responsible Clinician (RC) has the responsibility of ensuring the completion of a full physical examination soon after admission and will liaise with the GP. It is also the RCs responsibility to ensure that patient care planning takes proper account of physical needs and well-being. In the event of a patient refusing any medical treatment, the RC must ensure there is an assessment carried out on the patient’s capacity to consent. The medical leads are responsible for ensuring high standards of physical healthcare within their region and to ensure adherence to PiC’s Physical Healthcare Policy. The medical lead ensures the collation of evidence and liaises with training leads to make sure that all staff involved in physical healthcare attend relevant training programmes. It is the responsibility of the medical lead to disseminate areas of good practice within PiC, encouraging a culture of learning from good practice. During 2010 PiC has prioritised health promotion across its hospitals, with hospitals focusing on subjects such as smoking cessation, diet and nutrition, sexual health and weight management. The Group Medical Director and the Corporate Director of Nursing will monitor the effectiveness of the policy. Smoking cessation Every PiC hospital has an active smoking cessation programme and strategy. Hospitals use a variety of initiatives to help encourage smoking cessation amongst patients, for example, psychological / psychotherapeutic interventions, structural (e.g four smoking breaks per day), pharmacological, health counselling, stop smoking groups, and ‘time to quit’ challenges. One of our particularly successful smoking cessation treatment programmes was at PiC Learning Disability Services which included: 26 • provision of health information to patients in one to one sessions • provision of health information to patients in group sessions • access to health information from primary care for patients • access to nicotine replacement therapies and/or information about the same from primary care for patients • a ‘smoking timetable’ that placed limits on smoking times Section 3 – Our 2010 / 2011 priorities This preliminary audit showed a statistically significant shift in patients’ smoking status. One in three of the patients who were smokers on admission gave up smoking while in the programme, though women smokers appeared less likely than men to give up smoking (Figure 10). Figure 10 – PiC LDS Smoking Cessation audit by gender On admission All PiC hospitals continue to demonstrate an on-going commitment to smoking cessation as part of a holistic approach to physical and psychological care. We will continue to make every effort to encourage and enable smoking cessation amongst our patient groups. We will continue to monitor the efficacy of all current and emerging smoking cessation programmes. CPA Plus – the enhanced CPA process Much effort goes into preparation for the regular CPA reviews. We believe that reporting and planning for a patient’s care pathway is a continual process and should be managed accordingly. The quality of interaction between our team, the commissioner and the local care team can have a major impact on the pace of progress made by the patient along the care pathway. We have enhanced the process of routine feedback through more frequent and regular clinical reporting to the commissioning body. Such reporting is tailored to meet the needs of individual commissioners who may wish to focus on specific cohorts of patients or who wish to receive reports on all their patients but with specific detail on one or two. These reporting details will be formalised through existing contact arrangements. Important decisions, often delayed until the formal review, can now be taken at a timely point on the pathway. The formal CPA should become more of an opportunity to review performance and less a springboard for action. Progress should be more immediate and the result should be visible in greater patient satisfaction and reduced length of stay. PiC takes responsibility for maintaining constant communication with the commissioners at all significant points in the patient journey, not just at CPA reviews. This way issues are identified and important decisions taken in an efficient and effective way that always keep the patient at the centre of planning. Our standardised CPA documentation places greater emphasis on the future, on team and patient objectives and on how they will be achieved and by whom. This includes informed recommendations on anticipated length of stay and ongoing care pathway options. 100 Non smoker 80 36% Smoker 46% 60 40 64% 54% 20 0 Male Female At present 100 Non smoker Smoker 80 50% 62% 60 40 50% 20 38% 0 Male Female 27 Section 3 – Our 2010 / 2011 priorities 4. Deliver the recovery model in all PiC hospitals By the end of Quarter 1 2011 all PiC psychiatric hospitals were working within a clinical philosophy of recovery. At the end of Quarter 1 2011, 100% of patients were offered the opportunity to formally engage in the Recovery Approach. Recovery is “a way of living a satisfying, hopeful and contributing life even with limitations caused by illness” (Anthony, 1993), and is an influential idea in mental health policy internationally. This understanding of recovery has emerged from people who have personal experience of recovery in, with and from mental illness. The Recovery Model as it applies to mental health is an approach to mental disorder that emphasises and supports each individual’s potential for recovery The Recovery Model as it applies to mental health is an approach to mental disorder that emphasises and supports each individual’s potential for recovery. It must be emphasised that each individual’s journey to recovery is a deeply personal process. Recovery is seen within the model as a personal journey that may involve developing hope, a secure base and a sense of self, supportive relationships, empowerment, social inclusion, coping skills and meaning. The Recovery Model has now been explicitly adopted as the guiding principle of the mental health systems and has been incorporated into the NHS contract