Kirklees Community Healthcare Services Quality Account 2010 - 2011
advertisement

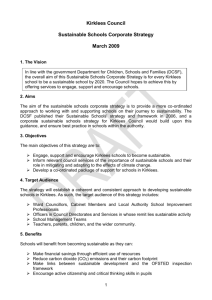
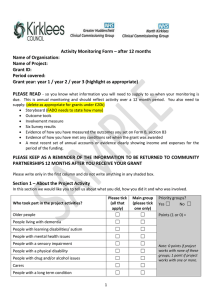
Kirklees Community Healthcare Services Quality Account 2010 - 2011 Contents Section One: 1.1 Foreword from the Chief Executive 4 1.2 Statement of Quality Assurance from the Chief Executive and Chair 5 Section Two: 2.1 2 Kirklees Community Healthcare Services 4 Priorities for improvement 6 6 2.11How will we monitor, measure and report these priorities? 7 2.2 Statements relating to the quality of services provided 9 2.2.1 Review of services 9 2.2.2 Participation in clinical audits 10 2.2.3 Participation in clinical research 11 2.2.4 Use of the CQUIN payment framework 12 2.2.5 Statements from Care Quality Commission 12 2.2.6 Data quality 12 | Quality Account 2010/11 Section Three: 14 3.1 Complaints 14 3.2 Claims and litigation 16 3.3 Local patient surveys 16 3.4 Patient opinion 16 3.5 Incident reporting and monitoring 17 3.6 Serious untoward incidents 17 3.7 Serious case reviews 17 3.8 Contract quality areas 18 3.9 Reducing mixed sex accommodation 19 3.10 Compliance with NICE guidance 20 3.11 NICE quality standards 20 3.12 Healthcare Associated Infections 20 3.13 Hand hygiene 20 3.14 Methicillin-resistant Staphylococcus Aureus (MRSA) 21 3.15 Screening patients for MRSA 21 3.16 Clostridium Difficile 21 3.17 Norovirus 21 3.18 PEAT (Patient Environment Action Team) 22 3.19 Compliance with national target for 18 weeks from referral to treatment 22 Section Four: 24 4.1 Appendix 1 24 4.1.1 24 CQUIN compliance information Section Five: 28 5.1 Statements from our Stakeholders 5.1.1 Kirklees Local Involvement Network 28 5.1.2 Kirklees Overview and Scrutiny Committee 28 5.1.3 Kirklees Primary Care Trust 28 5.1.4 Greater Huddersfield GP Commissioning Consortium 28 5.1.5 North Kirklees GP Commissioning Alliance 28 5.2 How to provide feedback on this account Quality Account 2010/11 | Kirklees Community Healthcare Services 29 3 Section one 1.1 Foreword Welcome to our first annual quality account. This document will demonstrate that the quality of our service is the lifeblood of this organisation. We are passionate about the care and support we provide and equally passionate about helping our staff to continually develop. We are an organisation providing a diverse range of services – from nursing in the home to specialised dentistry. All our colleagues in each of our services know that safety comes first every time. Our Board has ensured that we have robust and thorough procedures in place so that we learn quickly from mistakes and that we continually review our clinical practice to make sure we are performing to our best. I am particularly pleased that we have: • Successfully complied with the rigorous requirements of the Care Quality Commission (CQC) inspection at Holme Valley Memorial Hospital • Developed new systems to track quality improvement in areas such as nutrition, pressure sores and the healthy child programme • Worked to minimise any community acquired infections, including MRSA and C Difficile The next year brings us a new and exciting challenge. Kirklees Community Healthcare Services is becoming a community interest company (CIC), owned by the staff with membership from the community. It will operate under a new name – Locala Community Partnerships – and aims to continue to transform care within the community. My pledge is that Locala will continue to ensure safety comes first and that quality is the key driver to all the care and support we give. I look forward to reporting on quality improvement in future years. Robert Flack Managing Director, Kirklees Community Healthcare Services Chief Executive designate of Locala Community Partnerships 4 Kirklees Community Healthcare Services | Quality Account 2010/11 1.2 Statement of Quality Assurance from Chief Executive and Chair The Board of Kirklees Community Healthcare Services endorses the first quality account which puts improving quality and safety at the forefront of our work. We know our colleagues are committed to providing care which makes a genuine difference to people’s lives and that they are driven by the desire to improve their services. The Board is excited that the community interest company (CIC) that comes into being from October 2011 will have active involvement and direction from both staff and members of the community. The Board will listen to their experiences and respond by helping the organisation develop around the needs of the individual and the community they serve. This account has been reviewed by the Board, and to the best of our knowledge, accurately reflects both an overview of the quality of the services provided by Kirklees Community Healthcare Services during 2010-11 and our priorities for quality improvements during the next year. The information provided in this report is, to the best of our knowledge accurate and a reasonable reflection of our commitment to quality in 2010-11 Robert Flack Managing Director Suzy Brain England, OBE Chair Quality Account 2010/11 | Kirklees Community Healthcare Services 5 Section two 2.1 Priorities for improvement In this section of our report, we intend to focus on the future and 201112 in particular. It should be noted that this section of the report has not been planned in isolation but that the priorities discussed below have been agreed through discussion with our staff and commissioners. We believe that it is important that our priorities complement the Commissioning for Quality and Innovation (CQUIN) scheme, our compliance with the 16 essential standards for registration with the Care Quality Commission, and demonstrate our development over time. We have agreed that we will focus on a small number of important priorities during the next year and aim for significant improvement. Table 1 – 2011/12 priorities Lead Responsibility Category Aim Objective Priority 1: Clinical effectiveness To support patients to remain at home following discharge from hospital To increase the number of patients supported to remain at home for at least 90 days to 85% of all patients discharged from intermediate care units following a stay in hospital Patient safety To reduce the number of patients developing a pressure ulcer whilst in the care of KCHS To reduce the incidence of pressure ulcers by 50% Patient safety To reduce the number of falls experienced by patients within intermediate care inpatient rehabilitation units To reduce the number of patient falls by 50% Patient experience To ensure patients within the community nursing service receive a response appropriate to their needs within a specified timeframe To ensure that 80% of patients within the community nursing service receive a response from a health care professional within a specified time frame Patient experience To improve outcomes relating to child development and behaviour through the targeted intervention of community nursery nurses To ensure that a minimum of 50% of targeted interventions by a community nursery nurse result in positive outcomes for parents and children Sponsor: Clinical and Operations Lead Responsible manager: Head of Therapies Priority 2: Sponsor: Clinical and Operations Lead Responsible manager: Head of Localities Priority 3: Sponsor: Clinical and Operations Lead Responsible Manager: Head of Therapies Priority 4: Sponsor: Clinical and Operations Lead Responsible manager: Head of Localities Priority 5: Sponsor: Clinical and Operations Lead Responsible manager: Head of Localities 6 Kirklees Community Healthcare Services | Quality Account 2010/11 2.1.1 How will we monitor, measure and report these priorities? Each priority is being sponsored by an Executive Director. The Governance Committee will monitor each priority and report to the Kirklees Community Healthcare Services Board on progress. The reports to the Board from the Governance Committee will be made by the Non-Executive Director chairing the Governance Committee and will form part of the public agenda. The reports will be available to the public through the KCHS website: www.kirkleeschs.nhs.uk. Priority 