TRENDS IN U.S. REGULATORY APPROVALS OF
BIOPHARMACEUTICAL THERAPEUTIC ENTITIES
by
JAMES B. GRAHAM
B.S. Biological Sciences with Honors
Stanford University, 1998
Master of Business Administration
Alfred P. Sloan School of Management, MIT, 2004
SUBMITTED TO THE
HARVARD-MIT DIVISION OF HEALTH SCIENCES AND TECHNOLOGY
IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF
MASTER OF SCIENCE IN HEALTH SCIENCES AND TECHNOLOGY
AT THE
MASSACHUSETTS INSTITUTE OF TECHNOLOGY
JANUARY 2005
© 2005 Massachusetts Institute orTechnology
All rights reserved
Signature of Author
;..
/
;
Harvard-MIT Department of Health Sciences and Technology
2005
_..~~~~~~~_
~January,
Certified by ..........
.
Ernst R. Berndt
Louis B. Seley Professoof Apied Economics, Sloan School of Management
J
Certified by .........
2...A
\2.A....
..........
/
...............
Thesis Supervisor
.........................................
..................................
Isaac S. Kohane
Lawrence J. Henderson Associate Professor of Pediatrics, Health Sciences & Technology
Thesis Supervisor
Accepted by
..
..................................
-
....
...........................................................
Accepte by
Martha L. Gray
Edward Hood Taplin Profe sor of Medical & Electrical Engineering
(rni;reptnr
MThilkinrn
nf
Halth
c.oiepnPs
ndi Tchnnlnnov
v-4
-I
aVI Sv-vv Age -. v-r---nrxvirl-MTT
I.
OF TECHNOLOGY
Ah(WVEd
APR 0 5 2005
An.
I
.BRRE
LIBRARIES
_ _ _____II_
TRENDS IN U.S. REGULATORY APPROVALS OF
BIOPHARMACEUTICAL THERAPEUTIC ENTITIES
JAMES B. GRAHAM
Submitted to the Department of Health Sciences and Technology in partial fulfillment of
the requirements for the degree of Master of Science in Health Sciences and Technology
ABSTRACT
Pharmaceutical productivity, as measured by annual output of new molecular
entities and new therapeutic biologics, has fallen significantly since reaching a peak in
1996. According to Food and Drug Administration (FDA) data, the number of new drug
approvals (new molecular entities and new biologics) fell from 50 in 1996 to 29 in 2003
(FDA-BEP database 2004). Meanwhile, non-inflation adjusted expenditures for research
and development have almost doubled (PhRMA 2004).
This thesis uses time series analysis to characterize historical trends in new drug
introductions. Linear modeling and ARIMA modeling are employed to show that the
large increase in new drug approvals in 1996 is inconsistent with previous trends. The
hypothesis that the 1996 increase in new drug approvals is the consequence of additional
FDA processing capacity pursuant to the implementation of the Prescription Drug User
Fee Act (PDUFA) is considered and rejected, based on an analysis of the underlying
causes of the increase.
Next, approval trends before and after the implementation of PDUFA are
compared. Notably, the percentage of new drug applications resulting in approval has
increased since the implementation of PDUFA while the number of applications reviewed
per year has not changed significantly. The relationship between the success ratio and
drug withdrawal rates is examined, with inconclusive results.
Finally, seasonal trends in new drug application (NDA) submissions and
approvals are described for years preceding and following PDUFA. A significant plurality
of NDA approvals occur in the month of December before and after the implementation
of PDUFA, while December NDA submissions increase in the post-PDUFA period. The
ramifications of these observations on new review guidelines introduced in PDUFA II and
PDUFA III, as well as the implications for NDA submission strategy, are discussed.
Thesis advisors: Dr. Ernst Berndt (MIT Sloan) and Dr. Isaac Kohane (HST)
-3-
Dedication
For Katie, my light and my rock
"We make a living by what we get; we make a life by what we give."
- Winston Churchill
-4-
__
Acknowledgements
The author wishes to thank the following people for their research assistance,
thoughtful discussion, and aid in completing this thesis: Dr. Joseph Bonventre (HST),
Dr. Joseph DiMasi (Tufts CSDD), Bernadette Fendrock (HST), Dr. Howard Golub
(HST), Ed Hass (FDA), Dr. Fiona Murray (MIT Sloan), Dr. Isaac Kohane (HST), and
Marsha Warren (HST).
Professor Ernst Berndt (MIT Sloan) has been an exceptional thesis advisor,
providing guidance, encouragement, and invaluable insights on the nature of the
biopharmaceutical industry. Professor Berndt has generously provided numerous
research materials and many hours of his personal time. Without his help, this thesis
would not have been possible.
Additionally, the author wishes to thank all current students and graduates of the
Biomedical Enterprise Program for their excellent insights on this industry and their
unflagging support. In particular, the author would like to thank Adrian Gottschalk and
Matthew Strobeck, whose research on the biopharmaceutical industry laid the foundation
for many of the analyses presented here. Many of the conclusions presented in this thesis
are the result of discussions with these individuals. All errors are the responsibility of the
author.
-5-
TABLE OF CONTENTS
ABSTRACT
3
......................................................
TABLE OF CONTENTS ................................................................. 6
TABLE OF FIGURES .................................................................................................. 8
1. The significance of productivity in the biopharmaceutical industry .......................... 10
10
1.1
Recent trends in new drug introductions .........................................
1.2
New drug approvals are critical to the biopharmaceutical industry ................. 11
1.3
Balancing profits and productivity in the biopharmaceutical industry ............. 14
1.4
Biopharmaceutical investment in research and development .......................... 17
1.5
Possible explanations for the decline in new drug approvals ........................... 21
1.6
Organizational plan of this thesis ....................................
25
2. Time series analysis of annual new drug introductions 1965-2003 ........................... 27
27
2.1
How should new drug approvals be measured? ........................................
2.2
Rationale for application of time series analyses ..................
2.3
Linear regression on historical observations ....................................
34
2.4
Cyclicality in the biopharmaceutical industry .............................
37
2.5
ARIMA model for NTE approvals ................................................................ 39
2.6
Is the NTE approvals time series mean-reverting? ....................................
2.7
Hypotheses for the decline in NTE approvals since 1996 ............................... 46
3. What factors affect NTE approval volumes
?
.
.................... 33
43
47
..................................
3.1
An inventory model for the NDA approval process ........................................ 47
3.2
Limitations of publicly available data ............................................................. 50
3.3
Population of the NDA inventory model ....................................................... 53
3.4
Calculation of the Success Ratio ................................................................... 57
3.5
Was the increase in NDA approvals in 1996 due to an increase in action
volume, success ratio, or both? .......................................
-6-
____I·_
58
3.6
Dominance of success ratio contradicts the PDUFA hypothesis ..................... 59
3.7
Differences in Action Volume and Success Ratio observed before and after
implementation of PDUFA I .................................................................
3.8
61
Correlation of success ratio and withdrawal rate ............................................ 63
4. Seasonality in NTE Approvals
.
..................................................... 70
4.1
NTE approval volume is elevated in December .........................................
4.2
December effect is driven by a combination of industry submission practices
70
and PDU FA targets ..................................................................................... 71
4.3
December effect was established prior to implementation of PDUFA .......
4.4
NDA submission practices have changed pursuant to PDUFA I ....................78
4.5
PDUFA II review targets have attenuated the December effect for NTE
approvals .........................................
4.6
76
80
Implications of December effect on attainment of PDUFA III targets ............ 81
5. Discussion and conclusions .....................................................
83
5.1
Summary of findings .....................................................
5.2
Future biopharmaceutical industry productivity ............................................. 85
5.3
Better access to NTE filing and approval data is needed ................................ 86
5.4
Towards a systems analysis of the drug development process ......................... 87
83
Bibliography .....................................................
89
Appendix 1: Augmented Dickey-Fuller test ......................................................
93
Appendix 2: ARIMA specification ......................................................
96
Appendix 3: Monthly NTE approvals, 1965-2003 ..................................................... 98
Appendix 4: NDA Flowchart .....................................................
-7 -
100
TABLE OF FIGURES
Figure 1:
FDA NME and therapeutic biological product approvals: 1996-2003 ....................................... 11
Figure 2:
Annual new drug approvals and PhRMA member R&D expenditures 1965-2003 ................... 18
Figure 3:
Exponential curve fit for PhRMA member R&D expenditures, 1965-2003 ............................... 19
Figure 4:
R&D expenditures, total and as a percentage of revenue, 1965-2003 .
Figure 5:
R&D Expenditures by activity type 1999-2002 ............................................................
Figure 6:
Indexed R&D expenditures, Sales and NME introductions 1991-2001 ..................................... 24
Figure 7:
CDER NDA Approvals 1990-2003 ............................................................
30
Figure 8:
NMEs and NCEs by year, 1963-2003 ............................................................
31
Figure 9:
BLA and NME approvals, 1965-2003 ............................................................
33
Figure 10:
New Therapeutic Entity (NTE) introductions, 1965-2003 .......................................................... 34
Figure 11:
New Therapeutic Entity (NTE) introductions with trend line, 1965-1995 ............................... 34
Figure 12:
95% confidence interval for NTE approvals based on 1965-1995 observations ........................ 35
Figure 13:
New Therapeutic Entity (NTE) introductions with trend line, 1996-2003 ............................... 36
Figure 14:
NTE Residuals, 1965-1995 ............................................................
37
Figure 15:
Fourier transform of NTE residuals, 1965-1995 .............................................................
38
Figure 16:
Actual de-trended NTE approvals and fitted model ............................................................
40
Figure 17:
ARIMA (2,1,1) prediction of new NTE approvals, 1996-2003 ................................................... 41
Figure 18:
ARIMA (2,1,1) 95% confidence interval ............................................................
41
Figure 19:
Predicted ARIMA cumulative impulse response .............................................................
42
Figure 20:
Observed NTE approval response, 1996-2003 ............................................................
43
Figure 21:
Three random walk examples with a starting point of 0 and increment of + 0.5 ....................... 44
Figure 22:
Inventory model for NDA flow .............................................................
Figure 23:
Histogram of ratios of NME approvals / NDA approvals by year, 1990-2003 ........................... 51
Figure 24:
Pending NDA volume at beginning of calendar year ............................................................
54
Figure 25:
NDA submissions accepted by calendar year ............................................................
54
Figure 26:
NDA Approvals by calendar year ............................................................
55
Figure 27:
Unsuccessful NDAs - Withdrawals, Non-approvable and Approvable letters ........................... 55
Figure 28:
Comparison of New NDA submissions and NDA exits ............................................................
..............................
20
20
47
56
-8-
__
__
Figure 29:
Net flows in NDA filings under review, 1985-2003 ...................................................
56
Figure 30:
Success Ratio 1985-2003 ....................................................
57
Figure 31:
Action Volume and Success Ratio, pre- and post- PDUFA ...................................................
62
Figure 32:
Safety based NME withdrawals based on year of approval........................................................... 65
Figure 33:
Histogram of drug withdrawals by approval year...................................................
66
Figure 34:
Histogram of years from NDA approval to withdrawal, 1985-2000 .
67
Figure 35:
Success ratio vs. withdrawal rate, 1985-2000 ....................................................
68
Figure 36:
NTE approvals by calendar month, 1965-2003 ...................................................
70
Figure 37:
Review times (in months) for approved NTEs, 1965-1993 ...................................................
72
Figure 38:
Review times (in months) for approved NTEs, 1994-2003 ...................................................
73
Figure 39:
Approved NTE submissions by calendar month, 1965-2003...................................................
74
Figure 40:
NTE approvals by calendar month, 1994-2003 ..............................
Figure 41:
NTE approval percentages by calendar month, 1965-2003 ...................................................
77
Figure 42:
Approved NTE submissions by calendar month, 1965-2003 ...................................................
79
Figure 43:
Approved NTE submissions by calendar month, 2001-2003 ...................................................
80
Figure 44:
NTE approvals by calendar month, 2001-2003 ...................................................
81
...............................
....................................... 75
Table 1:
Upcoming biopharmaceutical product patent expirations ....................................................
13
Table 2:
Biopharmaceutical Mergers and Acquisitions 1988-2000 ....................................................
23
Table 3:
NDA submission type classifications...........................................................................................
28
Table 4:
Percentage of NDA filings designated NME vs. non-NME ....................................................
30
Table 5:
Success ratios, action volumes and NDA approvals 1985-2003 ...................................................
58
Table 6:
Goals of PDUFA I, II, III.....................................................
60
Table 7:
FDA Drug withdrawals 1971-2004 ...................................................
65
-9-
1.
The significance of productivity in the
biopharmaceutical industry
1.1
Recent trends in new drug introductions
The Food, Drug, and Cosmetics Act of 1938 mandated that every new
prescription drug marketed in the United States first receive approval from the U.S. Food
and Drug Administration (FDA). Drug manufacturers must submit to the FDA a New
Drug Application (NDA) comprised of a description of the drug, a statement of its
composition, an analysis of clinical safety data, and a discussion of quality control
protections. The Kefauver-Harris Amendment of 1962 added a requirement for
additional clinical data demonstrating efficacy. NDA approval allows the drug
manufacturer to market and sell the drug in the U.S. market according to labeling
approved by the FDA (Hilts 2003).
According to the FDA Center for Drug Evaluation and Research (CDER), the
NDA process applies to: any new drug molecule, any new salt of a previously approved
drug, any new chemical formulation of a previously approved drug, any therapeutic
combination of two or more previously approved drugs, and any new indication (claimed
use) for a previously approved drug ("NDA approvals" 2003). The FDA uses the term
"new molecular entity" (NME) to denote NDA approvals of the first variety (i.e.,
approvals for new drug molecules). Until recently, NME approvals did not include
biologic drugs, which comprise a growing proportion of marketed therapeutic drugs in the
U.S. (Gosse 1998). Before October 2003, new biological drugs were approved through a
parallel application process called a Biologics License Application (BLA). Since biologic
therapeutics are innovative drugs, the sum of BLA approvals and NME approvals
provides a more accurate measure of the productivity of the biopharmaceutical industry
than NME approvals alone.
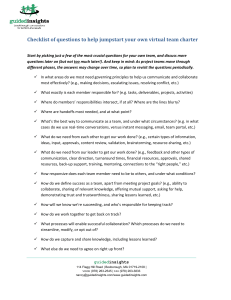
From 1996 to 2003, the number of new molecular entities (NMEs) produced
annually by the pharmaceutical industry dropped from 47 to 20, according to FDA data.
When therapeutic biologic products are included, the total number of new therapeutic
drugs dropped from 50 to 29 over this period, a decline of 42 percent (FDA-BEP
database 2004).
-10-
an
Figure 1:
FDA NME and therapeutic biological product approvals: 1996-2003
Source: FDA-BEP database 2004
The recent decline in new therapeutic products presents a significant challenge to
the biopharmaceutical industry. The 2004 Medco Drug Trend Report cites declining
new drug approvals as the primary driver for reduced prescription drug revenue in 2004
compared to 2003 (2004). The observed decline in the output of new drugs prompted
one industry analyst to pose the question, "Is the pharmaceutical business model
broken?" indicating the potential seriousness of declining new drug approvals on
biopharmaceutical industry profitability (Sylvester 2004). Compared to other industries,
the biopharmaceutical industry relies more heavily on new products to sustain profits and
revenues.
1.2
New drug approvals are critical to the biopharmaceutical industry
While innovation of various kinds is important in all industries, the unique
characteristics of the biopharmaceutical industry make product innovation crucial to
maintaining competitiveness in this industry.
First, from the perspective of long-term industry economics, value is created
primarily by product innovation. Biopharmaceutical companies invest heavily in research
and development, at an average rate of almost 16 percent of revenues (PhRMA 2004).
Studies by Scherer (2001) and Grabowski and Vernon (2002) have shown that profits are
-11-
directly related to research and development investment. Additionally, the U.S. Office of
Technology Assessment has shown that profits are tied to introductions of innovative new
products (1995). Innovative products lead to increased profits by allowing
biopharmaceutical firms to enter new disease treatment markets and expand existing
markets. New products also provide opportunities for competitive differentiation based
on the properties of the drug.
Second, pharmaceutical industry revenues are primarily generated from patentprotected products. When patents expire, generic entry significantly reduces the pricing
power of the branded company and revenues fall sharply. Generic competition reduces
the branded company's profits by eroding its market share and by increasing competitive
pricing pressures (Grabowski 2003). A 1993 study by the U.S. Office of Technology
Assessment found an average of 43 percent erosion in branded-company revenues derived
from a particular drug in the three years following the introduction of a generic
competitor (1993). A U.S. Congressional Budget Office study conducted a few years
later showed that market erosion by generic competitors had increased to 44 percent in
the first year of generic competition for drugs introduced between 1991 and 1993 (1998).
The ability of drug companies to generate profits from marketed drugs is largely
determined by the length of patent protection for marketed products.
Given the rapid revenue erosion associated with the introduction of generic
alternatives, successful biopharmaceutical companies must continually introduce new
patent-protected products to replace revenues lost to the expiration of patents for existing
products. Table 2 shows currently marketed drugs with anticipated patent expiry within
the next two years. In aggregate, these drugs currently account for $26.4B in annual
revenues (IMS 2004). Companies facing impending patent expirations for key products
must urgently seek to develop and introduce new patent-protected products to maintain
revenues and profits.
- 12 -
_I___
_
__
_
Possible
patent
expiration
2003 U.S. Retail
sales ($mm)
Brand name (generic name), manufacturer
Use
3Q2004
Diflucan (flucnazole), Pfizer
Cipro (ciprofioxacin), Bayer
Fungal infections
Bacterial infections
$269
$708
2004
Neurontin (gabapentin), Pfizer
OxyContin (oxycodone -controlled release), Purdue
Pharma
Epilepsy
Pain
$2,069
$1,914
1Q 2005
Celexa (citalopram), Forest
Xalatan (latanorost opthalmic solution), Pharmacia
Depression
Glaucoma
$1,220
$378
Duragesic (fentayl transdermal), Janssen
Pain
$1,063
3Q 2005
Zofran (ondansetron), GlaxoSmith Kline
Nausea
$577
4Q 2005
Allegra (fexofenadine) and Allegra-D
(fexofenadine/pseudoepinephrine), Aventis
Allergies
$1,859
1Q 2006
Lexapro (escitalopram), Forest
Prevacid (lansoprazole), Tap
Depression
Gastroesophageal
refulx disease, ulcers
$900
$3,529
Biaxin (clarithromycin), Abbott
Glucovance (glyburide/metformin), Bristol-Myers
Squibb
Bacterial infections
Diabetes Type 2
$285
$440
2Q 2006
Zithromax (azithromycin), Pfizer
Pravachol (pravastatin), Bristol-Myers Squibb
Baterial infections
Hyperlipidemia
$1,717
$1,680
3Q 2006
Zocor (simvastatin), Merck
Provigil (modafinil), Cephalon
Zoloftf (sertraline), Pfizer
Adderall XR (mixed amphetamine salts), Shire
$3,329
$274
$2,531
$583
Sonata (zaleplon), King
Hyperlipidemia
Narcolepsy
Depression
Attention deficit
hyperactivity disorder
Insomnia
Aciphex (rabeprazole), Esai
GERD, peptic ulcers
$1,000
4Q 2006
Table 1:
$115
Upcoming biopharmaceutical product patent expirations
Source: FDA Orange Book, IMS
Third, the critical role of governmental regulation makes public perception
particularly important for the biopharmaceutical industry. In 1961, the Senate
Committee on the Judiciary issued a report analyzing monopoly power in the
pharmaceutical industry. The committee identified four unique economic features of the
pharmaceutical industry: (1) it has a critical bearing on public health and welfare; (2) it
has a unique distribution system, in which physicians act as purchasing agents for patient- 13-
consumers while insurance companies and government agencies provide payment for
pharmaceutical products; (3) it exhibits inelastic demand for prescription medications;
and (4) it has low manufacturing and distribution intensity, resulting in low marginal
costs and high unit margins (U.S. Congress 1961). The 1962 Kefauver-Harris
amendment (which was informed by the 1961 hearings) and subsequent laws have sought
to balance the monopolistic characteristics of the drug industry, the interests of
biopharmaceutical firms and the needs of the American public.
