KIRKWOOD COMMUNITY COLLEGE IMMUNIZATION RECORD
advertisement

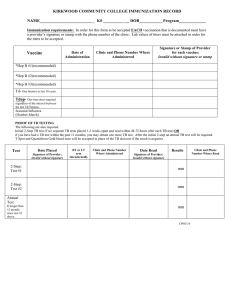
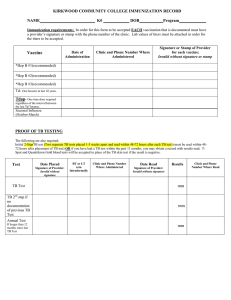
KIRKWOOD COMMUNITY COLLEGE IMMUNIZATION RECORD NAME_________________________ K# _________ __ DOB___________ Program_____________ Immunization requirements: In order for this form to be accepted EACH vaccination that is documented must have a provider’s signature or stamp with the phone number of the clinic. Lab values of titres must be attached in order for the titres to be accepted. Vaccine Date of Administration ******** Clinic and Phone Number Where Administered Invalid without Clinic Information ********************** Signature or Stamp of Provider for each vaccine: Invalid without signature or stamp ************************* *Hep B #1 Required before clinical experiences *Hep B #2 *Hep B #3 Measles #1 Measles #2 Not required if born prior to 1957 Mumps #1 Mumps #2 Not required if born prior to 1957 Rubella #1 Td- One booster in last 10 years. Tdap- One time dose required regardless of the interval between the last Td/Tetanus. Varicella #1 if no documentation of chickenpox disease Varicella #2 if no documentation of chickenpox disease Seasonal Influenza Fall/Winter only PROOF OF TB TESTING The following are also required: Initial 2-Step Mantoux (TB) test (Two separate TB test placed 1-3 weeks apart and read within 48-72 hours after each TB test). The 2nd TB test should only be done if the first TB test is negative and placed no earlier than 7 days after the 1 st TB test is read. As long as the 2nd TB test is placed within a year of the first that will meet the standard for a 2 nd TB in a 2 step TB test. T-Spot and Quantiferon Gold blood tests will be accepted in place of the TB skin test if the result is negative. Test Date Placed Signature of Provider: *Invalid without signature* RT or LT arm Intradermally Clinic and Phone Number Where Administered ************ Date Read Results Signature of Provider: *Invalid without signature* 2-Step: Test #1 mm 2-Step: Test #2 mm Annual Test If longer than 12 months since test #2 above. mm KDP 03/28/13 Clinic and Phone Number Where Read *************