Research Report
advertisement

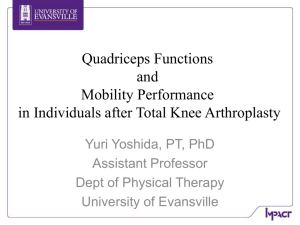
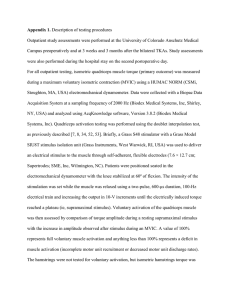
Research Report Early Postoperative Measures Predict 1- and 2-Year Outcomes After Unilateral Total Knee Arthroplasty: Importance of Contralateral Limb Strength Joseph A. Zeni Jr, Lynn Snyder-Mackler Background. Total knee arthroplasty (TKA) has been shown to be an effective surgical intervention for people with end-stage knee osteoarthritis. However, recovery of function is variable, and not all people have successful outcomes. Objective. The aim of this study was to discern which early postoperative functional measures could predict functional ability at 1 year and 2 years after surgery. Design and Methods. One hundred fifty-five people who underwent unilateral TKA participated in the prospective longitudinal study. Functional evaluations were performed at the initial outpatient physical therapy appointment and at 1 and 2 years after surgery. Evaluations consisted of measurements of height, weight, quadriceps muscle strength (force-generating capacity), and knee range of motion; the Timed “Up & Go” Test (TUG); the stair-climbing task (SCT); and the Knee Outcome Survey (KOS) questionnaire. The ability to predict 1- and 2-year outcomes on the basis of early postoperative measures was analyzed with a hierarchical regression. Differences in functional scores were evaluated with a repeated-measures analysis of variance. Results. The TUG, SCT, and KOS scores at 1 and 2 years showed significant improvements over the scores at the initial evaluation (P⬍.001). A weaker quadriceps muscle in the limb that did not undergo surgery (“nonoperated limb”) was related to poorer 1- and 2-year outcomes even after the influence of the other early postoperative measures was accounted for in the regression. Older participants with higher body masses also had poorer outcomes at 1 and 2 years. Postoperative measures were better predictors of TUG and SCT times than of KOS scores. J.A. Zeni Jr, PT, PhD, is Research Assistant Professor, Department of Physical Therapy, University of Delaware, 301 McKinly Laboratory, Newark, DE 19716 (USA). Address all correspondence to Dr Zeni at: jzenijr@gmail.com. L. Snyder-Mackler, PT, ScD, FAPTA, is Alumni Distinguished Professor, Department of Physical Therapy, and Academic Director, Graduate Program in Biomechanics and Movement Science, University of Delaware. [Zeni JA Jr, Snyder-Mackler L. Early postoperative measures predict 1and 2-year outcomes after unilateral total knee arthroplasty: importance of contralateral limb strength. Phys Ther. 2010;90: 43–54.] © 2010 American Physical Therapy Association Conclusions. Rehabilitation regimens after TKA should include exercises to improve the strength of the nonoperated limb as well as to treat the deficits imposed by the surgery. Emphasis on treating age-related impairments and reducing body mass also might improve long-term outcomes. Post a Rapid Response or find The Bottom Line: www.ptjournal.org January 2010 Volume 90 Number 1 Physical Therapy f 43 Early Measures After Unilateral Total Knee Arthroplasty T otal knee arthroplasty (TKA) has been proven to be an effective and cost-efficient intervention for end-stage knee osteoarthritis (OA). Most people who undergo TKA show marked improvements in function and reductions in pain compared with their preoperative condition.1,2 However, recovery of functional ability is variable, and not all patients experience significant improvements.3,4 The ability to predict which patients will have successful recoveries relies on the ability to identify factors that result in different functional outcomes. Preoperative measures that predict postsurgical functional status were examined in many previous investigations. Lower levels of preoperative quadriceps muscle strength (forcegenerating capacity) and selfperceived functional ability and a larger number of comorbidities have been shown to predict decreased functional ability 6 to 24 months after TKA.4 – 6 In the short term, greater preoperative knee pain and less preoperative range of motion (ROM) are related to reduced walking ability 2 months after surgery.7 Other factors, such as