As a result, the U.S. biopharmaceutical industry is highly regulated. As discussed
previously, FDA approval is required to market any prescription drug. Advertising claims
and product labeling must also be approved by the FDA. Marketing practices designed to
influence physicians are regulated by the FTC and FDA and pricing is influenced by
public health programs such as Medicare and Medicaid (DiMasi 1994).
Currently, proposals to allow drug importation from Canada and to allow Federal
Medicare administrators to negotiate volume discounts with drug companies are being
considered in the U.S. Congress. Implementation of either of these measures would lead
to significant downward pressure on U.S. biopharmaceutical revenues. Because public
opinion influences the policy choices of government, maintaining a positive perception
with the American public is vital to the continued success of the biopharmaceutical
industry.
1.3
Balancing profits and productivity in the biopharmaceutical industry
The pharmaceutical industry currently faces a number of public-relations
challenges including: increasing pressure for drug re-importation; damaging fallout from
the high-profile recall of Merck's COX-2 inhibitor, Vioxx (rofecoxib); and persistent
questions about pharmaceutical marketing practices directed towards physicians and
consumers. In another example of negative publicity, the New York Attorney General's
office recently investigated pharmaceutical manufacturer GlaxoSmithKline for fraud for
its decision not to disclose negative information about the off-label use of its antidepression drug, Paxil (paroxetine), in children (AHLA 2004). In response,
GlaxoSmithKline announced plans to make all clinical trial results available to the public
(Whiting 2004). A survey conducted by Harris Interactive in September 2004 found that
- 14-
____
111111111111
66 percent (+ 3 percent margin of error) of Americans felt that the prices of most
prescription drugs were "unreasonably high." Furthermore, 41 percent of survey
respondents cited "profit margin" as the main contributor to the price of pharmaceuticals,
while 33 percent cited "marketing and sales expenses." Only 22 percent cited "research
and development expenditures" (Harris 2004). High-profile safety failures, questionable
competitive tactics and high prices have created a negative public opinion of the
biopharmaceutical industry.
A simplistic glance at pharmaceutical industry profitability provides evidence
supporting the perception voiced in the Harris survey. As a group, the ten drug
companies in the Fortune 500 topped all three measures of accounting profitability in
2001, according to Fortune magazine's annual analysis of America's largest companies.
Pharmaceutical companies reported net margins of 18.5 percent (eight times higher than
the median), return on assets of 16.5 percent (six times the median), and return on
equity of 33.2 percent (more than three times the median) (Public Citizen 2002). In
2003, the pharmaceutical industry relinquished the top position in these categories, but
remained in the top four in each. The pharmaceutical industry ranked third in net
margins at 14.3 percent, second in return on assets with 10.3 percent and fourth in return
on equity with 22.1 percent (Fortune 2004). In terms of accounting profits, the
pharmaceutical industry is consistently more profitable than most other industries.
Biopharmaceutical firms achieve high accounting profits by exercising pricing
power resulting from high barriers to entry. Products are protected by the robust U.S.
patent system. High up-front costs associated with drug discovery and development
present another significant barrier to entry. These barriers provide limited product
exclusivity for biopharmaceutical firms. This exclusivity allows firms to price drugs
significantly above the marginal cost of production. When patents expire and generic
competition is allowed to enter, prices rapidly fall towards the marginal costs of
production and distribution. Biopharmaceutical company pricing power increases the
cost of pharmaceutical products to consumers by prolonging the time that products are
priced in excess of marginal cost. U.S. spending for prescription drugs is forecast to reach
$520 billion (not inflation adjusted) by 2013, more than twice its current level (Porter
2004). The cost of prescription drugs is substantial and the effects of pricing power by
the biopharmaceutical industry will continue to be felt by healthcare payers.
15 -
Industry defenders argue that the true cost of drug development and the economic
returns needed to justify investment require high accounting profits for marketed drugs.
Joseph DiMasi of the Tufts Center for the Study of Drug Development has published an
estimate of $896mm for the cost of developing a single new drug, including the costs of
failed drug development projects, invested capital and post-marketing clinical trial
obligations (2003). Paul Romer of Stanford University has shown that the promise of
temporary monopoly power can provide significant incentive for innovation (1994).
Many in the biopharmaceutical industry argue that only a credible promise of pricing
power can justify the large, risky investments required for drug development (PhRMA
2002).
The Orphan Drug Act of 1983 provides evidence supporting the hypothesis that
pricing power can spur innovation. The Orphan Drug Act was designed to increase
research and development efforts for rare diseases. Previously, few drug company
resources had been dedicated to developing therapies for rare diseases because the
revenue opportunities in these markets were less attractive than those for larger disease
populations. The Orphan Drug Act increased the relative attractiveness of markets for
rare diseases by legislating a temporary market monopoly for the first company to develop
a treatment for a particular orphan indication. The first product to successfully treat an
orphan indication is granted exclusivity for that indication, and a competing drug can only
enter the market if it is shown to be superior to the first drug (U.S. Congress 1983). The
Act has proven to be very successful. According to Kenneth Kaitin of Tufts CSDD,
between 1983 and 2001, 223 drugs and biological products for orphan diseases were
brought to market. In contrast, the nineteen years prior to 1983 saw approximately 40 to
60 such products come to market (Tufts CSDD 2002).
The Orphan Drug Act represents a successful balancing of the costs and benefits
of incentives for drug development. Although the Act results in higher prices for orphan
drugs, patients benefit by having access to drugs that would never have been developed
otherwise. Because the number of patients treated by orphan drugs is small, the
additional costs of exclusivity for orphan drugs is unlikely to significantly effect the overall
U.S. healthcare budget. For the biopharmaceutical industry overall, balancing the costs
of providing incentives for drug development with the benefits of new therapeutic
products is much more difficult.
- 16-
111-··1·11-·111····II
1
-
·-·
Providing beneficial drugs to those who need them is a social goal as well as a
business goal. In order to promote investment in the development of new drugs, the U.S.
supports regulations which enhance pricing power for biopharmaceutical firms. In
exchange, many expect the biopharmaceutical industry to provide innovative new drugs
that significantly lengthen and improve human life. New drugs with novel mechanisms of
action are more likely to provide significant incremental therapeutic benefit over existing
products. They may have superior efficacy or safety compared to existing products, better
side effect profiles, more convenient routes of administration, lower costs, or easier
distribution methods. At the very least, new drugs increase the number of differentiated
treatment options available to patients and their physicians. Despite continued support
for policies promoting innovation in the drug industry, the number of new drugs has
fallen significantly in the recent past. The factors driving approval trends will be a major
topic of this thesis.
1.4
Biopharmaceutical investment in research and development
Critics from the watchdog group Public Citizen have called for increased
investment in research and development by the biopharmaceutical industry (2002).
However, research and development expenditures have maintained a rapid growth
trajectory, even as new drug approvals have fallen. According to the annual reports of the
Pharmaceutical Research and Manufacturers of America (PhRMA), research and
development spending increased from $16.9B in 1996 to $33.2B in 2003, an increase of
96 percent over the seven year period, reflecting a compound annual growth rate of 10.1
percent (2004).
Though the increase in R&D spending is significant, a few weaknesses in the
PhRMA survey should be noted. First, expenditure data are not inflation adjusted.
Additionally, the PhRMA survey includes research and development expenditure data for
member companies only. The PhRMA member list was compared to Pharmaceutical
Executive magazine's list of the top sixteen biopharmaceutical companies by 2003
revenue (Trombetta 2004). Notably, Forest Laboratories, the fifteenth largest
biopharmaceutical firm, is not included in the PhRMA survey. In addition, it is unclear
whether Genentech (fourteenth by revenue) is included. Although Genentech is not itself
a member of PhRMA, Hoffmann-LaRoche, which owns a majority stake in Genentech, is
- 17-
a member. PhRMA representatives were not able to resolve whether Genentech
expenditures were included in the research and development data reported by HoffinannLaRoche. Other large biopharmaceutical companies not included in the PhRMA survey
include: Allergan, Gilead Sciences, and Chiron. Numerous smaller biotechnology firms
are not included in this survey. Finally, PhRMA survey data is self-reported.
Biopharmaceutical companies may employ different expenditure classification systems,
leading to potential non-standard reporting of research and development expenditures
across firms.
Figure 2 includes new drug approvals for comparison purposes. The number of
new drug approvals, in this case, equals the sum of FDA NDA approvals and biologic
drug approvals. A full discussion of various measures of new drug approvals is presented
in Section 2.1 of this thesis.
35
60
30
50
25 in
J. 40
20 a
30
20 =
z 20
10
10
5
0
1965
1969
1973
1977
1981
1985
1989
1993
1997
2001
Year
Figure 2:
Annual new drug approvals and PhRMA member R&D expenditures 1965-2003
Source: FDA, PhRMA
Various curve fit equations were tested for PhRMA reported pharmaceutical
research and development expenditures from 1965 to 2003. The best curve fit equation is
given by Equation 1, where xrepresents the year and yrepresents R&D expenditures in
USD billions. R 2 for this curve fit is 0.995.
- 18-
Equation 1: Curve fit equation for R&D expenditures, 1965-2003
y = (7*
108 )* eO
251
x
Though an exponential growth model best describes these data, expenditures
exceeded the model's predictions consistently from 1990 to 1995. In addition, research
and development expenditures for 2002 and 2003 are lower than those predicted by the
model. In particular, 2003 expenditures of $33.2B fall $13.4B short of the model's
prediction of $46.6B. This observation may indicate that growth in biopharmaceutical
research and development spending may be slowing after years of rapid growth.
1;n
U
45
a
40
Y. 35
e
30
X
25
C
aI
20
uJ
0 15
W
10
5
1960
1965
1970
1975
1980
1985
1990
1995
2000
2005
Year
Figure 3:
Exponential curve fit for PhRMA member R&D expenditures, 1965-2003
Figure 4 compares industry R&D expenditures to R&D spending expressed as a
percentage of total PhRMA member revenues. Since peaking in 1993, R&D spending
rates have actually declined slightly. Therefore, increases in overall industry revenues
must be driving recent growth in R&D investment.
- 19 -
·Jr
30
20%
18%
30 I
a,
e
16%
25
C
S
14% >
12%
20
a
10%
I
a
15
8%
6%
10
,Xs
26
C
S
a.
X
4%
5
2%
0%
1964
1968
1972
1976
1980
1984
1988
1992
1996
2000
Year
Figure 4:
R&D expenditures, total and as a percentage of revenue, 1965-2003
Source: PhRMA Annual Reports
Figure 5 presents a breakdown of R&D expenditures by development phase
(Cohen 2004). This figure indicates that an increasing portion of R&D spending is being
used for clinical development. Assuming uncategorized expenditures are clinical, clinical
spending as a percentage of total R&D expenditures increased from 35 percent in 1976 to
65 percent in 2002. Conversely, the percentage of expenditures dedicated to discovery
research has fallen by half, from 65 percent in 1976 to 35 percent in 2002.
Distribution of R&D Expenditures
Percent of
100%
total R&D
80%
60%
40%
20%
0%
ill
1976
I
I
,,,,,I
/
1977 1978
I
C--......--J
i
1980
I
I
L..........--I
/
1982
IIII
I
L--.......--I
l
1985
l
1987 1988
I
I
II
l
l
1989
p
l
I
1999 2001
I
l
2002
Year
Clinical Ph 1-3
Discovery
Figure 5:
Uncategorized
R&D Expenditures by activity type 1999-2002
Source: Cohen, 2004 (note years are not sequential)
-20-
·-
3Phase 4
[
I
Regulatory
Additionally, Figure 5 illustrates a marked increase in Phase IV commitments
since 1989. Phase IV studies are carried out after regulatory marketing approval, often in
response to FDA requests for additional long-term safety and efficacy data. In practice,
however, some Phase IV post-marketing studies are designed to enhance the marketing
position of the drug, in addition to satisfying regulatory requirements. Therefore,
nominal Phase IV expenditures may include significant marketing costs. A former
research head of a major pharmaceutical company states that up to 20 percent of the
allocated research and development budget of his group was actually controlled by the
company's marketing department (Douglas 2004). Since this portion of the R&D budget
is not used entirely for R&D purposes, it should be discounted when considering true
research and development expenditures.
As this discussion shows, the aggregate level of biopharmaceutical R&D spending
has never been higher and continues to increase rapidly. However, growth in R&D
spending as a percentage of total pharmaceutical revenues has declined slightly over the
past decade. The allocation of R&D expenditure across development phases has shifted,
from predominantly discovery research in the 1970's and 1980's to predominantly clinical
development today. Within clinical development, an increasing portion of nominal
research and development spending may be focused on marketing, not research, goals
(though this effect is likely small.) Overall, trends in research and development spending
are mixed. However, given the continued growth in overall R&D spending, lack of
investment is unlikely to be the major cause of the observed decline in new drug
approvals.
1.5
Possible explanations for the decline in new drug approvals
The multi-factorial nature of biopharmaceutical productivity makes isolating the
specific cause of falling approvals difficult. Three possible explanations for the observed
decline in biopharmaceutical productivity are summarized below.
First, industry analyst C.J. Sylvester of UBS Investment Research claims that the
industry is "midway in the adoption curve for new technologies, which will likely cause a
near-term decline in productivity" (2004). Sylvester identifies advanced research tools
enabled by the human genome project as the main new technology reducing short-term
- 21 -
productivity. Genomic data and complementary technologies in the areas of proteomics,
systems biology, combinatorial chemistry, and structural biology are increasingly
supplanting traditional target identification and compound screening methods in drug
discovery. These new technologies have dramatically increased the rate of discovery for
medically interesting biological targets.
Based on research conducted by McKinsey and Lehman Brothers in 2001, the
investment associated with implementing these new technologies is expected to increase
research and development costs dramatically (Edmunds, Tanio, and Ma 2001).
McKinsey analysis predicts that genomics, along with proteomics, bioinformatics, and
systems biology advances, will yield numerous novel drug targets. Novel drug targets
carry more risk compared with older, more validated, and better understood targets.
Therefore, as biopharmaceutical companies increasingly base drug development projects
on novel targets, failure rates are expected to rise. A McKinsey model of the R&D
process analyzed the consequences of moving from a drug development program
evaluating 50 targets per year with 30 percent novel content to 200 targets with 70
percent novel content. Applying their probability of success and investment assumptions,
this change would lead to an increase of new drug approvals from 2 per year to 3.6 per
year. However, costs associated with new technology implementation and higher attrition
rates were expected to increase research and development expenditures by up to 100
percent.
In reality, biopharmaceutical firm research and development expenditures are
constrained by market expectations and access to capital. Market expectations for
dividends and retained earnings limit reinvestment of firm profits into research and
development. Biopharmaceutical firms with marketed products usually invest
approximately 16 percent to 20 percent of revenues in research and development and
investors generally penalize biopharmaceutical firms from investing much more or much
less than this. The inability to access capital markets presents a hard limit on research
and development investment for companies without profitable products. In the context of
constrained research and development budgets, the McKinsey analysis suggests that the
implementation of new technologies has the potential to cause a short-term declines in
new drug introductions.
Second, some have argued that recent merger and acquisition activity in the
biopharmaceutical industry has temporarily depressed the output of new drugs as post- 22 -
___
merger integration activities have sapped resources and focus from ongoing drug
development projects. J.P. Garnier, CEO of GlaxoSmithKline recently stated, "Low
R&D productivity across the industry as a whole has affected every major
pharmaceutical player. Just getting bigger is not going to help any more." Mr. Garnier
goes on to state that large acquisitions "would simply be a distraction from what should
be the company's sole focus: producing new drugs" (Management Today 2004).
Number
of unique Percent
of firmsinvolved
Merger
values a
in uniquetransforming Totalmaketvalue of percentof indutry's
Numberdfirms transforming
in sample
mergers(ergemm) marketvalue
Year
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
Total/Average
Table 2:
121
125
134
190
196
212
216
243
267
286
288
302
228
3
12
9
6
3
5
18
12
13
16
21
25
22
165
2.5%
7.2%
5.2%
4.2%
2.6%
1.9%
9.7%
6.2%
5.2%
5.2%
8.3%
9.6%
10.8%
6.5%
1,309
27,971
15,843
1,924
1,325
8,385
37,174
36,732
36,714
20,492
67,741
157,708
100,750
514,068
0.6%
11.8%
5.1%
0.4%
0.2%
1.2%
5.9%
5.2%
4.0%
1.7%
4.5%
7.7%
5.0%
4.4%
Meenmegervalue as a
percentof acquiring
firm'svalue
Meanmergervalue aes
a
percentof tagetfirm's
value
33.2%
44.7%
28.8%
16.7%
32.5%
16.7%
22.8%
19.4%
29.4%
35.7%
27.3%
38.7%
37.2%
29.1%
n/a
121.0%
60.6%
112.0%
92.2%
n/a
110.0%
n/a
88.4%
54.0%
79.1%
118.0%
124.0%
96.9%
Biopharmaceutical Mergers and Acquisitions 1988-2000
Source: Danzon, et al. 2004
In spite of Mr. Garnier's view, the pharmaceutical industry has increasingly
embraced M&A. Table 2 shows that M&A activity has increased in terms of volume and
value. In 2000 (last year of available data), over 10 percent of firms in the
biopharmaceutical industry engaged in some form of M&A. These transactions
accounted for over S$100B in market value (Danzon, et al. 2004). The post-2000 decline
in market valuations of biotechnology and pharmaceutical companies caused market
values of transactions to decline, but transaction volume remains high according to Ernst
& Young's 2003 biotechnology industry report. The distractions associated with business
combinations certainly may have some impact on productivity in the short-term.
A third explanation holds that the decrease in new drug approval volumes can be
attributed to an increased emphasis on blockbuster drugs. Blockbusters, defined as drug
products with over $1B in revenues, accounted for approximately $95B in sales in 2002.
Of the 200 best-selling drugs in 2002, 50 were blockbusters, and they accounted for over
half of the total revenues of the group (Ernst & Young 2003). An increased focus on
- 23 -
blockbuster drugs could result in fewer new drug introductions, albeit with larger value
associated with each introduction.
Managers at Eli Lilly have developed a research and development productivity
model that captures the dynamics of the trend towards blockbusters. The Lilly model
defines biopharmaceutical productivity in two steps: first, R&D efficiency is defined as
the number of new products per unit of input; second, R&D effectiveness is defined as
value (i.e., revenue) created by a particular product (Mason 2004). Figure 6 illustrates
relative trends in R&D efficiency and effectiveness. While R&D expenditures have
continued to increase, the number of NMEs introduced has declined significantly from
1991 levels. Therefore, R&D efficiency has declined. However, sales have continued to
increase, keeping pace with R&D expenditures. By definition, R&D effectiveness (i.e.
revenue per product) has increased substantially.
Indexed growth (1991=100)
50
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
Year
-4- R&D expenditure
Figure 6:
-41- Sales
--
Number of NMEs
Indexed R&D expenditures, Sales and NME introductions 1991-2001
Source: CMR, IMS, Mason 2004
Increasing revenue per marketed product is consistent with a shift towards the
blockbuster model. However, this observation could also be the result of other changes in
the biopharmaceutical industry, such as lengthier patent protection, more favorable
- 24 -
_
__
reimbursement policies, or increased marketing effectiveness. It is unclear whether the
trends identified in the Lilly analysis are the result of an intentional shift in industry
strategy to pursue blockbusters, or if the effect shown in Figure 6 can be attributed to a
handful of unexpectedly market successes. Nevertheless, this analysis shows that while
output quantity (as measured by NMEs) has declined, output quality (as measured by
revenue per new drug) has increased. As a result, the overall revenue growth of the
industry has remained steady, even while the volume of new drug approvals has declined.
