Research Report
advertisement

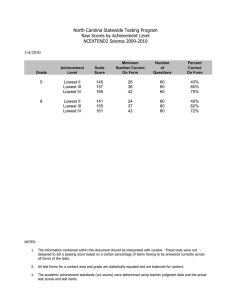
Research Report Sensory-Specific Balance Training in Older Adults: Effect on Proprioceptive Reintegration and Cognitive Demands Kelly P Westlake, Elsie G Culham KP Westlake, PT, PhD, MSc, is Post-Doctoral Fellow, Rehabilitation Research and Development Center, VA Palo Alto HCC, 3801 Miranda Ave, Palo Alto, CA 94304 (USA). Address all correspondence to Dr Westlake at: westlake@rrd. stanford.edu. EG Culham, PT, PhD, is Professor and Director, School of Rehabilitation Therapy, Queen’s University, Kingston, Ontario, Canada. [Westlake KP, Culham EG. Sensory-specific balance training in older adults: effect on proprioceptive reintegration and cognitive demands. Phys Ther. 2007;87:1274 –1283.] © 2007 American Physical Therapy Association Background and Purpose Age-related changes in the ability to adjust to alterations in sensory information contribute to impaired postural stability. The purpose of this randomized controlled trial was to investigate the effect of sensory-specific balance training on proprioceptive reintegration. Subjects The subjects of this study were 36 older participants who were healthy. Methods Participants were randomly assigned to a balance exercise group (n⫽17) or a falls prevention education group (n⫽19). The primary outcome measure was the centerof-pressure (COP) velocity change score. This score represented the difference between COP velocity over 45 seconds of quiet standing and each of six 5-second intervals following proprioceptive perturbation through vibration with or without a secondary cognitive task. Clinical outcome measures included the Fullerton Advanced Balance (FAB) Scale and the Activities-specific Balance Confidence (ABC) Scale. Assessments were conducted at baseline, postintervention, and at an 8-week follow-up. Results Following the exercise intervention, there was less destabilization within the first 5 seconds following vibration with or without a secondary task than there was at baseline or in the falls prevention education group. These training effects were not maintained at the 8-week follow-up. Postintervention improvements also were seen on the FAB Scale and were maintained at follow-up. No changes in ABC Scale scores were identified in the balance exercise group, but ABC Scale scores indicated reduced balance confidence in the falls prevention education group postintervention. Discussion and Conclusion The results of this study support short-term enhanced postural responses to proprioceptive reintegration following a sensory-specific balance exercise program. Post a Rapid Response or find The Bottom Line: www.ptjournal.org 1274 f Physical Therapy Volume 87 Number 10 October 2007 Balance Training in Older Adults P ostural control depends on the ability to extract peripheral sensory inputs, integrate this information within the central nervous system (CNS), and coordinate and execute an appropriate motor response. Proprioception is an essential component of this sequence of events, providing orientation information about passive and active movements and positions of the joints as well as the force resulting from muscular contractions. Agerelated changes in the ability to assess the contribution of proprioceptive inputs relative to those of other sensory inputs become evident under conditions in which the proprioceptive inputs are distorted or distorted and then suddenly restored.1 Whereas young adults who are healthy are able to restore balance quickly by taking advantage of sensory redundancy and centrally reweighing available information,2– 4 older adults do not as readily interpret misleading cues or recognize and reintegrate accurate proprioceptive information and therefore can experience postural instability.3,5 These effects are particularly evident when attentional resources are divided.3,6 – 8 Given that the sensory inputs related to various environmental conditions are constantly changing,9 the ability to adjust instantly to a change in sensory information is central to the reduction of fall risk in older adults.10 To date, there have been no reports of training interventions designed to enhance the ability of older adults to use proprioceptive information in balance control. The successful identification of training effects necessarily involves a randomized controlled trial with an exercise intervention designed to induce specific changes in the recognition and effective use of sensory information. Findings that sensory-specific balance exercises, such as training on unsteady support surfaces with transitions between October 2007 sensory environments, result in increased postural stability compared with the effects of nonspecific activity interventions, such as running or strength training, lend support to this theory.11–13 One method used to evaluate the contribution of proprioceptive inputs to postural control and the integrity of the integrative mechanisms within the CNS is to measure changes in postural sway during or following vibration applied over the muscle belly or tendon.14 This technique directly targets the primary muscle afferents contributing to proprioception and may effectively reflect a perturbation of this system. Muscle vibration evokes a sensation of movement in a direction that normally would cause elongation of the vibrated