a high body mass index (BMI), female sex, and older age, have been implicated as factors that predict poor short-term outcomes, higher per-patient costs, or higher postoperative complication rates.8,9 Although preoperative predictors may aid in the identification of people at risk for postoperative difficulties, it also is important to recognize Available With This Article at ptjournal.apta.org • Audio Abstracts Podcast This article was published ahead of print on December 3, 2009, at ptjournal.apta.org. 44 f Physical Therapy Volume 90 early postoperative factors that may predict poor long-term outcomes. Van den Akker-Scheek et al10 found that early postoperative evaluations of self-efficacy were better predictors of long-term outcomes than preoperative evaluations. This finding is important because most people receive outpatient physical therapy services after TKA, but preoperative therapeutic interventions are not as common. Physical therapists, therefore, can tailor rehabilitation regimens to maximize early postoperative self-efficacy, whereas increasing preoperative self-efficacy is not always feasible. No studies have evaluated the ability to predict long-term functional outcomes on the basis of early postoperative measures. The purpose of this study was to discern whether age, BMI, pain, knee ROM, and knee strength measured at an initial physical therapy evaluation could predict functional ability at 1 year and 2 years after surgery. We hypothesized that certain factors would best predict long-term outcomes. Identification of these factors will aid in the creation of targeted therapeutic interventions to maximize postoperative functional ability. Method One hundred and fifty-five people who underwent primary unilateral TKA for end-stage knee OA participated in the study (Tab. 1). Before surgery, participants were excluded if they reported symptomatic OA in the contralateral limb, as measured by maximal pain of greater than 4 on a scale of 1 to 10 in that limb during daily activities. All participants signed an informed consent form approved by the Human Subjects Review Board of the University of Delaware. Participants were treated 2 or 3 times per week for 6 weeks in the same outpatient physical therapy clinic. Outpatient physical therapy began shortly after they concluded Number 1 home-based therapy (under direct physical therapist supervision) and had their staples removed. The physical therapy regimen consisted of progressive lower-extremity strengthening exercises, modalities to control pain and inflammation, electrical stimulation to improve quadriceps muscle function, and manual therapy to improve ROM (Appendix). Quantitative clinical measurements were obtained at the initial evaluation and at 1 and 2 years after surgery. These measurements included age, height, weight, bilateral quadriceps muscle strength, knee flexion and extension ROM, the Timed “Up & Go” Test (TUG), and a stairclimbing task (SCT). Two subsets of the Knee Outcome Survey (KOS), the activities of daily living subset (KOS-ADLS) and the pain subset (KOS-Pain), also were used. Quadriceps Muscle Strength Quadriceps muscle strength was defined in this study as the volitional isometric force created by the quadriceps muscle. It was measured with the participants seated with their knees flexed to 75 degrees and their hips flexed to 85 degrees on a KinCom dynamometer.* Knee flexion of 75 degrees was chosen to ensure consistency between time points and participants. After surgery, it was likely that a percentage of the participants would not be able to achieve knee flexion of greater than 75 degrees. Seventy-five degrees of knee flexion during isometric knee extension also results in the greatest force output of the quadriceps muscle after TKA.11 Participants were given verbal encouragement to kick “as hard as possible” for 3 seconds. Three trials were completed, and the average of these trials was recorded. The raw force measured by the dy* Isokinetic International, 6426 Morning Glory Dr, Harrison, TN 37341. January 2010 Early Measures After Unilateral Total Knee Arthroplasty namometer, in newtons, was normalized to each participant’s BMI (N/ BMI), and this value