Quality Account 2009-2010
advertisement

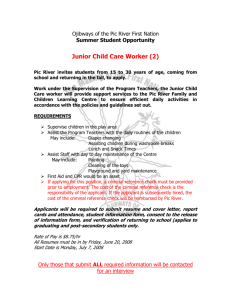
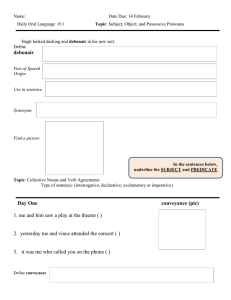
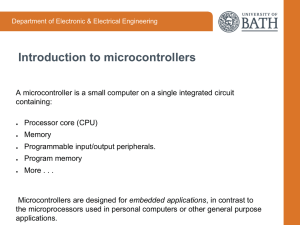
Quality Account 2009-2010 CONTENTS Page Corporate Statement 3 Care Quality Goals 3 Achievements 4 Moving Forward 17 Summary 20 2 Corporate Statement Partnerships in Care (PiC) aims to be the first choice Independent Sector provider of specialist mental health hospitals. Within PiC the needs of the patients always come first. In order to achieve this we have asked our patients to tell us what is important to them and from this have developed a set of patient priorities. We have promised to provide: Safe and secure hospitals The best clinical care delivered through defined care pathways Clean hospitals with good access to comfortable facilities Dignity and respect for patients Single sex accommodation We have a transparent and progressive approach in which we are always working to improve and develop our services. This Quality Account reports on how PiC has achieved against its stated aims and aspirations and the ongoing commitment and focus on these goals. PiC Care Quality Goals During 2009/10 consistently high quality care has been provided through: The continued delivery of high standards of patient safety by achieving the necessary standards as laid down by the Care Quality Commission (CQC) in England and those devised by the Quality Network for Forensic Mental Health Services. We continue to strive to improve our operational performance and in 2009/10 have declared compliance across all standards. Our ambition is to achieve year on year improvements Ensuring patients receive timely care by meeting company targets Continued retention of low assessment times with the majority of referred patients being assessed in four days Providing clean, modern and welcoming environments Further training to embed the Recovery Approach across all services Investments made in 2009/10 to refurbish a number of hospitals improving the physical security environments for patients, staff and the public 3 Ensuring we always provide patients with the best clinical care by fully considering the patient journey The establishment of the Corporate Clinical Governance Group during the year, which offers support to staff in developing and improving their services for the benefit of patients Closer working relationships with commissioners through: a stronger commissioner-facing team; the launch of an electronic newsletter produced specifically for commissioners; the development of a new website with advanced search function for commissioners Greater focus on recruitment and retention – strengthening the talent pool Continuing to improve internal communications across the Group, through centrally disseminated Team Brief an internal newsletters and further communication as necessary Establishing corporate departments and improving internal customer focussed services. A lot of work has been done in the year to review and adapt our corporate services to ensure that they are fit for purpose and provide better support to clinical teams. Staff have also worked closely with both clinical and non-clinical departments, using Lean principles to help departments work in a more efficient way Continual learning and development through training and attendance at relevant conferences Ensuring a financially sound organisation. PiC achieved a good financial position despite a challenging year for the majority of its hospitals and its competitors Achievements A number of incidences of significant improvement in performance can be evidenced as affecting quality of care delivery in positive ways. Patient Safety Patient safety is of particular consideration for PiC as a provider of secure care to the mentally disordered. We are committed to minimising risks and promoting a culture where improvements and lessons can be learned through experience. This commitment includes identifying actual and potential areas of risk through the reporting of adverse events and near misses. We have decided to focus on safety initiatives in a way that demonstrates improvement. A suite of ‘Key Safety Indicators’ [Absence without Leave; Seclusion; Self Harm; Medication Errors; Slips, Trips and Falls] have been identified and evidence is 4 collected, analysed and utilised to understand and improve on the safety of patients, staff and others in contact with our services. Chart One sets out number of occurrences against the indicators as compared to performance in the previous year. Charts Two (a) (b) offer a cumulative total of incidents but contrasts the numbers of those involving patients with those experienced by staff. Commentary A significant impacting factor on two of the key indicators has been the increased capacity across our service provision. The improvement of facilities and addition of bed numbers has seen a number of more disturbed patients coming into PiC care. The disruption created by the improvement of facilities whilst remaining in operation would have meant in some cases a change in routines and management