muscle. Accordingly, vibration of antagonistic muscle groups results in immediate disruption of the proprioceptive system.3 Postural responses to such a perturbation then can be assessed in a quiet standing position by recording center-ofpressure (COP) outcomes on a force platform.3,15 This position effectively reduces confounding variables, such as muscle activation, torque generation, and biomechanical changes, that are present during more dynamic tasks. Such variables inevitably would become a source of accurate proprioceptive information that could override the controlled effect of proprioceptive perturbation at the ankle joints. Because the present study represents one of the earliest reports on the ability to train sensory integration immediately following vibration perturbation, the quiet standing protocol was considered advantageous as a means to isolate changes in this ability. Thus, the primary hypothesis of the present study was that older adults, having completed a sensory-specific exercise program, would demonVolume 87 strate reduced postural destabilization and earlier restabilization immediately following the termination of proprioceptive perturbation through vibration in comparison with preexercise outcomes or with the outcomes in a falls prevention education group. These effects were postulated to improve during a concomitant cognitive task. The secondary hypothesis was that the enhanced postural stability would be reflected in superior scores on a balance performance scale and a balance confidence questionnaire. Method Study Participants and Study Design Participants were volunteers over 65 years of age who were healthy and recruited through advertisements and flyers in the community. Exclusion criteria were pre-existing major lower-extremity pathology (eg, chronic ankle instability or severe osteoarthritis), neurological disorders or balance difficulties (eg, vertigo, poor vision, dizziness, stroke, or epilepsy) that would prevent standing for the duration of the testing procedures without the aid of an assistive device, and health conditions (eg, heart disease, uncontrolled hypertension, chronic obstructive pulmonary disease, or osteoporosis) that would preclude participation in a balance exercise program. A brief clinical examination was used to screen for symptoms of peripheral neuropathy, which are considered a risk factor for falls.16 This examination identified the presence, diminution, or absence of sensation to light touch on the dorsal and plantar aspects of the foot, the Achilles tendon reflex, and position sensation of the big toe. Subjects demonstrating the absence or diminution of one or more of these characteristics were excluded from participation. Physician approval was required before the subjects were allowed to particNumber 10 Physical Therapy f 1275 Balance Training in Older Adults together position. Progressions to these tasks included simultaneous alterations of visual and vestibular inputs. To alter visual cues, participants were instructed to close their eyes, to engage vision with a reading or tracking secondary task, or to perform balance tasks with a distracting background, such as a checked pattern or moving people. To modify vestibular cues, participants were instructed to tilt their head backward or to quickly move their head side to side and up and down. Figure 1. Experimental setup of the vibrators at the Achilles and tibialis anterior tendons. Participants stood as steadily as possible with arms alongside the body, heels positioned according to height, and forefeet splayed to a comfortable stance. ipate in the exercise program. All subjects gave written informed consent prior to data collection. In this single-blind, randomized controlled trial, participants were assigned to an exercise group or a falls prevention education group. Both groups were assessed at baseline and within 1 week postintervention. Follow-up testing was done for the exercise group only at 8 weeks postintervention. Of the 64 older adults who responded to study advertisements, 44 met study criteria and were randomized into the exercise or education group. Eight participants dropped out of the study for reasons such as time commitment issues, lack of transportation, language barrier, and disinterest. By the end of the 8-week interventions, 17 and 19 participants remained in the exercise and education programs, respectively. The mean numbers of all visits attended 1276 f Physical Therapy Volume 87 by participants in the exercise group and the education group were 21.5 (89.9%) and 5.4 (66.3%), respectively. The 36 participants who completed the exercise (n⫽17) and education (n⫽19) interventions returned for postintervention testing. By the 8-week follow-up, conducted only with the exercise group, 15 participants returned for testing. Sensory-specific balance classes were held 3 times per week, for 1 hour each session, over an 8-week period. The exercise protocol followed the FallProof Program,17 which emphasizes static and dynamic balance exercises with transitions between different sensory conditions. Activities were designed to optimize and force use of the somatosensory system. Tasks included standing or walking on various support surfaces, such as a rocker board, foam, or narrow beam, and standing in a tandem position, a semitandem position, on