Clinical Outcomes Following Manual Physical Therapy and Exercise for Hip
advertisement

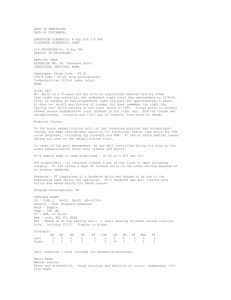
Clinical Outcomes Following Manual Physical Therapy and Exercise for Hip Osteoarthritis: A Case Series Cameron W. MacDonald, PT, DPT, GCS, OCS, FAAOMPT 1 Julie M. Whitman, PT, DSc, OCS, FAAOMPT 2 Joshua A. Cleland, PT, DPT, PhD, OCS, FAAOMPT 3 Marcia Smith, PT, PhD 4 Hugo L. Hoeksma, PT, PhD, MSc, MT 5 Study Design: Case series describing the outcomes of individual patients with hip osteoarthritis treated with manual physical therapy and exercise. Case Description: Seven patients referred to physical therapy with hip osteoarthritis and/or hip pain were included in this case series. All patients were treated with manual physical therapy followed by exercises to maximize strength and range of motion. Six of 7 patients completed a Harris Hip Score at initial examination and discharge from physical therapy, and 1 patient completed a Global Rating of Change Scale at discharge. Outcomes: Three males and 4 females with a median age of 62 years (range, 52-80 years) and median duration of symptoms of 9 months (range, 2-60 months) participated in this case series. The median number of physical therapy sessions attended was 5 (range, 4-12). The median increase in total passive range of motion of the hip was 82° (range, 70°-86°). The median improvement on the Harris Hip Score was 25 points (range, 15-38 points). The single patient who completed the Global Rating of Change Scale at discharge reported being ‘‘a great deal better.’’ Numeric pain rating scores decreased by a mean of 5 points (range, 2-7 points) on 0-to-10-point scale. Discussion: All patients exhibited reductions in pain and increases in passive range of motion, as well as a clinically meaningful improvement in function. Although we cannot infer a cause and effect relationship from a case series, the outcomes with these patients are similar to others reported in the literature that have demonstrated superior clinical outcomes associated with manual physical therapy and exercise for hip osteoarthritis compared to exercise alone. J Orthop Sports Phys Ther 2006;36(8):588-599. doi:10.2519/jospt.2006.2233 Key Words: arthritis, Harris Hip Score, manipulation, mobilization, passive range of motion 1 Physical Therapist, Centennial Physical Therapy, Colorado Sport and Spine Centers, Colorado Springs, CO; Fellow, Manual Physical Therapy Fellowship Program, Regis University, Denver, CO. 2 Assistant Professor, Department of Physical Therapy, Regis University, Denver, CO; Faculty, Manual Physical Therapy Fellowship Program, Regis University, Denver, CO. 3 Assistant Professor, Department of Physical Therapy, Franklin Pierce College, Concord, NH; Physical Therapist, Rehabilitation Services, Concord NH; Fellow, Manual Physical Therapy Fellowship Program, Regis University, Denver, CO. 4 Associate Professor, Department of Physical Therapy, Regis University, Denver, CO. 5 Professor, Department of Rehabilitation and Health Services, St Antonius Hospital, Nieuwegein, The Netherlands; Physical Therapist, Clinical Epidemiologist, Manual Therapy Certified, Netherlands Institute for Health Services Research, Utrecht, The Netherlands. This project is attributed to Centennial Physical Therapy, CSSC and the Regis University Fellowship Program in Orthopedic Manual Physical Therapy, Denver, CO, and received approval from the Institutional Review Board at Regis University, Denver, CO. Address correspondence to Dr Cameron MacDonald, Centennial Physical Therapy, Colorado Sport and Spine Centers, 5731 Silverstone Terrace #120, Colorado Springs, CO 80919. E-mail: physiocam@adelphia.net 588 O steoarthritis (OA) of the hip is described as a progressive loss of hyaline cartilage within the hip joint, sclerosis of subchondral bone, and the formation of bone spurs at the joint margins.2,18,34 Hip OA has been identified as a major cause of disability, with a prevalence of 10% to 20% in the aging population.20,52 When viewed as a predictor of functional disability, the overall condition of OA ranks fourth among women, and eighth among men.7,20,52 In addition to the personal disability associated with the disorder, OA also has a significant economic impact on the healthcare system. In the United States it is estimated that the number of people with OA in any region of the body will increase from 43 to 60 million by 2020, resulting in an estimated cost of over 100 billion healthcare dollars per year.20 Considering the personal and economic impact of OA, and the currently accepted ‘‘standard of care’’ for hip OA reported as joint replacement surgery,46 interventions with the potential to limit the disability and/or slow the progression of hip OA, potentially Journal of Orthopaedic & Sports Physical Therapy J Orthop Sports Phys Ther • Volume 36 • Number 8 • August 2006 TABLE 1. American College of Rheumatology criteria for classification of hip osteoarthritis. Referenced from Altman R et al.1 Cluster 1 used in this case series. Test Cluster 1 All 3 findings need to be present for diagnosis of patient with hip osteoarthritis • Pain reported in the hip • 115° hip flexion • 15° hip internal rotation CASE REPORT delaying or decreasing the number of joint replacements, demand further attention. Hip OA typically presents clinically as pain in the groin, lateral hip, and the medial thigh regions, sometimes extending distally to the knee.43 Patients with OA of the hip often experience morning stiffness, loss of motion, and pain with weight bearing on the affected limb.40,72 These impairments are often correlated with a loss of function, such as difficulty raising from a low chair, bathing, dressing the lower extremities, and ascending and descending stairs.47 The current American College of Rheumatology (ACR) guidelines for hip OA focus on pharmacological and surgical management.30 The role of exercise therapy is acknowledged, 3 but manual physical therapy (MPT) is not recognized in the most recently updated guidelines.29 Systematic reviews have concluded that exercise reduces pain and disability in patients with hip OA,59,68 but these benefits have been shown to yield only a moderate effect that typically regresses by 24 to 52 weeks following cessation of exercise therapy.70,71 With the side effects associated with medications prescribed for patients with hip OA (nonsteroidal anti-inflammatory medications), including gastrointestinal bleeds and cardiovascular disease,6,22,73 it seems reasonable to conclude that the roles of nonpharmocologic and noninvasive therapies, such as MPT, should be further explored. Research on the use of MPT in the treatment of hip OA is limited. In a recent literature search of electronic databases using Medline, OVID and Pedro, we identified only 2 references reporting the use of MPT techniques for patients with hip OA.34,48 First, Loudon48 reported on the use of MPT and exercise to treat a patient with hip OA. The author proposed that the benefits of the mobilization/manipulation (thrust and nonthrust) facilitated a return of function, which potentially could have prevented the need for a total hip arthroplasty (THA). The inherent limitations of a case report, however, do