was used as quadriceps muscle strength. Table 1. Participant Demographics at Initial Evaluation, 1 Year, and 2 Yearsa Characteristicb Knee ROM Active knee flexion ROM was measured with participants in the supine position. The axis of the goniometer was aligned over the lateral epicondyle of the femur. The distal arm was aligned with the lateral malleolus of the fibula, and the proximal arm was aligned with the long axis of the shaft of the femur and directed toward the greater trochanter. Participants were instructed to maximally bend their knees by flexing their hips and sliding their heels toward their buttocks. No overpressure was applied by the therapist during knee flexion. Three trials were performed, and the average knee flexion angle was recorded. All measurements were obtained with respect to full extension of the knee being 0 degrees and increasing knee flexion being recorded as positive values. Goniometric measurements in people with knee OA have been shown to be highly reliable.12 TUG The TUG is a functional test that has been used extensively to examine functional outcomes in people with knee OA and after TKA.5,13,14 The test begins with a participant seated in a chair with both feet touching the floor. When instructed to “go,” the participant rises from the chair, walks 3 m, turns around, returns to the chair, and sits down. Participants were instructed to complete the task as quickly as possible. They performed 2 trials, and the average time to complete the task was recorded. They were permitted to use the arms of the chair during standing and returning to a seated position. This test has excellent interrater and intrarater reliability in older adults and is responsive to changes after TKA.15,16 January 2010 Age, y 64.9 (8.7) Sex, % of men/women 57/43 Height, m 2 Years (nⴝ125) 1.72 (0.10) 89.1 (17.0) 91.2 (17.5) 94.1 (18.6) BMI, kg/m2 30.2 (4.9) 31.0 (5.2) 31.8 (5.7) 6.3 (4.1) 0.4 (2.8) 0.3 (2.9) 97.1 (15.0) 120.1 (10.4) 120.2 (11.3) 9.9 (4.1) 20.7 (8.5) 20.6 (8.8) Nonoperated quadriceps muscle strength, N/BMI 24.0 (8.7) 22.7 (9.4) 21.0 (9.3) Days since surgery 27.7 (3.7) Flexion AROM, ° Operated quadriceps muscle strength, N/BMI b 1 Year (nⴝ155) Weight, kg Extension AROM, ° a Initial Evaluation (nⴝ155) Values are reported as mean (SD) unless otherwise indicated. BMI⫽body mass index, AROM⫽active range of motion. SCT The SCT is a measure of a participant’s ability to ascend and descend a flight of 12 steps as quickly as possible in a safe manner. Participants began at the bottom of the stairs and, at the investigator’s instruction, ascended the steps, turned around, and descended the steps as quickly as possible with the use of the handrail only if needed for balance. Participants performed 1 practice trial and then 2 timed trials, the average of which was recorded. This test has been used to successfully measure recovery after TKA.5,15,17 KOS For the purpose of this study, we used 2 subsets of the KOS, the KOSADLS and the KOS-Pain. The KOSADLS consists of 14 questions pertaining to a participant’s ability to perform activities of daily living. The KOS-ADLS is represented as a percentage score, with higher scores indicating higher levels of selfperceived functional ability. With the KOS-Pain, participants rate their pain on a 6-point scale, in which 0 represents no pain and 5 represents pain that prevents daily activities. The KOS has been shown to have high reliability and validity in people with knee pathology.18,19 Data Analysis A hierarchical regression model was created to predict the TUG, SCT, and KOS-ADLS scores at 1 and 2 years after TKA. Baseline test scores and then participant age, BMI, KOS-Pain score, flexion ROM, quadriceps muscle strength of the limb that underwent TKA (“operated limb”), and quadriceps muscle strength of the limb that did not undergo TKA (“nonoperated limb”), all obtained at the initial physical therapy evaluation, were entered into the hierarchical regression model as independent variables, in that order. The order of the variables was chosen on the basis of their clinical relevance, and the baseline test scores were entered first to account for changes in each variable over time. Preoperative