DTD 5
Gait & Posture xxx (2005) xxx–xxx
www.elsevier.com/locate/gaitpost
Effect of skin movement artifact on knee kinematics during gait
and cutting motions measured in vivo
Daniel L. Benoit a,b,c,*, Dan K. Ramsey d, Mario Lamontagne f,g, Lanyi Xu f,
Per Wretenberg b,e, Per Renström a,b
a
Institution for Surgical Sciences, Section of Sports Medicine, Karolinska Institute, Stockholm, Sweden
b
Department of Orthopaedics, Karolinska Hospital, Stockholm, Sweden
c
Department of Mechanical Engineering, University of Delaware, 106 Spencer Lab, Newark, DE 19711, USA
d
Department of Physical Therapy, University of Delaware, Newark, DE, USA
e
Institution for Surgical Sciences, Section of Orthopaedics, Karolinska Institute, Stockholm, Sweden
f
School of Human Kinetics, University of Ottawa, Ottawa, Canada
g
Department of Mechanical Engineering, University of Ottawa, Ottawa, Canada
Received 6 November 2004; received in revised form 25 March 2005; accepted 9 April 2005
Abstract
Eight healthy male subjects had intra-cortical bone-pins inserted into the proximal tibia and distal femur. Three reflective markers were
attached to each bone-pin and four reflective markers were mounted on the skin of the tibia and thigh, respectively. Roentgenstereophotogrammetric analysis (RSA) was used to determine the anatomical reference frame of the tibia and femur. Knee joint motion
was recorded during walking and cutting using infrared cameras sampling at 120 Hz. The kinematics derived from the bone-pin markers were
compared with that of the skin-markers. Average rotational errors of up to 4.48 and 13.18 and translational errors of up to 13.0 and 16.1 mm
were noted for the walk and cut, respectively. Although skin-marker derived kinematics could provide repeatable results this was not
representative of the motion of the underlying bones. A standard error of measurement is proposed for the reporting of 3D knee joint
kinematics.
# 2005 Elsevier B.V. All rights reserved.
Keywords: Soft tissue artifacts; Movement analysis; In vivo; Three-dimensional analysis; Knee joint
1. Introduction
One of the most common methods to measure knee joint
motion is to track the motion of clusters of three or more
retro-reflective or light emitting markers affixed to the skin
of the shank and thigh. The marker configurations used may
influence the accuracy of the reconstructed data [1].
However, other factors may play a more significant role
in determining the validity of the results. When applied to
measuring knee joint kinematics based on the position of the
tibia and femur, the accuracy of these measurements is prone
* Corresponding author at: Department of Mechanical Engineering,
University of Delaware, Spencer Labs 126, Newark, DE 19716, USA.
Tel.: +1 302 831 2410/2423; fax: +1 302 831 3466/3619.
E-mail address: dbenoit@magma.ca (D.L. Benoit).
to error due to skin movement artifact [2]. A recent review
by Leardini et al. [3] identifies that previous investigations
have been lacking in sample size [4], or have had
methodological limitations [5,6]. While only three and
two subjects were evaluated in these studies, respectively,
the lack of agreement between the shape of the kinematic
profiles derived from the skin- and pin-markers poses an
important question as to how well skin-marker kinematic
profiles represent the underlying bones.
Others have used different techniques to quantify
movement artifact on the shank and thigh [2] but the
subjects investigated were from a population recovering
from leg fractures. In addition, only two subjects were
available with thigh mounted pin-markers and no subjects
were simultaneously instrumented with pin-markers on both
the shank and thigh. Recent progress using a 250 frame/s
0966-6362/$ – see front matter # 2005 Elsevier B.V. All rights reserved.
doi:10.1016/j.gaitpost.2005.04.012
GAIPOS-2158; No of Pages 13
DTD 5
2
D.L. Benoit et al. / Gait & Posture xxx (2005) xxx–xxx
stereoradiographic system is encouraging [7] but the
confined area of measurement limits the movement
possibilities of the subject.
Ideally, kinematic data would be reported with a standard
error of measurement that reflects the uncertainty of the
reported findings caused by this skin movement artifact
inherent in the measurement technique. When comparing
two groups of subjects and attempting to detect kinematic
differences associated with a population difference the
findings could be confidently reported with the knowledge
that observed differences are due to the population
differences and not measurement error.
Tracking the motion of the tibia and femur with surgically
implanted intra-cortical bone-pins instrumented with clusters of markers is an accurate means of directly measuring
skeletal motion under physiologically relevant testing
conditions [8]. Target clusters are tracked using any one
of the commercially available motion analysis systems and
movement of the underlying bones can be derived. The use
of percutaneous bone-pins mounted in the tibia and femur
and instrumented with no less than three reflective markers
can provide rigid body reconstruction using motion analysis.
Roentgen-stereophotogrammetric analysis (RSA) has been
used to relate the position of these markers to the anatomical
reference frame and to derive an anatomical coordinate
system to describe motion [9]. The principal is to reconstruct
the position of the bone-embedded markers to an anatomical
reference point, such as the deepest point of the
intercondylar groove for the femur and the most proximal
point of the medial condylar eminence for the tibia [4,5].