not allow for the identification of a cause-and-effect relationship. More recently, Hoeksma et al34 published the results of a randomized clinical trial comparing the effectiveness of 2 different therapy programs in a group of patients with hip OA. The results of this trial demonstrated the superiority of MPT plus exercise over exercise alone for improving pain and range of motion (ROM). A clinically meaningful difference was also found in favor of the MPT-plus-exercise group in function, as measured on the Harris Hip Score (HHS).34 In addition, these improvements were maintained at the time of the 6-month follow-up. Recently the Ottawa Panel for evidence-based clinical practice reviewed the role of exercise and MPT in the treatment of OA in general (not joint specific), and found that further research is needed on the individual effects of MPT for patients with OA.54 Test Cluster 2 Alternate cluster for diagnosis if all 3 findings are present • Pain with hip internal rotation • 60 minutes morning stiffness • 50 years of age Considering the limited published reports investigating the effectiveness of MPT in the management of hip OA, and the findings of the Ottawa Panel,54 a case series reporting clinical decision making and outcomes of patients treated with MPT and exercise is of value to the research literature. In particular, a case series allows for the presentation of the clinical decision-making process based on the best available evidence for treatment selection, rather than a stringent, predetermined protocol of interventions often used in large clinical trials. The purpose of this case series is to describe the clinical decision making used to treat a series of patients with hip OA, to report the clinical outcomes achieved by these patients, and to demonstrate the implementation of evidence-based practice into clinical patient care.34,61 CASE DESCRIPTIONS Patients referred to physical therapy with a diagnosis of hip OA or a primary report of hip pain, meeting the ACR classification for hip OA (Table 1),1 were screened to determine eligibility for participation in this case series. Satisfaction of the ACR guidelines, which are considered the diagnostic standard for hip OA in rheumatologic medicine, yields a positive likelihood ratio of 4.4 to 5.0, indicating a moderate shift in probability that the patient presents with hip OA.1,5,11,13 Further inclusion and exclusion criteria for this case series are listed in Table 2. A total of 7 patients satisfying all inclusion and exclusion criteria participated in this case series. Five were treated at Centennial Physical Therapy, Colorado Springs, CO, 1 patient was treated in The Hague, The Netherlands, and 1 in Concord, NH. This study was approved by the Institutional Review Board at Regis University, Denver, CO. Patient privacy, patient consent, and compliance with Health Insurance Portability and Accountability Act (HIPAA) guidelines was maintained through the course of this case series for patients treated in the United States, 58 9 TABLE 2. Inclusion and exclusion criteria. Inclusion Criteria • • • Referral to physical therapy with a diagnosis of hip pain or hip osteoarthritis 50-90 years of age Meet ACR classification for hip osteoarthritis Exclusion Criteria • Prior hip surgery • • Patient refusal of mobilization/manipulation techniques Clinical exam consistent with nonmusculoskeletal etiology of symptoms (malignancy, infection, etc) Rheumatoid arthritis Severe low back pain Recent spinal or knee orthopedic surgery Radicular pain below the knee* Osteoporosis • • • • • Abbreviation: ACR, American College of Rheumatology. *Radicular pain was defined as presenting with radiating pain into the lower extremity, in a recognized dermatomal path, consistent with pain primarily of spinal origin and not from the hip. TABLE 3. Patient demographics and outcomes at baseline. Patient Age (y) Sex Involved Hip 1 2 3 4 5 6 7 53 52 66 62 59 80 76 M M F F F M F Right Left Right Left Left Right Left Symptom Duration (mo) 60 9 36 9 3 2 9 with appropriate patient privacy maintained per institutional standards in The Netherlands. Examination have been shown to be reliable, and the summation of hip PROM (including flexion, extension, abduction, and internal and external rotation) has been shown to be valid in comparing total hip PROM between subjects.36 Because a loss of strength is purported to be a consequence of hip OA, and a potential cause of functional impairments, we believe that addressing strength deficits may be an important component of a rehabilitation program for this population.1,16,19,59,62 MMT was utilized to assess the major muscle groups of the hip. MMT has been reported to have good reliability (82% interrater agreement,55 = 0.6757) and validity for assessment of the hip extensors and flexors; however, no reliability data for measurements of hip abduction or rotation have been reported in the literature. The specific techniques for MMT of the hip are consistent with those reported in Magee.49 Techniques used to determine joint impairments included the assessment of hip joint end feels and evaluation of hip joint accessory motion.38,49,50 The interexaminer reliability of hip joint mobility through manual assessment has been reported to be good to excellent for pain provocation in flexion and internal rotation ( = 0.88 and 0.74), and fair to good without pain provocation, but the reliability of specific assessment of passive accessory mobility of the hip joint is unknown.8 Gait assessment was also included in this case series, with visual observation of the trunk, pelvis, and lower extremities during ambulation on a level surface. Deviations from normal hip and pelvic motion were recorded individually, with attention to a visible Trendelenburg sign, antalgic gait, or an altered step length.9,66 Outcome Measures Patients completed a number of baseline self-report questionnaires, followed by a comprehensive history and physical examination. The historical examination included patient age, sex, duration of symptoms, location and nature of symptoms, aggravating and easing positions or activities, occupation, symptom irritability, recreational and leisure activities, patient goals, medical history, and past surgical history. Baseline variables for all patients are shown in Table 3. The physical examination included a postural assessment,42 neurological assessment,44 hip passive range of motion (PROM) measurements, manual muscle testing (MMT) of the lumbopelvic, gluteal, and hip musculature,42,53 and assessment of passive accessory mobility of the hip joint.8,45,50 PROM was assessed using a standard dual-arm goniometer for hip flexion, abduction, internal/external rotation, and extension. Goniometric measures of hip PROM PROM, numeric pain rating score (NPRS), and a measure of disability (HHS) was collected at baseline. PROM and pain scores were included because these factors have been shown to be significantly associated with the disability experienced by those with hip OA.69 The NPRS was collected at the baseline examination and weekly thereafter until discharge. Patients were asked to report the highest level of pain experienced over the last 24 hours on a 0-to-10 