quadriceps muscle strength and knee ROM are predictors of postoperative outcomes and often are directly addressed during postoperative physical therapy.5,7 For this reason, the order of the regression was designed to determine whether Volume 90 Number 1 Physical Therapy f 45 Early Measures After Unilateral Total Knee Arthroplasty Figure 1. Significant improvements in results of the Timed “Up & Go” Test (TUG) and stairclimbing task (SCT) and in scores on the activities of daily living subset of the Knee Outcome Survey (KOS-ADLS) at 1-year follow-up and 2-year follow-up (asterisk indicates P⬍.001). Error bars represent 95% confidence intervals. knee strength and ROM would significantly improve the predictive ability of the model, even when the influence of age, BMI, knee pain, and baseline test scores was accounted for. A change in the F score from each step of the model to the next (the addition of each variable) was analyzed for significance (Pⱕ.05). An analysis of variance with 1 repeated measure (time) was used to determine differences in the TUG, SCT, and KOS-ADLS scores at the initial evaluation and those at 1 and 2 years after TKA. Results Participants reported to outpatient physical therapy an average (median) of 28 days after TKA. The median number of physical therapy treatments was 17, with 90% of the participants receiving 16 to 18 treatments. No participants reported any major neurological or cardiovascular events after surgery. The Mauchley test of sphericity was significant, suggesting unequal variances between the time points. When the Green46 f Physical Therapy Volume 90 house–Geisser correction was used, a significant effect of time on all of the outcome measures was revealed. The TUG, SCT, and KOS scores at 1 and 2 years showed significant improvements over the scores at the initial evaluation (P⬍.001) (Fig. 1). The TUG and SCT showed 34% and 53% reductions in the times needed to complete the tasks at the initial evaluation and at 1 year, respectively. The KOS-ADLS score increased by 52% between the initial evaluation and 1 year. Post hoc testing revealed no significant differences between 1 and 2 years (P⬎.43). For descriptive purposes, the TUG, SCT, and KOS-ADLS scores at 3 months after TKA (near the time of discharge from physical therapy) were 8.23 seconds (SD⫽1.87 seconds), 13.63 seconds (SD⫽4.76 seconds), and 78.6% (SD⫽12%), respectively. Early postoperative values were predictive of the TUG, SCT, and KOS scores at 1 year after TKA (Tabs. 2, 3, and 4). After the other variables in the regression were accounted for, Number 1 the quadriceps muscle strength of the nonoperated limb significantly improved the predictive ability of the model with respect to the TUG, SCT, and KOS-ADLS scores. Increased force production in the nonoperated limb was related to improved scores on the TUG, SCT, and KOS (Fig. 2). Age also improved the predictive ability of the model for the TUG and SCT times, and BMI improved the predictive ability for the SCT time. A younger age and a lower BMI predicted better functional outcomes in terms of faster times to complete the TUG and SCT. The KOS-Pain and strength of the involved limb did not predict scores for outcomes. The BMI was the most significant predictor of the KOSADLS score (P⫽.023), with a higher postoperative BMI predicting a lower KOS-ADLS score at 1 year after TKA. A stronger quadriceps muscle in the nonoperated limb also significantly contributed to the prediction of an improved KOS-ADLS score, whereas age, the KOS-Pain, knee flexion ROM, and quadriceps muscle strength of the operated limb did not. One hundred twenty-five participants returned for the 2-year followup. The remaining 30 participants either failed to return for the 2-year follow-up or had undergone TKA less than 2 years earlier. Similar to the 1-year results, the quadriceps muscle strength of the nonoperated limb significantly improved the ability of the model to predict the TUG and SCT times at 2 years after TKA, even when the other variables were accounted for (Pⱕ.011) (Tabs. 2 and 3). Age also significantly added to the predictive ability of the model for the TUG and SCT times, whereas the BMI, KOS-Pain, knee