The anatomical reference points are used to determine the
origin of each segment, respectively. Using RSA it is
possible to apply a bone-embedded, or anatomical, reference
system when describing joint motion in a laboratory
reference frame. This simplifies data interpretation and,
given an accurate and reproducible choice of anatomical
reference points and coordinate system alignment, allows
comparisons not only within subjects but also potentially
across subjects. Combining RSA with bone-pins allows an
accurate representation of the bones but is technically
difficult and invasive [10,11]. However, the advantages
include the ability to accurately represent tibio-femoral
kinematics and, although an invasive technique, subjects
have been shown to walk [5,6,9,12], run [4,9,13] and hop [5]
normally.
Knowledge of non-sagittal plane tibio-femoral kinematics is necessary if we are to improve our knowledge of
the mechanisms associated with knee joint injury and the
progression of knee joint degeneration. For example, the
anterior cruciate ligament (ACL) injury is believed to lead to
degenerative joint disease [14]. Since injury mechanisms of
the ACL are thought to combine tibio-femoral rotation with
anterior tibial translation [15], knowledge of combined
sagittal and non-sagittal plane tibio-femoral joint motion
under physiological conditions is essential for detecting
critical phases of motion that may predispose the ACL to
loading. To our knowledge there is no information in the
literature about the ability to accurately measure tibiofemoral joint motion in non-sagittal plane movements.
This lack of information seriously limits the ability to
investigate knee joint injury mechanisms using non-invasive
techniques.
The purpose of this investigation is to quantify the error
caused by skin movement artifact when reporting the
kinematics of the tibio-femoral joint during movements that
incorporate sagittal and non-sagittal plane rotations. We
hypothesise that skin movement error will reduce the ability
to accurately measure 3D tibio-femoral kinematics and that
non-sagittal plane movements will be most affected by skin
movement artifact.
2. Methods
2.1. Subjects
Eight healthy, moderately active, male subjects with no
history of knee injury or prior surgical treatment of the lower
limbs were studied (Table 1). Informed consent was
obtained from the subjects and the study was approved
by the Ethics Committee of the Karolinska Hospital,
Stockholm, Sweden.
2.2. Surgical procedure
Stainless steel Apex self-drilling/self-tapping pins (Stryker Howmedica AB Sweden, 3.0 mm diameter, #5038-2110) were inserted under local anaesthetic into the distal
femur and proximal tibia of the right leg [11] at the
Karolinska University Hospital (Stockholm, Sweden). The
femoral pin was inserted between the Iliotibial (IT) band and
the quadriceps tendon superior of the vastus lateralis to
minimise impingement problems. Following surgery subjects performed active flexion and extension movements
while standing to identify whether movement restrictions
were evident. Subjects were then transported by wheelchair
to the motion analysis laboratory for data collection. The
pins remained inserted for the duration of the test. Upon
Table 1
Subject characteristics
Subject
Age
Height (cm)
Weight (kg)
1
2
3
4
5
6
7
8
32
22
22
32
31
27
22
22
185
181
180
171
174
178
181
175
89
78
78
86
62
76
93
63
Average
26
178.1
78.1
DTD 5
D.L. Benoit et al. / Gait & Posture xxx (2005) xxx–xxx
3
completion of the experiments (approximately 2 h), subjects
returned to the operating theatre to have the dressing and
pins removed.
2.3. Motion recordings
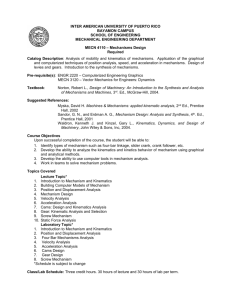
Fig. 1. (a) Picture of the bone-pin and surface marker configurations for a
representative subject. Note: the pins are inserted in the tibia and femur,
respectively. Each pin is instrumented with a target cluster, comprised of
four reflective markers. The skin is instrumented with four reflective surface
markers; (b) RSA procedure and calibration box. The right leg is extended
Triads of three non-collinear 7 mm reflective markers
(pin-markers) were affixed to the pins. Additional clusters of
four 10 mm surface markers (skin-markers) were affixed
onto the lateral and frontal aspects of both the right thigh and
shank (Fig. 1a and b). Skin-markers were spaced 10–15 cm
from adjacent markers within their respective cluster and
their arrangement was chosen to ensure they remained noncoplanar in at least two camera views throughout the range
of motion. Reflective markers were also placed on the right
heel, 5th metatarsal and lateral malleolus.
Bone-pin and skin-marker trajectories were tracked within
0.8 m3 measurement volume (1.1 m 0.8 m 0.9 m) using
four infrared cameras (ProReflex, Qualisys AB, Sweden),
sampling at 120 Hz. Marker coordinates were transformed
using the direct linear transform (DLT) and the raw 3D
coordinates exported and saved to a local computer for
analysis. The motion analysis system simultaneously collected both the skin- and pin-marker configurations for each
standing and movement trial.
Participants were asked to perform a series of normal
walking trials and lateral cutting manoeuvres. Each subject
was given several practice trials to familiarise themselves with
the pins and testing protocol. Ground reaction forces (GRF)
were measured simultaneously at 960 Hz using a Kistler force
plate (Kistler Instruments AG, Winterhur, Switzerland)
located midway through the measurement volume. For gait
testing, subjects walked along a 12 m walkway at a selfselected pace. Contact with the force plate and no evidence of
targeting were required for a trial to be considered.