scale, with 0 representing no pain and 10 the worst pain imaginable. Previous studies have demonstrated adequate reliability and validity for this type of NPRS, and a 2-point change has been reported to represent clinically meaningful change.10,23 Patient-perceived levels of disability were measured with the HHS (Table 4). The HHS is a 10-item functional assessment tool yielding a score of up to 100, with lower scores representing greater amounts of disability and 590 J Orthop Sports Phys Ther • Volume 36 • Number 8 • August 2006 TABLE 4. Outcome measure: Harris Hip Score. Referenced from Harris.28 Category Points 44 40 30 20 10 0 Case Presentations a 4-point change indicating clinically meaningful change.28,32 This questionnaire has been shown to be reliable in a patient population with hip OA and is All 7 patients included in this case series exhibited a loss of both passive hip flexion and internal rotation.45 Table 5 presents the initial PROM and NPRS and lists the initial examination ACR classification1 for each patient. Every patient presented with weakness of the hip external rotators and hip abductors on the affected side. Variable muscle weakness between patients was also identified in the ipsilateral hamstrings, hip extensors, and quadriceps. Muscle performance of the trunk and core (including the deep abdominal muscles) was examined to identify any primary control or muscle capacity deficits that may have indicated the need for interventions targeting these impairments.31 Specific individual examination findings for each patient participating in this case series are described in detail below. Patient 1 A 53-year-old, 100-kg male with a diagnosis of right hip pain and a 5-year history of pain and mobility limitations reported a progressive decrease in the ability to participate in bike riding and golf. In addition to the common findings for all patients previously described, this patient’s pain was reproduced with passive internal rotation of the right hip. Additionally, the patient exhibited an antalgic gait pattern and decreased step length on the right side. Patient 2 A 52-year-old, 83-kg male with a 9-month history of left hip pain reported increasing difficulty ascending and descending stairs, walking, and getting into and out of his car. The patient demonstrated a Trendelenburg gait pattern on the left side, indicating weakness of the left gluteus medius muscle.56 Additionally, he reported pain in the left hip region with a full squat and exhibited strength deficits in the left hamstrings (4/5) and gluteus medius (4/5) muscles. Patient 3 A 66-year-old female (body mass not reported) diagnosed with right hip OA and a progressive loss of functional status, reported that she had previously completed a bout of physical therapy (PT), which included functional and active exercises. According to the patient, this type of treatment was not beneficial in improving her function or disability level. She did not recall receiving any MPT. This patient exhibited decreased right hip extension during gait and reported being unable to ascend stairs comfortably. Patient 4 A 62-year-old, 73-kg female with a diagnosis of left hip pain reported a 9-month history of J Orthop Sports Phys Ther • Volume 36 • Number 8 • August 2006 591 5 4 2 11 8 5 0 11 7 5 4 2 0 11 8 5 2 0 4 2 1 0 4 2 0 5 3 0 1 0 4 0 Total score: /100 *ROM: no specific instructions for definition of partial ROM were available at the time of this case series for the HHS. For the purposes of this study, partial ROM was when either hip flexion was ⬍115° or internal rotation was ⬍15°. If both limitations were present this was scored as limited ROM. † Deformity: the presence of 1 of the following 4 deformities led to a 0 score in this category: less than 10° abduction, leg length discrepancy ⬎3.18 cm, flexion contracture ⬎30°, or leg fixed in ⬎10° internal rotation in extension. CASE REPORT Pain None Slight, occasional Mild, normal activity Moderate, activity concessions Marked, severe concessions Totally disabled Range of motion (ROM) Full Partial* Limited* Gait/limp None Slight Moderate Unable to walk Gait/support None Cane for long walks Cane, full time Crutch Two canes Unable to walk Gait/distance Unlimited 6 blocks 2 or 3 blocks Indoors only Bed and chair Function/stairs Normal Normal with banister Any method Unable Socks and shoes Easy With difficulty Unable Sitting Any chair 1 hour High chair 1⁄2 hour Unable to sit 1⁄2 hour Public transport Able Not able to use Deformity† Absence of all 4 Presence of 1 utilized as a primary outcomes tool for clinical research involving patients with hip OA.32,34,35,65 Radiographs were not used to guide clinical decision making in this study, as the relationship between radiographic presentation and disability from hip OA is variable and has not been shown to be predictive of response to MPT interventions.15,33,40,58 TABLE 5. Baseline measurements and ACR classification. From Altman et al.1 Patient 1 2 3 4 5 6 7 PROM Flex (deg) PROM IR (deg) NPRS Score* Meet ACR Hip Classification? 95 89 100 80 90 98 95 0 12 0 0 2 12 2 6 8 6 7 9 5 6 Yes Yes Yes Yes Yes Yes Yes Abbreviation: ACR, American College of Rheumatology; IR, internal rotation; NPRS, numeric pain rating scores; PROM, passive range of motion. *Pain was reported verbally by the patient on a 10-point NPRS, recording the worst pain felt over the last 24 hours. Zero represents no pain, with 10 as the worst pain imaginable progressive pain and dysfunction in the left hip. She reported sharp pain upon upright stance that radiated into the anterior left thigh and difficulty with functional and recreational tasks, including driving and skiing. The patient exhibited a left antalgic gait with decreased step length and no extension beyond 15° of flexion of the left hip. She reported that pain was most severe with supine passive left hip flexion. Patient 5 A 59-year-old, 70-kg female with a diagnosis of left hip OA reported left hip pain, with radiation down the medial thigh to the knee. A prior history of left buttock and low back pain was treated with chiropractic care, which resulted in mild improvements in these symptoms. Through observation of the patient’s gait, the therapist visually noted excessive pronation of the left midfoot. A valgus deformity was also noted at the left knee. Pain was most severe with passive left hip internal rotation. Patient 6 This patient was an 80-year-old, 75-kg male with a 10-week history of right hip and leg pain and a diagnosis of right hip OA. He reported difficulty with walking, pain on weight bearing, and loss of function. A hip scour test was positive for primary pain in the right hip.38,49 Patient 7 A 76-year-old, 61-kg female referred to PT with a diagnosis of bilateral hip degenerative joint disease greater in the left than the right hip. The patient reported the left hip pain resulted in a loss of function, as she was unable to complete gardening and was restricted in daily activities due to the left hip. Weakness was present bilaterally, but greater in the left abductors and external rotators (3+/5) compared to 4+/5 on the right side. No specific treatment was completed on the right hip. TABLE 6. Hip mobilization/manipulation techniques. Supine • • • • • • • Long-axis nonthrust oscillations in slight abduction Progression of above into abduction Nonthrust lateral glides of femur with a belt Lateral glides with combined rotations Long-axis thrust mobilization/manipulation in a loosepacked position Thrust mobilization/manipulation in less abduction (⬎15°) Hip flexion nonthrust inferior glides Sidelying • • • Anterior femoral nonthrust mobilization/manipulation Hip distraction with nonthrust medial femoral glide Hip distraction nonthrust medial glide plus abduction Prone • • Anterior nonthrust femoral glides Anterior nonthrust glides in figure-four position Three physical therapists completed all examinations and patient interventions in this case series. Five patients were treated by the primary author (C.M.), a physical therapist with over 10 years of clinical practice, 1 patient by a physical therapist (J.C.) with more than 5 years of clinical practice, and the final patient by a physical therapist (H.H.) with more than 10 years clinical practice. A summary of the techniques used in this case series is presented in Table 6. The MPT methods for addressing joint mobility were determined by the treating therapist and based on the clinical examination of each respective patient. We recognize that there is no reported reliability or validity of these techniques that might assist in selecting particular treatment interventions in MPT; however, each clinician used these techniques to guide the clinical decision making regarding the direction and magnitude of joint mobilization/ manipulation in each patient case, and whether to use thrust or nonthrust mobilization/manipulation techniques.4,38,49,50,63 Thrust mobilization/manipulation techniques were performed where a significant restriction in capsular end feel was identified in comparison to the contralateral side or where, in the judgment of the treating PT, there was an abnormally hypomobile ‘‘capsular’’ end feel when bilateral hip involvement was present. Thrust mobilization/ manipulation was not performed in the presence of a normal end feel when the hip was tested with a caudal distraction.14,38 Mobilization/manipulations were performed in the direction of identified restric- 592 J Orthop Sports Phys Ther • Volume 36 • Number 8 • August 2006 Interventions Description/Rationale of Selected Techniques The following techniques are described as they were most frequently implemented in this case series, along with the clinical decision making for their utilization. Nonthrust Long-Axis Oscillation Mobilization/ Manipulation This technique was used with the intent of encouraging relaxation of the muscles of the hip, decreasing tension in the soft tissues of the hip, and improving the elasticity of the joint capsule.18,51 This technique was utilized on all subjects at the beginning of treatment. A failure of this technique to restore capsular mobility was an indication to use thrust mobilization/manipulation techniques for patients treated in this case series. For this technique, the patient was supine, with the contralateral limb flat and slightly abducted or flexed at the hip and knee, based on patient comfort. Gentle and progressive long-axis distraction oscillations were performed by the therapist, with a 2-handed hold at the ankle as shown in Figure 1. Oscillations in this case series were repeated grade II or III nonthrust mobilization/manipulations with a progressive increase in intensity.50 Every attempt was made to ensure patient comfort and, if needed, the therapist performed the same technique with the hands above the knee. Progression of the distraction position into more abduction was utilized as motion improved to gain further ROM. Hip Joint Thrust Mobilization/Manipulation This technique was used with the intent of creating temporary relaxation of the muscles of the hip, decreasing tension in the soft tissues of the hip, and improving J Orthop Sports Phys Ther • Volume 36 • Number 8 • August 2006 the elasticity of the joint capsule, allowing for progression of mobility with other techniques.18,51 Thrust mobilization/manipulation was utilized on every patient in this case series. The thrust mobilization/manipulation of the hip joint was performed in a manner very similar to the techniques described by Hoeksma et al.34 It was initially performed in a position of approximately 30° abduction and slight flexion, and was progressed into less abduction (not less than 15°) and internal rotation of the hip to gain further capsular flexibility and to potentially decrease intra-articular pressure.18,51 Patient positioning was the same as for long-axis nonthrust mobilization/manipulations (Figure 1) and the technique was adjusted to address the direction of restriction identified by the treating therapist for each individual patient’s hip. In this case series, no specific number of thrust mobilization/ manipulations was utilized during each session, but clinical assessment following each thrust mobilization/manipulation was utilized to determine a change in joint end feel, and thrust mobilization/ manipulations were repeated based on the judgment of the treating physical therapist with consideration to the success of intervention and patient comfort. Sidelying Nonthrust Medial Mobilization/Manipulation This technique was intended to promote medial and inferior articular mobility of the femoral head in the acetabulum, with the ultimate goal of improving hip abduction and internal rotation. This technique was utilized by the primary author (C.M.) on 5 patients in this case series. Lateral nonthrust mobilization/ manipulation of the hip joint with a belt, as shown in Figure 2, was also used for the intent to improve hip abduction and internal rotation. As shown in Figure 3, a 2-person sidelying medial nonthrust mobilization/manipulation combined with distraction was utilized. The distraction force was first FIGURE 1. Long-axis nonthrust mobilization/manipulation of the hip in 15° to 30° abduction and 15° to 30° flexion. 593 CASE REPORT tions, with immediate reassessment of PROM and joint mobility to determine changes occurring after administration of the interventions. This was performed based on the clinician’s belief that intrasession changes would be predictive of a positive overall outcome given the recent reports on the positive predictive value of intersession changes for MPT interventions to the spine.26,67 Nonthrust mobilization/manipulations in this case series are defined as repetitive passive movement of varying amplitudes and of low velocity, applied at different points through the range of motion, depending on the effect desired.25 Thrust mobilization/ manipulation is defined as small-amplitude, highvelocity therapeutic movements of a joint.4 We are unaware of any reported adverse effects associated with hip nonthrust and thrust mobilization/ manipulation. However, Hoeksma et al34 reported that if osteophytes were noted on radiographs of the hip, they performed hip thrust mobilization/ manipulations with the hip in greater than 15° of abduction, theoretically to avoid acetabular impaction.34 active contraction by the patient of the external rotators of the hip, with the intent of increasing the anterior