flexion ROM, and quadriceps muscle strength of the operated limb did not. The trends were the same as those at 1 year, with a stronger quadriceps muscle and a younger age predicting January 2010 Early Measures After Unilateral Total Knee Arthroplasty Table 2. Timed “Up & Go” Test Results Modela Year 1 2 R R2 R2 Change F Change Significance of F Changeb TUG .587 .345 .345 80.581 <.001 TUG ⫹ age .657 .432 .087 23.264 <.001 TUG ⫹ age ⫹ BMI .663 .440 .008 2.126 .147 TUG ⫹ age ⫹ BMI ⫹ KOS-Pain .664 .441 .001 0.278 .599 TUG ⫹ age ⫹ BMI ⫹ KOS-Pain ⫹ ROM .671 .451 .010 2.720 .101 TUG ⫹ age ⫹ BMI ⫹ KOS-Pain ⫹ ROM ⫹ op quad muscle strength .672 .451 .000 0.065 .799 TUG ⫹ age ⫹ BMI ⫹ KOS-Pain ⫹ ROM ⫹ op quad muscle strength ⫹ nonop quad muscle strength .704 .495 .044 12.891 <.001 TUG .596 .355 .355 64.979 <.001 TUG ⫹ age .633 .401 .046 8.974 .003 TUG ⫹ age ⫹ BMI .645 .416 .015 3.061 .083 TUG ⫹ age ⫹ BMI ⫹ KOS-Pain .648 .419 .003 0.561 .456 TUG ⫹ age ⫹ BMI ⫹ KOS-Pain ⫹ ROM .650 .423 .004 0.735 .393 TUG ⫹ age ⫹ BMI ⫹ KOS-Pain ⫹ ROM ⫹ op quad muscle strength .654 .428 .005 1.018 .315 TUG ⫹ age ⫹ BMI ⫹ KOS-Pain ⫹ ROM ⫹ op quad muscle strength ⫹ nonop quad muscle strength .678 .460 .032 6.671 .011 a TUG⫽Timed “Up & Go” Test, BMI⫽body mass index, KOS-Pain⫽pain subset of the Knee Outcome Survey, ROM⫽range of motion, op quad⫽operated quadriceps, nonop quad⫽nonoperated quadriceps. b Values in bold type were significant at P⬍.05. Table 3. Stair-Climbing Task Results Modela Year 1 2 R R2 R2 Change F Change Significance of F Changeb SCT .656 .430 .430 115.510 <.001 SCT ⫹ age .694 .481 .051 15.008 <.001 SCT ⫹ age ⫹ BMI .704 .495 .014 4.128 .044 SCT ⫹ age ⫹ BMI ⫹ KOS-Pain .707 .500 .004 1.327 .251 SCT ⫹ age ⫹ BMI ⫹ KOS-Pain ⫹ ROM .721 .520 .021 6.405 .012 SCT ⫹ age ⫹ BMI ⫹ KOS-Pain ⫹ ROM ⫹ op quad muscle strength .721 .520 .000 0.000 .996 SCT ⫹ age ⫹ BMI ⫹ KOS-Pain ⫹ ROM ⫹ op quad muscle strength ⫹ nonop quad muscle strength .758 .574 .054 18.728 <.001 SCT .647 .419 .419 85.167 <.001 SCT ⫹ age .675 .455 .036 7.711 .006 SCT ⫹ age ⫹ BMI .685 .470 .014 3.162 .078 SCT ⫹ age ⫹ BMI ⫹ KOS-Pain .688 .474 .004 0.928 .337 SCT ⫹ age ⫹ BMI ⫹ KOS-Pain ⫹ ROM .697 .485 .012 2.556 .113 SCT ⫹ age ⫹ BMI ⫹ KOS-Pain ⫹ ROM ⫹ op quad muscle strength .699 .488 .003 0.650 .422 SCT ⫹ age ⫹ BMI ⫹ KOS-Pain ⫹ ROM ⫹ op quad muscle strength ⫹ nonop quad muscle strength .743 .552 .064 15.888 <.001 a SCT⫽stair-climbing task, BMI⫽body mass index, KOS-Pain⫽pain subset of the Knee Outcome Survey, ROM⫽range of motion, op quad⫽operated quadriceps, nonop quad⫽nonoperated quadriceps. b Values in bold type were significant at P⬍.05. January 2010 Volume 90 Number 1 Physical Therapy f 47 Early Measures After Unilateral Total Knee Arthroplasty Table 4. Knee Outcome Survey Results R R2 R2 Change F Change Significance of F Changeb KOS-ADLS .315 .099 .099 15.924 <.001 KOS-ADLS ⫹ age .316 .100 .001 0.180 .672 Modela Year 1 2 KOS-ADLS ⫹ age ⫹ BMI .363 .132 .032 5.248 .023 KOS-ADLS ⫹ age ⫹ BMI ⫹ KOS-Pain .377 .142 .010 1.655 .200 KOS-ADLS ⫹ age ⫹ BMI ⫹ KOS-Pain ⫹ ROM .377 .142 .001 0.087 .768 KOS-ADLS ⫹ age ⫹ BMI ⫹ KOS-Pain ⫹ ROM ⫹ op quad muscle strength .397 .158 .015 2.526 .114 KOS-ADLS ⫹ age ⫹ BMI ⫹ KOS-Pain ⫹ ROM ⫹ op quad muscle strength ⫹ nonop quad muscle strength .440 .194 .036 6.230 .014 KOS-ADLS .283 .080 .080 10.381 .002 KOS-ADLS ⫹ age .289 .083 .003 0.404 .526 KOS-ADLS ⫹ age ⫹ BMI .380 .144 .061 8.327 .005 KOS-ADLS ⫹ age ⫹ BMI ⫹ KOS-Pain .394 .155 .011 1.528 .219 KOS-ADLS ⫹ age ⫹ BMI ⫹ KOS-Pain ⫹ ROM .399 .159 .004 0.522 .472 KOS-ADLS ⫹ age ⫹ BMI ⫹ KOS-Pain ⫹ ROM ⫹ op quad muscle strength .399 .159 .000 0.013 .909 KOS-ADLS ⫹ age ⫹ BMI ⫹ KOS-Pain ⫹ ROM ⫹ op quad muscle strength ⫹ nonop quad muscle strength .409 .167 .008 1.100 .296 a KOS-DLS⫽activities of daily living subset of the Knee Outcome Survey, BMI⫽body mass index, KOS-Pain⫽pain subset of the Knee Outcome Survey, ROM⫽range of motion, op quad⫽operated quadriceps, nonop quad⫽nonoperated quadriceps. b Values in bold type were significant at P⬍.05. better functional outcomes at 2 years (Fig. 3). Similar to the 1-year results, BMI was the strongest predictor of the KOS-ADLS score at 2 years after TKA (P⫽.005) (Tab. 4); a lower BMI was related to a higher KOS-ADLS score at 2 years. The KOS-Pain and strength of the involved limb did not contribute significantly to any of the models. The R2 values for the TUG and SCT were more than twice the R2 values for the KOS-ADLS at 1 and 2 years (Tabs. 2, 3, and 4). Discussion The participants showed significant and clinically meaningful improvements in the first year after TKA. The recovery of function appeared to be nearly complete by this time because no improvements were seen between the 1- and 2-year time points. 