1.6
Organizational plan of this thesis
The recent decline in new drug approvals, if real, presents a significant challenge
to the biopharmaceutical industry. This thesis examines data from 1965 to 2003 to more
fully characterize trends and patterns in new drug approvals. Analysis presented in
Section 2 will show that new drug approvals increased steadily from 1965 to 1995,
experienced an unanticipated jump in 1996, and have declined thereafter. In addition,
periodicity in annual approval volumes will be considered. These analyses will provide
quantitative descriptions of features of the new drug approval time series.
Section 3 of this thesis seeks to explain time series trends described in Section 2.
An inventory model of new drug approvals is constructed to provide additional insight
into the factors influencing drug approval volumes. The impact of the Prescription Drug
User Fee Act (PDUFA) is specifically analyzed. This analysis identifies an increase in the
approval percentage of reviewed NDA filings as the major source of the 1996 increase in
new drug approvals. Implications of approval percentages on withdrawal rates are also
considered.
In Section 4, additional time series analysis reveals a seasonal pattern of elevated
new drug approvals in December. The impact of PDUFA on seasonal approval patterns
is discussed, as well. Seasonal workflow patterns at the FDA may affect the
implementation of future PDUFA review goals and should be included in the NDA
submission strategy of drug companies.
In general, the analysis summarized in this thesis shows that the biopharmaceutical
industry is an exceedingly complex system with many dynamic components. It is difficult
to consider any one aspect of the system in isolation due to the high degree of inter- 25 -
relatedness of the system and the large number of simultaneously changing variables.
Nevertheless, this system shows evidence of ordered behavior at the aggregate level.
Annual new drug approval volumes show sustained trends over time and may show
evidence of multi-year periodicity. These features of the system suggest the existence of
systems-level processes. This thesis represents an initial step towards developing a
systems dynamics analysis of drug development. Access to additional data from the FDA
and from the biopharmaceutical industry would enable the construction of a robust
systems model of the drug development process. Such a model could provide valuable
insights into improving the drug development system - leading to more innovative
therapies, a benefit to industry and society.
- 26 -
__
2.
Time series analysis of annual new drug introductions
1965-2003
2.1
How should new drug approvals be measured?
The biopharmaceutical industry provides an excellent source for the quantitative
study of innovation. Biopharmaceutical innovations almost always arrive in the form of
new molecules, which must go through a detailed regulatory review. In addition,
significant modifications to the formulation or administration of an existing drug must
also undergo review. In other industries, innovations are introduced incrementally and
without regulatory documentation. Multiple innovations may be introduced at the same
time, confounding the analysis of benefits provided by each discrete advance. The very
definition of a discrete product can be confusing. Taking personal computers as an
example, the base 2004 Dell Inspiron 1000 has a faster processor and more memory than
the 2003 Inspiron 1000. Should these models be considered as one product, or two? In
addition, this computer (as sold in 2004) has over 25 hardware, software, and service
configuration options available. Based on the conservative assumption that each
configuration option includes two choices (and assuming that configuration choices are
independent of each other), the 2004 Inspiron 1000 has 225 potential configurations
(Dell, 2004). Should each of the over 33 million configurations be considered a separate
product? Analyzing innovation in most industries is difficult and complex.
The biopharmaceutical industry lacks many of the analytical problems associated
with product definition. Rigorous regulatory review is mandated for every marketed
biopharmaceutical product. Each combination of active ingredient, administration route,
dosage level, etc. requires a distinct regulatory approval. In addition, regulatory filings
provide detailed descriptions of products' attributes. Products are clearly delineated and
their attributes are clearly defined and catalogued. Importantly, the public has access to
this information for all approved and marketed biopharmaceutical products. Clear
product definitions and accessible product data provide the basis for detailed analyses of
industry innovation.
Although biopharmaceutical products are more clearly defined and characterized
than products in many other industries, the terminology describing drug approvals is
moderately complex. Slightly different definitions of what constitutes a "new drug"
- 27 -
coexist in the industry. Definitions of new drugs have become more complex as new
technologies have given rise to new classes of drugs and combination products.
All new drugs, formulations, combinations, and dosages must undergo FDA
review. The review process centers on a regulatory filing document called a new drug
application (NDA). A flow chart of the NDA process is included in Appendix 4. NDA
filings are classified with a code that reflects both the type of drug being submitted and its
intended use or uses. Numbers 1 through 7 are used to describe the type of drug:
1.
New Molecular Entity
2.
New Salt of Previously Approved Drug (not a new molecular entity)
3.
New Formulation of Previously Approved Drug (not a new salt or new molecular
entity)
4.
New Combination of Two or More Drugs
5.
Already Marketed Drug Product - Duplication (i.e., new manufacturer)
6.
7.
New Indication (claim) for Already Marketed Drug (includes switch in marketing
status from prescription to OTC)
Already Marketed Drug Product - No Previously Approved NDA
The letters "S" and "P" are used to describe the review priority of the drug:
S.
Standard review for drugs similar to currently available drugs
P.
Priority review for drugs that represent significant advances over existing treatments
Table 3:
NDA submission type classifications
Source: FDA
Priority review is reserved for drug products which, if approved, would be a
significant improvement compared to marketed products in the treatment, diagnosis, or
prevention of a disease. Improvement can be demonstrated by: (1) evidence of increased
effectiveness in treatment, prevention, or diagnosis of a disease; (2) elimination or
substantial reduction of a treatment-limiting drug reaction; (3) documented enhancement
- 28 -
-11---------~-~1
of patient compliance; or (4) evidence of safety and effectiveness of a new subpopulation
(FDA, "Priority review" 1996). Priority applications are usually reviewed more quickly
than standard applications.
Do all NDA filings represent innovations in the biopharmaceutical industry?
Some types of NDA filings may be more or less innovative than others. For example, a
novel therapeutic molecule (type 1 NDA) that cures a previously untreatable, lethal
disease seems to be a more important innovation than a liquid formulation of a medicine
already available in a pill (type 3 NDA). On the other hand, discovering an unexpected
new use for an existing drug (type 6 NDA) may be more innovative than developing a
new therapeutic molecule that is very similar to an existing approved drug (type 1 NDA).
In short, the relative innovative content of different types of NDA filings is subjective. As
a practical matter, measures of innovation in the pharmaceutical industry have focused on
drugs introduced through type 1 NDA filings. This type of drug is referred to as a New
Molecular Entity (NME).
A new molecular entity (NME) is defined by the FDA as a new drug product
containing, as its active ingredient, a chemical substance marketed for the first time in the
United States (Riley and DeRuiter 2004). NME NDA submissions and approvals are the
responsibility of the Center for Drug Evaluation and Research (CDER), a division of the
FDA. Between 1990 and 2003, CDER approved 1171 NDAs. As illustrated in Figure 7,
of these, 399 (34 percent) were New Molecular Entities and 769 (66 percent) were nonNMEs (FDA, "Report" 2004).
- 29 -
140
120
100
80
60
40
20
0
1990
Figure 7:
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
CDER NDA Approvals 1990-2003
Source: FDA
Table 4 shows the percentage composition of NME filings compared to non-NME
filings. 1991 had the highest proportion of NME filings, equaling 48% of all NDA filings.
In 2002, NME filings only accounted for 22% of NDA filings, the lowest proportion in
this sample set.
NME
non-NME
Table 4:
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 Average
37.1% 47.6% 28.6% 35.7% 35.5% 34.1% 40.5% 31.7% 33.3% 42.2% 27.6% 36.4% 21.8% 29.2% 34.4%
62.9% 52.4% 71.4% 64.3% 64.5% 65.9% 59.5% 68.3% 66.7% 57.8% 72.4% 63.6% 78.2% 70.8% 65.6%
Percentage of NDA filings designated NME vs. non-NME
The FDA defines which NDA approvals are, and are not, NMEs. The Tufts
Center for the Study of Drug Development (Tufts CSDD) has defined an alternative to
the NME, the New Chemical Entity (NCE). An NCE is defined to be any new molecular
compound (excluding diagnostic agents, vaccines, and other biologic compounds) not
previously approved for human use by CDER. New salts, esters, and dosage forms of
previously approved compounds are also excluded (Tufts CSDD, "Glossary" 2004). In
practice, compounds that have never been used or tested in human subjects to comprise
NCEs. (Tufts CSDD, "Outlook" 2004).
Figure 8 illustrates the close agreement between FDA-defined NMEs and Tufts
CSDD defined NCEs. The high degree of correlation (correlation = .991) between the
- 30 -
-1-ilIi-----ilil--1-_I______
.
-ii
·_1
1_1__1111_114__1
two measures is reassuring. The difference between NME approval volumes and NCE
volumes is accounted for by a small number of molecules which Tufts CSDD considers to
be diagnostic (and therefore not an NCE), but are counted as NMEs by the FDA
(DiMasi, Interview 2004).
.......
n.....
45
40
35
30
o
25
Z
20
20
15
10
5
0
1963
1967
1971
1975
1979
1983
1987
1991
1995
1999
2003
Year
Figure 8:
NMEs and NCEs by year, 1963-2003
Source: FDA, Parexel Pharmaceutical Industry R&D Sourcebook 2004/2005
Through an ongoing collaboration between the FDA and the Harvard-MIT
Division of Health Sciences (HST), the author has been permitted access to a database
containing detailed information for FDA approved NMEs from 1965 to 2004. Tufts
CSDD does not publish its proprietary list of NCEs. Due to the additional transparency
afforded by the FDA database and the close congruity between FDA and Tufts CSDD
data, this thesis uses NMEs and NME-derived measures for new drug approvals.
Measuring new drug introductions became more complicated with the
introduction of the first therapeutic biologic molecule in 1986. The NME designation
does not include therapeutic biologic entities, an increasingly important drug class.
CDER has historically been responsible for reviewing applications for any new
therapeutic drug. However, due to specific regulatory rules in place in the 1980's, the
first therapeutic biologics were approved not by CDER, but by the Center for Biologics
Evaluation and Research (CBER). Prior to the 1980's, CBER primarily regulated blood
products and vaccines. The first biologic drugs, which were similar to naturally occurring
-31 -
proteins, fell under the purview of CBER. Biologic drugs were approved through the
Biologics License Application (BLA) process, which was similar to the NDA process.
BLA approvals for recombinant protein drugs by CBER increased from a total of 11 for
the period from 1989 to 1996 to a total of 17 from 1997 to 2002. On October 1, 2003,
the FDA transferred product oversight responsibilities for new therapeutic biologics
applications from CBER to CDER (FDA, "Transfer" 2004). As of that date, all new
drugs, regardless of composition, go through the NDA process under the aegis of CDER.
As the biopharmaceutical industry has continued to evolve, the separation of
biologic and small molecule drugs into different classes has become less relevant to the
structure of industry competition. Drug development companies often pursue
development programs in both biologic therapies and small molecule drugs to address a
target or pathway. Large pharmaceutical companies, which traditionally specialized in
small molecule drugs, have expanded into biological drug development by expanding
internal capabilities and by partnering with biotechnology firms. Likewise, some large
biotechnology companies have begun to conduct research on small molecule drugs.
Although some differences between the two classes of therapies persist (particularly with
respect to manufacturing, packaging, route of administration, and side effect profiles), for
the purposes of competitive analysis, small molecule drugs and therapeutic biologic drugs
are close substitutes in practice (M. Porter, 2000).
In this thesis both small molecules and biologics will be included in measures of
innovation. The term "New Therapeutic Entity" (NTE) will be used to denote the sum
of NMEs and new biologic drugs. Figure 9 shows annual NME and biologics approval
volume in a stacked area chart. The sum of approval volumes of NMEs and new biologic
drugs equals NTE approval volume from 1965 to 2003.
- 32 -
_
I
60
50
40
_
E 30
20
10
0
1965
Figure 9:
2.2
1969
1973
1977
1981
1985
Year
1989
1993
1997
2001
BLA and NME approvals, 1965-2003
Source: FDA-BEP database
Rationale for application of time series analyses
Previous analyses have sought to relate the level of new drug approvals to various
explanatory variables, for example R&D expenditures (Jensen 1984) or the presence of a
confirmed FDA Commissioner (Gottschalk 2004). However, the stochastic nature of
drug development, the changing regulatory environment and the changing composition of
the industry have complicated these analyses. In addition, much relevant data on the
drug development process is proprietary and confidential. Biopharmaceutical firms
maintain control over data contained in regulatory filings, making a complete analysis of
unapproved filings impossible. Some filing data is made available at the time of NDA
approval, but information regarding non-approved drug candidates is often impossible to
access. Industry-level statistics are limited to aggregate numbers reported by secondary
sources such as Parexel or Tufts CSDD.
Because granular data is not available, this thesis focuses on a careful analysis of
macro-scale trends and patterns in time series of approval volumes - with few assumptions
about the underlying causes of changes in approval patterns. By characterizing the
historical behavior of NTE approvals since 1965, I will attempt to develop insights into
the underlying dynamics of the biopharmaceutical industry.
- 33 -
Linear regression on historical observations
2.3
Figure 10 depicts NTE approval levels from 1965 to 2003. NTE approvals were
regressed against a time index (1964 = to) to yield a linear trend for NTE approval growth
from 1965 to 2003.
60
50
*
40
f
30
IZ
20
10
-
1965
1970
1980
1975
1985
1990
1995
2000
Year
Figure 10:
New Therapeutic Entity (NTE) introductions, 1965-2003
Source: FDA-BEP database
By inspection, the large number of NTE approvals in 1996 (50) seems
inconsistent with historical trends (i.e. it is an outlier.) The number of NTE approvals in
1996 was 51 percent higher than the 30 approvals in 1996, the next most prolific year.
35
30
25
a
20
X
.
l
15
10
5
1965
1970
1975
1980
1985
1990
Year
Figure 11:
New Therapeutic Entity (NTE) introductions with trend line, 1965-1995
Source: FDA
- 34 -
1995
In the years preceding 1996 (1965 - 1995), NTE approvals grew at a roughly
linear rate of approximately .48 NTEs per year. R2 for the 1965-1995 period is .57. Is
the large number of NTE approvals in 1996 anticipated by prior historical data? Data
from 1965 to 1995 was used to construct a linear model for NTE approvals. A 95
percent confidence interval for the expected approval volume (NTEt) was also
constructed:
Equation 2:
(NTE,) = 0.4762t + 10.316 + e
where t represents the year index (1964=0) and £ represents the variance of the model.
The regression yielded a standard error of 3.8. Under the assumption that e is normally
distributed with a mean equal to 0, Figure 12 depicts the 95 percent confidence interval
for (NTEt) based on observations from 1965 to 1995. Predicted NTE approvals are
estimated by projecting historical trends forward through the 1996-2003 period.
an
OU
50
m 40
g
g
30
U
20
10
1965
1970
1975
1980
1985
1990
1995
2000
Year
Figure 12: 95% confidence interval for NTE approvals based on 1965-1995 observations
Figure 12 shows that the number of NTE approvals in 1996 exceeds the upper
bound of the 95 percent confidence interval. Interestingly, approvals in 1991 also exceed
the upper bound of the 95 percent confidence interval, though by a much smaller margin.
Assuming the standard error calculated from 1965-1995 data, the chance that 1996
approvals would total 50 or more, compared to the expected value of 25.6, is 7.04*10 -1 1.
- 35 -
This simple analysis provides evidence that the high number of NTE approvals in
1996 is not anticipated by historical trends. In addition, the linear trend in NTE
approvals changes significantly after 1996. As shown in Figure 13, the slope of the linear
regression line changes from .57 to -3.05. R2 for this linear curve fit is .84.
UU
*
it
_
an~~~~~~~~~~~~~~~
..........
_
40
CL 30
I
. . .. .
: 20
y = -3.0476x + 48.714
2
R = 0.8407
..
..
10
1996
1997
1998
1999
i~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
2000
2001
2002
2003
Year
Figure 13:
New Therapeutic Entity (NTE) introductions with trend line, 1996-2003
Source: FDA-BEP database
Based on these figures, a simple linear regression model that reasonably describes
the behavior of NTE approvals in the 1965-1995 period fails to describe behavior in 1996
and afterwards. This could be due to at least two causes: either the original model was
incorrect and a more robust model can capture the behavior observed data, or the
underlying dynamics of the time series changed in 1996. If the latter is true, is the
departure from the historical trend permanent or temporary? A prolonged downward
trend in U.S. NTE approvals would likely have negative consequences for the
biopharmaceutical industry.
In order to incorporate cyclicality in this model, additional time series techniques
were applied to NTE approval volumes. Section 2.4 describes the results of Fourier
transform analysis used to characterize industry-level cycles in biopharmaceutical NTE
approvals. Section 2.5 summarizes the results of an ARIMA analysis which incorporates
autocorrelation and moving average terms in the prediction of NTE approvals.
- 36 -
c
I
2.4
Cyclicality in the biopharmaceutical industry
Duncan Moore and Andrew Baum of Morgan Stanley have observed that the
pharmaceutical industry is "much more cyclical than investors have given it credit for"
(2004). They cite macroeconomic cycles, product cycles and intellectual property cycles
as cyclical influences on pharmaceutical productivity.
Charting linear regression residuals reveals some evidence of cyclicality in NTE
approvals. By inspection, relative peaks of approvals occur in 1967, 1970, 1974, 1977,
1981, 1985, 1989, and 1991. Years between these local maxima are 3, 4, 3, 4, 4, and 2,
respectively. Evidence of negative autocorrelation also exists, as local maxima are
generally followed by declines.
12
1 1111~
· -·
·
........
.........
10
8
6
'a
4
nA
2
0
z
·o
A A
-
/K
(2)
(4)
(6)
L
(8)
1965
I
1970
1975
1980
1985
1990
1995
Year
Figure 14: NTE Residuals, 1965-1995
A Fourier transform was conducted to quantitatively analyze observed evidence of
cyclicality. Fourier analysis was conducted using SigView32, version 1.9.1.0 (SigView
2004). Prior to applying the Fourier transform, the following operations were applied to
the time series:
*
Linear trend was removed, resulting in residual plot shown in Figure 14
*
Zeros were expanded by a factor of two
*
Hamming window was applied
- 37 -
Transformation was done using the Cooley-Turkey Fast Fourier Transform
(FFT) algorithm (Harvey 1998). Results are displayed in Figure 15.
--...
CA$
. '
'o
.
......
./
,,,.
....
i,
.
DM
01
.
0t1S
I
0.2
31
Ii
I
i
4
I
44
Cycles per year
Figure 15: Fourier transform of NTE residuals, 1965-1995
Peak magnitude occurs at a frequency of .266 cycles per year, corresponding to a
period of 3.8 years. Using the method described by Koopmans (1974), a 95 percent
confidence interval was constructed for the peak frequency magnitude. The 95 percent
interval for the peak value has a lower bound of 0.349, which is higher than the mean
magnitude of the distribution (0.326).
Therefore, a frequency peak corresponding to a
period of 3.8 years is significantly different from the mean of the sample.
However, this Fourier peak fails to achieve 95 percent significance under Siegel's
more stringent test for spectral peak confidence (SigView 2004). In addition, the peak
shows significant spreading across the spectrum range (i.e. the peak is not crisply
defined.) Two major limitations in source data may reduce the power of this Fourier
analysis. First, the data set contains only 31 observations, too few to provide a high signal
to noise ratio. Second, the data set is divided into discrete annual units, which prevents
analysis at shorter time intervals. Analysis of data on monthly and quarterly bases was not
helpful due to large seasonality in approval patterns (discussed in detail in Section 4.) In
short, this analysis shows qualified evidence of cyclicality. Although this analysis does not
support definitive statements on multi-year cyclicality in NTE approvals from 1965 to
1995, it does provide support for application of ARIMA modeling tools, which can
incorporate cyclicality into the model of approval volumes.