glide of the femur through the contraction of the muscles across the posterior aspect of the hip joint (Figure 5). The combination of nonthrust mobilization/manipulation with active contraction by the patient was also used on a limited basis for the lateral gapping mobilization/manipulation combined with internal rotation in this case series (Figure 2). Treatment progression for each patient focused on frequent reassessment (both intrasession and at the end of each session of MPT) of joint accessory motion and PROM by the treating clinician.24,38,39,64,74 Where a restriction in hip joint mobility was still perceived by the treating therapist, FIGURE 2. Lateral nonthrust mobilization/manipulation of the hip with a belt, combining a lateral femoral glide with internal rotation. FIGURE 3. Two therapist caudal hip nonthrust mobilization/ manipulation with combined medial and inferior glide. One therapist (not visualized here) distracts the hip while the other therapist provides a medial glide to the hip. FIGURE 4. Anterior hip nonthrust mobilization/manipulation in modified figure-four position, allowing for less available abduction (knee on stool). applied, then a medial and inferior translation of the femoral head was provided by the second therapist, individualized to each patient based upon restrictions in motion detected by the examiner and progression of the treatment program. The technique was most often an oscillatory glide at the middle to end of range of osteokinematic motion, with the end range being the passive limit of available hip motion in a given direction at the point of first restriction.14 Prone Figure-Four Nonthrust Mobilization/Manipulation With Knee off Table We used this technique with the intent to improve anterior femoral glide, ultimately with the goal of improving physiologic hip extension and external rotation. This technique was utilized for 5 of 7 patients in this case series. Figure 4 shows the patient positioning and therapist hand placement for a prone anterior glide of the femoral head. The knee was placed off the table to allow for the technique to be completed where there was a restriction in abduction of the involved hip. This technique was also used in conjunction with an FIGURE 5. Anterior hip nonthrust mobilization/manipulation, using an active contraction of the hip external rotators to assist with the anterior glide. The patient actively pushes the knee into the therapist’s hand, facilitating a contraction, as the therapist mobilizes the femur anteriorly with the proximal hand (dashed line represents direction of push from patient’s muscle contraction). 594 J Orthop Sports Phys Ther • Volume 36 • Number 8 • August 2006 appropriate nonthrust and thrust mobilization/ manipulative interventions were continued. Joint MPT interventions were ceased once assessed joint end feel was considered normal, PROM equaled the contralateral side, no further progression could be made secondary to patient complaint of pain, or there was no noted progression following repeated mobilization/manipulations (3 sessions without change). Following mobilization/manipulation, patients were prescribed exercises, which were determined individually based upon the outcomes of their evaluation. Exercises were chosen primarily to strengthen the hip external rotator and abductor musculature, given the examination findings of consistent lateral hip weakness in these muscles for each patient. A home exercise program was established for each patient, with the most frequently prescribed exercises and hip stretches listed in Table 7. In general, exercises were completed in 3 sets of 10 repetitions without weight, then progressed with the addition of weight up to 4 kg as a maximum for gluteus medius training in hip abduction and external rotation with the knee flexed to 90° and the hip flexed to 45°. Patients were discharged from PT care if there was a plateau in improvements in pain and PROM, or once the patient reported 0/10 NPRS with an ability to continue home exercises independently. One patient did not complete the HHS at the initial evaluation; therefore, he was asked to complete a Global Rating of Change (GROC) at the time of discharge.10 This scale is a 15-point Likert scale ranging from a very great deal worse (–7), to no change (0), to a very great deal better (+7), with changes greater than +3 indicating a moderate change in patient status.37 OUTCOMES Hip flexion: baseline Hip flexion: discharge 130 120 Degrees • • • • Upright bicycle: 10 min Gluteus medius clamshell exercises: 3 sets of 12 Hip abduction in sidelying: 3 sets of 12 Core transverse abdominus: 2 sets of 20 in supine with hips flexed to 45° Bridge with straight leg raise: 3 sets of 10 Hip flexor stretch kneeling or sidelying: 30 sec × 3 Single leg balance: up to 60 sec Tandem stance eyes open or closed: up to 60 sec 110 100 90 80 70 60 1 2 3 4 Patient 5 6 7 FIGURE 6. Patients’ hip flexion passive range of motion as measured at baseline and at discharge. Hip IR: Baseline Hip IR: Discharge 30 25 20 15 10 5 0 The total number of PT visits ranged from 4 to 12, with a median number of 5 visits over a 2- to 5-week period. All 7 patients demonstrated and reported improvements in pain, hip mobility, and disability status over the course of PT care. The specific changes in patient hip flexion PROM, hip internal FIGURE 7. Patients’ hip internal rotation (IR) passive range of motion at baseline and discharge. Note: patients 1 and 3 had 0° hip IR at baseline. J Orthop Sports Phys Ther • Volume 36 • Number 8 • August 2006 595 1 2 3 4 Patient 5 6 7 CASE REPORT • • • • rotation PROM, total joint PROM, HHS, and NPRS are shown in Figures 6 through 10. The median improvement in total hip ROM was 82° (range, 70°-86°), the median improvement in pain on the NPRS was 5 points (range, 2-7 points), and the median improvement in disability on the HHS was 25 points (range, 15-38 points). Each patient in this case series progressed from meeting the ACR classification criteria for hip OA at examination, to not having the identified impairments for classification at discharge. Each patient registered clinically meaningful changes in hip ROM, hip pain, and hip function. Individual significant functional changes were a return to golf for patient 1, an ability to return to skiing by patient 4 immediately following participation in this case series, and a return to gardening by patient 7. Although long-term outcomes were not collected formally, the primary author of this study (C.M.) contacted 5 of the patients in this case series. Patient 1 reported no change in discharge (DC) status at 6 months post-DC, but sought further MPT care 15 Degrees TABLE 7. Home exercises. Exercises were commenced following manual physical therapy in the clinic, and progressed into home programs individualized to each patient. Completed 1 to 2 times per day. not require further care at 6 months post-DC. Two of these patients reported 100% function at 6 months, and one 80% improvement at 3 months and again at 6 months post-DC. Patient 4 continued to receive intermittent private care for hip MPT and was discharged from all PT care 6 months post-DC from this case series, with further functional gains in