48 f Physical Therapy Volume 90 As hypothesized, postoperative variables predicted scores on the TUG, SCT, and KOS-ADLS. A stronger quadriceps muscle on the nonoperated side and a younger age were the main variables related to improved 1and 2-year outcomes for the TUG and SCT. A lower BMI was important for maximizing self-reported measures of function at 1 and 2 years. Interestingly, these variables are not typically addressed during postoperative physical therapy. As expected, the participants in the present study showed dramatic increases in function at 1 year after TKA. This finding supports the general consensus that TKA is an effective intervention for restoring quantitative and self-perceived functional abilities.2,17,20,21 No improvements in the TUG, SCT, or KOS scores were seen between 1 and 2 years, suggest- Number 1 ing that the majority of functional recovery occurs within the first year after surgery. Other investigators examining multiyear outcomes have reported similar results.4,22 The early postoperative variables considered in the present study were better at predicting the scores of the quantitative functional measures at 1 and 2 years than at predicting the KOS-ADLS scores. The TUG and SCT had much higher R2 values than the KOS-ADLS at 1 and 2 years after TKA (Tabs. 2, 3, and 4). This inconsistency may be explained by the discrepancy between functional measures and self-reported measures of function.23,24 Quadriceps muscle strength and knee ROM are quantitative functional measures. An older age and a higher BMI also affected clinical measures and resulted in reduced strength, a lower freely choJanuary 2010 Early Measures After Unilateral Total Knee Arthroplasty sen walking speed, and impaired stair-climbing ability.25,26 Because most of the predictor variables are, or affect, quantitative measures, their predictive ability may have been oriented toward performancebased outcome measures rather than self-perceived functional ability. Many investigators have examined preoperative predictors of postoperative status in people who have undergone TKA; they concluded that greater preoperative knee flexion ROM and quadriceps muscle strength on the operated side or a higher level of self-perceived functional ability predicted improved outcomes.4,5,27,28 These variables often are addressed during physical therapy. The postoperative predictors noted in the present study were impairments that might not or cannot be addressed during physical therapy. Maximizing patients’ outcomes in minimal time is often the emphasis of physical therapy interventions. For this reason, clinicians focus on the most obvious functional deficits, such as knee ROM and strength of the operated limb. People who have undergone TKA show marked improvements in the quadriceps muscle strength of the operated limb after a course of physical therapy.17 However, in the present study, the strength of the nonoperated limb accounted for most of the variability in functional outcomes, with reduced strength predicting poorer outcomes. Rehabilitation regimens should also focus on improving the strength of the nonoperated limb because quadriceps muscle strength is strongly correlated with functional ability.29 If left untreated, weakness in the nonoperated limb may continue to impede functional ability and result in poorer 1- and 2-year functional outcomes. Although the inclusion of these variables may be vital to maximizing outcomes, knee flexion ROM and January 2010 Figure 2. Significant relationship between the quadriceps muscle strength of the nonoperated limb at initial evaluation and quantitative functional measures at 1 year. BMI⫽body mass index, SCT⫽stair-climbing