1: Priority 3: Situation The percentage of clients going home after a stay on a bedded unit is variable, fluctuating from 70 – 100% Situation We have a relatively high number of falls within the IMC bed bases compared to other non rehabilitation units Why is there a problem? The clients entering intermediate care bedded units are getting older and have multiple medical conditions. The final outcome for these individuals is less obvious than it would have been in the past and as such there is a greater risk of clients not ultimately going home. Why is there a problem? Rehabilitation by its very nature will involve the risk of falls. If we reduce all risks we will increase the length of stay on the unit and potentially increase the number of clients admitted to 24 hour care. Increased numbers of clients would not regain their previous level of mobility and independence. Initiatives to be implemented in 2011-12 Initiatives to be implemented in 2011-12 • Home assessments for all clients that are at risk of not going to their original home. • Implementation of Falls Risk Bands to identify high risk clients • Involvement of the social worker from day one to consider alternative home situations i.e. sheltered housing. • Mapping of falls on the unit to help identify any hot spots • Full assessment of equipment requirements to manage with independent living. • Increased ongoing assessment To support patients to remain at home following discharge from hospital To reduce the number of falls experienced by patients within intermediate care in-patient rehabilitation units • Increased signage around the ward • New call bell system • The purchase of pressure mats for high risk clients. Priority 2: To reduce the incidence of pressure ulcers caused whilst in the care of KCHS by 50% Situation KCHS treats the development of pressure ulcers very seriously as this delays mobilisation for patients and can result in deteriorating health and quality of life - often necessitating a hospital admission. KCHS is working with partners to ensure that patients receive the highest quality care in a timely manner and the appropriate equipment to support that care. KCHS community nurses understand what actions they can take that will have the most impact on patients in terms of quality of care given and value for money. Why is there a problem? KCHS is monitoring the prevalence of pressure ulcer development whilst patients are in its care and whilst system failure is not an excuse, recognises that more can be done particularly in work undertaken in residential homes. Initiatives to be implemented in 2011-12 • Robust systems for assessing a patient’s skin on admission to KCHS care in order to have a baseline when the skin deteriorates • Work with Kirklees Integrated Community Equipment Service and local acute partners to develop a whole system approach. Priority 4: To ensure that 80% of patients within the community nursing service receive a response from a health care professional within a specified time frame Situation KCHS has developed a Single Point of Access for community nursing which specifies the response time required within a time frame, according to priority. Why is there a problem? KCHS has had challenges in developing the systems to ensure that patients’ priorities are identified when care is ongoing and their needs change Initiatives to be implemented in 2011-12 • To develop a robust method of ensuring that each patient is given the right priority level at the point of referral (or referral for a new problem) • To collect information to assure KCHS that the patient’s need has been met according to the grade of priority • To monitor the number of calls waiting to be answered at the Single Point of Access as this is an indication of the quality of response provided Quality Account 2010/11 | Kirklees Community Healthcare Services 7 Priority 5: To ensure that a minimum of 50% of targeted interventions by a community nursery nurse result in positive outcomes for parents and children Situation KCHS has a vibrant health visiting service of which nursery nurses play an important part in providing parenting skills coaching for parents as part of the Every Child Matters outcomes for children. KCHS is striving to maximise the use of skills within the health visiting resource and to be the most productive and efficient that it can with a limited resource. Why is there a problem? We know that nursery nurses in different teams across Kirklees undertake different work and have not always had their work evaluated in terms of outcomes for children. Initiatives to be implemented in 2011-12 • To review the content and results of nursery nurse activity • To develop detailed information on what the nursery nurses are able to offer parents • To establish methods of evaluating the outcomes of nursery nurse interventions with parents and children as detailed in Every Child Matters The organisation has identified the areas for improvement and will review the quality of performance as described above. The framework will enable the organisation to be accountable for the quality of services it provides. Each of these initiatives will be supported through strong executive leadership and work with our main education providers to ensure that our staff are able to develop additional skills and competences. Training and education is an important part of quality and culture within the organisation. 8 Kirklees Community Healthcare Services | Quality Account 2010/11 2.2 Statements relating to the quality of services provided 2.2.1 Review of Services During 2010–11 Kirklees Community Healthcare Services provided a range of services across Kirklees. On 31 March 2011, we were providing care for over 259,000 people across Kirklees. The organisation is led by a Managing Director and currently has four operational service areas: • Localities • Therapies Our clinical services are supported by a number of central functions including Finance, Human Resources, Business support, Integrated Governance and Training. Kirklees Community Healthcare Services has reviewed all the data available to them on the quality of care in 100% of these services. The income generated by the NHS services reviewed in 201011 represents 100% per cent of the total income generated from the provision of NHS services by Kirklees Community Healthcare Services for 2010-11. • Long term conditions • Dental Localities Senior managers regularly spend time with clinical services to review issues with staff and consider governance concerns. Therapies Long term conditions District Nursing Occupational Therapy (acute, learning disabilities, children) Community Matrons Health Visiting Speech and Language Therapy (adults, children) Children’s Community Nursing (including Dermatology, Respiratory and Diabetes) School Nursing Primary care Gynaecological Service Children’s Immunisation team Family Nurse Partnership Community Rehabilitation Service MacMillan Nurse Specialists for care homes Looked After Children Accessible Homes team Continence Service Chlamydia Screening Jubilee Rehabilitation Service Community Diabetes Service Smoking Cessation Service Musculoskeletal Service Coronary Heart Disease Service Community Child Health Day Surgery Whitehouse GP practice Pupil Referral Service Maple Ward Broughton House GP practice Youth Offending Team Moorfields Primary Care Centre Nurse Advisors for Safeguarding Children and Adults Walk in Centre, Dewsbury District Hospital Breastfeeding initiative counsellor Podiatry Vasectomy Service Contraception and Sexual Health Dental Community Dental Service (Calderdale and Kirklees) Falls Assessment Intermediate Care Services Kirklees Integrated Community Equipment service Quality Account 2010/11 | Kirklees Community Healthcare Services 9 2.2.2 Participation in clinical audits During 2010-11, two national clinical audits covered NHS services that Kirklees Community Healthcare Services provides. During this period, Kirklees Community Healthcare Services participated in 100% of the national clinical audits in which it was eligible to participate. The