PROM and activity levels. Total Hip PROM: Baseline Total Hip PROM: Discharge 300 Degrees 250 200 150 100 DISCUSSION 50 1 2 3 4 5 Patient 6 7 months post-DC for symptoms at a lower intensity than those present initially (NPRS score, 2/10; initial was 6/10 with 0/10 at DC). Patients 5, 6, and 7 did This case series describes the rationale and clinical decision making regarding the incorporation of MPT and exercise into the treatment of hip OA. Patients receiving MPT interventions based upon the clinical examination, including directional nonthrust mobilization/manipulations and thrust mobilization/ manipulations of the hip demonstrated similar outcomes to the patients of the Hoeksma et al34 randomized clinical trial who received MPT and exercise. Significant changes in function as measured through the HHS and decreases in pain as recorded in the MPT group of the Hoeksma et al34 trial were also noted in this case series. This case series demonstrates the incorporation of the best available evidence into clinical practice for the use of MPT and exercise in the treatment of patients with hip OA. The fact that each patient satisfied the ACR classification for hip OA at initial examination, but not at discharge, also suggests a positive outcome for the patients in this case series. The primary impairments identified in the ACR guidelines may have been influenced by MPT.1 Improvements in PROM in flexion and internal rotation were the primary outcomes that changed the diagnostic classification of the patients in this case series. The specific MPT techniques described in this case series serve to illustrate potential primary interventions for patients with hip OA. The treatments in this case series were not based on a specific predetermined set of planned interventions or protocol but, rather, on the clinicians’ individual patient assessment of deficits in PROM, end feel, and loss of joint motion as perceived through manual joint assessment. The apparent success of manual interventions for hip OA promotes the potential of a decreased reliance on pharmaceutical management, improved quality of life, decreased pain, and decreased personal and community costs associated with hip OA.7,41,52 Medication usage was not recorded in this case series, and was not noted to be recorded in previous reported studies of MPT involving the hip.12,34 The rationale for this type of treatment approach in the management of hip OA is to restore functional motion to the hip, allowing for an increase in exercise participation and to potentially improve the nutrition and tissue health of the hip joint.18,35,39,51 596 J Orthop Sports Phys Ther • Volume 36 • Number 8 • August 2006 FIGURE 8. Patients total hip passive range of motion (PROM) at baseline and discharge. PROM includes flexion, extension, internal rotation, external rotation, and abduction. Baseline Discharge Harris Hip Scores (Range 0-100) 100 80 60 40 20 0 1 2 3 4 5 Patient 6 7 FIGURE 9. Harris Hip Scores (HHS) from evaluation and discharge, 0 represents total disability, 100 represents normal hip function and mobility. Minimum clinically important difference (MCID) for the HHS is 4 points (Hoeksma et al35). Patient 2 did not complete a HHS. Baseline Discharge NPRS (Range 0-10) 10 8 6 4 2 0 1 2 3 4 Patient 5 6 7 FIGURE 10. Patients reported maximal pain levels in the previous 24 hours, using a numeric pain rating scale (NPRS) where 0 represents no pain and 10 the worst pain imaginable. The minimum clinically important difference (MCID) for patients with low back pain is 2 points (Childs10). Patients 1 and 3 reported a 0 score on the NPRS at discharge. J Orthop Sports Phys Ther • Volume 36 • Number 8 • August 2006 and whether specific joint testing is necessary to guide mobilizations, or if general application of mobilization/manipulation to the hip will provide benefits in pain and disability for patients with hip OA. Future studies should also inquire into the usage of medications following MPT interventions for hip OA and identify the duration of long-term benefit following MPT for hip OA. CONCLUSIONS This case series highlights the use of nonthrust and thrust mobilization/manipulative techniques and exercise in the treatment of hip OA from an impairment-based MPT approach. Loss of PROM and pain in the hip formed the basis of the medical diagnosis in this case series, while restrictions in PROM, joint end feels, functional decline in mobility, and pain guided the MPT interventions. The utilization of specific techniques to increase joint mobility with complementary exercises appears to have contributed to gains in PROM, decreases in pain, and increased functional activity in this case series. Because a case series cannot establish a cause-and-effect relationship, further research, including randomized clinical trials, is necessary to uncover the exact effects of MPT and exercise for the treatment of hip OA. ACKNOWLEDGEMENTS We would like to graciously thank the faculty of Regis University, Denver Colorado, for their ongoing support of clinical research. REFERENCES 1. Altman R, Alarcon G, Appelrouth D, et al. The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hip. Arthritis Rheum. 1991;34:505-514. 2. Altman RD, Bloch DA, Dougados M, et al. Measurement of structural progression in osteoarthritis of the hip: the Barcelona consensus group. Osteoarthritis Cartilage. 2004;12:515-524. 3. American College of Rheumatology. Recommendations for the medical management of osteoarthritis of the hip and knee: 2000 update. American College of Rheumatology Subcommittee on Osteoarthritis Guidelines. Arthritis Rheum. 2000;43:1905-1915. 4. American Physical Therapy Association. Guide to Physical Therapist Practice. Second Edition. American Physical Therapy Association. Phys Ther. 2001;81:9-746. 5. Birrell F, Croft P, Cooper C, Hosie G, Macfarlane G, Silman A. Predicting radiographic hip osteoarthritis from range of movement. Rheumatology (Oxford). 2001;40:506-512. 6. Bjordal JM, Ljunggren AE, Klovning A, Slordal L. NSAIDs, including coxibs, probably do more harm than good, and paracetamol is ineffective for hip OA. Ann Rheum Dis. 2005;64:655-656; author reply 656. 