approaches that potentially could have unsettled patients. The data shows a sizable increase in the number of male patients self harming and patients overall where seclusion was indicated as the most appropriate management tool. A self harm chart outlining staff interventions for patients who swallow objects has been developed at Arbury Court. This piece of work has been cascaded through the clinical governance leads at each hospital. Research papers on the ‘Ingestion of Foreign Objects & Cylindrical Batteries in Psychiatric Settings’ were also circulated. During 2010 the company is introducing the audit tool from the National Patient Safety Agency (Preventing Suicide: A toolkit for mental health professionals). This provides a comprehensive audit relating to ward management as well as addressing care pathway needs of individual patients. Medication errors should be an occurrence that can be minimised through good governance. The fall of incidents to 134 in 2009/10 is noted. Medication errors are reported as clinical incidents through the company’s incident reporting framework. These are reviewed locally by clinical and nursing teams and corrective action is taken to prevent similar incidents from occurring. Themes arising from clinical incidents are reviewed annually by the Health & Safety Committee. Each incidence of absence without leave is reported to the various government departments in accordance with regulation requirements. In addition each incident facilitates a Serious Untoward Incident review in accordance with company policy. Lessons to be learned are cascaded through the Corporate Clinical Governance Committee; Health & Safety Committee and the PiC Group Security Officer. 5 Chart One: Num bers Key Safety Indicators 5,270 5,120 4,970 4,820 4,670 4,520 4,370 4,220 4,070 3,920 3,770 3,620 3,470 3,320 3,170 3,020 2,870 2,720 2,570 2,420 2,270 2,120 1,970 1,820 1,670 1,520 1,370 1,220 1,070 920 770 620 470 320 170 20 5,139 4,098 1,439 1,039 414 497 134 172 29 50 2007 2008 2009 2010 Year Medication Errors Self Harm Seclusion Slips, trips and falls Escapes and Absconsions Chart Two: (a) Incidents 25,000 22,500 22,901 20,000 Numbers 17,500 18,092 15,000 Staff Patients 12,500 10,000 7,500 5,000 2,500 3,787 3,930 0 2007 2008 2009 2010 Year 6 (b) Injuries 6,000 5,000 4,773 Numbers 4,000 3,974 Staff 3,000 2,000 Patients 1,956 1,849 1,000 0 2007 2008 2009 2010 Year Clinical Governance The inaugural meeting of the Corporate Clinical Governance Committee took place in September 2009. Services continue to be encouraged to share best practice initiatives through the corporate clinical governance newsletter. Individual units continue to submit minutes of their clinical governance meetings to the Corporate Clinical Governance Manager. ‘A guide to clinical governance’ continues to be used to assess the structures that underpin clinical governance activity and benchmark services against statutory, policy and best practice clinical governance standards. The audit cycle runs from April to March and seven audits have been completed. Clinical Governance Newsletter The first Corporate Clinical Governance Newsletter covered Storytelling (how patients can use storytelling as part of meaning interaction that develops and enhances their creative skills) and an Anti- Bullying working party. It also reported on the Have Your Say patient satisfaction model and national changes including the introduction of the Care Quality Commission & Mental Health Development Unit as well as changes to the complaints policy for England. The second newsletter covered: changes to the Care Quality Commission, the 25 hours activity project, corporate clinical governance developments, bullying behaviours, clinical audit developments, and initiatives in services for people who have a personality disorder. 7 The third edition included a paper from Dr Pancho Ghatak (PiC Midlands) who cohosted a workshop on ‘Person Centred Planning in Secure Settings’ with Dr Susan Johnston at the Faculty of Learning Disabilities Annual Conference 2009. There is also a report on the availability of Multi-lingual leaflets on patients’ rights under the MHA (England only). These can be accessed through the Clinical Governance page on the Company’s intranet. Services continue to be encouraged to share best practice initiatives through this newsletter. Patient Involvement Some hospitals took up the offer of a presentation on clinical audit to the patients’ councils that served to standardise understanding. During 2009/2010 the company introduced a new model for patient surveys. The model has been benchmarked against national guidelines and also meets some of the criteria of Part 2 (Service User, Carer and Staff Experience Surveys) of Schedule 3 (Managing Activity and Referrals, Care and Resource Utilisation Techniques and Retention of Payment Scheme) of the standard NHS multilateral contract for mental health and learning disability services Following a period of consultation the patient satisfaction survey ‘Have Your Say’ was finalised during Quarter 2. The model consists of four separate patient satisfaction questionnaires. Namely: 1. 