Before performing the lateral cutting manoeuvre,
subjects jumped for maximal horizontal distance. Their
longest measurement was recorded and marked on the floor
to determine the proper takeoff distance to the force
platform. From an initial standing position the subject
pushed off using the left leg and, upon landing onto their
right foot, immediately pushed off the platform, cutting to
the left at an angle of approximately 458.
Five measurement trials were recorded for each movement task as well as a standing reference trial before and
after each block of movement trials. Subjects stood in a
neutral position and were instructed to align their feet
parallel to the force platform to define the tibial and femoral
anatomical coordinate systems. The orientation of the target
clusters from the first reference trial was matched against the
second to verify the pins did not bend and the triad did not
rotate during testing.
through the box with the bone-pins and reflective markers in place. The knee
is flexed between 08 and 108, RSA recordings were taken following motion
analysis sessions.
DTD 5
4
D.L. Benoit et al. / Gait & Posture xxx (2005) xxx–xxx
2.4. RSA technique and anatomical reference frame
Following the motion analysis recordings, the leg was
extended through a biplanar calibration box (Cage 10, RSA
Biomedical Innovations, Umeå, Sweden) and biplanar
radiographs (RSA) were recorded (Fig. 1b). All radiographs
were taken with the subject supine and the knee flexed
between 08 and 108. From these radiographs, two local
anatomical reference points were identified and digitised
with the aid of an experienced RSA technician (Sahlgrenska
University Hospital Gothenburg, Sweden; see acknowledgements). In total, 19 points were digitised to derive the
anatomical reference system using UMRSA software
(version 5, Biomedical Innovations-AB, Umea, Sweden).
These included:
1–4.
5.
6.
7–8.
9.
10–14.
15.
16.
17–18.
19.
Tibial pin-markers.
Proximal medial tibial eminence (tibial reference
point).
The most distal point along a line trough point 5
and parallel to the long axis of the tibia.
Medial and lateral edges of proximal tibia
respectfully.
A distal point along a line drawn perpendicular
to the long axis of the tibia and running
originating at the tibial reference point.
Femoral pin-markers.
Proximal (deepest) point of the condylar groove
(notch)
(femoral reference point).
The most distal point along a line trough point
15 and parallel to the long axis of the femur.
Medial and lateral edges of the distal femur,
respectively.
A distal point along a line drawn perpendicular
to the long axis of the femur and originating
at the femoral reference point.
Zt
vector joining points 5 and 6; from the tibial origin
directed longitudinally along the tibial axis in the
frontal plane.
2.5. Kinematic technique
Custom written software (Matlab, Mathworks, USA) was
developed and validated to process the 3D kinematic
information derived from the bone-pins and surface markers,
respectively [16]. The kinematic profile was described using
the terminology and the ordered sequence of the Joint
Coordinate System (JCS) [17]. In brief, the bone-embedded
coordinate system is defined from the RSA coordinate data:
the digitised points are used to locate the origin and direction
of the anatomical reference frames. Transformation matrices
for the pin-markers of both tibia and femur were derived to
relate the position of these points to their respective
anatomical origins [17,18]. 3D pin-marker coordinates from
the standing reference trials (SRT) were used to determine
the transformation matrix from the laboratory reference
frame to the bone-embedded reference frame. This
transformation matrix was then used to determine the
location of the skin-markers with respect to the boneembedded reference frame (Fig. 2). Kinematic data for both
the pin- and skin-markers were derived and low-passed
filtered at 12 Hz using a 20th order FIR digital filter
(Matlab). The cut-off frequency was determined by running
a Fourier analysis that retained 95% of the original signal
(both angular and linear data) and by visual inspection.
The limited measurement volume allowed recording of a
limited pre-foot-strike phase and complete stance phase of
the walking and cutting movements. Foot-strike and toe-off
were determined using the force platform data and the
corresponding frame number was identified in the kinematic
data. The kinematic data was normalised to 100% stance
The origin of the femoral reference frame was located at
the deepest point of the intercondylar groove (point 15). The
origin of the tibial reference frame was located at the highest
point of the medial intercondylar eminence (point 5). Local
coordinate systems of the femur and tibia were defined as
follows:
Xf
Yf
Zf
Xt
Yt
cross product of vectors Zf and Yf; from the femoral
origin, directed laterally.
cross product of Zf and vector joining points 17 and 18;
from the femoral origin, directed anteriorly.
vector joining points 15 and 16; from the femoral origin
directed longitudinally along the femoral axis in the
frontal plane.
cross product of vectors Zt and Yt; from the tibial
origin, directed laterally.
cross product of Zt and vector joining points 7 and 8;
from the tibial origin, directed anteriorly.
Fig. 2. Schematic representation of the anatomical reference frames and the
bone-pin marker cluster configurations. Adapted from Benoit DL (2005):
motion analysis of the knee: kinematic artifacts, EMG normalisation and
joint forces. Ph.D. thesis, Karolinska Institutet, Stockholm.
DTD 5
D.L. Benoit et al. / Gait & Posture xxx (2005) xxx–xxx
phase (foot-strike to toe-off = 100%). Pre-foot-strike was
expressed as a function of the normalised stance phase and
ranges from 10% (or the longest duration of pre-foot-strike
for that given subject) to 0% (foot-strike).