597 CASE REPORT The actual pathophysiology behind the success of MPT interventions for hip OA is beyond the scope of this case series and will require further research. It is also recognized that improvements reported in this case series may be due to simply an increased level of activity, as causality can not be determined from a case series. The potential cost containment benefits of utilization of MPT for hip OA can be seen by a theoretical comparison of the cost of participation in this case series, to the cost of the potential eventual treatment of hip OA with a THA.46 The cost of PT services in this case series is estimated at $900 dollars (8 visits plus 1 evaluation) compared to an estimated $30 000 for a THA (including surgery and hospitalization at $23 332 plus rehabilitation).21 It is recognized that there is not a direct relationship of hip OA to THA, but the value of a longitudinal study looking at the number of patients needed to be treated to avoid 1 THA over a prolonged period of time would be of clinical value, especially given the decrease in total knee arthroplasty of 75% at 1 year in the MPT treatment group of the Deyle et al17 study with comparison to the control group, and the current reported number of THAs being 164 000 annually in the United States.27 As previously mentioned, we cannot infer a causeand-effect relationship from a case series. Further limitations include the fact that no intrarater or interrater testing or training was completed for the examination tests and measures and the MPT techniques utilized. No blinding occurred as the treating physical therapists completed all of the patient examinations in this case series. A directional causal effect cannot be extrapolated for specific MPT techniques as multiple techniques were used. The influence of the Hawthorne effect, which is the tendency of individuals to perform better in a research setting as they are being assessed,60 can not be ignored, as each therapist in this case series was aware that individual patient outcomes were being measured, but no subjects were excluded from outcomes reporting. However, despite the limitations of the case series, the outcomes presented are encouraging for the clinical utilization of MPT techniques and exercise in the treatment of hip OA and patients with primary hip pain satisfying the ACR classification for hip OA. Future studies should investigate the physiological mechanism that promotes improved joint function following nonthrust and thrust mobilization/ manipulation for hip OA. Research assessing the appropriateness of including MPT into the ACR guidelines for the treatment of hip OA, given the outcomes of the Hoeksma et al34 trial and this case series, is warranted. Studies should investigate whether thrust mobilization/manipulation generates a different clinical outcome than nonthrust mobilization/manipulation techniques for hip OA, 7. Brooks PM. Impact of osteoarthritis on individuals and society: how much disability? Social consequences and health economic implications. Curr Opin Rheumatol. 2002;14:573-577. 8. Browder DA, Enseki K, Fritz J. Intertester reliability of hip range of motion measurements and special tests [abstract]. J Orthop Sports Phys Ther. 2004;34:A1. 9. Browder DA, Erhard RE. Decision making for a painful hip: a case requiring referral. J Orthop Sports Phys Ther. 2005;35:738-744. 10. Childs JD, Piva SR, Fritz JM. Responsiveness of the numeric pain rating scale in patients with low back pain. Spine. 2005;30:1331-1334. 11. Cibulka MT, Threlkeld J. The early clinical diagnosis of osteoarthritis of the hip. J Orthop Sports Phys Ther. 2004;34:461-467. 12. Cliborne AV, Wainner RS, Rhon DI, et al. Clinical hip tests and a functional squat test in patients with knee osteoarthritis: reliability, prevalence of positive test findings, and short-term response to hip mobilization. J Orthop Sports Phys Ther. 2004;34:676-685. 13. Croft P, Cooper C, Wickham C, Coggon D. Defining osteoarthritis of the hip for epidemiologic studies. Am J Epidemiol. 1990;132:514-522. 14. Cyriax J. Textbook of Orthopaedic Medicine, 1: Diagnosis of Soft Tissue Lesions. 8th ed. London, UK: Bailliere Tindall; 1982. 15. Dekker J, Boot B, van der Woude LH, Bijlsma JW. Pain and disability in osteoarthritis: a review of biobehavioral mechanisms. J Behav Med. 1992;15:189214. 16. Dekker J, Tola P, Aufdemkampe G, Winckers M. Negative affect, pain and disability in osteoarthritis patients: the mediating role of muscle weakness. Behav Res Ther. 1993;31:203-206. 17. Deyle GD, Henderson NE, Matekel RL, Ryder MG, Garber MB, Allison SC. Effectiveness of manual physical therapy and exercise in osteoarthritis of the knee. A randomized, controlled trial. Ann Intern Med. 2000;132:173-181. 18. Duthrie R, Bentley G. Mercer’s Orthopaedic Surgery. 9th ed. Oxford, UK: Oxford University Press; 1996. 19. Ekdahl C, Andersson SI, Svensson B. Muscle function of the lower extremities in rheumatoid arthritis and osteoarthrosis. A descriptive study of patients in a primary health care district. J Clin Epidemiol. 1989;42:947-954. 20. Elders MJ. The increasing impact of arthritis on public health. J Rheumatol Suppl. 2000;60:6-8. 21. Epps CD. Length stay, discharge disposition, and hospital charge predictors. Aorn J. 2004;79:975-976, 979981, 984-997. 22. Fajardo M, Di Cesare PE. Disease-modifying therapies for osteoarthritis: current status. Drugs Aging. 2005;22:141-161. 23. Farrar JT, Young JP, Jr., LaMoreaux L, Werth JL, Poole RM. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94:149-158. 24. Greenman PE. Principles of Manual Medicine. 2nd ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 1996. 25. Grieve GP. Common Vertebral Joint Problems. 2nd ed. London, UK: Churchill Livingstone; 1988. 26. Hahne AJ, Keating JL, Wilson SC. Do within-session changes in pain intensity and range of motion predict between-session changes in patients with low back pain? Aust J Physiother. 2004;50:17-23. 27. Hall MJ, DeFrances CJ. 2001 National Hospital Discharge Survey. Advance Data for Vital and Health 598 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. Statistics. Available at: http://www.cdc.gov/nchs/data/ad/ ad332.pdf. Accessed July 25, 2003. Harris WH. Traumatic arthritis of the hip after dislocation and acetabular fractures: treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J Bone Joint Surg Am. 1969;51:737755. Hochberg MC. What a difference a year makes: reflections on the ACR recommendations for the medical management of osteoarthritis. Curr Rheumatol Rep. 2001;3:473-478. Hochberg MC, Altman RD, Brandt KD, et al. Guidelines for the medical management of osteoarthritis. Part I. Osteoarthritis of the hip.American College of Rheumatology. Arthritis Rheum. 1995;38:1535-1540. Hodges PW. Core stability exercise in chronic low back pain. Orthop Clin North Am. 2003;34:245-254. Hoeksma HL. Manual Therapy in Osteoarthritis of the Hip. Koninklijke De Swart: Den Haag; 2003. Hoeksma HL, Dekker J, Ronday HK, Breedveld FC, Van den Ende CH. Manual therapy in osteoarthritis of the hip: outcome in subgroups of patients. Rheumatology (Oxford). 2005;44:461-464. Hoeksma HL, Dekker J, Ronday HK, et al. Comparison of manual therapy and exercise therapy in osteoarthritis of the hip: a randomized clinical trial. Arthritis Rheum. 2004;51:722-729. Hoeksma HL, Van Den Ende CH, Ronday HK, Heering A, Breedveld FC. Comparison of the responsiveness of the Harris Hip Score with generic measures for hip function in osteoarthritis of the hip. Ann Rheum Dis. 2003;62:935-938. Holm I, Bolstad B, Lutken T, Ervik A, Rokkum M, Steen H. Reliability of goniometric measurements and visual estimates of hip ROM in patients with osteoarthrosis. Physiother Res Int. 2000;5:241-248. Jaeschke R, Singer J, Guyatt GH. Measurement of health status. Ascertaining the minimal clinically important difference. Control Clin Trials. 1989;10:407-415. Kaltenborn FM. Manual Mobilization of the Extremity Joints: Basic Examination and Treatment Techniques. 4th ed. Oslo, Norway: Olaf Norlis Bokhandel; 1989. Kaltenborn FM. The Spine, Basic Evaluation and Mobilization Techniques. 2nd ed. Oslo, Norway: Olaf Norlis Bokhandel; 1993. Kean WF, Kean R, Buchanan WW. Osteoarthritis: symptoms, signs and source of pain. Inflammopharmacology. 