- 38 -
-
-
--
-
----
2.5
ARIMA model for NTE approvals
Given evidence of periodicity discussed in Section 2.4, an attempt was made to
incorporate periodic fluctuations into the model of NTE approvals. In order to more fully
capture the periodic fluctuations of this time series, an Autoregressive Integrated Moving
Average (ARIMA) model was used to predict model behavior in 1996 and years
subsequent based on time series data for the 1965-1995 period. Multiple ARIMA
specifications were tried and the resulting analysis is presented in Appendix 2.
Differencing, autocorrelation, and partial autocorrelation were used to specify a stationary
and invertible ARIMA model.
An ARIMA model predicts future states of a particular time series based on past
behavior of the series. Two types of terms are employed in ARIMA models:
autoregressive terms and moving average terms. The autoregressive term extrapolates
variance terms for the current data point based on the observed variance of previous
points. The moving average term helps predict the current term by taking a weighted
average of previous terms. These tools can be applied to a basic time series. However, if
the time series is non-stationary, it must be differenced to produce a stationary series. An
ARIMA model combines autoregressive and moving average tools with the technique of
differencing to achieve stationarity (Pindyck and Rubinfeld 1997).
Using the E-views software application (E-views 2004), various ARIMA
specifications were compared. The best and most parsimonious fit was achieved with an
ARIMA (2,1,1) model. The first term (2) refers to the degree of autocorrelation.
Autocorrelation coefficients are estimated for the (t-1) and (t-2) terms. Interestingly, in
this specification, the AR(1) coefficient was not significant; however, the AR(2) coefficient
was significant. Overall the ARIMA (2,1,1) specification yields an Akaike's Information
Criterion (AIC) score of 5.4. The AIC is a number used to compare econometric
models, and is expressed algebraically as: AIC=ln (sm2) + 2m/T, where m is the number
of parameters in the model, and sm2 is the estimated residual variance: sm2 = (sum of
squared residuals for model m)/T. That is, the average squared residual for model m
(Primedia 2005).
The black line in the top section of Figure 16 represents the first difference of
NTE approval time series data from 1965-1995. The ARIMA (2,1,1) model predictions
are shown in gray. Residuals are plotted in the lower region of the graph (dotted line) and
- 39 -
do not show signs of significant heteroskedasticity, though 1991 represents a significant
deviation from the ARIMA prediction.
,-
5
0
1968 1970 1972 1974 1976 1978 1980 1982 1984 1986 1988 1990 1992 1994
Residual
Actual
Fitted
Figure 16: Actual de-trended NTE approvals and fitted model
The ARIMA (2,1,1) model shows a reasonable fit for the observed data. The
initial time series is non-stationary because it exhibits cyclical fluctuations with variable
period. If the period of fluctuation was reliably three years or four years, periodicity could
be filtered using common seasonal adjustment techniques. Because the period of cycles
varies from two to four years, simple seasonality adjustments are impractical. To achieve
stationarity, the ARIMA model was specified using first differences of observed NTE
approvals. The middle term (1) of the specification parameters refers to the first-degree
differencing used in this model.
The specified ARIMA (2,1,1) model was used to develop a counterfactual
prediction for NTE approvals for years 1996 through 2003. Figure 17 shows actual
historical approvals, predicted approvals for 1996-2003 and actual approvals for 1996- 40 -
_I___
__
2003. The ARIMA model predicts a slight up-tick in NTE approvals in 1996, but not
nearly the increase actually observed.
1965
1970
1975
1980
..... ARIMA(2,1,1) forecast
1985
1990
1995
2000
Aual NTE
Figure 17: ARIMA (2,1,1) prediction of new NTE approvals, 1996-2003
A 95 percent confidence interval for the ARIMA prediction was constructed using
the E-views software package and is included in Figure 18. In 1996, the 95 percent
confidence interval ranges from approximately 22 to 36 NTE approvals. As mentioned
earlier, the actual number of approvals in 1996 was 50, far greater than the upper bound
of the 95 percent confidence interval of the prediction.
40
Forecast: TOTALF
Actual: TOTAL
Forecast sample: 1996 2003
Included observations: 8
35.
30.
Root Mean Squared Error
Mean Absolute Error
Mean Abs. Percent Error
Theil Inequality Coefficient
Bias Proportion
Variance Proportion
Covariance Proportion
25.
20-
.........
'
.
. .........
15.
10
1996
-
1997
I 1
1998
I
1999
1
2000
I
2001
~
I
2002
Forecast NTE
Figure 18: ARIMA (2,1,1) 95% confidence interval
- 41 -
24003
10.73393
8.113892
20.45698
0.167604
0.401575
0.354632
0.243792
In conclusion, basic time series analyses show that the number of new NTE
approvals in 1996 is not anticipated by historical behavior prior to 1996. Using a linear
regression model derived from historical approval trends, the probability that 50 NTE
approvals would occur in 1996 by chance alone is less than 1 in 14 billion, indicating that
the observed result is highly unlikely given the estimated linear model. A more
complicated ARIMA analysis resulted in a prediction of approximately 28 NTE approvals
in 1996, with the upper bound of the 95 percent confidence interval of 36 NTE
approvals, significantly below the observed 50.
Finally, the E-views analysis package was used to predict the theoretical effect of a
one-time shock to the system under the ARIMA (2,1,1) model. Figure 19 shows the
predicted behavior of the ARIMA system as it returns to equilibrium after a one time
displacement of 32, which approximates the number of observed NTE approvals (50) in
excess of the number expected under the specified ARIMA model (28.) This analysis
predicts that NTE approvals will follow a dampened oscillation pattern as they return to
long term trends. Significant deviations from the expected trend persist for five or six
years until the system regains equilibrium. The dotted lines in Figure 19 represent the
confidence interval estimation + two standard deviations from the predicted mean.
Accumulated Response ± 2 S.E.
An
'4
u
-
200I
%\`· f
I
I
I
I
sI-----…-
-20
-40-
2
I
I
4
6
I
8
10
I
I
12
I
14
I
16
I
I
18
I
I
20
I
I
22
I
24
Year
Figure 19:
Predicted ARIMA cumulative impulse response
Figure 20 shows actual deviations in NTE approvals after 1996 compared to the
long-term observed from 1965 to 1995. As predicted by the ARIMA impulse response
model, the number of NTE approvals seems to gradually revert back to the long-term
trend. However, the specific behavior of the time series does not correspond to the
- 42 -
-----
-
predictions of the ARIMA impulse model. For example, the ARIMA model predicts a
large drop in the second year after impulse to a relative minimum below the long-term
trend. While the observed data shows a local minimum in the second year after 1996, the
minimum is not as dramatic as predicted by the ARIMA model. As predicted by the
ARIMA model, the system seems to be moving back towards equilibrium at long-term
growth rates. Additional data for years after 2003 will be needed to confirm this
prediction.
Zo
20
15
10
5
(5)
(10)
(1 SI
1996
1997
1998
1999
2000
2001
2002
2003
Year
Figure 20: Observed NTE approval response, 1996-2003
2.6
Is the NTE approvals time series mean-reverting?
These ARIMA predictions imply that the NTE approval time series is mean-
reverting, i.e. fluctuations away from the long-term trend of the systems are followed by
reversions to back to the trend. The Dickey-Fuller test provides an alternative means to
test for mean-reversion behavior in time series (Pindyk and Rubinfeld 1997).
The Dickey-Fuller test starts with the null hypothesis that the time series follows a
random walk. A random walk is a class of time series where each term is defined by the
previous term plus a change drawn independently from a probability distribution with a
mean of zero.
Yt = Y,-l + et
- 43 -
where Et has an expected value of 0, the expected value of (Et Es) is also 0, and s
E,
implying no autocorrelation with previous terms. A simple random walk can be
constructed according to the following rules:
(1) Choose a starting point
(2) Fix the absolute value of the change from one point in the path to the next as
constant.
(3) Starting from the last point, choose the direction of the change from that point to the
next. Direction is chosen at random and no direction is more likely than any other
For example, a random walk can be generated by successive flips of a fair coin, where
heads results in adding 0.5 and tails results in subtracting 0.5 from a starting point of 0.
Figure 21 shows examples of three trials of such a random walk.
10
6
4
2
0
-2
-4
-6
0
2
4
6
8
10
12
14
16
18
20
22
24
26
28
30
32
34
36
38
40
42
44
46
48
50
Figure 21: Three random walk examples with a starting point of 0 and increment of + 0.5
It can be shown that for each point Yt in a random walk series, all future points
have an expected value of yt. The standard deviation of a point I steps in the future is
given by /02 . The average straight-line distance between start and finish points of a
random walk of n steps is on the order of 4 (n). In fact, if "average" is understood in the
sense of root-mean-square, then the average distance after n steps is exactly 4(n) times the
step length (Pindyk and Rubinfeld 1997).
Whether a series follows a random walk has implications for the statistical analyses
applicable to the series. For mathematical reasons, common regression techniques may
yield spurious results when applied to random walks. At each point, the random walk
- 44 -
_
·I____· _·_·I·___1_
path is equally likely to move away from or back towards the starting point. Therefore,
the random walk is a purely stochastic process.
Practically, whether a series follows a random walk has implications for
understanding the underlying dynamics of the system and for predicting future points of
the series. Economists, Charles Nelson and Charles Plosser found evidence indicating
that GNP time series behaves like a random walk (1982). This observation challenged
the validity of earlier models that used other variables to predict GNP or assumed that
GNP growth reverted to long-term trends (Pindyk and Rubinfeld 1997). In A Random
Walk Down Wall Street, Burton Malkiel provides evidence that equity markets also
follow random walks. He argues that the random walk nature of the stock market makes
technical investing techniques futile in long term investing (1999). Studies subsequent to
Nelson and Plosser have found random walk behavior in many markets, including lumber
and tariff rates (Pindyk and Rubinfeld 1997)
External shocks to a random walk system would be expected to lead to lasting
effects on the subsequent time series. Because the system does not mean-revert, the effect
of a shock would be expected to last indefinitely. Therefore, if NTE approvals follow a
random walk, the effects of an one-time increase in NTE approvals would be expected to
linger. If NTE approvals are mean reverting, a one-time increase in approvals would be
followed by a decline back to the long-term trend.
Application of the Dickey-Fuller test to NTE approval data from 1965 to 1995
yields an F-statistic of 7.315. This analysis is presented in detail in Appendix 1. This Fstatistic value implies rejection of the random walk null hypothesis with 95 percent
confidence. Therefore, the NTE approval series is mean-reverting. The E-views software
package was also used to calculate the Dickey-Fuller F-statistic using an updated table of
F-statistics (McKinnon 1996). This analysis yielded an F-statistic consistent with
rejection of the random walk null hypothesis at the 99 percent confidence level. These
analyses predict that the system of NTE approvals will react to a one-time displacement
by reverting to the mean. These findings are consistent with the observation that the large
increase in NTE approvals in 1996 is followed by a decline back to the long-term trend.
- 45 -
2.7
Hypotheses for the decline in NTE approvals since 1996
Many hypotheses regarding the recent decline in NTE approvals attribute the
decline to new trends in the industry - i.e. a more stringent regulatory environment, more
regulatory delays, merger activity, adoption of new technologies, and similar trends.
These hypotheses are based on the assumption that underlying factors in the industry are
driving the observed decline.
Analysis presented in this Section presents the alternative hypothesis that the basic
dynamics of the industry have not changed. Rather, the biopharmaceutical industry
experienced a one-time surge (outlier) in new drug approvals in 1996 and has
subsequently been reverting to long-term trends in new approval volume. Section 3
elaborates an inventory model of NDA submissions and approvals to isolate the drivers
behind recent drug approval trends. This inventory model will enable more detailed
estimation of specific factors (e.g. new NDA submission volumes, approval rates, NDA
inventory levels, etc.) contributing to the observed behavior of the NTE approval time
series.
- 46 -
_-11__1-
·
-I-
_ _
3.
What factors affect NTE approval volumes?
3.1
An inventory model for the NDA approval process
Section 2 suggests that the increase in NTE approvals was not anticipated by
trends and cycles present in previous years. Did some underlying factor in the NTE
approval process change in 1996 to induce the observed increase in NTE approvals? Why
have NTE approvals been declining since 1996? This section investigates the drivers
behind changing trends in NTE approvals in recent years. The overall number of
approvals is disaggregated into component terms in order to isolate key factors in the
approval process. While this analysis does not yield the root cause of the rise and fall of
NTE approval volume, it does shed additional light on the underlying dynamics of the
observed system behavior.
Figure 22 illustrates an extremely simplified model of the drug approval process
from NDA submission to approval. A more detailed process diagram is included in
Appendix 4. This diagram pertains to approvals within a particular year. NDA
applications enter the review process for a particular year through two routes: (1) as
backlog carried over from the previous year and (2) as new NDA submissions received
during the year.
1
.k-||-"-||
: ill
iii
iiiw
ii··1
mill
X
?·····1
I·
i
·
m
lilllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllll
Figure 22: Inventory model for NDA flow
- 47 -
"Backlog" consists of all in-process NDA filings in the system at the beginning of
each calendar year and is equal to the number of outstanding applications at the end of
the previous year. The PAREXEL Pharmaceutical Industry sourcebook provides NDA
backlog data for the years 1984 to 2004 (Mathieu 2004).
New NDA submissions are applications submitted and accepted for filing during
the current calendar year. At the time of submission, the FDA checks each application
for completeness. The FDA may refuse to accept applications that do not contain all
required data and documentation required. The FDA specifies three criteria for rejecting
a new drug application (1993):
-
Omission of a section of the NDA required under 21 CFR 314.50, or incomplete
or haphazard presentation of such sections. Specific sections checked include:
comprehensive table of contents, accurate and complete summary of the
application, required technical sections (legible and properly labeled) with
integrated summaries, and complete tabulated case reports.
-
Clear failure to include evidence of effectiveness compatible with approval.
Specifically, this includes adequate, well-controlled clinical study data from at
least two trials with relevant endpoints.
-
Omission of critical ancillary data needed to evaluate effectiveness, safety, and
recommendations for use. These data include: animal carcinogenicity studies,
animal reproduction studies (for drugs that may be administered to women of
childbearing age), dose-finding studies, and safety database data and analysis.
This outcome is labeled "refusal-to-file" and results in issuance of a "refusal-to-
file" letter. Imclone's application for Erbitux, submitted in 2000, resulted in a highprofile refusal-to-file letter. CEO Samuel Waksal and his acquaintance, Martha Stewart,
traded Imclone shares prior to the company's disclosure of receipt of this letter, leading to
convictions for insider trading and obstruction of justice, respectively (Hays 2004).
Applications that meet filing requirements and are accepted by the FDA comprise "New
Submissions" in Figure 22.
Accepted new drug applications combined with backlog applications outstanding
at the beginning of the year define the pool of applications that can potentially be
- 48 -
I
_
_
approved by the FDA in a given calendar year. This pool is represented as "Active
NDAs" in Figure 22.
Active NDA filings can exit the review process in one of two ways. They may be
withdrawn by the sponsor or they may be reviewed by the FDA. Withdrawals occur prior
to official FDA action. This exit path is denoted by the "Withdrawals" box in Figure 22.
Increasingly, NDA sponsors voluntarily withdraw submissions and resubmit revised
applications at later dates (Medco 2004, Hass 2004). PDUFA articulates clearly-defined
review period targets for new NDA filings starting at the date of acceptance. Review
performance guidelines for amended applications, however, are less well-defined. Thus,
for applications that require amendments, withdrawing and resubmitting a revised
application may lead to a faster approval than amending existing applications piecemeal.
The pool of active NDA filings remaining after withdrawals are subtracted
comprise the pool of actionable NDAs. Active NDAs for which no decision is issued in
the calendar year remain in inventory and feed into backlog for the next calendar year
(denoted by the dotted arrow in Figure 22.) When the FDA officially reviews and issues a
decision on an active NDA filing, it may issue one of the three decisions: "nonapprovable", "approvable" or "approved" (FDA 1993).
A non-approvable letter indicates that the NDA has not satisfied the FDA's
standards for safety or efficacy. Non-approvable letters often indicate serious problems
with the potential product and sponsor sponsors often choose to forego additional
development on programs deemed "non-approvable." Non-approvable NDAs that are
resubmitted often require additional clinical trial data or expensive new Phase III clinical
trials. A non-approvable letter is a significant setback for a drug development program.
The second type of letter is an "approvable" letter, which indicates the NDA may
be approved if certain deficiencies and questions are answered appropriately. Approvable
letters may or may not specify the deficient areas of interest to the reviewers. Often the
NDA's deficiencies can be addressed through continued dialogue between the sponsor
and the agency, additional statistical analysis of existing data, or performance of additional
small studies in animals or humans. Additional information is submitted to the FDA in
the form of revisions or addenda to the current application.
- 49 -
The third type of action is issuance of an approval letter. An FDA approval grants
the sponsor the right to publicly market the drug in compliance with FDA restrictions on
labeling, advertising, indications, and patient targeting. Approvals represent success for
the sponsor, and are almost always announced by a company press release. In addition,
NDA approvals are tracked and published by the FDA.
Considered together, the various input and outcome states included in Figure 22
represent a complete model of the NDA approval process. Populating the described
model with available data, will provide a basis for drawing conclusions about causes of
recent trends in drug approvals.
3.2
Limitations of publicly available data
The time series analysis presented in Section 2 focused on NTE approvals. As
discussed previously, NTE approvals are defined as the sum of NME applications
approved by CDER and BLA applications approved by CBER. NTE approvals are one
reasonable measure of the innovative output of the biopharmaceutical industry and
represent a subset of all NDA approvals. As shown in Figure 7 and Table 4 on page 30,
approximately 34 percent of all NDA approvals from 1990 to 2003 were classified as an
NME/NTE. All biologic drug BLA filings are considered to be NTEs.
Unfortunately, the data required to populate the inventory model presented in
Figure 22 for NTE applications is not available publicly. Therefore, the inventory model
analysis was performed on overall NDA applications, not the specific subset of NDA
applications designated as NTEs. This weakens the conclusions drawn from the
inventory analysis because they are not directly comparable to the time series results
found in Section 2. In addition, general NDA filings include many applications for items
with relatively little innovative content (e.g. product line extensions for related indications
or small changes in buffer formulation.)
Nevertheless, an inventory model may provide some insight into changes in the
NTE approval process, if ratios of NTE approvals and filings to overall NDA approvals
and filings remain consistent over the observed period. The ratio of non-NME approvals
- 50 -
_____
I_
to overall NDA approvals remains fairly consistent for the period from 1990 to 2003, as
shown in Figure 23.
8.0
I
(.U -'
E 6.0
t
I
' 4.0
- --
E. 3.0
E
, 2.0 1 0
.
i
0.0 I ----. ..
0.175
..
17.5%22.5%
-- -
-- -
22.5%27.5%
27.5%32.5%
32.5%37.5%
37.5%42.5%
.--
42.5%47.5%
47.5%52.5%
Ratio of NME approvals to Total NDA approvals
Figure 23: Histogram of ratios of NME approvals / NDA approvals by year, 1990-2003
For the fifteen years in the sample, seven years had a ratio of NME approvals to
total NDA approvals of between 32.5% and 37.5%. Assuming that the ratio of NME
applications to overall NDA filings is similarly consistent, one can infer trends in NTE
filings and approvals based on NDA filings and approvals. This approach is not optimal,
but is the most practical approach given the lack of public data on NTE filings.
Why is NME filing data not available? First, the information contained in NDA
filings is proprietary to the sponsor. Biopharmaceutical industry sponsors are
understandably protective of the specifics of NDA filings. Competing firms could use
information in regulatory filings to inform their drug development strategy. Companies
could attempt to copy products being developed by competing firms. They could also
develop marketing messages that seek to preemptively attack competing drug programs
while they are in NDA review.