one leg, or in a feet- Number 10 Measurement of Central Integration and Attentional Capacity The mean COP velocity for the total COP path length was measured on a force platform* as an estimate of the frequency of postural corrections. Of the COP stability parameters, COP velocity generally is considered to be most useful in identifying agerelated changes and fall risk.18 –20 The mean velocity also demonstrated the highest sensitivity to the effects of vibration on posturographic measurements21 and had the smallest reproducibility error (intraindividual standardized coefficient of variation of 14) over a 1-week period.20 Data were sampled at 200 Hz and smoothed with a fourth-order double-pass Butterworth filter with a cutoff frequency of 10 Hz. Proprioceptive input was perturbed by use of 4 vibrators oscillating at 80 Hz, 1 mm in amplitude,2,22 and secured at both ankles with 3-cm-wide elastic bands (Fig. 1). The COP velocity was measured for each of the 45-second postural conditions shown in Table 1, completed as one set in a random order, followed by 3 minutes of seated rest. * Biodex Medical Systems Inc, 20 Ramsay Rd, Shirley, NY 11967. October 2007 Balance Training in Older Adults Three sets were performed, and the average of 3 trials was recorded for each condition. Conditions 3 and 4 included 5 seconds of stable standing followed by 10 seconds of vibration activation3,21 and then 30 seconds of deactivation. The initial 5 seconds was used so that participants could become acclimated to standing on the force platform prior to the onset of vibration. The third, 30-second interval was used because previous work had indicated that 10 seconds was insufficient for complete recovery of postural stability in the absence of vision in either a young or an older population.3 The COP velocity was analyzed over 5-second intervals from the moment the vibration was turned off, at 15.05 to 20 seconds (time 1), 20.05 to 25 seconds (time 2), 25.05 to 30 seconds (time 3), 30.05 to 35 seconds (time 4), 35.05 to 40 seconds (time 5), and 40.05 to 45 seconds (time 6). For the secondary task in conditions 2 and 4, participants counted backward by 3 from a random 3-digit number as quickly and accurately as possible throughout the 45-second trials.7 Clinical Measures The Fullerton Advanced Balance (FAB) Scale was used to measure functional limitations associated with 10 high-level balance tasks incorporating tests that challenge sensory integration.23 The FAB Scale included modified clinical tests for sensory integration in balance: walking with head turns, Functional Reach Test, 360-degree turn, tandem walking, one-leg stance, 2-foot jump, step up and over, and reactive postural control. Scores ranged from 0 (unable) to 4, with a maximum score of 40. Psychometric testing of this scale indicated good convergent validity compared with the Berg Balance Scale (⫽.75) and demonstrated high test-retest (⫽.96), intrarater (⫽.97–1.00), and interrater (⫽.94 –.97) reliability.23 The October 2007 Table 1. Postural Conditions Used to Evaluate Proprioceptive Reintegration With or Without a Secondary Task a Testing Conditiona Description 1 Quiet standing, eyes closed 2 Quiet standing, eyes closed, secondary task 3 Quiet standing, eyes closed, vibration 4 Quiet standing, eyes closed, vibration, secondary task The duration of each condition was 45 seconds. responsiveness of the FAB Scale following an exercise intervention had not yet been established. The Activities-specific Balance Confidence (ABC) Scale was used to assess participants’ level of balance confidence in performing particular tasks.24 Confidence in performing each task was rated on a scale of 0 (no confidence) to 10. The ABC Scale showed excellent internal consistency (Cronbach alpha⫽.96), testretest reliability (r⫽.92), and validity for community-dwelling older people.24,25 The Physical Activity Scale for the Elderly (PASE) was used to determine group equivalences in activity levels outside of the treatment intervention. Scores ranged from 0 to greater than 400, depending on subjects’ reported activity intensities and frequencies over 7 days. The PASE showed good test-retest reliability (r⫽.75) and validity for older subjects who were healthy.26,27 The concentric isokinetic strength of the hip, knee, and ankle flexor and extensor muscles of the dominant leg was assessed by use of an isokinetic dynamometer (AMTI Multiaxis Force Platforms, model OR 6-7)† set at a velocity of 60°/s. These measurements were taken in consideration of the potentially confounding influ† Advanced Medical Technologies Inc, 176 Waltham St, Watertown, MA 02172. Volume 87 ence of strength (force-generating capacity) between and within groups. Following one practice trial, an average of the best 3 of 5 peak torque values normalized to body weight was recorded. Data Analysis The effects of the interventions on the ability of older adults to regain postural stability with or without a secondary task were assessed by use of a group ⫻ time interval ⫻ visit (2 ⫻ 6 ⫻ 2) analysis of variance (ANOVA) for repeated measures on the last 2 factors. The dependent variable was COP change scores, obtained by subtracting COP velocity averaged over 3 trials for each time interval of conditions 3 and 4 from the average COP velocity in the three 45-second trials in conditions 1 and 