2.6. Statistical analysis
Three points of interest during the stance phase of the
walking and cutting cycle were chosen for statistical
analysis: heel strike (HS); mid-stance point (corresponding
with maximum knee flexion angle during the first 60% of
stance) (MS); and toe-off (TO). The kinematic data
derived from the bone-pins was considered the ‘gold
standard’ of measurement. Paired, two-tailed Student’s ttests were used to determine if skin derived kinematics at
the three time-points differed from those derived from the
bone-pins. Kinematic data at HS, MS, TO are often
extracted and used for comparisons of populations in gait
studies. As we were interested in the validity of making
such comparisons, we chose to treat each extracted point
as independent. Accuracy of the skin-marker kinematics
was calculated as the absolute difference between skin and
pin knee flexion/extension, abduction/adduction and
internal/external rotation angles and medio/lateral,
antero/posterior and distraction/compression translations
at HS, MS and TO.
In addition, the standard error of estimate (S) was
calculated for both walking and cutting. In this approach, the
error is implicitly assumed to arise entirely from the skinmarker data (Y), while the pin-marker data (X) is assumed to
be without error (E). In other words, since we assume that X
for a given point in time is accurate, then Y will predict X
such as (Y + E) within a certain confidence interval for that
given time point (see Appendix A for a description of S).
This data was calculated by comparing the pin- and skinmarker data across all subjects for each trial and at every
time point, with the average calculated across time points
(total number of time points: n = 110 walking, n = 105
cutting due to a shorter observed pre-foot-strike phase in
some subjects).
5
3. Results
Of the eight subjects, two subjects (numbers one and three
in Table 1) had data that were not usable: one subject was
excluded due to incomplete RSA data that rendered
transformation impossible, while the second subject bent
the femoral pin during knee flexion, the result of an interaction
with the soft tissue and musculature. No subjects experienced
significant pain and/or discomfort during the experiments and
all reported being able to move their knee freely despite pin
implantation. However, one subject was limited to three trials
for both walking and cutting while another was limited to
three trials for walking as recommended by the attending
surgeon to reduce exposure time for these subjects.
Simultaneously recorded high-speed digital video files
(100 frames/s; JVC model DVL9000, Japan) of the motions
indicated that all subjects contacted the force plate with the
heel during walking and the mid-foot during cutting.
Figs. 3 and 4 display rotations and translations of a
representative subject during both walking and cutting,
respectively. Absolute error between the skin-marker and
pin-marker kinematics at heel strike, mid-stance and toe-off
during the walking and cutting motions are noted in Table 2.
A significant difference in reporting skin-marker derived
kinematics with respect to actual tibio-femoral kinematics is
evidenced at heel strike, mid-stance and toe-off for both
walking and cutting rotations and translations. In the stance
phase of walking the average rotational absolute error
ranged from 2.48 to 4.48 while translational errors ranged
from 3.3 to 13.0 mm. In the cutting movement the range of
absolute errors and maximum absolute error were higher for
both rotations (3.38 to 13.18) and translations (5.6 to
16.1 mm) respectively.
The relationship between skin and pin derived kinematic
profiles observed across subjects differed considerably.
Figs. 5 and 6 illustrate the average error due to skin
movement for each during the stance phase of walking and
cutting, respectively. In Figs. 5 and 6 a positive value describes
an over-estimation, zero described perfect agreement and
negative values describe an under-estimation of the skin-
Table 2
Absolute error values of skin-marker derived kinematics at three time points during walking and cutting of knee rotations and translations: flexion–extension
(Flex/Ext), adduction–abduction (Add/Abd), internal–external rotation (Int/Ext); medio–lateral (Med/Lat), anterior–posterior (Ant/Post) and distraction–
compression (Dist/Comp)
Rotations (degrees S.D.)
Flex/Ext
Add/Abd
Translations (mm S.D.)
Int/Ext
Med/Lat
Ant/Post
Dist/Comp
Walk
Foot-strike
Mid-stance
Toe-off
2.8 (2.6)a
2.4 (2.0)a
2.7 (2.4)
2.5 (2.7)
3.1 (3.3)
4.4 (3.2)a
2.8 (2.0)a
2.4 (1.1)
2.2 (2.1)
5.0 (2.6)
5.5 (3.1)a
8.0 (5.7)
7.7 (4.4)a
6.2 (5.4)
13.0(5.0)a
5.0 (2.9)a
3.3 (2.4)a
5.0 (2.5)a
Cut
Foot-strike
Mid-stance
Toe-off
3.9 (2.9)
4.0 (2.5)
4.2 (2.7)
6.7 (5.4)a
5.9 (3.1)a
13.1 (9.8)
5.4 (4.2)a
5.4 (4.0)a
3.3 (1.8)a
7.3 (4.4)
5.9 (4.5)a
13.9(10.1)
5.6 (5.1)a
6.7 (4.4)a
16.1 (8.9)
6.3 (4.0)a
5.6 (3.8)a
8.3 (6.2)a
a
Significant difference between skin- and pin-marker data (two-tailed paired Student’s t-test, p < 0.05).