2004;12:3-31. Kellgren JH. Osteoarthrosis in patients and populations. Br Med J. 1961;5243:1-6. Kendall FP. Muscles, Testing and Function. 4th ed. Baltimore, MD: Lippincott, Williams &Wilkins; 1993. Khan AM, McLoughlin E, Giannakas K, Hutchinson C, Andrew JG. Hip osteoarthritis: where is the pain? Ann R Coll Surg Engl. 2004;86:119-121. King JT, Jr., Moossy JJ, Tsevat J, Roberts MS. Multimodal assessment after surgery for cervical spondylotic myelopathy. J Neurosurg Spine. 2005;2:526-534. Klassbo M, Harms-Ringdahl K, Larsson G. Examination of passive ROM and capsular patterns in the hip. Physiother Res Int. 2003;8:1-12. Koh J, Dietz J. Osteoarthritis in other joints (hip, elbow, foot, ankle, toes, wrist) after sports injuries. Clin Sports Med. 2005;24:57-70. Lin YC, Davey RC, Cochrane T. Tests for physical function of the elderly with knee and hip osteoarthritis. Scand J Med Sci Sports. 2001;11:280-286. Loudon JK. Manual therapy management of hip osteoarthritis. J Man Manip Ther. 1999;7:203-208. J Orthop Sports Phys Ther • Volume 36 • Number 8 • August 2006 63. Steultjens MP, Dekker J, van Baar ME, Oostendorp RA, Bijlsma JW. Muscle strength, pain and disability in patients with osteoarthritis. Clin Rehabil. 2001;15:331341. 64. Stoddard A. Manual of Osteopathic Technique. 3rd ed. London, UK: Hutchinson; 1980. 65. Tak E, Staats P, Van Hespen A, Hopman-Rock M. The effects of an exercise program for older adults with osteoarthritis of the hip. J Rheumatol. 2005;32:11061113. 66. Trendelenburg F. Trendelenburg’s test: 1895. Clin Orthop Relat Res. 1998;3-7. 67. Tuttle N. Do changes within a manual therapy treatment session predict between-session changes for patients with cervical spine pain? Aust J Physiother. 2005;51:43-48. 68. van Baar ME, Assendelft WJ, Dekker J, Oostendorp RA, Bijlsma JW. Effectiveness of exercise therapy in patients with osteoarthritis of the hip or knee: a systematic review of randomized clinical trials. Arthritis Rheum. 1999;42:1361-1369. 69. van Baar ME, Dekker J, Lemmens JA, Oostendorp RA, Bijlsma JW. Pain and disability in patients with osteoarthritis of hip or knee: the relationship with articular, kinesiological, and psychological characteristics. J Rheumatol. 1998;25:125-133. 70. van Baar ME, Dekker J, Oostendorp RA, Bijl D, Voorn TB, Bijlsma JW. Effectiveness of exercise in patients with osteoarthritis of hip or knee: nine months’ follow up. Ann Rheum Dis. 2001;60:1123-1130. 71. Weigl M, Angst F, Stucki G, Lehmann S, Aeschlimann A. Inpatient rehabilitation for hip or knee osteoarthritis: 2 year follow up study. Ann Rheum Dis. 2004;63:360368. 72. Wolfe F. Determinants of WOMAC function, pain and stiffness scores: evidence for the role of low back pain, symptom counts, fatigue and depression in osteoarthritis, rheumatoid arthritis and fibromyalgia. Rheumatology (Oxford). 1999;38:355-361. 73. Wong M, Chowienczyk P, Kirkham B. Cardiovascular issues of COX-2 inhibitors and NSAIDs. Aust Fam Physician. 2005;34:945-948. 74. Wyke BD. Articular neurology and manipulative therapy. In: Glasgow EF, Twomey LT, eds. Aspects of Manipulative Therapy. Melbourne, Australia: Churchill Livingstone; 1985:72-77. J Orthop Sports Phys Ther • Volume 36 • Number 8 • August 2006 599 CASE REPORT 49. Magee DJ. Orthopedic Physical Assessment. 3rd ed. Philadelphia, PA: W.B. Saunders Co; 1997. 50. Maitland GD. Peripheral Manipulation. London, UK: Butterworth Heinemann; 1986. 51. Mink A. Extremiteiten: Functie-Onderzoek en Manuele Therapie [in Dutch]. Houten, The Netherlands: Bohn Stafleu Van Lochem; 1990. 52. Odding E, Valkenburg HA, Stam HJ, Hofman A. Determinants of locomotor disability in people aged 55 years and over: the Rotterdam Study. Eur J Epidemiol. 2001;17:1033-1041. 53. O’Sullivan PB, Twomey L, Allison GT. Altered abdominal muscle recruitment in patients with chronic back pain following a specific exercise intervention. J Orthop Sports Phys Ther. 1998;27:114-124. 54. Ottawa Panel. Ottawa panel evidence-based clinical practice guidelines for therapeutic exercises and manual therapy in the management of osteoarthritis. Phys Ther. 2005;85:907-971. 55. Perry J, Weiss WB, Burnfield JM, Gronley JK. The supine hip extensor manual muscle test: a reliability and validity study. Arch Phys Med Rehabil. 2004;85:1345-1350. 56. Petrofsky JS. The use of electromyogram biofeedback to reduce Trendelenburg gait. Eur J Appl Physiol. 2001;85:491-495. 57. Pollard H, Lakay B, Tucker F, Watson B, Bablis P. Interexaminer reliability of the deltoid and psoas muscle test. J Manipulative Physiol Ther. 2005;28:52-56. 58. Reijman M, Hazes JM, Pols HA, Bernsen RM, Koes BW, Bierma-Zeinstra SM. Role of radiography in predicting progression of osteoarthritis of the hip: prospective cohort study. BMJ. 2005;330:1183. 59. Roddy E, Zhang W, Doherty M, et al. Evidence-based recommendations for the role of exercise in the management of osteoarthritis of the hip or knee--the MOVE consensus. Rheumatology (Oxford). 2005;44:67-73. 60. Roethlisberger J, Dickson WJ. Management and the Worker. Cambridge, MA: Harvard University Press; 1966. 61. Sackett DL. Clinical epidemiology. what, who, and whither. J Clin Epidemiol. 2002;55:1161-1166. 62. Sims K. The development of hip osteoarthritis: implications for conservative management. Man Ther. 1999;4:127-135. ERRATA CORRECTION: ALTMAN’S CRITERIA FOR OSTEOARTHRITIS OF THE HIP AND KNEE I n 1991, Altman and colleagues1 published criteria for classification of osteoarthritis of the hip, of which one criterion was “less than or equal to 60 minutes of morning stiffness.” This criterion was erroneously published by the JOSPT as greater than 60 minutes in TABLE 3 of the article by Cibulka and Threlkeld3 (August 2004) and in TABLE 1 of the article by MacDonald et al5 (August 2006). Also, one of the criteria for classification of idiopathic osteoarthritis of the knee, as published by Altman et al2 in 1986, was less than 30 minutes of stiffness. This was incorrectly published as stiffness greater than 30 minutes in the text of the article by Cliborne et al,4 in the November 2004 issue of the JOSPT. We apologize for these errors and have corrected reprints of the articles, which are available to members and subscribers for download on the JOSPT web site (www.jospt.org). T REFERENCES 1. Altman R, Alarcon G, Appelrouth D, et al. The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hip. Arthritis Rheum. 1991;34:505-514. 2. Altman R, Asch E, Bloch D, et al. Develop- ment of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum. 1986;29:1039-1049. 3. Cibulka, MT, Threlkeld, J. The early clinical diagnosis of osteoarthritis of the hip. J Orthop Sports Phys Ther. 2004;34(8):461-467. 4. Cliborne AV, Wainner RS, Rhon DI. Clinical hip tests and a functional squat test in patients with knee osteoarthritis: reliability, prevalence of positive test findings, and short-term response to hip mobilization. J Orthop Sports Phys Ther. 2004. 34(11):676-685. 5. MacDonald CW, Whitman JM, Cleland JA, Smith M, Hoeksma HL. Clinical outcomes following manual physical therapy and exercise for hip osteoarthritis: a case series. J Orthop Sports Phys Ther. 2006;36(8):588-599. journal of orthopaedic & sports physical therapy | volume 37 | number 9 | september 2007 | 573