2, respectively. The equivalences of COP velocity across the six 5-second intervals and over the entire 45second time interval during condition 1 were verified by use of data from 10 randomly selected participants (F⫽0.37; df⫽6,54; P⫽.76). Changes in strength and clinical measures were determined by use of a group ⫻ visit (2 ⫻ 2) repeatedmeasures ANOVA for continuous variables or a Friedman test for categorical variables. The outcomes for the exercise group at the 8-week follow-up were compared with the outcomes at baseline and postintervention by use of a Number 10 Physical Therapy f 1277 Balance Training in Older Adults COP Velocity Change (cm/s) A COP Velocity Change (cm/s) B 4.0 3.5 3.0 2.5 2.0 1.5 1.0 0.5 0.0 -0.5 -1.0 4.0 3.5 3.0 2.5 2.0 1.5 1.0 0.5 0.0 -0.5 -1.0 Exercise Group * Education Group * 1 2 3 4 Time Interval 5 6 Exercise Group Education Group * * 1 2 3 4 Time Interval 5 6 Figure 2. Change in center-of-pressure (COP) outcomes following vibration in exercise and education groups postintervention (X⫾SD). (A) COP sway velocity change score following vibration perturbation. (B) COP sway velocity change score following vibration perturbation and while performing a secondary task. *Significant difference between groups (P⬍.044). repeated-measures ANOVA or a Friedman test with visit as the within-subject factor. Significant interaction effects (P⬍.05) were analyzed with Bonferroni-adjusted post hoc tests. Statistical procedures were performed with SPSS, version 11.5.‡ ‡ SPSS Inc, 233 S Wacker Dr, Chicago, IL 60606. 1278 f Physical Therapy Volume 87 Results Proprioceptive Reintegration Quiet standing with vibration (condition 3). The first objective of this study was to examine postural recovery following vibratory perturbation without a secondary task. A visit ⫻ time ⫻ group interaction was identified (F⫽3.82; df⫽5,170; P⫽.019). Group differences were found only during time interval 1 (F⫽4.36; df⫽1,35; P⫽.044), with Number 10 less destabilization occurring in the exercise group (change score [X⫾SD], 1.31⫾0.91 cm/s) than in the education group (2.00⫾1.05 cm/s) postintervention (Fig. 2A). Separate analysis of the exercise group revealed a visit ⫻ time interaction (F⫽8.62; df⫽5,80; P⬍.001), indicating training effects on both the time to restabilize and the amount of destabilization (Fig. 3A). Change scores began to stabilize during time interval 4 at baseline and during earlier time interval 3 postintervention. A reduction in the extent of destabilization was indicated by a significant decrease in change scores from baseline to postintervention during time interval 1 (2.23⫾1.18 versus 1.31⫾0.91 cm/s) (P⫽.002), with a trend toward significance during time interval 2 (0.72⫾0.76 versus 0.43⫾0.52 cm/s) (P⫽.081). Analysis of the education group revealed a nonsignificant visit ⫻ time interaction (F⫽0.42; df⫽5,90; P⫽.70), indicating no change in the ability to stabilize following vibration. The COP change scores for the exercise group were different postintervention (1.31⫾0.91 cm/s) and at the 8-week follow-up (2.11⫾1.50 cm/s) during time interval 1 (P⫽.029), suggesting that postintervention improvements were not maintained. No differences were identified between baseline (2.29⫾ 1.19 cm/s) and the 8-week follow-up (P⫽1.00). Quiet standing with vibration and secondary task (condition 4). The second objective of this study was to examine postural stability following vibratory perturbation during secondary task performance. One outlier in the education group was identified as having a mean change score greater than 3 standard deviations above the group mean and was excluded from subsequent analysis. A visit ⫻ time ⫻ group interaction October 2007 Balance Training in Older Adults The inclusion of the 8-week follow-up change scores for the exercise group revealed a visit ⫻ time interaction (F⫽2.93; df⫽10,140; P⫽.012), with higher change scores at the 8-week follow-up (2.05⫾ 1.47 cm/s) than postintervention (1.14⫾0.61 cm/s) during time interval 1 (P⫽.023). These results further support the fact that improvements in the ability to stabilize after the exercise intervention were not maintained. The response accuracy and speed of performance of the secondary task are shown in Table 2. No differences were identified between groups, nor was there a group ⫻ visit interaction. October 2007 COP Velocity Change (cm/s) Analysis of group differences for each time interval across baseline and postintervention visits indicated a difference in the extent of destabilization during time interval 1 (F⫽4.90; df⫽1,34; P⫽.034) postintervention, with lower mean change scores in the exercise group (1.12⫾0.58 cm/s) than in the education group (1.71⫾0.85 cm/s) (Fig. 2B). Separate analysis of the exercise group revealed a visit ⫻ time interaction (F⫽5.76; df⫽5,80; P⫽.001) (Fig. 3B). No improvements in the time to stabilize were noted. Further analysis of change scores between baseline and postintervention as a function of each time interval revealed a difference during time interval 1 (P⫽.002). This finding confirmed that there was less destabilization during the 5 seconds immediately following vibration as a result of the exercise intervention. Analysis of the education group revealed a nonsignificant visit ⫻ time interaction (F⫽1.27; df⫽5,85; P⫽.30). A B COP Velocity Change (cm/s) was revealed (F⫽3.13; df⫽5,165; P⫽.018). 