Second, data on NME filings is difficult to compile due to complexity in the
definition of an "NME filing." While the definition of an approved NME is well
established and straightforward, the definition of an "NME submission" is more complex.
At the time of submission, NDAs are classified into one of the seven types enumerated
previously in Table 3. Type 1 NDA submissions are basically "NME submissions."
However, this definition is complicated by the fact that multiple NDA submissions for the
- 51 -
same molecule can simultaneously be classified as type 1 (Hass 2004). A hypothetical
example may help clarify this concept:
Drug company A develops a therapeutic molecule that has various effects on the
human immune system. The company discovers that the molecule is effective in
treating three distinct autoimmune diseases: multiple sclerosis, Crohn's disease,
and rheumatoid arthritis. The FDA requires separate NDAs for each proposed
indication. Therefore, the drug company prepares and files three distinct NDAs
at approximately the same time. Each application is classified as type 1 and
accepted into the NDA review process. For any of a number of possible reasons,
one of the three applications is approved before the other two. By definition, the
first approved NDA for this molecule is considered the NME approval. When the
first application is approved, the other two applications are reclassified as type 6
(in this example). If the two other applications are eventually approved, they will
not be considered NMEs. Rather they will be additional indications for the
previously approved drug.
Because of this, there is not a 1:1 relationship between type 1 NDA submissions
and approved, rejected or withdrawn NMEs. Adjusting NDA counts to exclude duplicate
type 1 NDAs for the same molecule proved impractical due to limitations in the data
available from internal FDA tracking systems and a lack of available research resources.
Finally, reliable, consistent information on NDA withdrawals, approvable letters
and non-approvable letters is unavailable from public sources. Public companies must
issue press releases for material events, however, criteria for materiality are subjective and
at the discretion of the sponsor company. For large companies, NDA withdrawals or
non-approvable letters may be justfiably considered "non-material" if the decision does
not significantly affect the expected financial performance of the firm. Furthermore,
private companies are not under SEC obligation to publish press releases on events,
material or otherwise. Due to incomplete reporting of unsuccessful NDAs, it is
impossible to compile a complete record of the outcomes of all NDA filings based on
public data. Ideally, data on all process outcomes (i.e. withdrawals, approvals, approvable
letters, and non-approvable letters) could be incorporated into the model. As a practical
matter, only information on approvals is reliably available. As a result, only two process
outcomes are considered in this analysis: NDA approvals and everything else.
- 52 -
_I
_____
"Everything else" includes withdrawals, approvable letters and non-approvable letters.
The term "Unsuccessful NDAs" is used to denote these outcomes.
3.3
Population of the NDA inventory model
In order to construct a simple inventory model, we must have the following data:
(1) beginning and ending inventory, (2) new submissions, (3) new approvals and (4) new
rejections and withdrawals. Combining these relationships provides a means for
calculating inventory backlog:
i
Initial inventory
(backlog at end of previous year)
+
New NDAs submitted and accepted
Sponsor withdrawals
Non-approvable decisions
Approvable decisions
Approval decisions
Ending inventory
(backlog at end of the year)
Rearranging the terms of this relationship, withdrawn, non-approvable and approvable
NDA filings can be expressed in terms of beginning and ending inventory, new
submissions, and approvals.
Equation 3:
Starting Inventory
+ New Submissions
- New Approvals
- Ending inventory
= N u+
-
Withdrawals
W
Non-approvable decisions
+ Approvable decisions
A new variable, "Unsuccessful NDAs", is defined as the sum of withdrawals, nonapprovable decisions and approvable decisions. Populating the right side of equation with
- 53 -
data reported by Parexel and the FDA enables calculation of unsuccessful NDAs by year.
Plots of right-hand side variables are shown in Figures 24-26. A plot of Unsuccessful
NDAs is shown in Figure 27. All plots are shown on the same scale to aid comparison.
NDAs pending at beginning of year
JUU
-~
250
200
150
100
50
A
1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Figure 24: Pending NDA volume at beginning of calendar year
Source: PAREXEL Pharmaceutical Industry Sourcebook 2004/2005
NDA Submissions
"'.!
II
............
....__............
.....
___
........
.....-
250
200
150
100
50
0
1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Figure 25: NDA submissions accepted by calendar year
Source:, FDA
- 54 -
NDA Approvals
300
250
200
150
100
50
0
1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Figure 26:
NDA Approvals by calendar year
Source: PAREXEL Pharmaceutical Industry Sourcebook 2004/2005
Unsuccessful NDAs
--
-
-
250
200
150
100
50
0
1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Figure 27:
Unsuccessful NDAs - Withdrawals, Non-approvable and Approvable letters
The most notable trend from these plots is the decrease in the number of
outstanding NDAs, from 272 in 1985 to 102 in 2003. This steady, prolonged decrease
indicates that more NDAs are leaving the FDA approval process than are entering. As
shown in Figure 28, exiting applications significantly outnumbered entering applications
in 1986, 1990-1992, 1996, and 2000. New submissions significantly outnumbered
exiting NDAs in 1989, 1999, and 2003.
- 55 -
New submissions vs. Approvals and Unsuccessful Applications
---n
zuu
175
150
125
100
75
1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Figure 28: Comparison of New NDA submissions and NDA exits
Figure 29 plots the difference between new submissions and exiting applications to give
net flows of NDA filings into the review process. Large negative flows occurred in 1986
and 2000. Given the large number of NTE approvals recorded in 1996, a large negative
outflow in NDA filings was expected for that year. Interestingly, NDA net flows are only
moderately negative for 1996.
Net flows in NDA filings under review
I._
qU
20
0
-20
-40
-60
-An
1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Figure 29:
Net flows in NDA filings under review, 1985-2003
- 56 -
···YLYLILII·I·III1111
_·_
_·· _
I
I
3.4
Calculation of the Success Ratio
The inventory analysis presented in Section 3.3 also enables the calculation of a
ratio of successful (i.e. approved applications) to all NDA exits.
Equation 4:
SuccessRatio =
Approvals
(StartingInventory- EndingInventory)+ NewSubmissions
This ratio captures the true "success ratio" of NDA submissions by including
withdrawals as well as non-approvable and approvable decisions. Figure 30 illustrates the
wide variance in the success ratio over the period from 1985 to 2003. Success ratio values
vary from a low of less than 50 percent in 1991 to highs of approximately 90 percent in
1989, 1996 and 1997.
Success Ratio
-en
II .WU
0.900
0.800
0.700
0.600
0.500
0.400
1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Figure 30: Success Ratio 1985-2003
The FDA does not publish a success ratio or ratios of non-approvable, approvable
and approved applications. However, the 2000 PDUFA performance report to Congress
did cite an increase in the percentage of filed NDAs that ultimately gained approval from
approximately 66 percent in the years prior to the enactment of PDUFA to 80 percent
- 57 -
after PDUFA (FDA 2000). These approximate approval rates are consistent with the
success ratios shown in Figure 30.
The success ratio can be linked to overall approval volume by multiplying it by the
number of NDAs acted upon in a particular year, as shown in Equation 4.
Equation 5:
NDAApprovals = Action Volume * SuccessRatio
where "action volume" is defined as the sum of all FDA decisions (i.e. approvals,
approvable letters and non-approvable letters) plus sponsor withdrawals. Since complete
data on withdrawals is not available, they cannot be separated from other NDA process
exits. Table 5 shows action volumes, success ratios and NDA approvals for recent years.
Year
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
Table 5:
3.5
Action Volume
151
185
132
121
98
124
137
126
99
112
123
146
135
130
113
151
99
117
94
Success Ratio
66.2%
53.0%
52.3%
55.4%
88.8%
51.6%
46.0%
72.2%
70.7%
55.4%
66.7%
89.7%
89.6%
69.2%
73.5%
64.9%
66.7%
66.7%
76.6%
ADprovals
100
98
69
67
87
64
63
91
70
62
82
131
121
90
83
98
66
78
72
Success ratios, action volumes and NDA approvals 1985-2003
Was the increase in NDA approvals in 1996 due to an increase in
action volume, success ratio, or both?
Table 5 allows for the disaggregation of drivers contributing to elevated NDA
approvals in 1996 compared to previous years. 49 more NDAs were approved in 1996
- 58 -
compared to 1995, an increase of 60 percent year over year. Both the success ratio and
action volume increased as well. The success ratio increased from 66.7 percent in 1995 to
89.7 percent in 1996 and action volume increased from 123 in 1995 to 146 in 1996.
The relative contribution of action volume and the success ratio can be calculated
by estimating the increase in NDA approvals attributable to one of these variables while
holding the other constant. Holding the success ratio constant at the 1995 level of 66.7
percent and multiplying by the increase in action volume from 1995 to 1996 results in an
estimated increase of 15.3 NDA approvals. The converse calculation holding the action
volume constant yields an estimate of 33.7 NDA approvals attributable to the increase in
success ratio. From this, we can calculate the percentage of the 1996 increase attributable
to increase in the success ratio (68.7 percent) versus the increase attributable to increase
in action volume (31.3 percent). While increases in action volume and success ratio both
contribute to the increase in NDA approvals in 1996, the success ratio effect dominates
the action volume effect by a more than 2:1 margin.
3.6
Dominance of success ratio contradicts the PDUFA hypothesis
One hypothesis for the increase in 1996 approvals holds that the implementation
of the Prescription Drug User Fee Act of 1992 (PDUFA) provided additional application
processing capacity for FDA review. Prior to 1992, the FDA required an average of two
and a half years to review an NDA, with some review periods stretching well over eight
years. Many observers in industry and at the FDA attributed the length of review times to
lack of processing capability, or throughput, at the FDA. Inadequate processing
capability was attributed to resource constraints at the FDA. Applications sometimes
remained unexamined in FDA backlog for months or years. Officials at the FDA
concluded that the approval process could be accelerated with additional resources,
particularly additional reviewers. Funds for additional reviewers were not available in
existing FDA budgets and the U.S. Congress did not appropriate additional funds for this
purpose. As a result, the FDA considered alternative means to solve its resource
problems.
- 59 -
The Prescription Drug User Fee Act of 1992 (PDUFA I) was an attempt to
address the resource problem. It established, for a five-year period, a mandatory fee of
roughly $200,000 to be submitted by sponsoring companies at the time of NDA
submission. PDUFA funding allowed the FDA to add many new employees and invest
more heavily in information technology. After the implementation of PDUFA, observed
average processing time fell by half, to eighteen months (FDA 1998). Because of this
success, the Food and Drug Administration Modernization Act of 1997 (FDAMA)
reauthorized user fees for an additional five-years and increased the user fee schedule
(PDUFA II). The user fee arrangement was authorized again in 2002 (PDUFA III) as
part of the Bioterrorism Preparedness and Response Act of 2002 (FDA 2004). In order
to partially justify the collection of user fees from biopharmaceutical industry sponsors,
the FDA agreed to institute performance goals under PDUFA. Essentially, the FDA
committed to meeting measurable performance targets specifically related to response
times and decision speed. Performance goals for PDUFA I, PDUFA II, and PDUFA III
are summarized in Table 6.
Goal
PDUFA
I
Complete review of priority original new drug and biologic 90% within 6 months
applications and efficacy supplements
Complete review of standard original new drug and biologic 90% within 12 months
applications and efficacy supplements
PDUFAII
PDUFA II
90% within 10 months
Complete review of manufacturing supplements
90% within 6 months
90% within 4 months if prior approval needed, 6 months otherwise
Complete review of resubmitted new drug and biologic
applications
90% within 6 months
90% of Class in 2 months and 90% of Class 2 in 6 months
Complete review of resubmitted efficacy supplements
No Goal
90% within 6 months
Discipline review letters for pre-submitted 'Reviewable
units" of new drug and biologic applications
No Goal
90% in 6 months
Report of substantive deficiencies (or lack thereof)
No Goal
90% within 14 days of filing date
Respond to industry requests for meetings
No Goal
90% within 14 days
Meet with industry sponsor within set times
No Goal
90% within 30, 60 or 75 days, depending on type of meeting
Provide industry sponsor with meeting minutes
No Goal
90% within 30 days
Communicate results of complete industry responses to
FDA clinical holds
No Goal
90% within 30 days
Resolve major disputes appealed by industry
No Goal
90% within 30 days
Complete review of special protocols
No Goal
90% within 45 days
Electronic application receipt and review
No Goal
Inplace by the end of FY 2002
Table 6:
90% of Class I in 2 months and
90% of Class 2 in 6 months
IEnhanced by the end of FY 2007
Goals of PDUFA I, 11,111
Source: Table adapted from Gottschalk, 2003. FDA "Reauthorization"2004.
- 60 -
--- --
---II---------
As mentioned above, the implementation of PDUFA resulted in a 50 percent drop
in review times. Incremental resources provided through user fees and the additional
accountability imposed by publicized performance goals both likely contributed to an
increase in the volume of applications reviewed and acted on by the FDA, driving down
review times. Notably, PDUFA did not set goals for approval volume or ratio - only
response times. Therefore, the success ratio discussed in Section 3.4 would not be
expected to change a priori.
Did the increase in NTE approvals in 1996 result from the increased processing
capacity, or throughput, provided through PDUFA? This hypothesis is consistent with
the observed drop in approval times. However, if increased throughput was, in fact, the
primary driver for the rise in NDA approvals in 1996, action volume would be expected to
be the major contributing factor of the increase in NDA approvals.
As discussed in Section 3.5, observed data do not support the hypothesis that
increased throughput primarily led to increased NDA approvals in 1996. The effect of
the increase in success ratio outweighed the effect of increased action volume by more
than a 2:1 margin. This result was unexpected and provides evidence against the
hypothesis that PDUFA-associated throughput gains drove the 1996 increase in NDA
approvals.
3.7
Differences in Action Volume and Success Ratio observed before
and after implementation of PDUFA I
This finding prompted a more general analysis of changes in action volume and
success ratio before and after the implementation of PDUFA I. In FDA publications, the
PDUFA period is defined as beginning on January 1, 1994. Accordingly, for this analysis,
the pre-PDUFA period is defined beginning from the first available data point (1985)
through the end of 1993. The post-PDUFA period is 1994-2003.
- 61 -
Action Volume
-In
1OU
Success Ratio
fn
,r
l,L
I) Hnn
730 /U
-
/0
0.600
100
0.400
50
0.200
0
,
pre-PDUFA
0.000
0.000
,
,
pre-PDUFA
post-PDUFA
post-PDUFA
Figure 31: Action Volume and Success Ratio, pre- and post- PDUFA
Figure 31 illustrates the changes in action volume and success ratio before and
after the implementation of PDUFA. The additional resources provided by PDUFA
would be expected to increase overall action volume; instead, a six percent decrease is
observed. Although this observation runs counter to expectations set by PDUFA, it could
be partially explained by the general decline in NDA backlog shown in Figure 24. In
order for the FDA to process NDA filings, the industry must first supply them. It is more
difficult to explain the 16 percent increase in the success ratio in the post-PDUFA era
compared to the pre-PDUFA era. PDFUA itself does not stipulate targets related to
overall approvals or approval ratios.
Some have argued that the user fee arrangement of PDUFA has aligned the FDA
too closely with the interests of the industry that it is charged with regulating (E. Porter
2004). Each iteration of PDUFA legislation (PDUFA I, II, and III) has included a
renewal requirement which requires Congress to reauthorize the user fee arrangement for
five additional years. It is conceivable that the five-year PDUFA renewal process has put
pressure on the FDA to work more closely with the biopharmaceutical industry so that
drug manufacturers will support renewal. The threat of losing user fees and therefore
having to cut staff and other expenditures may make the FDA more receptive to the
interests of sponsors (FDA Review 2004). FDA reviewers may have a more favorable
inclination towards industry priorities in the post-PDUFA environment. Since obtaining
NDA approval is the highest priority of drug company sponsors, one might expect
approval rates to increase.
- 62 -
1111
A number of alternative hypotheses could also account for the observed increase in
success ratio. First, the increase in success ratio may be due to improved NDA quality.
As biopharmaceutical companies have matured, they may have become more adept at
conducting clinical research, selecting good drug candidates and generating complete,
accurate regulatory filings. Industry consolidation has put a larger number of new drug
applications in the hands of the experienced regulatory affairs departments of large
companies. Second, an increase in the number of "me-too" drugs which follow a
mechanism of action of a precedent drug may have removed some regulatory risk from the
approval process. The existence of related precedent drugs with well-documented safety
records may help sponsors address FDA questions regarding safety and efficacy. Third,
additional FDA review resources may lead to better interaction between the
administration and industry. FDA reviewers may have more time to work with industry
sponsors to address actively weaknesses in potential applications. In this way, additional
FDA resources could lead to higher quality regulatory filings and a higher success ratio.
Although the reasons for the increase in the success ratio are unclear, any trend that could
compromise historically high standards for safety and efficacy of U.S. drugs should be
thoroughly examined. More research is needed understand the reasons for the increase in
the NDA success ratio.
3.8
Correlation of success ratio and withdrawal rate
The FDA conducts post-marketing surveillance of marketed drugs and can order
the withdrawal of any drug that proves to be unacceptably risky or ineffective. A drug
withdrawal occurs when the FDA determines that the risks associated with a marketed
drug outweigh its benefits. Usually the FDA issues a Public Health Advisory detailing the
specific risks of the drug. If the risk is serious enough to merit an official withdrawal
proceeding, the sponsor company usually voluntarily withdraws the drug from the market
(Meadows 2002). An analysis was conducted to examine whether the withdrawal rate is
correlated to the success ratio of a particular year. A regression of annual withdrawal
rates against success ratios yields an R2 of .21. The coefficient of the explanatory term is
.039 and the p-value is .078. This analysis provides some evidence for a weak positive
correlation between success ratio and withdrawal rate. However, the effect does not reach
- 63 -
95% significance. Furthermore, the explanatory coefficient is very small which implies
that the success ratio must change dramatically to get even a small increase in withdrawal
rates.
According to Sidney Wolfe, Director the Health Research Group, "changes in
FDA review and approval policies in the past several years appear to have led to a
significant decline in the safety and efficacy standards for new drugs" (2002). The
withdrawal rate - the percentage of drugs eventually withdrawn out of all drugs approved
in a particular year - is a common way to measure the effectiveness of the FDA review
process. Drugs that are initially approved by the FDA and later withdrawn are usually
perceived as "mistakes" in the approval process. This perception may be misleading,
however, as some drugs withdrawals are due to errors in prescribing, widespread
inappropriate use of the drug, or violation of FDA-approved prescribing and usage
warnings. In some cases, withdrawals do not indicate a mistake by the FDA, but rather
an inability of doctors or patients to use the drug responsibly. In addition, some safetybased withdrawals are the result of exceedingly rare side effects that would have been
almost impossible for the FDA to have foreseen (Meadows 2002)
The 2003 FDA Report to the Nation addressed the issue of drug withdrawals
prior to PDUFA and under PDUFA. Between January 1, 1971, and December 31, 1993
the FDA approved 477 new molecular entities, of which 13 (2.7 percent) were eventually
withdrawn. Nearly all the drugs approved in this period were received before the FDA
implemented PDUFA review goals. Between January 1, 1994 and April 30, 2004, the
FDA approved 303 NMEs, and 7 (2.3 percent) have been withdrawn. Drugs approved in
this period were reviewed after the implementation of PDUFA (FDA 2003). These
results are summarized in Figure 32.
As Figure 32 indicates, the total percentage of withdrawals in the post-PDUFA
era (2.3 percent) is less than the withdrawal percentage for years prior to PDUFA (2.7
percent). However, these data do not include the recent withdrawal of rofecoxib (Vioxx),
which was approved in 1999. When it is included as a withdrawal, the post-PDUFA
withdrawal percentage increases to 2.6 percent. This is still comparable to withdrawal
rates prior to the implementation of PDUFA. Therefore, the evidence does not support
the assertion that PDUFA has led to an increase in withdrawal rates.