national clinical audits and national confidential enquiries that Kirklees Community Healthcare Services was eligible to participate in during 2010–11 are as follows: • National Sentinel Audit for Stroke • National Paediatric Diabetes Audit The national clinical audits and national confidential enquiries that Kirklees Community Healthcare Services participated in during 2010–11 are as follows: • National Sentinel Audit for Stroke • National Paediatric Diabetes Audit The national clinical audits and national confidential enquiries that Kirklees Community Healthcare Services participated in, and for which data collection was completed during 2010-11 are listed below alongside the number of cases submitted to each audit or enquiry as a percentage of the number of registered cases required by the terms of that audit or enquiry. Percentage of registered cases required Number of cases submitted National Sentinel Audit for Stroke 28 100% National Paediatric Diabetes Audit 67 100% The reports of two national clinical audits were reviewed by the provider in 2010-11 and Kirklees Community Healthcare Services intends to take the following actions to improve the quality of healthcare provided National clinical audit National Sentinel Audit for Stroke Actions • To increase FAST awareness of Community and Intermediate care staff • To contribute to therapy review being undertaken by NHS Kirklees • To develop care planning templates on SystmOne so that patient goals can be monitored • To improve data collection systems within SystmOne National Paediatric Diabetes Audit • To Identify and target population with HbA1c above 9.5% • To give intensive education and support to those identified • To ensure child or young person is initially followed up by telephone and subsequently in a nurse led clinic or home visit • To repeat HbA1c on a four monthly basis 10 Kirklees Community Healthcare Services | Quality Account 2010/11 Clinical audit is supported by the Integrated Governance team. All local clinical audits are agreed through the Audit and Effectiveness Committee. Reports are considered and action plans for quality improvement reviewed through this committee. The reports of 20 local clinical audits were reviewed by the provider in 2010-11 and Kirklees Community Healthcare Services intends to take the following actions to improve the quality of healthcare provided: Safeguarding Safeguarding policy requires that when information about vulnerable children is shared between health visitors and school nurses with general practice teams, work should be structured with reference to a ‘Best Practice Framework’. The Best Practice Framework is detailed in NHS Kirklees Safeguarding Children Policy. This policy further outlines the standard of record keeping of the information sharing that should take place, and requires that health professionals utilise a ‘communication child protection template’, that is available on the SystmOne electronic health record, to record this area of safeguarding work. The use of this template prompts a high standard of record keeping that focuses on improving the safety and wellbeing of children, and also enables reports of this area of safeguarding work to be generated, which provides information about trends and incidence of this aspect of safeguarding children work. Use of the template was therefore audited. The audit results indicate that the communication child protection template is being used with increasing frequency by health visitors and school nurses working in locality teams, when they discuss vulnerable children with colleagues in general practice. The increasing frequency that the template is being used suggests that increasingly discussions between health visitors, school nurses and general practitioners in respect of vulnerable children is structured and focused, and agreement to a specific action plan that will be influential on a child’s safety is being made. Chlamydia In November 2010 the National Chlamydia Screening Programme carried out a quality assurance audit of turnaround times from the time of the test to results being received, and to positives being treated. The audit covered a two week period from 1-12 November. The audit showed that Kirklees Community Healthcare Services has met all the standards required. Kirklees Community Healthcare Services is aware of the importance of clinical audit in improving the quality of the services it provides and as such aims to undertake even more clinical audit during the next year. 2.2.3 Participation in clinical research During the past year, we have concentrated on developing the framework within which we can examine our compliance with evidence based practice through clinical audit and benchmarking against NICE guidance. The number of patients receiving NHS services provided or subcontracted by Kirklees Community Healthcare Services in 2010-11 that were recruited during that period to participate in research approved by a research ethics committee was 178. Participation in clinical research demonstrates Kirklees Community Healthcare Services commitment to improving the quality of care we offer and to making our contribution to wider health improvement. Our clinical staff stay abreast of the latest possible treatment possibilities and active participation in research leads to successful patient outcomes. Kirklees Community Healthcare Services was involved in conducting nine clinical research studies in eight specialities during 2010-11. There were seven clinical staff participating in research approved by a research ethics committee at Kirklees Community Healthcare Services during 2010-11. External reviews Our systems are subject to periodic review by the West Yorkshire Audit Consortium. During 2010-11, reviews were undertaken in four areas: records management, incident reporting, clinical governance and risk. All were awarded a ‘Significant Assurance’ grading which shows that we had established sound systems of internal organisational control but that there is still more that we can do. As a result, action plans have been developed and are being monitored. Our progress in these areas will be reviewed. 2.2.4 Use of the CQUIN payment framework A proportion of Kirklees Community Healthcare Services’ income in 2010-11 was conditional on achieving quality improvement and innovation goals agreed between Kirklees Community Healthcare Services and NHS Kirklees through the Commissioning for Quality and Innovation (CQUIN) payment framework. Further details of the agreed goals for 2010-11 and for the following 12 month period are available electronically at the link below Our achievement against both the regional and local CQUIN targets is shown in Appendix 1. www.institute.nhs.uk/world_class_commissioning/pct_portal/cquin.html Quality Account 2010/11 | Kirklees Community Healthcare Services 11 2.2.5 Statements from CQC 2.2.6 Data Quality Kirklees Community Healthcare Services is required to register with the Care Quality Commission and its current registration status is registered and licensed to provide services. This means that it has been agreed that our services meet the essential standards of quality and safety. These standards are available electronically at www.cqc.org.uk. We accept responsibility for providing good quality information to support effective patient care. We participate in NHS Kirklees information governance processes and are supported by the Director of Patient Care and Professions who is currently our designated Caldicott Guardian. The Care Quality Commission has not taken enforcement action against Kirklees Community Healthcare Services during 2010-11. The Care Quality Commission undertook an unannounced inspection to Holme Valley Memorial Hospital on 16 June 2010 to assess that we were adequately protecting patients, staff and others from healthcare associated infection. On the inspection, it was found that there was no cause for concern regarding our compliance with the regulation on cleanliness and infection control. The organisation meets with the Care Quality Commission’s link manager on a quarterly basis