4.0 3.5 3.0 2.5 2.0 1.5 1.0 0.5 0.0 -0.5 -1.0 4.0 3.5 3.0 2.5 2.0 1.5 1.0 0.5 0.0 -0.5 -1.0 *† Baseline Postintervention † † † *‡ ‡ 1 2 ‡ 3 4 Time Interval 5 6 Baseline Postintervention *† † † *‡ 1 ‡ ‡ 2 3 4 Time Interval 5 6 Figure 3. Change in center-of-pressure (COP) outcomes following vibration at baseline and postintervention in exercise group (X⫾SD). (A) COP velocity change scores following vibration perturbation. (B) COP velocity change scores following vibration perturbation and while performing a secondary task. *Significant difference between baseline and postintervention (P⬍.006). †Significant difference between baseline time intervals (P⬍.025). ‡Significant difference between postintervention time intervals (P⬍.001). Clinical Measures Means and standard deviations for clinical measures are shown in Table 3. In terms of the FAB Scale, the Friedman test revealed differences between visits in the exercise group (2⫽16, P⬍.001). Post hoc analysis revealed differences between baseline and postintervention total scores (P⫽.001) and between baseline and 8-week follow-up total scores (P⫽.001), suggesting that the improvements in functional balance Volume 87 postintervention and at follow-up were maintained. Specific details regarding changes in the mean and standard deviation of each FAB Scale item are shown in Table 4. Post hoc analysis revealed differences between baseline and postintervention for items 6 (one-leg stance), 7 (standing on foam), and 9 (walking with head turns) and differences between baseline and the 8-week follow-up for item 9 (Bonferroni-adjusted P value of ⬍.025). Number 10 Physical Therapy f 1279 Balance Training in Older Adults Table 2. Accuracy and Speed of Backward Counting by 3 During Condition 4a Parameter XⴞSD for the Following Group: Baseline a Postintervention 8-wk Follow-up Exercise Education Exercise Education Exercise Accuracy (no. of correct responses/total no. of responses) 0.94⫾0.093 0.96⫾0.035 0.95⫾0.06 0.97⫾0.05 0.94⫾0.06 Speed (no. of responses/s) 0.41⫾0.13 0.44⫾0.16 0.47⫾0.16 0.47⫾0.15 0.43⫾0.19 Condition 4⫽quiet standing, eyes closed, vibration, secondary task. group ⫻ visit interaction (P⫽.44) were identified, thereby supporting group equivalences at baseline and postintervention. Regarding the PASE scores, no differences were identified between groups or visits at baseline or postintervention; significantly lower scores were found in the exercise group at the 8-week follow-up than postintervention (P⫽.003). Interestingly, a Pearson correlation analysis between PASE scores and time interval 1 for conditions 3 and 4 revealed no relationships (r⫽⫺.16, P⫽.13, and r⫽ ⫺.06, P⫽.57). Discussion The results of the present study appear to support the original hypothesis that the ability of older adults to reintegrate proprioceptive inputs is augmented following sensoryspecific training, and this effect is not likely to be attributable to an increase in lower-extremity strength or activity level. Although a few studies reported training effects on postural stability when proprioceptive input was reduced,28,29 an improved ability of older adults to recognize and use the restoration of accurate proprioceptive information had not previously been documented. For the ABC Scale questionnaire, a group ⫻ visit interaction was identified (F⫽4.27; df⫽1,34; P⫽.047), with a lower balance confidence score postintervention than at baseline only for the education group (F⫽4.56; df⫽1,18; P⫽.047). In terms of strength at the hip, knee, and ankle, no main effect of group (P⫽.66) or visit (P⫽.072) and no Although it may be argued that enhanced signals arising at the level of the proprioceptive receptors may account for the postural improvements, we recently demonstrated that this mechanism is not likely to be the substrate for change.30 With only 1 of 3 proprioceptive measures indicating improvements with training in our previous work, it was difficult to ascribe a training effect at the peripheral level. However, without sufficient physiological evidence from receptor isolation techniques, such as microneurography,14 the possibility of an increase in the discharge of these receptors cannot be discounted. A more probable explanation for these results is an increase during the training intervention in the attention allocated to proprioceptive cues (explicit learning), which eventually Table 3. Clinical Measures for Exercise and Education Groups at Baseline, Postintervention, and 8-Week Follow-up Clinical Measurea XⴞSD Score for the Following Group: Baseline Exercise FAB Scale PASE ABC Scale b,c Postintervention Education Exercise b 8-wk Follow-up Education Exercise 35⫾5c 31⫾5 32⫾8 35⫾4 33⫾8 102.4⫾45.0 99.1⫾44.0 127.3⫾57.6d 101.6⫾51.4 84.8⫾9.3 87.5⫾10.7e 85.7⫾9.5 79.1⫾24.2e 79.5⫾24.9d 85.0⫾9.7 a ABC⫽Activities-specific Balance Confidence, FAB⫽Fullerton Advanced Balance, PASE⫽Physical Activity Scale for the Elderly. Significant difference between baseline and postintervention FAB Scale scores (P⬍.001). Significant difference between baseline and 8-week follow-up FAB Scale scores (P⫽.02). d Significant difference between postintervention and 8-week follow-up PASE scores for exercise group (P⫽.003). e Significant difference between baseline and postintervention ABC Scale scores for education group (P⫽.047). b c 1280 f Physical Therapy Volume 87 Number 10 October 2007 Balance Training in Older Adults Table 4. Mean (⫾SD) and Friedman Mean Rank for Scores on the Fullerton Advanced Balance (FAB) Scale for the Exercise Group FAB Scale Item Baseline Group XⴞSD XⴞSD Mean Rank Mean Rank 1.9 4⫾0 2.0 4⫾0 2.0 .39 2. Forward reach 4⫾1 1.9 4⫾0 2.1 4⫾1 1.9 .26 3. 