2. 3. 4. My CPA Meeting Your Environment – What I think of where I live Information - What I have been told My Care and Treatment The intention is for these to be completed at different times throughout the calendar year. This model aims to: Standardise the patient satisfaction questionnaires across the Company and all patient groups Make the questionnaires more service user friendly and more manageable for patients who have short concentration spans Increase the profile of patient satisfaction surveys and how feedback can be used to shape service delivery Reduce duplication in current reporting systems by using the data presented through these questionnaires in other linked audit projects, primarily CPA 8 To provide timely feedback to management teams on themes evidenced by patient experience Service users, family members and carers involvement PiC is committed to involving service users, family members and carers in developing our services. We do this by: Holding ward community meetings for patients Seeking feedback on current issues from patient representatives or councils Carrying out regular service user satisfaction surveys Regularly reviewing themes arising from formal complaints Minutes from patient’s council meetings are reviewed regularly by a senior governing committee at each hospital and action is taken to address issues raised Care Programme Approach (CPA) The document was designed to focus on the Care Pathway for the patient thus integrating individual professional reports. The process to evaluate the CPA document commenced in the last quarter of 2009 with questionnaires designed for clinical staff, Commissioners and Case Managers being circulated. All completed questionnaires were returned by 31st January 2010. There were a total of 113 returned staff questionnaires from 17 units. This ranged from 14 completed questionnaires at The Spinney with only 1 questionnaire being returned from Aderyn and Pelham Woods. Unfortunately only two responses were received from Case Managers and as one of these had only recently taken up post they did not feel qualified to comment. Three quarters of respondents felt the CPA document was laid out in a logical way, although only just over half reported that the document facilitates ease of access to information when needed and several believed the document to be unwieldy. A diverse range of responses was recorded on the remaining 16 questions leaving a number of recommendations for the Corporate Clinical Governance Committee to consider in completing the evaluation. 9 Physical Health check The Physical Health Check system and associated guidelines developed by Rethink were circulated through the Medical Directors Forum. It was decided that as all services have General Practice input that these documents would be made available to the relevant GP. Physical health promotion is also a component of the clinical governance audit. A corporate physical healthcare policy was produced during 2009 and circulated for comments. This policy was ratified by the CMG early in 2010. Referrals to Assessments PiC has set a standard that wherever possible assessments will take place within three days of referral. This standard was not achieved, which was largely due to the number of referrals received for people who were in prison. Access to prisons can be problematic, either through the restriction caused by security-related protocols or through PiC wishing to maintain its relationship with Commissioners, whereby some referrals are received without clear indication that they have been agreed by the Commissioning team. PiC would seek that clarification prior to arranging an assessment thereby prolonging the period between referral and assessment. Regardless of the above considerations PiC has still managed to achieve a credible average time of four days between referral and assessment. Despite the awareness of some blockages inherent to the process/system, PiC will retain the three days target during 2010/11 with the intention of addressing known inhibitors and further reviewing the target in the light of any additional emerging evidence. Targets should always be meaningful and achievable. 10 Chart Three: Infection Control The profile of infection control was raised across the company during the outbreak of swine flu using the 'Catch it, Bin it, Kill it' campaign. This was reinforced at the corporate Health and Safety meeting in May 2009 as well as the directive that Primary Nurses should be holding one to one sessions with patients to talk about general infection control issues. Some patients and staff within PiC were affected by the first outbreak and it is highly likely that this will be the case with a second wave expected in 2010. The strategy for pandemic influenza was circulated to the CMG at the beginning of the outbreak of swine flu. The strategy was ratified by the Corporate Management Group in 2009 and reflected 'A National Framework for responding to an influenza pandemic' as well as Department of Health