- 64 -
_
I
______·
·__I
·
_·_
_
111_ 1__··__
__
3.00% -
2.7%
C
"L;· r-cli- s···'
2.3%
:,
Cu
0
.Q::,: 1F6;;iC?
Z 2.00% -
d·: (::".·r:·;
- ;···· ·······
I· :-:'': ··· :
9. :·-:i...
:···:...I : ··.·
"::·
13_
c 1.00%
a)
C
C.)
a)
0.00%
-----
,-------
pre-PDUFA (13)
---
PDUFA (7)
Figure 32: Safety based NME withdrawals based on year of approval
Table 7 summarizes data for all FDA approved drug withdrawals since 1971.
Notes
Withdrawn drua
ADDroval year Withdrawal year
2000 Never approved by FDA
Phenylpropanolamine
Fenfluramine
1973
1997
Azaribine
1975
1976
Ticrynafen
1979
1980
Zomepirac
1980
1983
1982
1982
Benoxaprofen
Nomifensine
1984
1986
1987
Suprofen
1985
Terfenadine
1985
1998
Encainide
1986
1991
Astemizole
1988
1999
1992
1993
Flosequinan
Temafloxacin
1992
1992
Cisapride
1993
2000
Dexfenfluramine
1997 Not an NME
1996
Bromfenac
1997
1998
Cerivastatin
1997
2001
Grepafloxin
1997
1999
Mibefradil
1997
1998
1997
Troglitazone
2000
Rapacuronium
1999
2001
Alosetron*
2000 Returned to market in 2002 with restricted distribution
2000
Rofecoxib
1999
2004
Table 7:
FDA Drug withdrawals 1971-2004
- 65 -
Figure 33 shows withdrawal volume by year of FDA approval. The
implementation of PDUFA in 1994 is denoted by the dotted line. The most interesting
feature of this histogram is the comparatively large number of withdrawals (5) in 1997.
This chart includes the withdrawal of rofecoxib in 2004.
Withdrawals by Approval Year (1973-2003)
7-
Al[~~~~~
*
~PDUFA
50
c 4-
e 3U.
2-
1-
I~~~~~+n~8nd+4
+
0-
1973
1979
1985
1991
1997
2003
Year
Figure 33: Histogram of drug withdrawals by approval year
Source: FDA
As the September 2004 withdrawal of rofecoxib illustrates, withdrawals may lag
approval by many years. To date, the longest lag between approval of a drug and its
withdrawal is 24 years - for fenfluramine, a weight loss drug. The lag between approval
and withdrawal may generate misleading results when withdrawal trends are analyzed too
soon after approval. Figure 34 illustrates the distribution of lag times between NDA
approval and withdrawal for drugs withdrawn since 1985.
In 1999, the FDA produced a chart comparing drug withdrawal rates before and
after the implementation of PDUFA in 1994. This analysis compared withdrawal rates
for approvals in the four years before PDUFA to the four years after PDUFA. The chart
indicated a withdrawal rate of only 1.2 percent in the four years (1994-1998) under
PDUFA at that time (FDA 1999). Since then, four additional drugs from the 1994-1998
approval cohort have been withdrawn from the market. In fact, 1997 approvals have the
- 66 -
111111111·11·····11111
--
I
--
highest withdrawal rate of any on record. In this example, the FDA analyzed withdrawal
data to quickly after approval, and therefore underestimated the withdrawal rate.
Years from NDA approval to withdrawal (1985-2000)
?r
o -t
5
t
4t
X
3 -
2
~ ~~~~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
·:-
J
-
--
1
I1
0
5
15
10
Years on market
20
25
Figure 34: Histogram of years from NDA approval to withdrawal, 1985-2000
Source: FDA
The calculation of success ratios in Section 3.4 enables the comparison of success
ratios with withdrawal rates. Withdrawal rates for a particular year were calculated by
dividing the number of withdrawals for drugs approved in a particular year by the number
of NDA approvals in that year. Withdrawal rates (independent variable) for 1985-2000
were regressed against calculated success ratios (explanatory variable) for those years.
Data for years after 2000 were not included because approval was too recent to ensure a
meaningful estimation of the withdrawal rate.
- 67 -
Success ratio vs. withdrawal rate (1985-2000)
x no/
J.U/O -
0
4.0% S
'
3.0% -
·
2.0%-
0
0
0.0%
40%
0
*
1.0% ......-O--d
--
50%
o
0
a,
-----
60%
0
0
O
~
70%
I ,
80%
O
90%
100%
Success ratio
Figure 35: Success ratio vs. withdrawal rate, 1985-2000
The regression results are summarized in Figure 35. Regression of withdrawal
rate against success ratio yields an R 2 of .21. The coefficient of the explanatory term is
.039. Thus, for each 10% increase in the success ratio, the expected withdrawal rate will
increase .39%. From 1985 to 2000 the average number of NDA approvals per year was
approximately 84. Therefore, for an average year, a .39% increase in withdrawal rate
corresponds to an additional .32 withdrawals. In other words, if these regression results
are valid, the success ratio must increase by over 30% to increase the expected number of
withdrawals in an average year by 1. The highest success rate in the data set is 85 percent
(in 1984) and the mean success rate for the period analyzed was 75 percent. For an
average year, it is impossible for the success ratio to increase by more than 25 percentage
points and unlikely that it will increase by any more than 15. This constraint on success
rate fluctuations further mitigates its potential impact on withdrawals.
Although a relationship between success ratio and withdrawal rate may exist, it is
weak. In addition, the coefficient of the success ratio explanatory term fails to reach 95
percent significance in this regression analysis (p-value = .078). The 95 percent
confidence interval for this explanatory variable also includes 0, indicating that the success
ratio could be positively or negatively related to withdrawal rate. Finally, much of the
observed effect is driven by one year, 1997. Five drugs approved in 1997 were later
- 68 -
withdrawn from the market. Incidentally, 1997 also had a relatively high success ratio. If
data from 1997 are excluded from the analysis, the p-value associated with the
explanatory variable drops from .07 to .23. In other words, the regression result is not
robust.
Nevertheless, given that only sixteen withdrawals were recorded for NDAs
approved from 1985 to 2000 and only nine years in the 1985-2000 window had any
withdrawals, an explanatory variable p-value of .078 is fairly low. Although the current
analysis does not definitively support the conclusion that success ratio and the withdrawal
rate are related, these variables should continue to be monitored as additional data
becomes available. In addition, comparing the success ratio of only type 1 NDA filings to
withdrawal rates would be a more relevant and specific analysis, since only type 1
approvals have ever been withdrawn.
A statistically significant relationship between the success ratios and withdrawal
rates would add support for industry critics who argue that less stringent FDA approval
policies increase public health risks. On the other hand, rejecting a relationship between
success ratio and withdrawal rate would lead to the conclusion that the FDA approval
rates (within reasonable bounds) do not significantly affect withdrawal rates - and,
consequently, do not influence public health risk.
- 69 -
4.
Seasonality in NTE Approvals
4.1
NTE approval volume is elevated in December
Using the FDA/BEP database described previously, quarterly and monthly
seasonal trends in NTE approvals were charted and analyzed. Appendix 3 includes a plot
of NTE approvals by month from 1965 to 2003. This time series reveals a pronounced
increase in NTE approvals in the month of December. A histogram of NTE approvalmonth frequency is shown in Figure 36. For the 966 NTEs approved between 1965 and
2003 (inclusive), 217 were approved in the month of December (approximately 22.5
percent.) This observation is consistent with analysis published by the Tufts Center for
the Study of Drug Development, which noted an end-of-year surge in approvals in an
1998 Tufts CSDD Impact Report. According to Tufts data, 107 NCE approvals from
1995 to 1997, 29 (27.1 percent) occurred in the month of December (Tufts 1998).
The data presented in Figure 36 was analyzed using a X2 test to determine whether
the December increase in NTE approvals is significant. The X2 statistical test for
uniformity yields a test statistic of 279.8, corresponding to a p-value of 1.58*10-53. The
hypothesis that monthly NTE approvals follow a uniform distribution is rejected with very
high confidence.
NTE APPROVALS BY CALENDAR MONTH (1965.2003)
zou
217
~
200 ::·.:
····
II
, 150
z
;·:
a:i
:::
0 100
oLU 5
:: 50
64
54
42
61
60
78
i":
.··-
71
-··.t
0
I
T
1
2
I
-a
_II
3
4
_42_
7377 LIA-~
.
5
6
7
MONTH
8
Figure 36: NTE approvals by calendar month, 1965-2003
Source: FDA
- 70 -
____I·
9
10
11
12
When the month of December is excluded, the x2 test applied to NTE approval volumes
for other months fails to reject the uniform distribution hypothesis at the 95 percent
confidence level. The number of NTE approvals for January through November
approximately follow a uniform distribution. The large number of December NTE
approvals significantly differs from the approval volumes of other months. The elevated
volume of NTE approvals in December compared to other months is referred to as the
"December effect."
4.2
December effect is driven by a combination of industry submission
practices and PDUFA targets
Reasons for the December effect are unclear. Through personal communication,
FDA economist Ed Hass suggested that a combination of industry NDA submission
practices and PDUFA-specified review targets have resulted in the observed increase in
December approvals. For NDAs submitted after the implementation of PDUFA I,
elevated December NDA submissions coupled with the PDUFA twelve month review
target, may lead to an elevated number of December approvals. This hypothesis will be
referred to as the submission hypothesis.
New drug applications are subject to PDUFA-specified review times. PDUFA I
set review targets of six months for priority applications and twelve months for standard
applications (FDA, "Reauthorization" 2004). Based on these targets, FDA approval
decisions delivered in accordance with PDUFA guidelines would be expected to lag NDA
submission dates by six or twelve months, assuming that reviews are delivered near their
respective deadlines. If NDA submissions are elevated in particular month, PDUFA
review guidelines could lead to subsequent increases in approvals six and twelve months
later. Anecdotal evidence suggests that industry sponsors submit more new drug
applications in December compared to other months. Therefore, it is hypothesized that
the December effect is the result of elevated industry NDA submissions in December and
June, combined with review periods approximating the PDUFA-specified six and twelve
month maximum. This hypothesis was tested by examining monthly NDA submission
volumes and analyzing FDA review times.
- 71 -
FDA review times have changed significantly since 1994. Since PDUFA I was
passed into law in 1992 the FDA has been successful in meeting most of the targets
specified in the legislation. After implementation of PDUFA I targets in 1994, the
percentage of NDAs reviewed within PDUFA guidelines increased from 55 percent in
1994 to 90 percent in 1997 (FDA, "Performance Report" 2002). The impact of PDUFA
on review times is evident in histograms comparing approval times before and after
January 1994.
Approved NTE review times in months (pre 1/1994) n=586
100 T
I
--
OU oni
O 60e
r
40-20
0
-
0
i oU
.WU
U 12.0
4iu
6.0
18.0
BuPUM.UIiUI
24.0
30.0
36.0
42.0
48.0
Month bins
Figure 37: Review times (in months) for approved NTEs, 1965-1993
Source: FDA. Bin 49 includes all review times greater than 48 months
Figure 37 shows the distribution of review times for NTE applications approved
from 1965 through 1993. Approval volumes increase steadily as review times lengthen
from one month to twelve months. Volumes then reach a plateau from twelve to 24
months. After 24 months, approval volumes gradually decline. Notably, over 13.6
percent of NTE approvals had review times greater than 48 months. Although not shown
here, volumes for review times greater than 48 months continue to decrease
asymptotically to zero for review periods between 49 and 136 months. The lengthiest
review period in this sample was 136 months (eleven years, four months) for the 1984
approval of Janssen's pimozide. Although detailed statistical analysis was not performed,
no specific review periods predominate in the sample. Instead, the distribution of review
- 72 -
-
-
-·-··
·-.·
-··---·-
-_·_·
.··-__
times seems to gradually rise, plateau and decline, with a moderate level of stochastic
variability throughout the sample.
In contrast, review periods of six and twelve months dominate the distribution of
review times after January 1994, as shown in Figure 38. Unlike the distribution of review
times prior to 1.994, this distribution exhibits large spikes in approval volumes at six and
twelve month time periods. 11.6 percent of NTE applications approved after January
1994 were approved in six months, and 12.4 percent were approved in twelve months. In
addition, in the post-1994 sample, only 4.1 percent of NTE applications require more
than 48 months for review, although this number may be artificially low due some
submitted, but yet-to-be-approved, applications are likely not included in the sample.
Approved NTE review times in months (post 1/1994) n=363
1Ann
80
oc
60
a
40
LL
20
a~n~pan$/n~uea~·-n·4ip~non
~aa-
0
0
6.0
12.0
18.0
24.0
30.0
Month bins
36.0
I9
3 -"-
42.0
48.0
Figure 38: Review times (in months) for approved NTEs, 1994-2003
Source: FDA. Bin 49 includes all review times greater than 48 months
Figure 38 provides support for the assumption that PDUFA I has increased the
number of NTE applications approved six and twelve months after submission. The
proportion of six month to twelve month approvals is approximately 1:1, with slightly
more twelve month approvals. This is basically consistent with the observation that 60
percent of NTE applications were classified as standard reviews and 40 percent as priority
reviews over the 1994-2003 period. The implementation of PDUFA I has led to a
marked increase in the proportion of six and twelve month review times. Therefore,
- 73 -
elevated volumes of NTE application approvals would be expected to lag jumps in NTE
submissions by intervals of six and twelve months.
Are more NTE applications submitted in June and December? Figure 39 shows
the volume of NTE applications submitted by month from 1994 to 2003. For the period,
81 NTE applications were submitted in December, more than double the submissions of
any other month. June was the next most popular month with 38 NTE submissions,
although June submissions are much closer the overall average. It was also noted that
relative peaks in submission volume occur in March, June, September, and December,
which are the last months of each fiscal quarter. Biopharmaceutical management
objectives tied to quarter-end deadlines may promote the submission behavior exhibited
in Figure 39.
NTE SUBMISSIONS BY CALENDAR MONTH (1994-2003)
..........................--..--..................... ..--...
90 - . .... .............
0
8
...........
------... .
___.____
--
..
_____
__
_____
Co)70
_
C 60
X
z
50
40
E
36
...
0
m
r 20
z 10
!
20
38
_
.
--19
16
0
1
2
3
4
5
6
7
8
9
10
11
12
MONTH
Figure 39: Approved NTE submissions by calendar month, 1965-2003
Source: FDA
A X2 test was performed for NTE submission data. Testing against the uniform
distribution hypothesis yields a test statistic of 111.3, corresponding to a p-value of
1.02*10-18. Thus, we can again reject the null hypothesis of uniform distribution with
very high confidence. There is a statistically significant increase in NTE submissions in
December.
This analysis supports the submission hypothesis. The expected magnitude of this
effect can be conservatively estimated by multiplying the number of excess December
- 74 -
I----LIII-_·I_-i-·
-Y·_·-^·---i·
11-1 - 11--·--.111·^1___i-l.l
IUIIII---·1I
II *
·--------
I
-- -__1·_- 11·_1-·-
submissions (51) by the percentage of submitted applications approved in exactly twelve
months (12.4). The expected impact of these factors is conservatively estimated to be an
excess 6.3 NTE approvals in December compared to other months. Actual data for NTE
approvals in the post-PDUFA period is presented in Figure 40.
NTE APPROVALS BY CALENDAR MONTH (1994-2003)
-· --
- --- --------· ·--..---··---·-- ·-......I.....
n,
ou
- - - - - - - - - - - - - --- ------------
7,-
... ............
70
..
- -..... .- ...............
67
--.. .....
co 60
. 50
w
__ _ _ ._ _ ._
Z
0 40
LL
eq
--
30
a 30
w
I-
32
30
27
:
21
38
_--=
-
---
22
20
Z 20
z
10
0
C
I...-
_
1
2
3
v
,
4
5
6
7
8
9
10
11
12
MONTH
Figure 40: NTE approvals by calendar month, 1994-2003
Source: FDA
Figure 40 illustrates the December effect for NTE approvals from 1994 to 2003.
The mean number of approvals by month is 30.25. Adding the conservative estimate of
6.3 additional approvals from the submission hypothesis yields an estimated December
approval volume of approximately 37 NTEs. In actuality, the excess December approval
volume over the average is almost 37 NTEs - many more than the estimated 6.3.
If all excess December submissions (51) are assumed to be at PDUFA-mandated
six and twelve month lags and the historical proportion of standard applications to priority
applications (60:40) is assumed to hold, an excess of 31 approvals would be predicted for
December and 20 for June. Even in this aggressive case, the predicted excess does not
account for the full magnitude of the December effect. In addition, the submission
hypothesis predicts a secondary peak in NTE approvals in June - when priority
applications submitted in December are approved. However, June NTE approvals are
not elevated compared to other months.
- 75 -
The evidence presented here supports the hypothesis that the combined effects of
elevated December NTE application submissions and the established twelve month
PDFUA review target result in a significant increase in December NTE approvals.
However, the magnitude of the December effect exceeds the expected increase based on
the submission hypothesis alone. In addition, the submission hypothesis also predicts an
elevation in NTE approvals in June. Observed approval patterns are not consistent with
this prediction. Although the combination of industry submission schedules and PDUFA
review times partially explains the December effect, it do not account for all of it.
Additional contributing factors must also exist.
4.3
December effect was established prior to implementation of PDUFA
As discussed previously, the submission hypothesis imples constraints on review
times such that approvals follow submissions at a fixed interval. Since 1994, PDUFA has
provided constraints on review times in the form of review guidelines specifying six and
twelve month review targets for priority and standard applications, respectively. Prior to
1994, no such constraints existed. As evidenced by Figure 37, no specific length of review
predominated.
If the submission hypothesis were the only driver of the December effect, one
would expect to observe no December effect prior to the implementation of PDUFA in
1994. On the contrary, the December effect is observed well before 1994. In fact, the
December effect was greatest during the late 1980's, as shown by the monthly approval
volume plot in Appendix 3. The submission hypothesis cannot explain the strong
December effect in the pre-PDUFA period.
- 76-
1
NTE APPROVALS; PERCENTAGE BY CALENDAR MONTH
25.0%
1i 20.0%
Z 15.0%
It
; 10.0%
z
5.0%
0.0%
1
2
3
4
5
6
7
8
9
10
11
12
MONTH
Figure 41: NTE approval percentages by calendar month, 1965-2003
Source: FDA
Figure 41 compares the percentage of NTEs approved in each month for the
period from 1965 to 1993 with the monthly percentages for the period from 1994 to
2003. Surprisingly, the December effect is more pronounced in the period prior to the
implementation of PDUFA. 25.6 percent of all NTE approvals occurred in the month of
December in the period from 1965 to 1993, compared to 15.5 percent after 1994.
The causes for the December effect prior to the implementation of PDUFA
remain unresolved. One hypothesis is that FDA reviewers follow seasonal work patterns
organized around the fiscal year calendar. Workflow seasonality is common in many
organizations and is often the result of policies or procedures that favor specific workflow
timing. For example, enterprise software companies have notoriously "back-end loaded"
quarters, where it is common for over 50 percent of quarterly revenue to be booked in the
last weeks of the quarter. This effect is due to incentive structures in the enterprise
software industry, which reward sales representatives based on quarterly targets.
Customers have come to recognize the additional pressure on the sales representative near
the end of a quarter and often delay purchase decisions to that time in order to exploit
potential negotiating leverage over a representative in danger of missing her quarterly
goals.
Similarly, FDA reviewers may have implicit annual review quotas. FDA annual
reports sometimes include positive commentary touting the large number of new drugs
- 77 -
approved during a particular year. Pharmaceutical industry interest groups closely
monitor the performance of the FDA and may focus on the agency's annual report as the
basis for criticism. The FDA may have incentives to accelerate processing of nearly
complete applications in December in order to publish annual approval data that will be
well-received by industry. More research is needed to understand the incentives in place
for FDA reviewers. Certainly, PDUFA has placed specific constraints on review times.