task, TUG⫽Timed “Up & Go” Test. strength on the involved side should not be overlooked. It also is possible that the quadriceps muscle strength of the nonoperated limb represents disease progression on the nonoperated side.30 –32 People undergoing unilateral TKA often have bilateral joint disease.33 The more involved joint is typically replaced first, with the hope that improved functional ability will reduce the symptoms on the nonoperated side. However, the incidence of replacement of the cognate joint is relatively high, at 37%, by 10 years.33 It has been shown that the status of the nonoperated limb at 3 years after surgery best predicts the functional ability of the operated limb at that time point.34 Those data support our finding that reduced quadriceps muscle strength of the nonoperated limb predicted poorer long-term functional outcomes. If we can assume that quadriceps muscle weakness is related to disease progression, then people with more advanced OA in the nonoperated limb after TKA may expect poorer outcomes at 1 and 2 years after TKA. Although age is a variable that cannot be addressed by rehabilitation, age-related impairments, such as poor balance and strength, can be treated with rehabilitation.35,36 In addition to treating the deficits imposed by the surgery, physical therapists should focus on improving balance and generalized lowerextremity strength in older participants. Although further research is warranted, a rehabilitation regimen that incorporates training to treat age-related functional deficits may lead to improved functional outcomes. The older participants in the present study may have had a greater risk for poorer outcomes secondary Volume 90 Number 1 Physical Therapy f 49 Early Measures After Unilateral Total Knee Arthroplasty participants tended to have shorter TUG and SCT times. Although some participants with a quadriceps muscle strength of less than 30 N/BMI did have quick TUG and SCT times, others did not. This finding was clinically meaningful and suggested that if the quadriceps muscle strength of the nonoperated limb at the initial evaluation was greater than 30 N/BMI, then participants would likely achieve nearly normal TUG and SCT scores at 1 and 2 years after surgery. A quadriceps muscle strength of less than 30 N/BMI might not result in similar satisfactory outcomes. Figure 3. Significant relationship between the quadriceps muscle strength of the nonoperated limb at initial evaluation and quantitative functional measures at 2 years. BMI⫽body mass index, SCT⫽stair-climbing task, TUG⫽Timed “Up & Go” Test. to delayed recovery of muscle function after surgery; this notion provides support to the suggestion that undergoing TKA earlier in the course of OA or earlier in a patient’s life may improve functional outcomes.3,37 A higher BMI also was found to predict poorer outcomes, particularly those described by self-reported measures. This interesting finding suggests that having a high body mass or being overweight may skew how people view their functional capacity, even if there are no quantitative changes in function. Providing patients with access to nutrition and weight loss services is essential to reducing body mass after TKA because TKA alone does not facilitate weight loss.38 Clinicians and patients should treat high body mass as a separate concern that will not be resolved merely through improved 50 f Physical Therapy Volume 90 functional ability after TKA. Rehabilitation programs should include a cardiovascular component for patients with a high body mass after surgery. Although the TUG and SCT are measures that validly and reliably quantify functional ability, they do have a ceiling effect. However, these tests are still sensitive enough to measure differences between people with and without knee pathology39 (Figs. 2 and 3). The strength of the relationship between the quadriceps muscle strength of the nonoperated limb at the initial evaluation and the functional measures varied depending on the quadriceps muscle strength. When the quadriceps muscle strength was less than 30 N/BMI, there was much more variability in the data, whereas above 30 N/BMI, the relationship was less