Guidelines specific to mental health services. Regional Executive Directors continue to be responsible for overseeing the implementation of the strategy at a local level. Research and Audit The Clinical Governance Audit Tool aims to provide a corporate vision for the strategic development of Clinical Governance across the Company. It attempts to achieve this through setting and monitoring performance standards under the seven pillars of Clinical Governance bringing together a variety of cross company initiatives. The standards incorporate national guidance on clinical governance, PiCs operational policy and the Standards for Better Health issued by the Department of Health (DH). This strategy helps to identify the direction PiC is taking towards the delivery of its services. It is intended to be a living document and will evolve in response to new 11 initiatives and as lessons are learnt through implementation. Each hospital / service is audited against these standards at a minimum of once per calendar year. There have been a number of research papers published involving PiC clinical staff during the year. In addition the company continues to organise, sponsor and attend a large number and a wide variety of clinical conferences. Ligature Audit A ligature audit tool has been drafted and reviewed by the Corporate Clinical Governance Committee and will be trialled at two sites during 2010. Infection Control A self assessment audit tool has been developed for the Health and Social Care Act 2008. The implications for PiC are that all services registered with the CQC meet the standards in the guidelines by April 2010. The standards state that PiC will need a Director of Infection Prevention and Control (DIPC) who reports to the board annually. Initial scoping indicates that the management of infection control is currently fragmented across the group with non clinicians in some areas having sole responsibility. Following discussion it was proposed that infection control should be primarily nurse led and that the PiC Corporate Director of Nursing would integrate the role of the Director of Infection Prevention and Control with current responsibilities. This initiative will be taken forward through the Infection Control Group and fed through to the Director of Nursing forum. Patient Involvement Each hospital holds patient council meetings looking at all aspects of the patient experience throughout the hospital. Members of the local senior management team will be party to council meetings reporting their activity to SMT. The minutes and outcomes of patient council meetings are monitored through the corporate clinical governance audit. Seclusion The use of seclusion as part of managing violent and aggressive patients has been audited against the standards outlined in The Mental Health Act (1983) Code of Practice and Violence, and the short-term management of disturbed/violent behaviour in psychiatric inpatient settings and emergency departments (NICE Clinical Guideline 25). 12 The audit has been in three parts. Part A considers the physical layout and specification of rooms / facilities that may be used in the seclusion of patients. Part B examines the systems in place to support and regulate seclusion at local level, such as policies, procedures and training and Part C considers the quality of seclusion interventions and associated documentation, with regard to individual patient incidents. Slips, Trips and Falls Slips, Trips and Falls are reviewed quarterly by the Health and Safety Committee through the PiC Accident and Incident reporting process. Policies and Procedures In accordance with proper governance and in reflection of PiC’s commitment in responding to patient needs and prevailing evidence a range of policies, practices and procedures, and guidance notes were promulgated or reviewed during 2009. These all respect the expectations of its stakeholders. Examples of these are: 1. Clinical and Corporate Governance Clinical Audit January 2009 Legal Policy – Legal Claims July 2009 Guidance on Contracted Out Services July 2009 Nursing Patients in Isolation or Seclusion August 2009 Confidentiality Policy October 2009 Data Protection Policy October 2009 Sex & Violence March 2010 Complaints Policy & Procedure March 2010 2. 3. The Patients’ Experience/Journey Harassment March 2009 Policy for Working within the May 2009 Discharge – Leaving the Service June 2009 Human Resources 13 Retirement Policy March 2009 Employment of People from Overseas August 2009 Redundancy Policy September 2009 Recruitment and Retention Policy November 2009 Sickness Absence March 2010 Discipline and Appeals Policy March 2010 4. Health and Safety Control of Substances Hazardous to Health January 2009 PiC Health, Safety & Environmental Policy Statement October 2009 Environmental Management & Sustainable Development October 2009 Manual Handling 5. January 2010 Finance Company Credit Cards May 2009 Cheque Destruction Procedures June 2009 Care First Income Reconciliation Procedures June 2009 Compliance & Control Standards for Patient / Resident Monies