to maintain a regular dialogue. Participation in Special Reviews Kirklees Community Healthcare Services has participated in special reviews by the Care Quality Commission relating to the following areas during 2010-11: Supporting life after stroke Kirklees Community Healthcare Services intends to take the following action to address the conclusions or requirements reported by the Care Quality Commission: • A group with members from Kirklees Community Healthcare Services, Mid Yorkshire Hospitals Trust and NHS Kirklees has been established to look at how patient pathways could be improved within existing resources and what could have the most impact with limited investment. • The group agreed actions which included mapping the existing pathways for each element of the pathway; identifying blockages in the pathway; looking at separating costs between organisations , reducing waiting times for rehabilitation services Kirklees Community Healthcare Services has made the following progress by 31 March 2011 in taking such action: • P athways have been mapped and greater clarity has been given for each service in the pathway. As a result of this work referral forms/information is being standardised for referrals into Intermediate Care services. • W aiting times for rehabilitation services have reduced and this work will continue to reduce waiting times further. • C onsideration has been given to separating costs for stroke between organisations so as to strengthen community based rehabilitation and support services. Outreach Occupational Therapy and Physiotherapy from acute hospital services has been established as resources allow to bridge the gap between secondary and community services whilst further work is done by NHS Kirklees Support for families with disabled children [the data collection period was January – February 2011; the results are expected to be available in Spring 2011 when we will review the findings and develop action plans in response] “Thank you for the loving care you gave Mum over the last few months. You all do a fantastic job, sometimes in very difficult circumstances.” 12 Kirklees Community Healthcare Services | Quality Account 2010/11 Most of our services now use electronic records through SystmOne which provides a single clinical information system and reduces the number of times a patient is required to provide personal data. We have adopted mobile technology which enables the clinical professional to have access to records whilst providing care, whatever the location and saves the clinician having to return to base. This equipment also includes an alarm system to enhance staff safety. The project has been subject to strict governance arrangements to ensure that patient information is secure. Kirklees Community Healthcare Services will be taking the following actions to improve data quality: • Implement the mandatory data set for Community Services in KCHS to ensure consistency of data collection within all clinical services. • Achieve the Data Quality Priorities as set out in the contract for community services with NHS Kirklees. • Ensure the appropriate use of SystmOne functionality to support the accurate recording of patient activities. • Develop Data Quality measures that will support the collection and reporting of information to evidence clinical / patient outcomes. NHS Number Clinical records audit At the end of March 2011 we had 147,292 clinical records of which 99.4% included the patient’s NHS number and 99.5% included the patient’s GP. Record keeping is an essential, integral and legally required part of the patient care process. Patients/clients benefit from records that demonstrate effective assessment and planning of care which supports high quality clinical interventions. All health care professionals are expected to provide accurate, comprehensive and concise information which justifies the rationale regarding treatment, care and support that is planned and provided for the patient/client. They are also required to comply with both locally agreed policies and professional guidelines. The auditing of records and acting on the results allows for the assessment of the standard of record keeping which in turn identifies any areas where improvements might be made (NMC 2009). A total of 610 clinical records for KCHS were audited in 2010. We plan to increase this number year on year. The following graph shows the age breakdown of our patients: Kirklees Community Healthcare Services Age Bands 50% 45% 40% 35% 30% 25% 20% 15% 10% 5% 0% Age Band 0-5 Age Band 6-10 Age Band 11-15 Age Band 16-20 Age Band 21-25 Age Band 26-30 Age Band 31-35 Age Band 36-40 Age Band 41-45 Age Band 46-50 Age Band 51-55 Age Band 56-60 Age Band 61-65 Age Band 66-70 Age Band 71-75 Age Band 76-80 Age Band 81-85 Age Band 86-90 Age Age Age Age Band Band Band Band 91-95 96-100 101-105 106-110 We have been working to increase the number of patient records that include the ethnic background as stated by the patient. This has increased from 17.7% in April 2010 to 50.3% in March 2011. The breakdown is shown in the graph below: Kirklees Community Healthcare Services Ethnic Coding 50% 45% 40% 35% 30% The audit provided information about specific issues regarding electronic records which has proved invaluable as services adopt electronic record keeping. It identified areas for improvement which have been incorporated into mandatory training and to a more specific audit on the electronic record keeping of the Supporting Families’ service. 25% 20% Clinical coding error rate 15% 10% Clinical coding is a process which translates the medical language of patients’ records into an internationally recognised code describing the diagnosis and treatment of a patient. 5% 0% British Irish Other White White and White and Other Black Black Mixed Caribbean African Background Indian Pakistani Bangladeshi Other Caribbean Background African Other Black Chinese Any Other Not Given Information Governance Toolkit attainment levels Information quality and records management are assessed using the Connecting for Health Information Governance Toolkit which provides an overall assessment of data systems, standards and processes. The toolkit is completed by specialists advising the NHS Kirklees Information Governance Group and is validated by NHS Kirklees directors before submission. Kirklees Community Healthcare Services Information Governance Assessment Report score is incorporated within the NHS Kirklees overall score for 2010-11, which was 67% and was graded Red. NHS Kirklees has developed an action plan to manage the issues identified and Kirklees Community Healthcare Services is also working to develop its own systems and processes for separate assessment in 2012. Quality Account 2010/11 | Kirklees Community Healthcare Services was not subject to the Payment by Results clinical coding audit during 2010-11 by the Audit Commission. “Keep up the fantastic job you’re doing – we need more nurses like you.” Kirklees Community Healthcare Services 13 Section Three Review of Quality Performance 3.1 Complaints Community organisations have not previously been required to develop and publish a Quality Account. As a result, this report focuses on the information that is currently available. In future years, we will be including a review of progress on our quality initiatives. During the year, 22 letters of complaint were received relating to our services. In that period there were over 750,000 patient contacts. We encourage all clinicians and all services to respond immediately to issues raised by patients and carers. The information below, therefore, refers solely to written complaints that have been received. We aim to acknowledge all letters within three days. A manager, independent of the service concerned, is appointed to investigate the issues. This person makes contact with the person complaining and works with them and the service concerned to resolve the issues. At the end of the process a full written response is provided and we aim to complete this process within 28 days. When this is not possible, the complainant is kept