DTD 5
6
D.L. Benoit et al. / Gait & Posture xxx (2005) xxx–xxx
Fig. 3. Walking trials of a representative subject, subject-4. Knee joint flexion (+)/extension () (Flex/Ext), adduction (+)/abduction () (Add/Abd) and
internal (+)/external () (Int/Ext) rotation data is presented in the left column while lateral (+)/medial () (Med/Lat), anterior (+)/posterior () (Ant/Post) and
distraction (+)/compression () (Dist/Comp) are in the right column. Pin-marker labels are unfilled, skin-markers in bold.
marker derived knee joint rotations and translations. During
walking (Fig. 5) there appears to be some agreement across
subjects in the shape of the error profile for some rotations
(flexion/extension; internal/external) and translations (anterior/posterior; distraction/compression). With respect to the
magnitude and direction of the error (over or under-estimation
of joint position) there appears to be some agreement for
distraction/compression.
During cutting (Fig. 6) there appears to be greater
agreement in the shape of the error curves for both rotations
DTD 5
D.L. Benoit et al. / Gait & Posture xxx (2005) xxx–xxx
7
Fig. 4. Cut movement trials of a representative subject, subject-4. Knee joint flexion (+)/extension () (Flex/Ext), adduction (+)/abduction () (Add/Abd) and
internal (+)/external () (Int/Ext) rotation data is presented in the left column while lateral (+)/medial () (Med/Lat), anterior (+)/posterior () (Ant/Post) and
distraction (+)/compression () (Dist/Comp) are in the right column. Pin-marker labels are unfilled, skin-markers in bold.
(adduction/abduction, internal/external rotation) and translations (lateral/medial; antero/posterior) while the magnitude and direction of the error (over or under-estimation of
joint position) also shows agreement for distraction/
compression and antero/posterior translations.
While the absolute error is the absolute difference
between the skin-marker and pin-marker derived kinematics, the average standard error of the estimate (S)
describes the error associated with predicting pin-marker
based tibio-femoral kinematics from skin-marker derived
kinematics. The average S for walking and cutting
movements is found in Table 3 and represents the
expected margin of error when predicting tibio-femoral
joint motion using skin-markers. These error values were
higher in the cutting movement for both rotations and
translations.
DTD 5
8
D.L. Benoit et al. / Gait & Posture xxx (2005) xxx–xxx
Fig. 5. Progression of error due to skin movement during walking for all subjects. Figure show the average difference between skin-marker and pin-marker data
for each subject as it progressive during stance. A positive value describes an over-estimation, zero described perfect agreement and negative values describe an
under-estimation of the skin-marker derived knee joint rotations and translations. Left column: knee joint flexion (+)/extension () (Flex/Ext); adduction (+)/
abduction () (Add/Abd) and internal (+)/external () (Int/Ext). Right column: lateral (+)/medial () (Med/Lat); anterior (+)/posterior () (Ant/Post) and
distraction (+)/compression () (Dist/Comp).
4. Discussion
The purpose of this investigation was to quantify the error
caused by skin movement artifact when reporting the
kinematics of the tibio-femoral joint during movements that
incorporate sagittal and non-sagittal plane rotations. Skin
movement artifact is inherent in motion analysis using
surface markers and this study represents a comprehensive
record of the effect of skin movement during gait in healthy
subjects and, to our knowledge, the only record of the effect
DTD 5
D.L. Benoit et al. / Gait & Posture xxx (2005) xxx–xxx
9
Fig. 6. Progression of error due to skin movement during cutting for all subjects. It shows the average difference between skin-marker and pin-marker data for
each subject as it progressive during stance. A positive value describes an over-estimation, zero described perfect agreement and negative values describe an
under-estimation of the skin-marker derived knee joint rotations and translations. Left column: knee joint flexion (+)/extension () (Flex/Ext); adduction (+)/
abduction () (Add/Abd); internal (+)/external () (Int/Ext). Right column: lateral (+)/medial ()() (Med/Lat); anterior (+)/posterior () (Ant/Post) and
distraction (+)/compression () (Dist/Comp).
of skin movement during the cutting movement. We found
within subject data to be repeatable when using either the
skin or pin mounted markers for both the walk and cut. This
was encouraging however as the error associated with skin
movement artifact differed widely across subjects. Skin
movement of the thigh and shank may be large enough to
mask the actual movements of the underlying bones, thus
making reporting of knee joint kinematics using skinmarkers potentially uncertain.
With three subjects Reinschmidt et al. [4] reported
average errors relative to the range of motion of the knee
during the stance phase of running of 21% (flexion/
DTD 5
10
D.L. Benoit et al. / Gait & Posture xxx (2005) xxx–xxx
Table 3
Average standard error of the estimate (S) describing the error associated with predicting tibio-femoral kinematics from skin-marker derived kinematics
Rotations (8)
Walk
Cut
Translations (mm)
Flex/Ext
Add/Abd
Int/Ext
Med/Lat
Ant/Post
Dist/Comp
2.5
6.3
3.6
4.5
2.9
3.0
5.9
8.0
6.8
5.5
2.7
7.1
Average calculated for each data point of the stance phase (average of 110 data points) based on the estimated prediction of all walking (n = 25) and cutting
(n = 28) trials. For a description of S see Appendix A.
extension), 63% (internal/external rotation) and 70%
(abduction/adduction). No discussion of the error in recording joint translation was reported while an inadequate
calibration area added 28 measurement error to the rotational
data. Though only two subjects were observed over a limited
stance time, Houck et al. [6] found absolute differences of up
to 2.28 in the sagittal plane, 2.78 in the frontal plane and 1.88
in the transverse plane, while up to 13.9 mm of linear
displacement was observed during walking. The results of
these studies are comparable to those observed in our study.