August 2009 Finance Department Sage Users - Starters & Leavers September 2009 Capital Purchasing January 2010 Capitalisation Policy January 2010 Procedures for Budgeting & Budget Management January 2010 Care First Client Billing Procedures February 2010 Cash Book & Bank Reconciliation Procedures February 2010 Standing Financial Instructions March 2010 14 Staff Training and Supervision Governing bodies such as the General Medical Council (GMC), Nursing & Midwifery Council (NMC) and British Psychological Society (BPS) continue to emphasise that it is the individual practitioner’s responsibility to maintain their professional knowledge and competence. This is a requirement for revalidation or re-registration and should be monitored through the professional supervision and the appraisal process. Clinical and managerial supervision is an important element of staff development and PiC aims to see a consistent structured application across all its services. The vast majority of services have staff supervision programmes in place with others under direction to make supervision core to staff development. Achieving full uptake and the improvement of the co-ordination and evaluation captured data is an objective for PiC during 2010/11. Complaints The Company’s annual Complaints meeting involving all hospitals was held at Church Farm Lodge on Monday 6th April 2009, this is in addition to the meetings held at each hospital to review complaints handling and management. From 1st April 2009 the Parliamentary and Health Service Ombudsman and the Healthcare Commission (now CQC) became the public body for the complainant to appeal to if they are unhappy with the local resolution. (This only applies in England) The Ombudsman’s principles are: Getting it right; Being customer focused; Being open and accountable; Acting fairly and proportionately; Putting things right; Seeking continuous improvement. The Ombudsmen will adopt these principles when considering the standard of the complaint handling by the bodies within her jurisdiction. There are three publications where these principles are outlined. These are: 1. Principles of Good Administration 2. Principles of Good Complaint Handling 3. Principles for Remedy Corporate policy has been updated to reflect these changes and to integrate the standardised paperwork used across the group. In addition a PowerPoint presentation was drafted to standardise complaint training at the point of induction. The charts below denote the complaints activity for the year. Four (b) shows the average time taken to manage the two stages of complaints namely Acknowledgement (target 3 days) and Closure (target 28 days). 15 At tit ud eo fs taf Bu ft lly ow ing ar /h ds ar pa as tie sm Bu nt en lly t ing by /H p a ar tie as nt sm en tb yS ta ff Cli nic C om al En Ca vir pla re on int m sP en ro ta ce nd ss D do me iscri m sti i Le n Inf c( ga inc atio or lm n m lud att ati es er on ... s( /C inc om lud Lo m ss es un /D ica ac am ce tio ss ag n to eo r fP ec o ro rd p .. er M ty ed /V ica alu lC ab ar les ea nd Tr ea tm en t No tS ta te d Nu rsi ng C are Ph ys ica la ssa Ot ult he Ph r by ys pa ica t ien lA t ssa ult by Sta ff Pr iva cy /D Ra ign cia ity lH ara ss me nt Re str ain Se Se cu t xu rit y/ al Sa As fet sa ult y by Se Pa xu tie al As nt sa ult by St aff Number of Complaints Chart Four: (a) 160 150 140 130 120 110 100 90 80 70 60 50 40 30 20 10 0 Complaint Cate gory of Complaint Upheld Partially Upheld Not upheld Withdrawn Not deemed a complaint Passed To Other Referred to ward Ongoing (b) Formal complaints are reviewed regularly by the local Senior Management Team and action is taken to address any themes arising from these. In addition an annual complaint report is produced by the Company; this is reviewed by the Corporate Clinical Governance Committee. 16 Moving Forward PiC has identified nine priority areas for addressing and improving all aspects of care quality enhancing the patient experience and outcome. In support of these priorities a provisional list of specific activities has been set out below. Our Priorities for 2010/11: 1. Improve the patient experience 2. Further, strengthen the management of risk and patient safety – improved risk management at regional level and national Patient Safety First campaign launched across the Company 3. Improve clinical outcomes for patients – Quality Accounts established making information about quality and clinical outcomes available and focussing on improving the patient experience 4. Contribute to whole system recovery – improving care pathways 5. Improve financial management 6. Increase utilisation of high quality estates and reduced occupancy costs 7. Making better use of facilities 8. Improve Information Management and Technology to support executive decision making – delivery of the first year of electronic patient records strategy and benchmarking of service delivery costs to ensure we provide good value for money 9. Grow our referral base – implement plans to increase out patient base, improving working relationships with commissioners increasing the number of those choosing our hospitals 10. Further work with our units in the area of patient involvement, for example through patient involvement and engagement newsletters Clinical Engagement During 2009/10 Regional Services developed their own performance and quality standards, which include a range of quality indicators relevant to each region. These will be refined to meet the needs of patients, Commissioners and the NHS contract for 2010/11. The regions will receive regular reports on metrics relating to patient safety, patient experience, clinical effectiveness, use of agency staff and enhanced observation. The regions will use selected quality indicators to develop programmes for continuous quality improvement. 