fully informed of how the investigation is progressing. The investigating manager also produces recommendations for service improvement with are developed into an action plan. The implementation of this plan is monitored through the Audit and Effectiveness Committee. Learning from complaints It is crucial that the organisation learns from all issues raised and ensures changes in practice to further the provision of high quality services. The following describes some of these changes that have occurred: 1.System implemented to ensure that telephone messages are collected and responded to on day of receipt 2.Procedures established to improve the management of distraught children and parents within clinic settings 3.Funding for additional therapy staff provided by commissioner to improve waiting times 4.Working with other providers to improve the patient’s journey from one provider to another Any complainant who remains unhappy after their complaint has been investigated is provided with the opportunity to meet with a manager and the relevant clinical staff in a further attempt to resolve the issues. All complainants are informed of their right to refer the issue to the Health Service Ombudsman. During 2010-11 no complaints were referred in this way 14 Kirklees Community Healthcare Services | Quality Account 2010/11 The table below shows the number of complaints by service: Service Year 2010-11 complaints Dermatology 1 Podiatry 1 Continence 3 District Nursing 5 Single Point of Access 1 Home Laundry 1 Dental 2 Multi-agency hospital discharge 1 Intermediate care 1 Contraception and Sexual Health (CaSH) 1 Community Rehabilitation team 1 Health Visiting 3 Musculo-skeletal service North 1 Total 22 Reasons for the complaint - Written complaints received from 1 April 2010 to 31 March 2011, by subject of complaint (using Department of Health categories) Reason for complaint Number of complaints Admissions, discharge and transfer arrangements 2 Appointments delay / cancellation (outpatient) 2 Attitude of staff 2 All aspects of clinical treatment 5 Communication / information to patients (written and oral) 4 PCT commissioning (including waiting lists) 5 Personal records (including medical and / or complaints) 1 Other 1 “A big thank you for all you did for my Mum. I am so glad I finally met you, such an understanding, kind, caring and gentle person. Thank you so much.” Quality Account 2010/11 | Kirklees Community Healthcare Services 15 3.2 Claims and litigation There are currently seven claims registered with the NHS Litigation Authority dating back to 2007. Of these claims, four relate to clinical negligence and three to personal injury. All cases are actively managed by our Governance team, lawyers and NHS Litigation Authority. 3.3 Local patient surveys During the year, we have used patient questionnaires across 42 of our services. The number of questionnaires sent out varied across the services as some had a set target within their service specification and others randomly handed them out at clinics over the period of a week or a month. Following return and collation, the results were considered by each service and improvement plans implemented, of which examples are shown below. In the Day Surgery Unit at Holme Valley Memorial Hospital, patients commented on the lack of reading material in the waiting area. As a result, magazines and newspapers are now provided. In the CaSH service at Princess Royal Health Centre, concerns were expressed about privacy in the reception area which has resulted in a risk assessment being undertaken and the glass partition being reviewed. The Community Matron survey showed that 91% of respondents knew how to contact a Community Matron and 92% of respondents rated the personal manner of staff as very good or excellent. The questionnaire allowed the matrons to identify areas for improvement which were: To aim to provide care plans to all patients on the caseload and endeavour to review these as appropriate at least six monthly To discuss future goals/goal setting with all patients where possible once their condition is stabilised and allows this to be feasible/practical. A Reception services survey suggested that staff have a friendly professional approach on Reception and on the phone and that the public feel the staff provide good customer services. It was identified that better quality of patient information could be displayed in the reception areas. Reception Supervisors now promote campaigns each month which may involve displaying promotional materials for weekly/national campaign days e.g. National No Smoking Day. The reception supervisors recognised the importance of monitoring confidentiality when attending the reception area so therefore asked patients for their perceptions. This highlighted a potential for improvement so the supervisors have organised clear notices advising patients that should they wish to discuss their personal details in confidence, this option is offered to them. Staff are also encouraged to be sensitive towards the needs of the client when attending reception and offer the option to speak in private with the member of staff. Clients using the Jubilee Rehabilitation Service gave positive feedback regarding all aspects of the service from the surroundings, to staff knowledge as well as how well the clients feel that their needs were attended to. This client satisfaction questionnaire is scored out of a possible 72. The clients that were surveyed gave the service an average score of 66. One area for improvement was identified. Several patients commented that they waited a while for the ambulance to collect them from home. The key aspect was to set realistic expectations for patients. For example the appointment cards now state that the pick-up time is estimated as the ambulance has to collect other service users and the route changes constantly. Waiting times continue to be monitored and patients provided with a comfortable area in which to wait. 16 Kirklees Community Healthcare Services | Quality Account 2010/11 3.4 Patient Opinion Patient Opinion is a social enterprise organisation that offers the opportunity for patients to share their experiences with others and to gain support from each other. People can submit stories via the internet, postal system or telephone calls with the opportunity for organisations to respond. We have encouraged patients attending Moorfields Primary Care Centre to share their experiences through these systems and are delighted that 16 patients have done so during the past year. Of these, 15 were overwhelmingly positive about the care they had received from the services at Moorfields whilst one was concerned about the waiting time for an appointment. As a result of this feedback, we have reviewed our clinic appointments to reduce waiting times. We are now considering how we can extend this system to other services provided by Kirklees Community Healthcare Services. 3.5 Incident reporting and monitoring The National Patient Safety Agency (NPSA) suggests that high levels of incident reporting should be viewed as positive. Those organisations that report incidents are more likely to have systems and processes in place to learn from incidents. During 2010-11 we have further enhanced the safety culture within Kirklees Community Healthcare Services. This has included Incident Monitoring training which was delivered to the senior and middle managers, individual training to teams and primary research undertaken by one of our managers, the recommendations of which will be shared and implemented within the organisation. Over this year, incident reports from staff have increased by 100% which shows that work to increase the profile of incident reporting has been successful. However, reporting is only part of the challenge and learning from incidents is of paramount importance. The organisation’s Incident Monitoring Group meets monthly and works to ensure that learning is shared not only within the organisation but with other agencies such as the acute trusts and social care. We continue to review and adjust membership, thus ensuring that the most appropriate professionals are involved in the incident monitoring process. Trends and themes are identified and where necessary, concerns are elevated to the Risk Committee. The distribution of a monthly newsletter ensures that feedback and learning on the most pertinent incidents is received by all staff within the organisation. Quarterly reports are submitted to the Governance Committee. We are aware that the increasingly diverse nature of care being delivered in the community by a variety of health professionals means that patient safety is even more important. We will continue to ensure that patient safety is paramount and that our incident reporting and monitoring systems and processes are constantly reviewed to meet the ever changing demands in community healthcare provision. 