Comparing kinematic data collected simultaneously from
surface markers and that of bone-embedded marker systems
fixed to an external fixation device, Cappozzo et al. [2]
reported skin-marker movement of 1–3 cm on the shank and
thigh, respectively leading to slightly higher rotational errors
then found in our study. However, the external fixator and the
fracture suffered by the subjects may have affected the
normal skin movement, walking ability and normal muscle
mass of the test subjects.
Using an externally fixed ‘bone tracker’ Manal et al.
[1,19] found that linear translations of the knee joint using
skin-markers of 2.1–7 mm depending on the plane of
movement, with average rotation errors below 38. Individual
subject deviations ranged between 48 and 78, depending on
the skin-marker configuration. These observations were
solely related to skin movement of the shank during the
stance phase of walking. It can be reasoned that errors would
likely have been higher had the effect of thigh skin
movement also been measured however the fact that their
results are comparable to our study shows promise for the
use of less invasive techniques to track bone motion.
With respect to walking, the profile of the error curves
appears to be somewhat similar in flexion/extension, internal/
external rotation, anterior/posterior translation and distraction/compression. However, the direction of the error (over/
under-estimation) differs widely in magnitude. It seems that if
the initial error could be estimated at a given time point (footstrike for example), the error could potentially be predicted
for that subject and the aforementioned parameters. This
however requires further investigation.
The error of subject 5 during walking consistently differs
from that of the other subjects around 60% of the stance
phase. Using the marker tracking portion of the QTrac
(Qualisys AB, Sweden) analysis software, visual inspection
of this subject’s raw pin-marker data revealed that tibiofemoral motion did occur around this time point when
visualised with the pin-markers. This movement pattern was
not witnessed using the skin-markers and thus contributed to
the altered error pattern around this time point. We believe
that the skin-markers were incapable of tracking this
underlying motion, as it should have been simultaneously
detected. The bone-pins and marker triad of this subject
were not found to be damaged or loosened upon removal and
this occurrence was not witnessed during the cutting trial,
which was performed after the walking trials. We therefore
believe this detected motion was a function of their walking
style and anatomy.
During the cut the profile of the error curves appears to be
more consistent than during walking. While the error
magnitudes are generally larger it appears that the skin
moves in a more consistent pattern across subjects and
indicates that the skin-markers were not sensitive enough to
track the motions of the underlying bones for this more
ballistic movement. The most important example is in the
measure of anterior/posterior tibial translation where skinmarker kinematics would have indicated a posterior
displacement in all subjects at 50% stance. This could be
indicative of the thigh marker clusters not responding to the
deceleration of the limb and thus continuing their forward
motion relative to the shank.
Knowledge of 3D motion in ACL deficient subjects is of
interest for both understanding the injury mechanisms as
well as the progression of degenerative joint disease. Recent
studies have attempted to identify compensatory mechanisms in ACL deficient subjects using skin-marker based
kinematics [20–22]. Although these studies associate altered
tibio-femoral rotations and translations during gait [21,22]
and a pivoting motion [20] with ACL deficiency, it is clear
from the results of our investigation that the reported
differences fall within the expected margin of error when
predicting tibio-femoral kinematics using skin mounted
markers. A set of standards for presentation of tibio-femoral
kinematics seems needed and could be derived from the data
in our study.
Since the subjects had sterile bandages around the pin
insertion sites and were instrumented with EMG electrodes,
it is possible that the skin movement at or near these points
could be reduced, similar to the findings of Manal et al. [1]
when using so called under-wrap. The skin-markers were
placed as far from the sterile bandages as possible, while still
maintaining adequate marker separation. The EMG electrode placement over the vastus lateralis, vastus medialis and
rectus femoris on the thigh and medial gastrocnemius on the
shank is common in human movement analysis and
DTD 5
D.L. Benoit et al. / Gait & Posture xxx (2005) xxx–xxx
therefore could represent a normal testing situation when
combining EMG and motion analysis. Although as little
wrapping as possible was used, it is possible that our testing
setup did reduce skin movement in these areas. In addition,
intra-cortical bone-pins could potentially alter the normal
walking and hopping patterns of the subjects in this study.
Previous studies have indicated that the kinematic profiles of
subjects using this technique are similar to those using noninvasive techniques [4,6,9]. None of the subjects expressed
discomfort while performing the walking or cutting trials in
this study. With regards to the cutting trials, there is limited
information to use for comparison however it is possible that
the movement would be less vigorous when using bone-pins
and possibly result in less skin movement. The results of this
study could therefore be safely extended to others as, at the
very least, a minimum approximation of skin movement
during cutting and walking.