360° turn 3⫾1 1.8 3⫾1 1.9 4⫾1 2.3 .05 4. Step up and over 4⫾0 1.9 4⫾0 2.0 4⫾0 2.0 .37 5. Tandem walk 3⫾1 1.8 4⫾1 2.3 a 3⫾1 1.9 .14 a 6. One-leg stance 3⫾1 1.6 3⫾1 2.2 3⫾1 2.2 .02b 7. Stand on foam, eyes closed 3⫾1 1.7a 4⫾0 2.2a 4⫾0 2.0 .02b 8. 2-foot jump 3⫾1 1.8 3⫾1 2.1 3⫾1 2.1 .35 Total score c XⴞSD P 4⫾0 10. Reactive postural control b 8-Week Followup Group 1. Stand with feet together, eyes closed 9. Walk with head turns a Mean Rank Postintervention Group a,c 2⫾1 1.5 2⫾1 1.6 31⫾5 1.2a,c 3⫾1 a 2.3 3⫾1 c 2.2 .01b 3⫾1 2.2 3⫾1 2.2 .12 35⫾4 2.5a 35⫾5 2.3c ⬍.001b Significant difference between baseline and postintervention scores (P⬍.025). Significant difference between testing sessions (P⬍.05). Significant difference between baseline and 8-week follow-up scores (P⬍.025). led to a less attentionally demanding recovery of postural stability (implicit learning).31 Improvements in postural control in the exercise group without evidence of reductions in the accuracy or speed of the counting task support this theory. As the accuracy of peripheral input declines with age, attentional resources become more focused on the control of posture.1 Thus, the introduction of a sufficiently challenging secondary task or postural condition often results in reduced task performance or instability.6,32 Because the specific instructions provided to participants in the present study were to maintain focus on the secondary task, evidence that stability was increased suggests an implicit learning effect. Our previous finding that a velocity discrimination test was the only proprioceptive outcome to improve with exercise also suggests enhanced central mechanisms.30 This test required subjects to identify the faster of 2 presented velocities until the smallest velocity difference was October 2007 identified correctly. Thus, a greater extent of cognitive resources was necessary for this test than for other proprioceptive measures, meaning that the possibility of improved attention cannot be ruled out. Besides the possible influence of attention in recognizing and selecting proprioceptive information, it also has been suggested that attention is involved in sensory integration under conditions of sensory conflict.33 One surprising outcome was the decrease in COP velocity change scores (ie, reduced destabilization) during secondary task performance relative to the results obtained in the nosecondary-task condition (Fig. 2). Although the difference was not significant, it was evident in both the exercise and the education groups. In contrast, previous studies6,33,34 demonstrated a destabilizing rather than a stabilizing effect with the addition of a secondary task. These conflicting results may be reconciled by a recent study demonstrating that Volume 87 postural stability improved or declined relative to baseline performance depending on the cognitive demands of the secondary task.32 Perhaps the task of counting backward by 3, used in the present study, did not represent a sufficiently challenging cognitive task to tax attentional resources effectively. Nevertheless, the finding that the extent of destabilization was reduced postintervention with or without a secondary task suggests that either a shift in attention or increased attentional capacity is possible. A follow-up training study involving a more cognitively demanding secondary task under conditions of sensory conflict may bring further clarity to this discussion. Several authors3,4,35 have proposed that the explanation for impaired postural responses in older adults lies in age-related changes in central integration mechanisms. During the exercise intervention in the present study, sensory inputs were manipulated by altering the support surface Number 10 Physical Therapy f 1281 Balance Training in Older Adults or by reducing the sensory redundancy of the visual and vestibular systems; these manipulations forced participants to effectively reweigh remaining inputs within the CNS.17 The direct beneficial consequences of these tasks were reflected in the ability of the participants to regain stability, likely by taking advantage of the restored proprioceptive information and integrating it with vestibular inputs and other sensorimotor cues. Evidence of similarly enhanced central integration following sensory training has been found in studies demonstrating improved stability during the manipulation of proprioceptive, vestibular, or visual systems or all of these by use of the Sensory Organization Test (SOT).28,36 Although the use of a sway reference standing surface during the SOT is considered to be a proprioceptive perturbation, the muscle spindles serving this system cannot be targeted as precisely as with vibration. These studies also were limited because of the use of a cross-sectional design including seasoned tai chi practitioners36 and the use of the SOT for both training and testing procedures,28 which may have resulted in a learning effect.37 The functional significance of the results of the present research was evident because