17 Services Development and Improvement Plan PiC will work together with the Commissioner to develop the Services Development and Improvement Plan (the “Plan”). The Plan is separate to the CQUIN scheme indicators set out in the NHS Contract. The key areas of the Plan are as follows: PiC will commence implementation of the DH’s Relational Security Guidelines (See, Think, Act) by the end of Q1 PiC will reviewing the CPA document to include a recovery plan for each patient by the end of the Q2 PiC will commence implementation of the electronic patient records by the end of Q3 PiC will develop a range of information to be distributed to carers for service improvement by the end of Q4 Medicines Management Each hospital is required to have in place the following: There is a policy in place on the Administration of Medication An up-to-date service level agreement with supplier of pharmaceuticals Audits o Lloyds Pharmacy carry out an annual audit on prescribing habits o Charge Nurse audits the medicine card on a monthly basis Proper prescription Check compliance with signatures Emergency 62 all paperwork Levels of use of PRN medication o Consent : T2 T3 All new employed first level nurses will undergo an eight week drug assessment prior to administering drugs to patients All first level nurses will undergo annual drug assessments (NMC) The Clinical Nurse Managers or equivalent is a member of the local intelligence network (LIN) BNF plus Mental Health Act Code of Practice are on each of the ward areas. Care Quality Commission – standards 2000 o Accountable officer for control drugs. A designated person on site usually the Registered Manager if a first level nurse NICE Guidelines o Prescribing and monitoring of drugs and their side effects including A Typical Anti-psychotic 18 Error Management o Database needs to be established to monitor all drug errors (establish what constitutes a drug error) o Train and support staff who have made errors prior to reassessment Secure Patient Activity Charter Each hospital will have to be able to evidence that their patients are being offered 25 hours of structured and meaningful activity per week. Each patient should have an individual timetable outlining the sessions offered to them on a weekly basis. This timetable should be reviewed at internal CPA meetings to ensure that the sessions are linked to direct patient care and treatment The named “Therapy Manager”, manages the timetable for each ward. Therefore, any clinician wishing to change or start sessions with individual patients need to approach this person so that the timetable is formalised The Therapy Manager will have an overview of the variety of sessions offered to the patients on each ward and site and this will be discussed with the Multi Disciplinary Teams to ensure the sessions are needs led and link to each individual care plan A database needs to be established and available on each of the wards computers to enable evidencing of sessions offered to the patient group All ward staff should have access to this database and be able to use this database effectively and in particular run off information for any visiting commissioner requiring information on their patients Training and coaching is carried out with staff using the database with the rationale of embedding this into the hospital culture At each CPA meeting including external meetings all data should be run off for each individual patient as part of the discussion of the patients care and treatment Service Management Teams for each service should be reviewing the level of activity for individual patients as part of their agenda Ideally one database should be used throughout PiC The responsible person for patient engagement for each site should carry out an audit every three months to ensure compliance Note: As a guide activity should be offered in the following areas: 30% Treatment 30% Education/Vocation 40% Recreation 19 SUMMARY The Quality Account represents an accurate reflection of Partnerships in Care’s achievements and priorities for improvement and progress towards its aspirations and commitment to the Patient Experience. Reporting on progress on elements of the account will be by way of the company’s governance processes as too will any changes in data that may emerge between the completion of the document and the reporting period. 20