compliance tool by commissioners through utilisation of the Recovery Star, which is a tool for supporting and measuring change when working with adults of working age who are accessing mental health services. As an outcomes measurement tool it enables organisations to measure and summarise progress. The stated elements of recovery are: Hope Finding and nurturing hope has been described as a key to recovery. It is said to include not just optimism but a sustainable belief in oneself and a willingness to persevere through uncertainty and setbacks. Secure base Appropriate housing, a sufficient income, freedom from violence, and adequate access to health care has also been proposed. Self Recovery of a durable sense of self (if it had been lost or taken away) has been proposed as an important element. Supportive relationships A common aspect of recovery is said to be the presence of others who believe in the person’s potential to recover, and who stand by them. While mental health professionals can offer a particular limited kind of relationship and help foster hope, relationships with friends, family and the community are said to often be of wider and longer-term importance. Empowerment and inclusion Empowerment and self-determination are said to be important to recovery, including having self-control. 28 Section 3 – Our 2010 / 2011 priorities Coping strategies The development of personal coping strategies (including self-management or self-help) is said to be an important element. Figure 11 – Recovery Star Summary Report – PiC medium and low secure services Meaning 15 Developing a sense of meaning and overall purpose is said to be important for sustaining the recovery process. This may involve recovering or developing a social or work role. “The Recovery Star lets you say where you think you are on the Recovery Star chart. It is elements of your life where you get to say were you think you are and get to see where you need to progress in order to achieve a higher scoring. The point of this is to monitor your progress month to month. The Recovery Star points out your strengths and weaknesses, so although you may be strong and score high on one thing you might discover you’re not so strong on something else and therefore need to work on that to progress. It’s all about helping you discover in what area of your life you need help.” 22 63 Patient quote Engagement with Recovery Star % of patients engaging in their Recovery Star We have audited the impact of the Recovery Star across our medium and low secure services as well as within our rehabilitation services, during 2010 and 2011. % of patients discharged prior to full engagement with the Recovery Star % of patients refusing to engage with the Recovery Star Key findings of the medium and low secure findings (Figure 11) include: • 63% patients engaging • 22% patients discharged prior to engagement • 15% patients refusing to engage Figure 12 – Pie chart showing number of patients within It should be noted that recorded data did not include that of our Brain Injury Services or Ayr Clinic (Scotland), due to differing data required by contract. Key findings of the rehabilitation findings (Figure 12) include: • 85% patients engaging • 14% patients discharged prior to engagement • 1% patients refusing to engage For the purposes of this data collection, PiC rehabilitation findings included: Abbey House, Aderyn, Pelham Woods, Tennyson House, The Willows, as well as the relevant wards of Kneesworth House, PiC Learning Disability Services, Llanarth Court and Oaktree Manor. PiC Rehab Services engaged with Recovery Star 1 14 85 % of patients engaging in their Recovery Star % of patients discharged prior to full engagement with the Recovery Star % of patients refusing to engage with the Recovery Star 29 Section 3 – Our 2010 / 2011 priorities 4. Deliver the recovery model in all PiC hospitals (cont) Recovery Star in Learning Disability Services A team from across PiC has been working alongside Triangle Consulting, developers of the Recovery Star, in conjunction with nine other NHS and Independent Sector Learning Disabilities Services to draft the new Learning Disability Recovery Star. This work has included attendance at workshops with other members of the working group. To represent patient and staff views, a focus group session was held at PiC Burston House Hospital in March. A total of 14 patients and members of staff form across PiC LDS and Oaktree Manor met with the Director of Triangle Consulting to contribute to a draft of the new Learning Disabilities Recovery Star. The team from PiC will continue to contribute to the wider working group and both PiC LDS and Oaktree Manor have been selected as sites for a 3-4 month pilot of the Learning Disabilities Star in the summer of 2011. Triangle Consulting is hoping to have the final version of the Learning Disabilities Recovery Star available by the end of 2011. PiC have been approached to contribute to a version of the Recovery Star for client with autistic spectrum disorders. Action • 30 To further standardise the Recovery data collection and analysis Section 3 – Our 2010 / 2011 priorities 5. Continue to improve on overall quality, whilst not increasing costs Our commitment to value for money PiC is committed to working in partnership with commissioners to support the national quality, innovation, productivity and prevention (QIPP) initiatives. PiC has a programme to standardise all essential clinical processes and the complimentary documentation across all hospitals during 2011. March 2011 saw the launch of the first of these documents – the Referral Assessment Report and Pre-admission Care Plan. We believe it is imperative that our assessments of potential new patients are timely, consistent and of the highest quality. A good and detailed assessment will inform early care plans and be subject to review at care programme approach (CPA) meetings. We will seek commissioner feedback on the consistency of our processes during the second half of 2011 as part of what will be a regular review process. The next stage in our standardisation programme will be a CPA policy