However, other implicit or explicit incentives likely influence the review process. The
strong December effect prior to the implementation of PDUFA provides evidence for
seasonal workflow patterns that may be associated with incentives based on annual review
volume. Understanding these incentives may provide actionable insight into FDA
operations.
4.4
NDA submission practices have changed pursuant to PDUFA I
Section 4.3 discussed the unexpected finding that the December effect existed
prior to the implementation of PDUFA. This finding weakens the hypothesis that the
December effect is the result of industry submission practices coupled with PDUFA
review guidelines.
Figure 42 illustrates another unexpected result, namely that NTE application
submission patterns have changed significantly since the implementation of PDUFA.
Specifically, December submissions have increased dramatically. Prior to 1994, NTE
application submissions were relatively evenly distributed across all months. The most
popular month for submissions was March, followed by December. Although a
2
test
does reject the uniformity hypothesis at the 95 percent confidence level, if March is
excluded, the distribution of approval volumes over the remaining months (including
December) can be described by a uniform distribution. After 1994, the percentage of
December submissions increases significantly. For the period from 1994 through 2003,
22.3 percent of NTE applications were submitted in December, more than double the
average for other months. At 10.5 percent, June was the next most popular month for
NTE submissions.
- 78-
NTE SUBMISSIONS; PERCENTAGE BY CALENDAR MONTH
as: no/
LZ.U7o
20.0%
,
w
uI
z
15.0%
U.
0
- 10.0%
w
n
z
5.0%
0.0%
'1
2
3
4
5
6
7
8
9
10
11
12
MONTH
Figure 42: Approved NTE submissions by calendar month, 1965-2003
Source: FDA
The findings in Figures 41 and 42 provide evidence that basically reverses the
direction of causality in the submission hypothesis. The implementation of PDUFA, and
its associated review guidelines, did not significantly change the predilection for
December NTE approvals However, it did initiate a change in application submission
practices. The increase in December applications benefits the FDA because it enables the
agency to meet the targets specified by PDUFA I without altering existing calendar
workflow patterns. Why industry sponsors would alter submission patterns, however, is
not clear. It is possible that biopharmaceutical companies began to prefer December
approvals in the mid-1990's due to some exogenous reason. For example, perhaps equity
investors are more receptive to news in December. On the other hand, the increase in
December NDA submissions after PDUFA could be due to FDA reviewer behavior.
FDA reviewers may have managed to maintain their December workflow schedule by
encouraging industry sponsors to submit standard applications in December or by gating
receipt of applications to favor December submissions. Many other explanations are
possible. More research is needed to isolate the root causes for the observed December
effect in submissions and approvals.
- 79 -
PDUFA II review targets have attenuated the December effect for
4.5
NTE approvals
PDUFA II, passed with the Food and Drug Administration Modernization Act of
1997 (FDAMA), included provisions to reduce the review period target from twelve
months to ten months for standard NTE applications. Specific performance targets were
structured as follows: 30 percent of standard applications reviewed within 10 months in
FY1999, 50 percent in FY2000, 70 percent in FY2001, and 90 percent in FY2002 and
thereafter. In 2002, the FDA reported that it had achieved the ten month review target
for standard NTE applications in 81 percent of cases in 2001 and 95 percent of cases in
2002 (FDA, "Performance Report" 2003). According to this data, the FDA successfully
achieved the revised performance targets specified in PDUFA II.
In order to achieve the ten month review target, the December effect for
submissions, approvals (or both) should change. If the December effect in submissions
persists, an increase in October approvals would be expected. If the December effect in
approvals persists, application submissions in February would be expected to increase.
Data collected from 2001 (when PDUFA ten month targets were 81 percent
implemented) to 2003 indicate that the December effect in approvals is weakening, while
the December effect in application submissions remains robust.
NTE SUBMISSIONS BY CALENDAR MONTH (2001-2003)
JU
25
SC, 20
w
z
zL 15
0
w
m 10
z
5
0
1
2
3
4
5
6
7
MONTH
8
9
10
11
12
Figure 43: Approved NTE submissions by calendar month, 2001-2003
Source: FDA
- 80 -
_IIU
L 1_1__ Ip ^__··IIIIIIIIIII.
.__.____l-_.^·__·L-·
-IIII-L-C I·
..
._
_
_
As shown in Figure 43, for the 86 NTE applications approved between 2001 and
2003, 24 (27.9 percent) were submitted in the month of December. While the December
effect for submissions remained robust, the December effect for approvals weakened over
this period.
NTE APPROVALS BY CALENDAR MONTH (2001-2003)
MA
I
14
12
to
1i 10
w
6------
7-----~--8
8
8
z
0o 6
w
4
4
:
5
,:
-
-
::;i... ·
z
2
ji-,
,:
,
0
1
Figure 44:
2
3
4
5
6
7
MONTH
,
,
,
8
, , , , , .~~~~~~~~~~~:
9
10
11
12
NTE approvals by calendar month, 2001-2003
Source: FDA
Figure 44 shows that December is not the dominant month for NTE approvals for
the 2001-2003 period. May and November account for relatively more approvals
compared to other months, although the volume of NTE approvals is more evenly
distributed than in other periods analyzed above. Interestingly, October approvals, which
lag December submissions by ten months, show only modest signs of increase.
4.6
Implications of December effect on attainment of PDUFA III targets
In 2002, the user fee arrangement was authorized again as part of the Bioterrorism
Preparedness and Response Act of 2002 (PDUFA III) (FDA 2002). The provisions of
PDUFA III maintained the review goals specified in PDUFA II: a six month review target
for priority applications and a ten month review target for standard applications.
Although the FDA has successfully achieved PDUFA II targets thus far, the analysis
presented in this section suggests that the administration may experience some difficulty
in maintaining target performance in the future.
- 81 -
If industry sponsors continue to submit a large percentage of NTE applications in
December, the FDA will have to alter its workflow seasonality to maintain attainment of
PDUFA III targets. Specifically, the administration would be expected to experience
increases in activity in June and October as the six and ten month review deadlines for
NTE applications submitted in December come due. Despite the FDA's initial success in
achieving PDFUA II targets, implicit incentives and human nature may continue to favor
increased seasonal activity at the end of the fiscal year. Without strong leadership and a
consistent plan to insure that reviewer behaviors are consistent with PDUFA goals, the
continued attainment of PDUFA III goals may be difficult.
Finally, industry NTE application sponsors should remain cognizant of seasonal
patterns in FDA workflow. A submission strategy that takes FDA activity patterns into
account may have a greater chance of smooth and efficient approval than one that ignores
these considerations. Most sponsors push to submit NTE applications as soon as possible
in order to gain marketing approval as quickly as possible. This allows the sponsor to
begin to sell and generate revenue from the approved drug. The benefits of additional
revenue generation are usually quite significant and likely outweigh any possible benefits
provided by a more strategic submission date. However, in cases where flexibility exists,
industry sponsors should target NTE application submission dates that take advantage of
historical FDA activity patterns. For standard applications, a February submission date
allows FDA reviewers to satisfy the ten month PDUFA III review target while
maintaining a traditional December-oriented workflow schedule. Likewise, priority
applications submitted in June are consistent with December approval.
Industry sponsors should carefully consider the risks and benefits of continuing to
concentrate NTE application submissions in December. While this practice dovetailed
well with PDUFA I targets, it may be counter-productive under the targets specified by
PDUFA III. December submission of a standard application carries two potential
drawbacks: first, December submission favors additional FDA review activity in October
instead of December and second, applications submitted in December must compete with
a large number of other December submissions for FDA resources. Therefore, industry
sponsors may consider increasing scheduled submissions for calendar months other than
December.
- 82 -
__IIIILIIII__I__I______
_______1___1________·____
5.
Discussion and conclusions
5.1
Summary of findings
In this thesis, I have used a variety of time-series analyses to provide insights into
recent trends in biopharmaceutical productivity. This analysis has focused on the last
stage of the drug development process, NDA approval. In particular, I have considered
the impact of the Prescription Drug User Fee Act (PDUFA) and its subsequent
amendments. Previous studies have focused on the impact of PDUFA on review times
for drug applications (Kaitin 2002). Review times are particularly relevant to
biopharmaceutical companies because reducing time to market results in increased
present value of drug programs. Faster approval of drugs which address serious unmet
medical needs also benefit patients for whom no other treatment options are available
(Gottschalk 2004.) In contrast, this thesis focuses on recent trends in the overall output
of innovative drugs. Over the long term, trends in biopharmaceutical productivity are
more relevant to the success of the industry and health of patients.
Section 2 of this thesis examines the behavior of NTE approval time series in
order to gain insight into the underlying patterns and trends affecting drug approvals. As
many industry observers have noted, output of new drugs has been declining in recent
years (DeLamarter 2003). I have documented that NTE approvals shifted from a pattern
of linear growth at an annual rate of .48 NTEs per year from 1965 to 1995, to a linear
decline of 3.04 NTEs per year from 1996 to 2003. Notably, these trends are demarcated
by a large increase in NTE approvals in 1996. This increase is not predicted by a either
linear model of NTE approvals or an ARIMA (2,1,1,) model constructed with data
collected from 1965 to 1995. A simple description of the observed trends in NTE
approvals would be: steady growth from 1965-1995, a large jump in 1996, and a steady
decline thereafter.
What is driving this behavior? Why was there a large jump in NTE approvals in
1996? One commonly suggested explanation states that implementation of PDUFA in
1994 led to increased approvals in 1996, based on additional FDA review resources
provided by the Act. Section 3 examines the validity of this hypothesis. The number of
NDA approvals in a particular year can be expressed as the product of the number of
applications reviewed and the success ratio of reviewed applications. If the increased
- 83 -
review capacity provided by PDFUA caused the jump in approvals in 1996, we would
expect the number of applications reviewed to increase. Based on the provisions of
PDUFA alone, the success ratio would not be expected to change. On the contrary, the
data suggests that only one-third of the observed increase in 1996 NTE approvals can be
explained by increased FDA capacity. Over two-thirds of the increase is explained by an
increase in the success ratio.
In reports to Congress, FDA Commissioners Jane Henney and Mark McClellan
cited an increase in NME approval rates after the implementation of PDUFA. According
to FDA reckoning, approval rates for NMEs rose from 66 percent prior to PDUFA to 80
percent afterwards (FDA, "Performance Report" 2001, 2003). These observations are
consistent with the analysis presented in Section 3, which documented a rise in the NDA
success ratio from 62 percent for 1985-1993 to 72 percent for 1994-2003.
The withdrawal of rofecoxib (Vioxx) by Merck following the issuance of an FDA
Public Health Advisory in September 2004 has increased public scrutiny of FDA approval
policies. Some have suggested that safety and efficacy standards have been lowered,
thereby leading to an increase in the number of dangerous drugs in the U.S. market
(Wolfe, 2002). At first glance, the increase in the success ratio documented in Section 3
is consistent with this criticism of FDA approval practices.
Does an increase in the success ratio lead to riskier approved drugs? Marketing
withdrawals are one measure erroneous approvals, though, in actuality, withdrawals may
result from a number of factors, including failure to prescribe and use the drug according
to FDA-approved labeling. If relaxation of FDA approval standards has led to more
dangerous drugs on the market, observed withdrawal rates would be expected to increase.
For NDAs approved before 2001, the percentage of approved NDAs eventually
withdrawn has not changed significantly from the period before the implementation of
PDUFA (2.7 percent) to the period after PDUFA (2.6 percent.) In addition, my analysis
did not find significant evidence that increased success rates correlate with higher rates of
withdrawal. Although the FDA is approving a larger proportion of NDA filings postPDUFA, increases in withdrawals have not followed. This analysis does not support the
argument that changes in FDA policy related to PDUFA have increased public health
risks.
- 84 -
_
_·_11___1_·
Finally, Section 4 examines seasonality in NTE approvals. FDA/BEP data show
that approvals increase in December. This observation holds true both before and after
the implementation of PDUFA, suggesting that the December effect is not the result of
PDUFA review targets. Interestingly, industry submission practices have changed since
the implementation of PDUFA. For reasons that remain unclear, industry has
increasingly submitted NTE applications in December since the implementation of
PDUFA in 1994.
Ten month review targets for standard NTE applications were adopted under
PDUFA II and reaffirmed in PDUFA III. This new review timeline has eroded the
December effect in approvals. My analysis suggests that if industry sponsors continue to
favor December submission of NTE applications, FDA reviewers will experience a peak
in review activity in June (for six month reviews) and October (for ten month reviews.)
An activity peak in October may conflict with traditional seasonal workflow patterns in
place at the FDA. I predict that traditional workflow patterns will present an important
challenge to the long-term achievement of PDUFA II and PDUFA III review goals. In
addition this analysis suggests that standard NTE applications submitted in February,
which have review schedules consistent with PDFUA targets and historical FDA workflow
patterns, should be processed more efficiently by FDA reviewers. Finally,
biopharmaceutical sponsors should consider FDA workflow patterns when developing
NDA submission strategies.
5.2
Future biopharmaceutical industry productivity
This thesis was initially focused on the recent declines in annual NTE approvals.
Research on this topic began in 2003, after declines in new drugs approvals had been
recorded in five of the previous six years. Subsequently NTE approvals showed a
rebound in 2003.
Analysis presented in this thesis suggests that future NTE approval rates will
return to historical trends. Analysis of the NTE approval time series revealed a pattern of
steady growth combined with periodic oscillations in NTE approval volume from 1965 to
1995. This pattern was broken in 1996 by a large jump in NTE approvals. Since 1996,
yearly NTE approvals have fallen without the periodicity observed prior to 1996. These
observations led to the hypothesis that the recent decline is the result of (1) a temporary
positive shock in NTE approvals in 1996 followed by (2) a prolonged period of declining
- 85 -
approvals as the system regained equilibrium. This hypothesis is consistent with the
observation that the NTE time series is mean reverting according to the Dickey-Fuller
test. This hypothesis suggests that NTE productivity will eventually return to the growth
rate (approximately equal to +.48 NTEs per year) seen prior to 1996.
However, one piece of evidence contradicts this hypothesis. The calculated net
outflow of NDA filings under review has significantly reduced the number of NDA filings
in the FDA approval process. As shown in Figure 29, the number of NDA filings leaving
the review process (via approval, rejection, voluntary withdrawal, or issuance of
approvable letters) has exceeded the number of NDA submissions in thirteen out of the
eighteen years from 1985 to 2003. This observation could be the positive result of faster
FDA response times. On the other hand, it could indicate a decline in the number of new
NDA submissions. Will the biopharmaceutical industry be able to consistently provide
quality new drug applications to fill the NDA pipeline? More research into trends
upstream in the drug development process will be needed to answer this question.
5.3
Better access to NTE filing and approval data is needed
A major barrier to conducting research on biopharmaceutical productivity is the
lack of public data on unapproved new drug applications. Detailed analysis of NTE
submissions is impossible because the necessary data is not publicly available. Data that
does exist is often proprietary and expensive to procure. In addition, available data is
often presented in aggregate, without detailed explanation of the methodologies used to
compile and analyze the data.
These data are not publicly available for several reasons. First, sponsor companies
claim that information about unapproved applications is confidential and sensitive.
Therefore, neither biopharmaceutical companies or the FDA shares this data. Second,
even if drug companies waived confidentiality for unapproved applications, the FDA does
not possess the resources needed to collect, process and provide data to the public in a
useful format. Data collection and analysis is not directly related to processing NDA
filings, and is generally considered a non-critical function at the FDA (Hass 2004)
The interests of biopharmaceutical companies in keeping this data confidential are
outweighed by the public interest in understanding the dynamics of the drug approval
- 86 -
_
I·lllllIIIIIIIL
·· -_.___1_1_-
_·
__
process. Data regarding NDA submissions could be particularly helpful in analyzing the
success or failure of the drug industry in providing truly innovative therapies.
Considering the vast public investment in drug research provided through NIH, NCI and
other public organizations, the public has a legitimate claim on general information about
drug applications, both approved and unapproved. Specific sensitive information about
the chemical composition or key clinical characteristics of drugs could be kept
confidential. However, general data regarding the submission and dispensation of NDA
filings should be available to the general public. Government officials should work with
industry to expand the breadth of drug development information available to the pubic
while protecting the competitive interests of biopharmaceutical companies.
5.4
Towards a systems analysis of the drug development process
Observed trends and cyclicality in NTE approvals prior to 1996 are suggestive
systems-level processes. The drug development process is a massive system of interrelated flows of intellectual capital, financial capital and development expertise through
various stages of the research, development, and approval process.
Systems dynamics tools have proven extremely useful in disentangling complex
processes and characterizing important influences on the system (Sterman 2000). These
tools could be very useful for identifying bottlenecks and isolating non-obvious
relationships between different aspects of the drug development and approval process.
Understanding the nature dynamic relationships in the drug approval process may allow
the drug industry and regulatory authorities to work together to produce beneficial drugs
more efficiently.
However, constructing a detailed systems dynamics model of the biopharmaceutical industry would require massive amounts of data, much of which is now
unavailable publicly. A systems approach will require cooperation between regulatory
authorities, drug companies and drug development researchers. Although developing a
framework for increased disclosure will require a great deal of work by all stakeholders,
the benefits could be significant. The resulting model would be a powerful tool for
understanding and improving the drug development process.
- 87 -
The analysis set forth in this thesis provides a first step towards developing such a
model. Further data-driven analysis of components of the drug development process
could generate ideas for significant improvements in the drug development cycle. The
small costs of publicly disclosing additional drug development process data would pale in
comparison to the benefits resulting from even small process improvements that bring
larger numbers of life-saving biopharmaceutical innovations to the market faster.
- 88 -
L
III
__1
·__
__
Bibliography
AHLA, "New York AG Spitzer Addresses AHLA's Annual Meeting." News Release, June 29, 2004.
Booth B. and Zemmel R. "The search for blockbuster drugs: Efficacy isn't everything." The McKinsey
Quarterly 4 (2004).
Biomedical Enterprise Program. "Approval data." FDA-BEP database, 2004.
Cohen, F. "Macro Trends in Pharmaceutical Innovation." Crownstone Group. 2004.
CMR International. Pharmaceutical Investment and Output. Proc. of CMR International. London, 2002.
Surrey: CMR, 2002.
Danzon, P., A. Epstein, S. Nicholson. Mergers and Acquisitions in the Pharmaceutical and Biotech
Industries. NBER Working Paper No. W10536. June 2004.
Delamarter, J. "Biotechnology partnerships: medicine for an ailing industry." Nature Biotechnologv 8
August 2003.
Dell Computer, Inc. "Inspiron product information." December 2004. <http://configure.us.dell.com>.
DiMasi, J. Personal interview. November 2004.
DiMasi, J. "A New Look at United States Drug Development and Approval Times." American ournal of
Therapeutics 3 (1996): 1-11.
DiMasi, J. "Risks, regulation, and rewards in new drug development in the United States." Regulatory
Toxicology and Pharmacology 19.2 (1994): 228-35.
DiMasi, J., R. Hansen, H. Grabowski. "The price of innovation: new estimates of drug development costs."
Tournal of Health Economics (2003).
DiMasi, J., et al. "Cost of Innovation in the Pharmaceutical Industry." Tournal of Health Economics 10
(1991): 107-142.
Douglas, F. Personal interview. November 2004.
Edmunds, R., P. Ma, C. Tanio. "Splicing a cost squeeze into the genomics revolution." The McKinsev
Quarterl 2 (2001): 15-9.
Ernst & Young. Resilience: Americas Biotechnology Report 2003. Washington, D.C.: Ernst & Young, 2003.
FDA. New Drug Evaluation Guidance Document. Washington, D.C.: FDA, July 12, 1993.