The kinematics derived from the bone-pin-markers was
used as a so called ‘gold standard’ in this study. This assumes
the pins were rigidly fixed to the underlying bones and can be
used to represent true bone motion. There are potential
sources of error that could act alone or concurrently to
contradict this assumption [4,9–11]: the pins could move in
the bone, the marker cluster could move on the pin, the pin
could bend and/or the pins could vibrate. Mechanical testing
of the pins used in this study found that deflections larger than
0.4 mm caused permanent deformations that were visually
detectable [11]. The orientation of the target clusters from the
first reference trial was matched against the second to assess
potential marker cluster movement or pin-bending. This, in
addition to visual observation of removed pins for signs of pin
bending, as well as in the RSA images when digitising,
resulted in the exclusion of two subjects. The remaining six
subjects showed no evidence of pin bending or marker cluster
rotation and we therefore concluded that the pins were rigidly
fixed to the bones and no bending or marker cluster movement
corrupted the data. The bone-pin and marker-cluster complex
resonant frequency was found to be 90 Hz [11] and was
filtered out using the previously described low pass filter. We
have therefore concluded that bone-pin derived kinematic
measurement is a suitable ‘gold standard’ of measurement
under our testing conditions.
In this study, kinematic crosstalk was minimised by
rotating the knee joint flexion axis to minimise abduction
angle. This technique was tested on all six subjects however
only two subjects showed moderately reduced abduction
angles and were ‘corrected’ with this technique. This
correction could potentially have masked true abduction/
adductions or internal/external rotations of the lower leg.
However, it was decided that the reduction in artifact from
kinematic crosstalk was of greater importance. RSA is
highly accurate however the choice of the anatomical points
is subject to human error [23]. Very small changes in
digitised locations would amount to large changes in axial
alignment of the anatomical coordinate system. The fact that
four of six subjects required no axis realignment to reduce
11
kinematic crosstalk is an indication of well-chosen
anatomical points and well-aligned anatomical coordinate
systems. Furthermore, since the transformations and axes
are equivalent for both the skin- and pin-markers, neither
crosstalk nor the correction method would affect within
subject comparisons.
The determination of the anatomical reference points
used to establish the anatomical coordinate systems proved
to be far more difficult than originally anticipated. The
anatomical differences across subjects were significant with
respect to the medial and lateral edges of the tibia and femur,
for example. This applies not only to the location of the point
across subjects due to the size and location of the tibial
eminence relative to the plateau or the depth of the
intercondylar groove, but also the within subject relative
position of one condyle to the other. This could explain intersubject differences in limb abduction/adduction angle, for
example. In addition, if the knee joint was not fully extended
during the RSA image collection then moving into a joint
position more extended than this RSA image position will
result in a hyperextension recorded during the moving trials.
However, since the effective comparisons made in this study
are within subject and made with the same reference systems
within subject, the inter-subject differences in anatomical
reference frame alignment will not affect the comparison of
skin-marker to pin-marker kinematics.
It should also be noted that standard skin-mounted
anatomical reference markers were placed all subjects
during the standard reference trials and were visible in the
RSA images (medio-lateral femoral epicondyles and mediolateral tibial plateau). It was clear that the anatomical
reference point skin-marker locations were not representative of the underlying anatomy. In spite of this they were
relatively well-aligned to each other. Visual observation of
the femoral condyles in the RSA images clearly shows
anatomical alignment differences across subjects that would
likely not be reflected when using skin-markers for
anatomical reference frame alignment and could thus
conceal natural limb position biases.
The data from this study suggests that the use of skinmarkers to describe knee joint motion must be presented
with an envelope of accuracy that describes the artifact
imparted by skin movement of the markers. Although this
error varies throughout the stance phases of gait and cutting,
we propose the use of the average standard error of the
estimate when reporting the accuracy of skin-marker derived
kinematics. This estimate of the error (S) associated with
predicting tibio-femoral kinematics from skin-markers
would allow for the reporting of non-sagittal plane
kinematics within approximately 65% confidence interval
(for 95% confidence interval use 1.96 S) that may be
relevant in situations where large differences between
populations may be detected. Note that the use of S implies
that the error is randomly distributed about the actual tibiofemoral kinematic parameter for a given measurement data
point. The error in this study does not appear to be randomly
DTD 5
12
D.L. Benoit et al. / Gait & Posture xxx (2005) xxx–xxx
distributed within each subject. However, the direction of the
skin movement artifact is not repeatable across subjects in
this study and others [1,4,6] where skin movement artifact
has been evaluated. An error estimate that is not based on the
direction of the error is therefore preferred.
where n is the number of observations (comparisons), y the
skin-marker derived kinematic data point, and x is the bonepin derived kinematic data point
References
5. Conclusions
This study indicates that skin mounted reflective markers
display significant limitations in predicting 3D kinematics of
the knee joint. The absolute errors presented in this study
offer a guideline to which conclusions may be drawn from
3D knee joint kinematics for walking and cutting motions.
Although surface marker attachment methods affect knee
joint kinematics these affects are below those caused by skin
movement artifacts as reported in this study. We therefore
propose the use of a standard error of measurement when
presenting knee joint kinematic data. The data presented in
Table 3 could be used as guidelines when discussing findings
across populations. An additional finding of this study is that
the surface marker derived kinematics can present repeatable profiles within a subject for various movements
(Figs. 4 and 5). These repeatable patterns must not be
misinterpreted as accurately representing skeletal kinematics, at least beyond the sagittal plane of movement where
the error is small relative to the total movement. When
measuring knee joint kinematics under similar conditions
observations based on measurements below the standard
errors described in this study must be guarded.
