PRACTICUM Agreement
advertisement

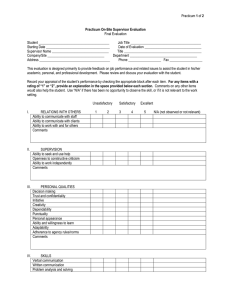
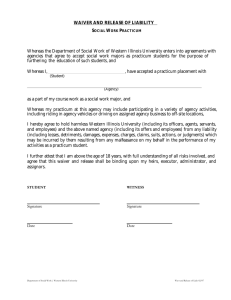
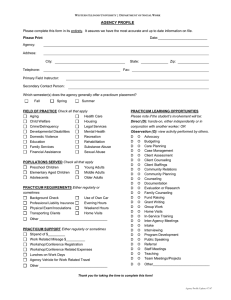
PRACTICUM Agreement Student Name:_____________________ High School:__________________ Home Phone:_______________________ School Phone:_________________ Name of Faculty Practicum Advisor:___________________________________ Practicum Worksite:______________________________________________ Address:_______________________________________________________ Practicum Supervisor:__________________ Supervisor's Title:____________ Supervisor's Phone:____________________ Supervisor's E-Mail:___________ Title of Practicum Position:_________________________________________ Term of Practicum: _____Fall______Winter _____Spring _____Summer Practicum Work Schedule:_________________________________________ Practicum Start Date:__________________ Agreement This contract may be terminated or amended by the student, faculty practicum advisor, or employer at any time upon written notice to the Program Coordinator. If, for any reason, the Practicum is terminated prior to the official ending date, the student will not receive any credit. The student must work a total of 45 hours between the dates set forth for that semester/term. Attendance at each of scheduled Career Development meetings is mandatory. You must complete the entire 45-hour program and attend the assigned meetings. Failure to attend these meetings, complete the guided journal or complete the 45 hours may cancel your participation in this program, forfeit your credit and disqualify you from future participation. Student Signature:__________________________ Date:_______________ Parent/Guardian Signature:____________________ Date:_______________ Worksite Supervisor Signature:_________________ Date:_______________ H.S. Representative Signature:__________________ Date:_______________ -Over- D:\282215094.doc 5/28/2016 Practicum Site Policy Adherence Agreement for Student Program Participants I, the undersigned, acknowledge that I will abide by the regulations and policies of my practicum site host with respect to confidentiality at the worksite, computer and equipment usage and all other regulations and policies set forth by my workplace. I agree to participate in the Workplace Learning Connection Student Practicum Program under the conditions set forth by the Workplace Learning Connection, my high school and my internship site host. ________________________ Student Name Printed ________________________ ___________________ Signature Date Signed Learning Goals for my practicum ( Use the SMART model-specific, measurable, attainable, realistic and timely-please list a minimum of two learning goals for your internship): _______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ ____________________________________ This document will become part of the student's permanent high school career development file when the Internship has been completed. Please make sure all signatures are completed. Please return this form to the address printed below. Thank you! Workplace Learning Connection Linn Regional Center 1770 Boyson Rd Hiawatha, IA 52233 (319) 398-1040 Workplace Learning Connection 1810 Lower Muscatine Rd. Iowa City, IA 52240 (319) 887-3970 Workplace Learning Connection Student Internship Program provides equal opportunity to all persons regardless of age, race, creed, color, sex, national origin, or handicap. The Mission of The Workplace Learning Connection is to develop our future workforce by connecting business and education in relevant, work-based learning activities for K-12 students and teachers in Area 10. Additional career information is available at: www.workplace-learning.org D:\282215094.doc 5/28/2016