FDA. Electronic Orange Book. November 2004. <http://www.fda.gov/cder/ob/default.htm>.
FDA. FY2000 Performance Report to Congress for the Prescription User Fee Act of 1992 as Reauthorized
and Amended by the Food and Drug Administration Modernization Act of 1997. Washington, DC: GPO,
2001.
FDA. FY2002 Performance Report to Congress for the Prescription User Fee Act of 1992 as Reauthorized
and Amended by the Food and Drug Administration Modernization Act of 1997. Washington, DC: GPO,
2003.
FDA. FY2003 Performance Report to Congress for the Prescription User Fee Act of 1992 as Reauthorized
and Amended by the Food and Drug Administration Modernization Act of 1997. Washington, DC: GPO,
2004.
- 89 -
FDA. "Priority Review Policy." Manual of Policies and Procedures, Research. 6020.3. Rockville, MD: FDA,
1996.
FDA. "Report to the Nation: Improving Health through Human Drugs." Rockville, MD: FDA, 2001.
FDA. "Report to the Nation: 2003." Rockville, MD: FDA, 2004.
FDA. "Transfer of Therapeutic Products to the Center for Drug Evaluation and Research." U.S. Food and
Drug Administration Online 7 Sept 2004. Jan 2005. <http://www.fda.gov/cber/transfer/transfer.htm>
FDA. "PDUFA Reauthorization, Performance Goals and Procedures." U.S. Food and Drug Administration
Online November 2004. December 2004. <http://www.fda.gov/oc/pdufa/PDUFAIIIGoals.html>
FDA Review (A project of the Independent Institute). "History of Federal Regulation: 1902-Present." The
Independent Institute. Oakland, CA. 2004.
"Fortune 500 industry report." Fortune Magazine 149.7 (2004): F26.
Gosse, M., et al. "Effects of US regulatory policies on the research, development, and approval of new
biotechnology derived biopharmaceuticals: points to consider for OECD member countries." Biotechnolog
medical innovation and the economy: a survey. Paris: OECD, 1998.
Gottschalk, A. "Improving the Efficiency of the Later Stages of the Drug Development Process: Survey
Results from the Industry, Academia, and the FDA." Diss., M.I.T., 2004.
Grabowski H. and Vernon J. Prospects for returns to pharmaceutical R&D under health care reform in ed.
Robert Helms. Competitive Strategies in the Pharmaceutical Industry. Washington, D.C. AEI Press. 1996.
Grabowski, H., J. Vernon, J. DiMasi. "Returns on R&D for 1990s new drug introductions".
PharmacoEconomics 20 (2002): 11-29.
Grabowski, H. "Patents and new product development in the pharmaceutical and biotechnology industries."
Georgetown Public Policy Review 8 (2003): 87-104.
Harris Interactive. "Survey on Prescription Drug Prices, Hospital Costs and Doctors' Fees." PRNewswire.
Sept. 20, 2004.
Harvey, A. Time Series Models, 2nd edition. Cambridge, MA: MIT Press, 1993.
Hass, Ed. Personal Interview. 18 October 2004.
Hays, C.L. "Martha Stewart's Sentence: The Overview." New York Times 17 July 2004.
Hilts, Philip J. Protecting America's health: the FDA. business, and one hundred years of regulation. New
York: Alfred A. Knopf, 2003.
IMS Health. "Patent Focus." IMS Health International database. London: IMS Health, 2004.
Jensen, E. "Research expenditures, regulation, and innovation in the ethical pharmaceutical industry." Diss.
M.I.T., 1984.
Kaitin K., ed. "Approval times for new drugs fell by more than a year during PDUFA." Tufts Center for the
Study of Drug Development Impact Report 2002 4 (Nov/Dec 2002): 6.
Koopmans, L.H. The Spectral Analysis of Time Series. New York: Academic Press, 1974.
Kuhn, Thomas. The Structure of Scientific Revolutions, 3rd Edition. Chicago: University of Chicago Press,
1996.
Malkiel, Burton. A Random Walk Down Wall Street: The Best Investment Advice for the New Century.
New York: W.W. Norton &Co., 1999.
- 90 -
_______
_1_1__11_______1_____1_1
Mason, T. R&D Productivity: How Should it be Measured? A Perspective Based on Fundamental
Principles. Proc. of DIA Annual Meeting. Eli Lilly & Company. 15 June 2004.
McKinnon, James G. "Numerical Distribution Functions for Unit Root and Cointegration Tests." Tournal of
Applied Econometrics 11 (1996):601-618.
Meadows, M. "Why Drugs Get Pulled Off the Market." FDA Consumer magazine Jan.-Feb. 2002.
Medco. "Drug Trend Report: Navigating the New Health Economy." Drug Trend 6:1 (May 2004)
Moore, D., A. Baum. "Cycles in R&D Productivity: Apologies to Thomas Kuhn." Morgan Stanley Equity
Research. 30 June 2004.
"The MT Interview: JP Gamier, CEO of GlaxoSmithKline." Management Today 1 March 2004.
Nelson, C. and Plosser, C. "Trends and random walks in macro-economic time series: some evidence and
implications." Tournal of Monetary Economics, 10 (1982): 139-162.
Olson, Mary K. "Pharmaceutical Regulation." The New Palgrave Dictionary of Economics and the Law. Ed.
Peter Newman. New York: Stockton Press, 1998. 40-45.
Mathieu, M.P., ed. Parexel's R&D Statistical Sourcebook 2004/2005. Waltham, MA: Parexel International
Corporation, 2004.
Pharmaceutical Research and Manufacturers of America (PhRMA). Delivering on the Promise of
Pharmaceutical Innovation: The Need to Maintain Strong and Predictable Intellectual Property Rights.
Washington, DC: PhRMA, 2002.
Pharmaceutical Research and Manufacturers of America (PhRMA). Pharmaceutical Industry Profile 2004.
Washington, DC: PhRMA, 2004.
Pindyk, R. and D.Rubinfeld. Econometric Models and Economics Forecasts. 4th ed. Boston: Irwin
McGraw-Hill, 1997.
Porter, E. "Why Do Drugs Always Have to Cost So Much?" New York Times 14 November 2004: 3:5.
Porter, M. Strategic Issues for Biotechnology Companies. Proc. of Bio 2000 Economic Forum. March 27,
2000.
Primedia. "About.com Economics." About.com Online. January 2005. 13 January 2005.
<http://economics.about.com/cs/economicsglossary/g/akaikes.htm>
Public Citizen. America's Other Drug Problem: A Briefing Book on the Rx Drug Debate. Washington,
D.C.: Public Citizen, 2002.
Romer, P., "The Origins of Endogenous Growth." The Tournal of Economic Perspectives. 8.1 (1994): 3-22.
Scherer F.M. "The link between gross profitability and pharmaceutical R&D spending. An analysis that
answers the question: What does the pharmaceutical industry really do with its profits?" Health Affairs 20
(2001) 216-220.
SigView 9.1. Computer Software. SigView, Inc. 2004.
Sterman, J. Business Dynamics - Systems Thinking and Modeling for a Complex World. Boston: Irwin,
McGraw-Hill, 2000.
Sylvester, C.J., et al. "Is R&D Productivity Improving?" UBS Global Equity Research, March 10, 2004.
Trombetta, W. "Industry Audit: Running the Numbers on Pharma's Top Performers." Pharmaceutical
Executive September 2004.
- 91 -
Tufts CSDD. "Biotechnology Has Become Vital to Orphan Drug R&D, According to the Tufts Center for
the Study of Drug Development." News Release, March 22, 2002.
Tufts CSDD. "Database Snapshot - End-of-the-Year Surge in Approvals." Tufts CSDD Impact Reoort
23:1 (February 1998): 8.
Tufts CSDD. "Gloassary of terms." Tufts CSDD Online 7 January 2005. 13 January 2005.
<http://csdd.tufts.edu/InfoServices/Glossary.asp>.
Tufts CSDD. Outlook 2004 Report. Boston: Tufts CSDD, 2004.
U.S. Congress. Orphan Drug Act of 1983 (P.L. 97-414). Washington, D.C.: GPO, 1983.
U.S. Congress, Congressional Budget Office. How increased competition from generic drugs has affected
prices and returns in the pharmaceutical industry. Washington D.C.: GPO, 1998.
U.S. Congress, Office of Technology Assessment. Patent term extension and the pharmaceutical industry.
Washington, DC: GPO, 1981.
U.S. Congress, Office of Technology Assessment. Pharmaceutical R&D: Costs. risks and rewards. OTA-H522. Washington, DC: GPO, 1993.
U.S. Congress, Office of Technology Assessment. Innovation and commercialization of emerging technology.
OTA-BP-ITC-165. Washington, DC: GPO, 1995.
U.S. Congress, Senate Committee on the Judiciary. Administered prices: Drugs: Report of the Committee on
the udiciarv, United States Senate, made by its Subcommittee on Antitrust and Monopoly. pursuant to S.
Res. 52. viii, 374 p.; 23 cm. Washington, D.C.: GPO, 1961.
Riley, T., J. DeRuiter. "New Drug Review." U.S. Pharmacist Online March 2004. January 2005.
<http://www.uspharmacist.com/index.asp?page=ce/3069/default.htm>
Warner, Rebecca. Spectral Analysis of Time-Series Data. Cambridge, MA.: MIT Press, 1998.
Whiting, R. "Drugmakers Respond To Calls For Public Database Of Trials." Information Week. 25 June
2004.
Wiggins, S., "Product quality and regulation and new drug introductions: some new evidence from the
1970s." The Review of Economics and Statistics 63.4 (1981): 615-619.
Wolfe, S., et al. "Recent Events Arguing Against Things Getting Better as Suggested by the FDA."
May, 2002.
- 92 -
_
__·
_I
_·_·I^
· _I_
I
AMA 1
Appendix 1: Augmented Dickey-Fuller test
An Augmented Dickey-Fuller (ADF) test is a test for a unit root in a time series sample.
An ADF test is a version of the Dickey-Fuller test for a larger and more complicated set of
time series models.
The Dickey-Fuller tests for random walk behavior by comparing regression results from
two regression equations, an unrestricted equation and a restricted one.
Form of time series equation:
Y, = a +/t + pY,_, + Et
Unrestricted regression:
Y - Y-i = a + t
(-
)Yt_
Restricted regression:
Yt -Yt,-
= a
The augmented Dickey Fuller equation includes terms for autocorrelation with preceding
terms.
Form of time series equation:
P
Yt = a + fit + PYt,
+
E ijAy,-j
+
t
j=1
Unrestricted regression:
p
Yt -
=a+ t+(p- )Yt, +
j=l
Restricted regression:
aY -y
= (aY+
jAYt-j
j=1
- 93 -
jAYt-j
+
Et
An Augmented Dickey Fuller test was performed on time series data for NTE approvals
from 1965-1995 using the technique described by Pindyck and Rubinfeld (1997).
Regression results for ADF with two lag terms are summarized below.
Unrestricted regression
Coefficients Standard Error
a
13.97
3.92
0.19
0.67
13
(p-1)
-1.36
0.36
0.27
A1
0.33
A2
0.01
0.19
I residuals 2
Restricted regression
Coefficients Standard Error P-value
a
0.66
0.85
0.441
A1
-0.52
0.17
0.005
A2
-0.48
0.17
0.010
P-value
0.0015
0.0013
0.0008
0.2271
0.9483
E residuals 2
366.3
580.6
The summed squared residuals of the restricted and unrestricted regressions are used to
calculate the Dickey Fuller F-statistic according to the following equation:
F
(N - k)(ESSR - ESSUR )
q(ESSR )
Where N = number of observations, k = number of parameters in unrestricted regression
and q = number of parameter restrictions.
Using N=30, k=5, q=2, ESSUR=366.3, and ESSR=580.6, an ADF F-statistic of 7.315
was calculated. Referring to the Dickey-Fuller table excerpt below (Dickey and Fuller,
1981), an ADF F-statistic of 7.315 corresponds to a rejection of the random walk
hypothesis at the 95 percent confidence level.
Probability of a smaller value
Sample
size (N)
25
50
100
250
500
Xo
95%
7.24
6.73
6.49
6.34
6.30
6.25
90%
5.91
5.61
5.47
5.39
5.36
5.34
- 94 -
98%
8.65
7.81
7.44
7.25
7.20
7.16
The ADF test was repeated using the E-views software analysis package. The E-views
ADF analysis engine uses updates F-statistic tables described by McKinnon (1996). The
result of this analysis was rejection of the null hypothesis (random walk) at the 99 percent
confidence level.
Augmented Dickey Fuller test (from E-Views Analysis):
We can reject the null hypothesis of a unit root at the 99% level.
Null Hypothesis: TOTAL has a unit root
Exogenous: Constant, Linear Trend
Lag Length: 2 (Automatic based on SIC, MAXLAG=7)
Augmented Dickey-Fuller test statistic
Test critical values:
1% level
5% level
10% level
t-Statistic
Prob.*
-5.234730
-4.323979
-3.580623
-3.225334
0.0012
*MacKinnon (1996) one-sided p-values.
Augmented Dickey-Fuller Test Equation
Dependent Variable: D(TOTAL)
Method: Least Squares
Date: 11/12/04 Time: 13:52
Sample (adjusted): 1968 1995
Included observations: 28 after adjustments
Variable
Coefficient
Std. Error
t-Statistic
Prob.
TOTAL(-1)
D(TOTAL(-1))
D(TOTAL(-2))
-1.866188
0.654440
0.200325
0.356501
0.257033
0.181323
-5.234730
2.546131
1.104799
0.0000
0.0181
0.2807
C
16.69968
3.559072
4.692146
0.0001
@TREND(1965)
1.022306
0.200559
5.097290
0.0000
R-squared
Adjusted R-squared
S.E. of regression
Sum squared resid
Log likelihood
Durbin-Watson stat
0.693227
0.639876
3.359363
259.5624
-70.90538
2.100601
Mean dependent var
S.D. dependent var
Akaike info criterion
Schwarz criterion
F-statistic
Prob(F-statistic)
- 95 -
0.321429
5.597973
5.421813
5.659706
12.99353
0.000011
Appendix 2: ARIMA specification
A forecast model was specified based on historical levels of NTE approvals. This process
was modeled as an ARIMA (2,1,1) process.
Sample: 1965 1995
Included observations: 30
Autocorrelation
*** l|
*.
I**.
.*1 .
*.
*| .
*~ .
*
*
.
.
,* .
*1|
.
Partial Correlation
***IE1
** .*
.**i|
.
.
|
.
.
I
.
.
*
.
. *1| .
* 1* . .
.
. *i
.
.**
.
. *
*. .
.
. *1|
.
I
.
.
.
*1
AC
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
-0.321
-0.305
0.099
0.202
-0.125
-0.155
0.092
0.082
-0.129
-0.092
0.191
0.044
-0.109
0.033
0.000
0.000
PAC
Q-Stat
Prob
-0.321
-0.455
-0.267
-0.004
-0.048
-0.159
-0.137
-0.099
-0.179
-0.281
-0.143
-0.083
-0.058
0.023
-0.113
-0.135
3.4121
6.6019
6.9501
8.4528
9.0545
10.014
10.366
10.660
11.426
11.829
13.675
13.778
14.454
14.521
14.521
14.521
0.065
0.037
0.074
0.076
0.107
0.124
0.169
0.222
0.248
0.297
0.251
0.315
0.343
0.412
0.486
0.560
ARIMA Specification:
Estimation Equation:
D(TOTAL) = C(1) + [AR(1)=C(2),AR(2)=C(3),MA(1)=C(4)]
Substituted Coefficients:
D(TOTAL) = 0.5399082359 + [AR(1)=-0.09873513192,AR(2)=-0.4346657648,MA(1 )=0.9904559665]
- 96 -
^x
·.--_-_
I^1.·1^
-mr-u---
__-.-_..
.r- .----- r
---r
I_-
Sample (adjusted): 1968 1995
Included observations: 28 after adjustments
Convergence achieved after 14 iterations
Backcast: 1964
Variable
Coefficient
Std. Error
t-Statistic
Prob.
C
AR(2)
AR(1)
MA(1)
0.539908
-0.434666
-0.098735
-0.990456
0.050426
0.175305
0.175370
0.042603
10.70691
-2.479476
-0.563009
-23.24859
0.0000
0.0206
0.5787
0.0000
R-squared
Adjusted R-squared
S.E. of regression
Sum squared resid
Log likelihood
Durbin-Watson stat
0.670774
0.629621
3.406857
278.5603
-71.89430
2.333775
Mean dependent var
S.D. dependent var
Akaike info criterion
Schwarz criterion
F-statistic
Prob(F-statistic)
Inverted AR Roots
Inverted MA Roots
-.05-.66i
.99
-.05+.66i
Inverse Roots of AR/MA Polynomial(s)
Specification: D(TOTAL) C AR(2) AR(1) MA(1)
Sample: 1965 1995
Included observations: 28
AR Root(s)
Modulus
Cycle
-0.049368 + 0.657441i
0.659292
3.817834
No root lies outside the unit circle.
ARMA model is stationary.
MA Root(s)
0.990456
Modulus
Cycle
0.990456
No root lies outside the unit circle.
ARMA model is invertible.
- 97 -
0.321429
5.597973
5.421021
5.611336
16.29944
0.000005
Appendix 3: Monthly NTE approvals, 1965-2003
oR
a
0
a)
88
C)D
88
X
0
6
O
8
8
co
V
D
CI
O
_
CN
d
cO
8 88
8
0
0)
0
D
N
10
M
6
8
N
6
o
-
0
1<
I)
a
0
0
o
'I
I
0
(U
0
a)
o
a)
N
0
N
0
a
I
0
m
c"
04
T
I
r
0
a.
a)
-c
e0
a)N0
_
c~
0a)
o
a
B
0
'O1 0r
CL
a
OY
0
r.00)
CD
a)
0
o
co
T
I
0
ID
0
0
tD
-
o
o
D
OT
I
'7
in
ie
~o
CD
a)
t'
N
to
U)
t
·
Nu
-
Aouenboij
___
IULI
Ikuenb
ro
C
__________
__________
I-.L--X·IIIICII.I*--I----II1 --L-I·L_·_I--I-·I__1_11_
._
o
0
AouenbeJd
98 _._ __ .
_ .
_ ._ _
_
_ __
_
... ..- .---.-_
cO o 9o
o
o
oo
oo
9oo
oo
o
oo
0 eeo
0
oo
a)
W
0
0
0
0
0
0
0
0
r-
U
U)
U-
V)
N
-
0
o
o
N
a,
O2
O
I
m
O
aw
O
O
o
o
o1
0Nu
o
C,
0
O0
o
a,
C5
T.=
o
I
0)
Tm
0
a
as
T
rI
OI
e
o
O,
O
_
m
.2
tL
ol
ab
I)
m
a:
O,
.0
a,
I
ao
a2
O
.0
a,
a,
co
o
0
10
0)
aI
aw
co
o,O
m
0
ao
o.
U)
U)
Vt
N'U
C)
10)
'IT
'
o
o0
NO
0
Aouenbaj
Aouenbij
- 99 -
-
("uenbe 0
!
i
i
Appendix 4: NDA Flowchart
Process map for NDA approval:
Revieew b y CDER
I
Medical
I
I
Biophannaceutical
l
.~~r
-I
Pharmacology
ar
F
Statistical
N
.
i
Chemistry
. ,
Adviso ry
Committee
_
.
-I
I-
A1816~
Microb ilo gy
*
_
|
.
pr
(1) Labeling in this context means
officalinstrutions for use
areperrmrmea
- 100 -
·----
---------
-·
--
--
Sacin
.... ....
.. .. . ... ... .. I
IV
sncan c malltrs
_
-------- ·-·-------------
I·-
-- ····-- --------- ·---------·
·-·---
-
-------------
Meetings with
X6
n
-ent
_as~nmas
I1