of improvements in the FAB Scale scores in the exercise group. These results, demonstrating responsiveness to training, further support the validity of FAB Scale scores. Interestingly, the items demonstrating improvements across visits were items 6 (one-leg stance), 7 (standing on foam), and 9 (walking with head turns), each of which comprises an element of sensory integration. However, even though subjects showed improvements in and maintenance of FAB Scale scores at the 8-week follow-up, the improvements did not translate to the maintenance of enhanced postural stability following vibratory pertur1282 f Physical Therapy Volume 87 bation. This lack of an effect suggests that there are context-dependent differences following a targeted training intervention and thereby supports the need for ongoing sensory training. In turn, compensatory sensory mechanisms may be selected more efficiently under conditions of sensory deprivation38 or restoration. The decrease in balance confidence in the education group postintervention may be explained by discussions centered on effective means of reducing fall risk. An increased awareness of these topics may have underscored the apprehension experienced during functional balance tasks until changes could be implemented. Two recent studies examining the effectiveness of falls prevention education reported similar findings, with almost half of the participants demonstrating increased fear of falling39 and a 28% increase in 1 or more falls40 at follow-up. Seasonal variations in PASE scores may account for the reduction in scores at the 8-week follow-up in the exercise group.26 Follow-up testing occurred during both the winter and the summer months, when either snow and ice or high heat and humidity may have forced participants indoors. Arguably, the reduction in activity level may explain the lack of retention in the ability to reintegrate proprioceptive information effectively. However, without a significant correlation between PASE scores and COP velocity in the first 5 seconds following vibration, this theory is not substantiated. Conclusion The results of the present study suggested that sensory-specific exercise had a training effect on proprioceptive reintegration. However, 2 limitations should be mentioned. The first limitation is that 8-week follow-up scores were not obtained for the education group. Therefore, although Number 10 improvements in the FAB Scale scores were maintained in the exercise group, it remains unclear whether the control group also experienced changes over the 8-week time period. The second limitation is that the participants were older adults who were healthy rather than older adults with balance impairments, who may have benefited to a greater extent. Future research may include a group of older adults with declining balance to assess the effect of training on central sensory reintegration. Such an investigation also may include a kinematic and kinetic analysis of the effect of vibration on dynamic stability tasks. A combination of findings from these studies and those from the present study may lead to more efficient balance exercise interventions and, ultimately, to a reduction in fall risk in older adults. Both authors provided concept/idea/research design, writing, and data analysis. Dr Westlake provided data collection, project management, fund procurement, and subjects. Dr Culham provided facilities/equipment and consultation (including review of manuscript before submission). This study was approved by Queen’s University Health Science and Affiliated Teaching Hospitals Research Ethics Board. Data from this study were presented at the International Congress of the World Confederation for Physical Therapy; June 2– 6, 2007; Vancouver, British Columbia, Canada. Dr Westlake was supported by a Canadian Institutes of Health Research Fellowship. This article was received September 7, 2006, and was accepted May 8, 2007. DOI: 10.2522/ptj.20060263 References 1 Kristinsdottir EK, Fransson PA, Magnusson M. Changes in postural control in healthy elderly subjects are related to vibration sensation, vision and vestibular asymmetry. Acta Otolaryngol. 2001;121:700 –706. 2 Hay L, Bard C, Fleury M, Teasdale N. Availability of visual and proprioceptive afferent messages and postural control in elderly adults. Exp Brain Res. 1996; 108:129 –139. October 2007 Balance Training in Older Adults 3 Teasdale N, Simoneau M. Attentional demands for postural control: the effects of aging and sensory reintegration. Gait Posture. 2001;14:203–210. 4 Quoniam C, Hay L, Roll JP, Harlay F. Age effects on reflex and postural responses to propriomuscular inputs generated by tendon vibration. J Gerontol A Biol Sci Med Sci. 1995;50:B155–B165. 5 Camicioli R, Panzer VP, Kaye J. Balance in the healthy elderly: posturography and clinical assessment. Arch Neurol. 1997;54: 976 –981. 6 Shumway-Cook A, Woollacott M. Attentional demands and postural control: the effect of sensory context. J Gerontol A Biol Sci Med Sci. 2000;55:M10 –M16. 7 Woollacott M, Shumway-Cook A. Attention and the control of posture and gait: a review of an emerging area of research. Gait Posture. 2002;16:1–14. 8 Rankin JK, Woollacott MH, ShumwayCook A, Brown LA. Cognitive influence on postural stability: a neuromuscular analysis in young and older adults. J Gerontol A Biol Sci Med Sci. 2000;55:M112–M119. 