Acknowledgements
The authors would like to thank Birgitta Runtze for her
aid with the RSA data and Mark Carpenter for his advice
with data analysis and the manuscript in general. This
project was partially funded by grants from the Centrum for
Idrottsforskning-Sweden and Nature Sciences and Engineering Research Council-Canada.
Appendix A
Standard error of the estimate: a measure of the error
associated with predicting the value of x from the dependant
observation y:
sffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi
X 2ffi
X
1
S¼
y
n
y2 nðn 2Þ
2
P
P
P
n xy x
y
2
P
P
n x2 x
[1] Manal K, McClay I, Stanhope S, Richards J, Galinat B. Comparison of
surface mounted markers and attachment methods in estimating tibial
rotations during walking: an in vivo study. Gait Posture 2000;11:38–
45.
[2] Cappozzo A, Catani F, Leardini A, Benedetti MG, Croce UD. Position
and orientation in space of bones during movement: experimental
artifacts. Clin Biomech 1996;11:90–100.
[3] Leardini A, Chiari L, Della CU, Cappozzo A. Human movement
analysis using stereophotogrammetry. Part 3. Soft tissue artifact
assessment and compensation. Gait Posture 2004.
[4] Reinschmidt C, van den Bogert AJ, Nigg BM, Lundberg A, Murphy N.
Effect of skin movement on the analysis of skeletal knee joint motion
during running. J Biomech 1997;30:729–32.
[5] Ramsey DK, Lamontagne M, Wretenberg PF, Valentin A, Engstrom B,
Nemeth G. Assessment of functional knee bracing: an in vivo threedimensional kinematic analysis of the anterior cruciate deficient knee.
Clin Biomech 2001;16:61–70.
[6] Houck J, Yack HJ, Cuddeford T. Validity and comparisons of tibiofemoral orientations and displacement using a femoral tracking
device during early to mid stance of walking. Gait Posture 2004;
19:76–84.
[7] Tashman S, Collon D, Anderson K, Kolowich P, Anderst W. Abnormal
rotational knee motion during running after anterior cruciate ligament
reconstruction. Am J Sport Med 2004;32:975–83.
[8] Ramsey DK, Wretenberg PF. Biomechanics of the knee: methodological considerations in the in vivo kinematic analysis of the
tibio-femoral and patellofemoral joint. Clin Biomech 1999;14:595–
611.
[9] Lafortune MA, Cavanagh PR, Sommer III HJ, Kalenak A. Threedimensional kinematics of the human knee during walking. J Biomech
1992;25:347–57.
[10] Lundberg A. On the use of bone and skin-markers for human movement research. Hum Movement Sci 1996;15:411–22.
[11] Ramsey DK, Wretenberg PF, Benoit DL, Lamontagne M, Nemeth G.
Methodological concerns using intra-cortical pins to measure tibiofemoral kinematics. Knee Surg Sport Tr A 2003;11:344–9.
[12] Levens AS, Inmanm VT, Blosser JA. Transverse rotation of the
segments of the lower extremity in locomotion. J Bone Joint Surg
(Am) 1948;30:859–72.
[13] Lafortune MA. Three-dimensional acceleration of the tibia during
walking and running. J Biomech 1991;24:877–86.
[14] Von Porat A, Roos EM, Roos H. High prevalence of osteoarthritis 14
years after an anterior cruciate ligament tear in male soccer players: a
study of radiographic and patient relevant outcomes. Br J Sport Med
2004;38:263.
[15] Peterson L, Renstrom PA. Sports injuries: their prevention and
treatment, 3rd ed., Martin Duntz; 2003. p. 271–93.
[16] Lafontaine D, Benoit DL, Lamontagne M, Xu L. Validation of joint
rotation and translation calculations using a joint coordinate system
approach. In: Proceedings of the 12th annual meeting of the European
society of movement analysis for adults and children; 2003.
[17] Grood ES, Suntay WJ. A joint coordinate system for the clinical
description of three-dimensional motions: application to the knee. J
Biomech Eng 1983;105:136–44.
[18] Challis JH. A procedure for determining rigid body transformation
parameters. J Biomech 1995;28:733–7.
[19] Manal K, McClay DI, Galinat B, Stanhope S. The accuracy of
estimating proximal tibial translation during natural cadence walking:
bone vs. skin mounted targets. Clin Biomech 2003;18:126–31.
DTD 5
D.L. Benoit et al. / Gait & Posture xxx (2005) xxx–xxx
[20] Ristanis S, Giakas G, Papageorgiou CD, Moraiti T, Stergiou N,
Georgoulis AD. The effects of anterior cruciate ligament reconstruction on tibial rotation during pivoting after descending stairs. Knee
Surg Sport Tr A 2003;11:360–5.
[21] Knoll Z, Kocsis L, Kiss RM. Gait patterns before and after anterior
cruciate ligament reconstruction. Knee Surg Sport Tr A 2004;12:7–14.
13
[22] Georgoulis AD, Papadonikolakis A, Papageorgiou CD, Mitsou A,
Stergiou N. Three-dimensional tibio-femoral kinematics of the anterior cruciate ligament-deficient and reconstructed knee during walking. Am J Sport Med 2003;31:75–9.
[23] Ryd L, Yuan X, Lofgren H. Methods for determining the accuracy of
radiostereometric analysis (RSA). Acta Orthop Scand 2000;71:403–8.