3.6 Serious Untoward Incidents We have had two serious untoward incidents this year, both related to the security of patient identifiable information. Formal investigations were undertaken into both incidents, including a root cause analysis. Action plans were subsequently developed and these have been implemented. Key learning for us as an organisation related to colleagues adhering to the requirements of our policies regarding email management and the storing and transfer of patient identifiable information. This learning has been cascaded throughout our organization and compliance has been monitored for assurance. 3.7 Serious Case Reviews There have been three serious case reviews related to children and one related to an adult this year. Our Named Nurses have produced Independent Management Reviews for each of these reviews regarding our involvement in the cases. These are then submitted to the appropriate Safeguarding Board. We are represented at both the Children’s and Adult’s Local Safeguarding Boards and actively participate in the management and review of these serious case reviews. Each of the serious case reviews has resulted in actions for us an organisation. This learning has been cascaded throughout the organisation and is incorporated into ongoing training and supervision. “My District Nurse was extremely punctual and caring. Her motivation and encouragement led to a quick and positive recovery.” Quality Account 2010/11 | Kirklees Community Healthcare Services 17 3.8 Contract quality areas Our contract to provide care includes a number of quality requirements. These are shown in the table below, and include our achievements in 2009-10, the targets that were set for 2010-11 and our actual performance as measured on 31 March 2011. 2009-10 Actual 2010 -11 Target 2010-11 Actual 0 2 0 Delayed transfers of care to be maintained at a minimal level 21% Not below 2009-10 performance 26% Failure to have a Delivering Same Sex Accommodation Plan or missing a milestone in the Plan 0 Requirements continue to be met 0 Proportion of children who complete recommended immunisations by 12 Months 97% 95% 95.8% Proportion of children who complete recommended immunisations by 24 Months 93.8% 95% 95% Proportion of children who complete recommended immunisations by 5 Years 91.9% 95% 92.1% Four week smoking quitters (Specialist Service) Actual 607 453 520 Childhood Obesity Measurement Coverage - Reception Year 91% No target 92% Childhood Obesity Measurement Coverage- Year 6 87% No target 92% Quality Requirement Community acquired MRSA bacteraemia Improvement In addition, there are a number of nationally specified targets with which we are required to comply and a number of Never Events which are serious, largely preventable patient safety incidents that should not occur if the available preventative measures have been implemented. Our compliance is shown right: “I can’t express how grateful I am that these professional women, who must see hundreds of patients a week, took the time and energy to make me feel completely safe and comfortable with a procedure I had been dreading.” 18 Kirklees Community Healthcare Services | Quality Account 2010/11 Nationally Specified Event Percentage of Service Users seen within 18 weeks across all speciality groups for admitted and non-admitted pathways Rates of Clostridium Difficile acquired in the community 4 hour maximum wait in A&E from arrival to admission, transfer or discharge Breach of the Same Sex Accommodation Requirements 2009-10 2010 -11 2010-11 Actual Target Actual 100% 95% 99.5% 0 < 11 3 100% 98% 100% 0 0 0 Improvement 2009-10 2010 -11 2010-11 Improvement Actual Target Actual Never Event Wrong site surgery 0 0 0 Retained instrument post-operation 0 0 0 Misplaced naso-or orogastric tube not detected prior to use 0 0 0 3.9 Reducing mixed sex accommodation Kirklees Community Healthcare Services has declared full compliance with the national target for single sex accommodation. Within the 20 bedded ward at Holme Valley Memorial Hospital, 15 beds are provided in five three-bedded wards, and there are five single rooms. The accommodation can be used by either men or women as all these rooms have en-suite toilet and shower facilities. The ward moved into its present accommodation in August 2009. The ward area was specifically designed for the client group. As part of the rehabilitation process, all patients are fully dressed through the day. Because all admissions are planned, there is no situation in which single sex accommodation requirements would be breached. The layout of the ward allows patients to move rooms as their condition improves which enables both male and female admissions to be managed. Maple Ward would be able to accept a husband and wife admission but they would be either within two single rooms or in two separate bed bays. However, the admission of two sisters or brothers could be facilitated within one bed bay. The combination of environment and care processes fully supports the patients’ dignity and privacy. This is also monitored through a discharge questionnaire. Analysis of returns consistently demonstrates that patients and their carers are appreciative of the environment and care provided. “I want them (the staff) to know that the work they do, the time they take to make people feel secure and their unfailing good grace is so very much appreciated.” Quality Account 2010/11 | Kirklees Community Healthcare Services 19 3.10 Compliance with NICE guidance 3.11 NICE Quality Standards The National Institute for Health and Clinical Excellence (NICE) provides guidance, sets quality standards and manages a national database to improve people’s health and prevent and treat ill health. Implementing NICE guidance benefits everyone – patients, carers, the public and the NHS. It helps ensure consistent standards in care, equal access to care and improvement in the quality of care provided. During the period from 1 April 2010 and 31 March 2011, 121 pieces of guidance have been issued. The standards are sets of specific statements that act as markers of high quality, cost effective patient care, covering the treatment and prevention of different diseases and conditions. They are developed from the best available evidence in partnership with NHS and social care professionals and service users, and address the three dimensions of quality: clinical effectiveness, patient safety and patient experience. Of the eight standards published during 2010-11, we have determined that four of them have relevance to the services that we provide. We have completed the assessment of our current compliance against three of the standards: stroke, dementia and venous thromboembolism prevention and are actively considering our compliance against the standard concerning Diabetes in Adults. During 2011-12, we will be working with our commissioners and colleagues from other organisations to ensure that we are able to provide evidence that our patients are receiving high quality care. 3.12 Health Care Associated Infections The guidance falls into five categories: Effective infection prevention and control is essential to ensure the safety of patients in our care, through avoiding Healthcare Associated Infections (HCAIs), as well as providing excellent patient experience. We are