9 Peterka RJ. Sensorimotor integration in human postural control. J Neurophysiol. 2002;88:1097–1118. 10 Peterka RJ, Loughlin PJ. Dynamic regulation of sensorimotor integration in human postural control. J Neurophysiol. 2004;91: 410 – 423. 11 Xu D, Hong Y, Li J, Chan K. Effect of tai chi exercise on proprioception of ankle and knee joints in old people. Br J Sports Med. 2004;38:50 –54. 12 Beard DJ, Dodd CA, Trundle HR, Simpson AH. Proprioception enhancement for anterior cruciate ligament deficiency: a prospective randomised trial of two physiotherapy regimes. J Bone Joint Surg Br. 1994;76:654 – 659. 13 Gauchard GC, Gangloff P, Jeandel C, Perrin PP. Influence of regular proprioceptive and bioenergetic physical activities on balance control in elderly women. J Gerontol A Biol Sci Med Sci. 2003;58: M846 –M850. 14 Burke D, Hagbarth KE, Lofstedt L, Wallin BG. The responses of human muscle spindle endings to vibration of noncontracting muscles. J Physiol. 1976;261: 673– 693. 15 Vuillerme N, Teasdale N, Nougier V. The effect of expertise in gymnastics on proprioceptive sensory integration in human subjects. Neurosci Lett. 2001;311:73–76. October 2007 16 Richardson JK, Ashton-Miller JA. Peripheral neuropathy: an often-overlooked cause of falls in the elderly. Postgrad Med. 1996;99:161–172. 17 Rose DJ. FallProof! A Comprehensive Balance and Mobility Training Program. Windsor, Ontario, Canada: Human Kinetics; 2003. 18 Maki BE, Holliday PJ, Fernie GR. Aging and postural control: a comparison of spontaneous- and induced-sway balance tests. J Am Geriatr Soc. 1990;38:1–9. 19 Lafond D, Corriveau H, Hebert R, Prince F. Intrasession reliability of center of pressure measures of postural steadiness in healthy elderly people. Arch Phys Med Rehabil. 2004;85:896 –901. 20 Raymakers JA, Samson MM, Verhaar HJ. The assessment of body sway and the choice of the stability parameter(s). Gait Posture. 2005;21:48 –58. 21 Uimonen S, Sorri M, Laitakari K, Jamsa T. A comparison of three vibrators in static posturography: the effect of vibration amplitude on body sway. Med Eng Phys. 1996; 18:405– 409. 22 Ribot-Ciscar E, Rossi-Durand C, Roll JP. Muscle spindle activity following muscle tendon vibration in man. Neurosci Lett. 1998;258:147–150. 23 Rose DJ, Lucchese N, Wiersma LD. Development of a multidimensional balance scale for use with functionally independent older adults. Arch Phys Med Rehabil. 2006;87:1478 –1485. 24 Powell LE, Myers AM. The Activitiesspecific Balance Confidence (ABC) Scale. J Gerontol A Biol Sci Med Sci. 1995;50A: M28 –M34. 25 Myers AM, Powell LE, Maki BE, et al. Psychological indicators of balance confidence: relationship to actual and perceived abilities. J Gerontol A Biol Sci Med Sci. 1996;51:M37–M43. 26 Washburn RA, Smith KW, Jette AM, Janney CA. The physical activity scale for the elderly (PASE): development and evaluation. J Clin Epidemiol. 1993;46:153–162. 27 Washburn RA, McAuley E, Katula J, et al. The physical activity scale for the elderly (PASE): evidence for validity. J Clin Epidemiol. 1999;52:643– 651. 28 Hu MH, Woollacott MH. Multisensory training of standing balance in older adults, I: postural stability and one-leg stance balance. J Gerontol. 1994;49:M52– M61. Volume 87 29 Tsang WW, Hui-Chan CW. Effect of 4- and 8-week intensive Tai Chi training on balance control in the elderly. Med Sci Sports Exerc. 2004;36:648 – 657. 30 Westlake KP, Wu Y, Culham EG. Sensoryspecific balance training in older adults: effect on position, movement, and velocity sense at the ankle. Phys Ther. 2007;87: 560 –568. 31 Orrell AJ, Eves FF, Masters RS. Implicit motor learning of a balancing task. Gait Posture. 2006;23:9 –16. 32 Huxhold O, Li SC, Schmiedek F, Lindenberger U. Dual-tasking postural control: aging and the effects of cognitive demand in conjunction with focus of attention. Brain Res Bull. 2006;69:294 –305. 33 Redfern MS, Jennings JR, Martin C, Furman JM. Attention influences sensory integration for postural control in older adults. Gait Posture. 2001;14:211–216. 34 Condron JE, Hill KD. Reliability and validity of a dual-task force platform assessment of balance performance: effect of age, balance impairment, and cognitive task. J Am Geriatr Soc. 2002;50:157–162. 35 Stelmach GE, Teasdale N, Di Fabio RP, Phillips J. Age related decline in postural control mechanisms. Int J Aging Hum Dev. 1989;29:205–223. 36 Tsang WW, Wong VS, Fu SN, Hui-Chan CW. Tai Chi improves standing balance control under reduced or conflicting sensory conditions. Arch Phys Med Rehabil. 2004;85:129 –137. 37 Grindstaff TL, Christiano KE, Broos AM, et al. Assessment of a practice effect in serial sensory organization testing scores of healthy adults. Percept Mot Skills. 2006; 102:379 –386. 38 Bayouk JF, Boucher JP, Leroux A. Balance training following stroke: effects of taskoriented exercises with and without altered sensory input. Int J Rehabil Res. 2006;29:51–59. 39 Rucker D, Rowe BH, Johnson JA, et al. Educational intervention to reduce falls and fear of falling in patients after fragility fracture: results of a controlled pilot study. Prev Med. 2006;42:316 –319. 40 Chang JT, Morton SC, Rubenstein LZ, et al. Interventions for the prevention of falls in older adults: systematic review and metaanalysis of randomised clinical trials. BMJ. 2004;328:680. Number 10 Physical Therapy f 1283