and documentation with guidance which delivers more frequent communication with all stakeholders from the point of admission and throughout the care pathway. Further, it will endorse the concept of greater internal challenge within multidisciplinary teams and CPA meetings and, in doing so, continue to keep the focus on reducing length of stay and minimising delayed discharge. The feedback we have received so far from case managers has been rewarding with significant comment around the positive impact the new framework is having on the decision-making process. Treatment timeline framework In the six months leading to March 2011 a programme was devised that allowed service delivery to be described in a consistent and linear fashion, extending from referral through to discharge planning. Whilst this framework is not a ‘one size fits all’ approach, it depicts how clinicians interact with the patient, each other and with other external stakeholders to maximise the opportunities for progress towards the defined goals. We will continue to encourage feedback on the suitability of this document and review its format in the light of comment and advice. The feedback we have received so far from case managers has been rewarding with significant comment around the positive impact the new framework is having on the decision-making process 31 Section 3 – Our 2010 / 2011 priorities 6. Continue to review patterns of demand and, where necessary, adjust clinical offerings Patterns of demand for our services have inevitably changed over time. Whilst all our hospitals provide both national and local centres of excellence, the repatriation of patients close to home has been a priority for commissioners. In an environment of rapid change we have adjusted some of our services. Principally: • Calverton Hill Hospital in Nottinghamshire now offers a male learning disability service in conditions of medium security • Hazelwood House, part of PiC Midlands, has been refurbished and provides low secure rehabilitation for male learning disabled residents • The Dene in Sussex has opened a male low secure mental illness service Going forward, we will continue to review services in light of demand and commissioner needs. Delivering Same Sex Accommodation – Declaration of Compliance PiC is proud of its achievement of providing secure accommodation with single sex wards 32 PiC is proud of its achievement of providing secure accommodation with single sex wards for all patients. Patient dignity is further maintained through the provision of single bedrooms with access to single sex toilets. Section 3 – Our 2010 / 2011 priorities 7. Continue to develop information management and technology systems Monthly and quarterly monitoring reports have been adopted across the company to allow single, consolidated reporting. The Electronic Patient Records Project In this reference period PiC engaged Coldharbour Systems Limited as its partner to implement their Acute and Mental Healthcare Enterprise System (Electronic Patient Record). This integrated system met a wide range of requirements including patient administration, patient clinical records, invoicing, staff rostering, corporate clinical governance, and business intelligence reporting tools. The first stage was the implementation of CAREnotes – the Patient Information Process to enable MHMDS reporting. The software was configured in April 2010, tested in May, and piloted at Kneesworth House in June. The first stage of CAREnotes was then rolled out to all 23 of PiC’s hospitals by March 2011. The Coldharbour Acute and Mental Healthcare System aims to deliver a programme of change that will keep PiC at the forefront of mental health care practice. The benefits of the project for PiC and commissioners include: • professional, clear and compliant patient records • accurate comprehensive reports which are simple to produce, from a single central database • reports that will satisfy our customers requirements for more information about their patients • more focused and better informed staff • efficiencies that come from removing duplication of effort, errors and inaccuracies • wider engagement and empowerment of all PiC staff with a unified source of patient and business information This integrated system met a wide range of requirements including patient administration, patient clinical records, invoicing, staff rostering, corporate clinical governance, and business intelligence reporting tools PiC Website We regularly review and update the Partnerships in Care website. In June 2010 we migrated the website to a new hosting centre, with a refreshed user interface allowing a more timely update of information. We will be creating new content for patients, relatives and carers in July 2011. Information Governance Statement of Compliance (IGSOC) We have achieved information governance statement of compliance (IGSOC) and an N3 connection application has been submitted and accepted. We expect this to be installed and implemented by the end of June; this will allow us to make our MHMDS submissions and allow NHS mail accounts to staff. 33 Who was involved in the development of this report? This Quality Account has been developed with input from many staff groups across PiC. Namely, information has been provided by our Corporate Director of Nursing, Clinical Governance Commitee and Information Manager. Our communication team has helped pull the information together into an accessible format. Please give us your feedback This is the second year that we have produced a Quality Account and we welcome any feedback about content, style or any other issues. If you want to comment, please email either our Corporate Director of Nursing (Doreen.McCollin@partnershipsincare.co.uk), or our general Info address (info@partnershipsincare.co.uk). Alternatively, please write to Doreen McCollin, Corporate Director of Nursing, Partnerships in Care, 2 Imperial Place, Maxwell Road, Borehamwood, London, WD6 1JN 34 35 For further information please visit our website: www.partnershipsincare.co.uk Partnerships in Care 2 Imperial Place Maxwell Road Borehamwood Hertfordshire WD6 1JN