proud of our infection control achievements, some of which are set out below: • Cancer service guidance • Clinical guidelines • Interventional procedures • Public health guidance 3.13 Hand Hygiene • Technology appraisals Of the guidance issued during the past 12 months, 27 documents have been determined as having relevance to the services we provide. All of these documents have been closely considered by the relevant services using the baseline assessment tool provided by NICE. In 11 cases, evidence has been provided by services to demonstrate that they are fully meeting the standards; and, in a further seven cases, services were able to declare partial compliance. More recent guidance (nine documents) continues to be considered by the relevant services. When services are unable to show that they are fully meeting the standards, an action plan is developed and implemented. These action plans are monitored through the organisation’s Audit and Effectiveness committee until full compliance is achieved. Studies show that infection rates can be reduced by 10-50% when healthcare staff regularly clean their hands. The introduction of alcohol hand rub has been important in improving hand hygiene compliance in healthcare and is recommended for routine use in the clinical environment when hands are not visibly soiled. Alcohol hand gel at the point of care is critical in increasing the likelihood that staff will clean their hands at the appropriate times. All staff are provided with community hand hygiene packs for home visits. The National Patient Safety Agency (NPSA) developed the ‘clean your hands’ campaign which was extended to community services in 2008. All staff are required to provide clinical care ‘bare below the elbows’. This has been included in our Clinical Dress Code policy. Audit tools which measure compliance with hand hygiene requirements include the ‘bare below the elbows’ requirement. During the past year, staff compliance across all our services with these standards has been 98%. In addition, in 2009-2010 we introduced a monitoring tool for use by staff undertaking catheter care. This has been further enhanced by the introduction of electronic care plans for urinary catheter insertion and continuing catheter care and catheter training for all clinical staff. Compliance with these standards for the last year has been 96%. A simple guide for catheter hygiene has also been developed for carers, home care and care home staff for patients in their own homes which have to be signed and dated daily by the carer. Where compliance against these standards has not been demonstrated, additional training is provided with close monitoring until compliance has been consistently achieved. “Many thanks for all the care and kindness from everyone during my stay at the Hospital. Food and cleanliness all very good.” 20 Kirklees Community Healthcare Services | Quality Account 2010/11 3.14 Methicillin-resistant Staphylococcus Aureus (MRSA) We were set a target by NHS Kirklees of no more than two cases of MRSA during 2010-11. During this year no patients receiving care from Kirklees Community Healthcare Services staff have been diagnosed with an MRSA bacteraemia. 3.15 Screening patients for MRSA Mandatory screening of all patients admitted to intermediate care beds and patients undergoing podiatric surgery was introduced in 2009 in line with Department of Health policy. During 2010-11, 471 patients were screened, all of whom had a negative result. Performance against this policy is monitored on a monthly basis and has consistently achieved 100%. 3.16 Clostridium Difficile Incidence of Clostridium Difficile is also monitored closely. We were given a target of no more than 10 cases. During the year, three patients have been diagnosed as having Clostridium Difficile whilst in the care of our staff. In each case, an in-depth review has been undertaken and recommendations for improvement implemented 3.17 Norovirus “Thank you for your compassion and your care. My Mum could not have wished for better during the last days of her life and I will always be grateful to you for this.” There has been one outbreak of diarrhoea and vomiting in the ward at Holme Valley Memorial Hospital during 2010-11 which has resulted in the closure of the unit to admissions, transfers and discharges for 15 days. (An outbreak is defined as two or more connected patients with the same symptoms ). The outbreaks were caused by the Norovirus which is the most common cause of gastroenteritis in healthcare settings. It is a highly contagious virus which causes short term but severe diarrhoea and / or vomiting. The outbreaks affected 15 patients and 24 staff. All staff observed the outbreak policy and compliance was closely monitored by our Senior Infection Prevention and Control Nurse. Quality Account 2010/11 | Kirklees Community Healthcare Services 21 3.18 PEAT (Patient Environment Action Team) PEAT is an annual assessment of inpatient healthcare sites in England with more than 10 beds. The assessment was started in 2000 and has been managed by the National Patient Safety Agency (NPSA) since 2006. It is a benchmarking tool to ensure improvements are made in the non-clinical aspects of a patient’s healthcare experience. It highlights areas for improvement and shares best practice across the NHS. The annual assessment took place at Holme Valley Memorial Hospital in March 2011. The team included a non-executive director and a representative from the Hospital’s League of Friends. Scores from all organisations are submitted to the National Patient Safety Agency and are available on the NPSA website: http://www.nrls.npsa.nhs.uk/patient-safety-data/peat/ Results Year Environment Food Privacy and dignity 2011 (provisional) Good Excellent Excellent 2010 Good Excellent Good 2009 Good Excellent Excellent 3.19 Compliance with National Target for 18 weeks from referral to treatment The 2004 NHS Improvement Plan set out the concept that no-one would have to wait longer than 18 weeks from GP referral to treatment. This target applies to services that provide assessment and treatment but which may need to refer onwards to a consultant led service. Over the year, 100% of the relevant services were compliant with this approach. Across these services, the average waiting time was four weeks. 22 Kirklees Community Healthcare Services | Quality Account 2010/11 Quality Account 2010/11 | Kirklees Community Healthcare Services 23 Section four: Appendix 1 Quality priority Aim Rationale Objectives Achievement 80% of people with a Long Term Condition have a single personalised care plan 90% 80% of people on an end of life pathway have a single personalised care plan 100% 100% of Patients identified as being End of Life are on the End of Life Care Register 100% 80% of Patients identified as being End of Life are on the Liverpool Care Pathway or equivalent 13% 90% of patients who express their preferred place of death, actually died in that place 97% 80% of CAFs for 0-5 year olds are initiated by health professional 82% 65% of CAFs for 6-11 year olds are initiated by health professional 42% 40% of CAFs for 12-18 year olds are initiated by health professional 39% 60% of CAFs for 0-5 year olds are led by health professional 43% 65% of CAFs for 6-11 year olds are led by health professional 38% 40% of CAFs for 12-18 year olds led by health professional 39% Regional Indicators Long Term Conditions End of Life Care Vulnerable children 24 Improving and sharing personalised care plans for patients with long term conditions Improving the quality of palliative care Increase the use of the Common Assessment Framework (CAF) for vulnerable children Patients will begin to experience seamless responsive care in accordance with their wishes and agencies will have a single, common vehicle to improve communication and understanding. This will reduce unnecessary admissions into hospital and increase health outcomes. Patients and carers will be able to expect the highest possible standards of end of life care Improve safeguarding of vulnerable children Kirklees Community Healthcare Services | Quality Account 2010/11 Quality priority Child protection supervision Nutrition Pressure ulcers on community wards Pressure ulcers in non-ward areas Aim Rationale Maintain high levels of Child Protection Supervision given to staff that have regular contact with children, young people and parents “Effective communication is important to promoting good standards of practice and to support individual staff members” (Working Together to Safeguard Children, DH 2006) Achieving best practice standards as set out in Essence of Care Improvement in pressure ulcer prevention and management in line with Essence of Care Reduction in the number of pressure ulcers requiring care within the community Objectives Use of a validated nutritional indicator screening tool will be encouraged to reduce rates of malnutrition and associated adverse outcomes Inpatients experience care that maintains or improves the condition of their skin and underlying tissues for all ages All Patients experience care that maintains or improves the condition of their skin and underlying tissues for all ages Quality Account 2010/11 | Achievement 85% of staff who are eligible for child protection supervision have child protection supervision within each quarter 90% 100% of admitted patients who underwent nutritional screening within 24 hours of admission 100% 100% of High nutritional risk patients with appropriate referrals/ continuing care plans in place 21% 100% of patients with a grade III pressure ulcer or above have had a root cause analysis investigation 100% No patients acquire a pressure ulcer within10 days of admission to the ward 0 < 19 patients with one or more pressure ulcers, with the highest ulcer having NICE Trigger Grading III in quarter four. 26% < 17 patients with one or more pressure ulcers, with the highest ulcer having NICE Trigger Grading IV in quarter four. 9 100% of root cause analysis investigations undertaken for patients with NICE Grade III pressure ulcers and above. 52% Kirklees Community Healthcare Services 25 Quality priority Aim Rationale Objectives Achievement Local Indicators Incidence of pressure ulcers Discharge Care Planning 26 Reduce the incidence of all grades of pressure ulcers Maintaining more people at home through movement towards a multi disciplinary approach to discharge planning with patients and carers fully involved and informed along the process. Pressure ulcer incidence data provides good evidence regarding quality of care provided to patients and it is important to note that pressure ulcers are increasingly being linked to elder abuse and neglect (Clarkson 2007). This indicator closely links with the Regional indicator around discharge planning for people with Long Term Conditions. The two combined indicators support the efficiency saving for non-elective admissions where we can influence through this incentive scheme Kirklees Community Healthcare Services | Quality Account 2010/11 100% of all patients to have had a Waterlow Pressure Ulcer Risk Assessment 82% 50% reduction in the incidence of all grades of pressure ulcers by 31st March 2011 293 100% reduction in community acquired pressure ulcers of grade 3 and 4 Insufficient data 10% reduction in length of stay through effective discharge/care planning by Quarter 3 2010-11 45% 20% reduction in length of stay through effective discharge/care planning by Quarter 4 2010-11 46% 10% reduction in readmissions Quarter 3 2010-11 21% 20% reduction in readmissions Quarter 4 2010-11 18% Quality priority End of Life Aim Rationale Objectives Achievement Increase in patients who are on an End of Life care pathway dying in their place of choice 50 - 60% of deaths occur in acute hospitals with patients experiencing an average of 18 days as an inpatient spread over 2 - 3 admissions in the last year of life. 50% of all patients on an End of Life care plan dying in their place of choice 97% And a reduction in hospital as place of death Approximately half of all complaints made to acute trusts relate to an aspect of end of life care. 40% reduction in hospital as place of death, where hospital is not the place of choice by Quarter 4 2010/11 Data not available 100% compliance with the urinary catheter Essential Steps Audits 98% 40% reduction in community acquired urinary tract infections Data not available The indicator incorporates questions which are known to be important to patients and where past data indicates significant room for improvement across England and is based upon the national indicator for acute trusts. 90% positive score across five questions by September 2011 100% Required by the Care Quality Commission 50% of all patients on Community Services caseload aged 65 yrs or over have received a dementia assessment by Quarter 4 2010-11 59% 50% of patients in crisis receive a response from a trained health professional within 1 hour - by Quarter 2 2010-11 68% 80% of patients in crisis receive a response from a trained health professional within 1 hour in Quarter 4 2010-11 86% A reduction in urinary tract infections through compliance with the Essentials of Care audits as required by the NHS Kirklees Infection Control Team to by NHS Kirklees Infection Control team. 60% of healthcare associated infections are related to catheter care. Patient Experience Surveys Improve the responsiveness to personal needs of patients Early Assessment of Dementia Early assessment and diagnosis of dementia to improve the quality of care for patients with dementia Reduction in Urinary Tract Infections Single Point of Access/Rapid Response Trained health professional response within one hour will lead to improved quality of care for and outcomes for patients in crisis Required by the Care Quality Commission Quality Account 2010/11 | Kirklees Community Healthcare Services 27 28 Kirklees Community Healthcare Services | Quality Account 2010/11 Section five: Statements 5.1 Statements from our Stakeholders 5.1.1 Kirklees Local Involvement Network No comments received. 5.1.2 Kirklees Wellbeing and Communities Scrutiny Panel The Well-Being & Communities Scrutiny Panel welcomes the opportunity to comment on Kirklees Community Healthcare Service’s Quality Account for 2010/11. The Panel has not had extensive involvement with KCHS during the last 12 months, although they have maintained a watching brief on the development of the community interest company (CIC). The Panel would like to see closer engagement in the coming months with KCHS as the CIC comes into being, particularly in respect of the implications for potential health service users. The Scrutiny Panel also hope to work more closely with KCHS over the next 12 months to develop their understanding of the actions being taken to address the priorities. 5.1.3 Kirklees Primary Care Trust No comments received. Quality Account 2010/11 | Kirklees Community Healthcare Services 29 5.1.4 Greater Huddersfield GP Commissioning Consortium We welcome the chance to comment on this first quality report and we do appreciate this is still early days for this new provider unit. The areas we would like to see worked on are as follows: We would like to see more work on clinical priorities. This would be best aimed at areas such as Children CAF, % patients on the Liverpool care pathway and nutrition plans. We feel the SPA needs to record outcomes rather than just times of response. We would like to know what actions have come from the complaints / significant events. How is this learning being incorporated into new ways of working. We look forward to working together in the future. 5.1.5 North Kirklees GP Commissioning Alliance No comments received. 5.2 How to provide feedback on this Quality Account If you would like to request a copy of this document in an alternative format or other language or have any queries about its content, please contact the Integrated Governance Team: Tel: 01924 351440 Email: gwen.ruddlesdin@kirkleeschs.nhs.uk This report is also available at www.kirkleeschs.nhs.uk 30 Kirklees Community Healthcare Services | Quality Account 2010/11 Quality Account 2010/11 | Kirklees Community Healthcare Services 31 June 2011