variable and Number 1 Despite the ceiling effect and the fact that the TUG and SCT scores reached a plateau within 1 year after surgery,29 we chose to include these measures to capture dysfunction that might have been associated with disease progression in the nonoperated limb. Functional ability, as determined with outcome measures, declines with time since surgery,40 possibly because of complications related to advanced age or deterioration of the cognate joint. We wanted to use a consistent set of measurement variables throughout the study, and although we did not expect to see much further improvement after 1 year, we wanted to ensure that we would be able to identify functional deficits if they occurred. The present study had a few limitations. First, the KOS-ADLS has been used to extensively evaluate people with knee pathology, although the instrument has not yet been validated for people with TKA. However, it is not likely that this instrument would be any less valid than similar measures of functional ability. Second, radiographs were not evaluated for disease progression in the contralateral limb, although correlations of radiographic disease progression and functional ability are weak.31,41 Finally, the determination January 2010 Early Measures After Unilateral Total Knee Arthroplasty of 30 N/BMI of quadriceps muscle strength as a cutoff for success with the TUG and SCT was based on a qualitative analysis of the data, and this value did not represent a statistical cutoff value. Traditional statistical methods of determining cutoff values rely on a dichotomous variable that represents success or failure. With the data and methodology used in the present study, no such dichotomous outcome variables were defined. Future investigations should be performed to evaluate disease progression on the contralateral side in relation to long-term functional ability. Additionally, future studies should be done to determine clinically and statistically meaningful cutoff values for variables that predict success or failure after TKA, such as quadriceps muscle strength. Because a portion of the variability was not explained by the variables selected in the present study, future work also should incorporate different predictor variables that might account for a portion of the unexplained variability. Of the variables selected, the strength of the nonoperated limb, age, and BMI explained most of the variability in functional outcomes at 1 and 2 years after TKA. The weakness of the nonoperated limb, older age, and higher BMI at the initial evaluation predicted poorer functional outcomes. Treatment regimens after TKA should focus on improving the strength of the nonoperated limb in addition to treating the deficits imposed by the surgery. People with more advanced disease progression on the nonoperated side may also experience poorer functional outcomes after TKA. Future research should focus on evaluating the effects of tailored rehabilitation protocols that incorporate bilateral quadriceps muscle strengthening, cardiovascular and weight loss regimens, and exercises January 2010 to reduce age-related impairments on long-term functional outcomes. Both authors provided concept/idea/research design, writing, and data analysis. Dr Snyder-Mackler provided project management, fund procurement, and facilities/ equipment. This study was approved by the Human Subjects Review Board of the University of Delaware. An abstract based on the data was presented at the 2009 World Congress of the Osteoarthritis Research Society International; September 10 –13, 2009; Montreal, Quebec, Canada. Funding for the study was provided by National Institutes of Health grants R01HD041055 (NICHD) and P20RR016458 (NCRR). This research also was funded by the National Center for Research Resources of the National Institutes of Health. This article was received March 17, 2009, and was accepted August 13, 2009. DOI: 10.2522/ptj.20090089 References 1 Cushnaghan J, Bennett J, Reading I, et al. Long-term outcome following total knee arthroplasty: a controlled longitudinal study. Ann Rheum Dis. 2009;68:642– 647. 2 Hawker G, Wright J, Coyte P, et al. Healthrelated quality of life after knee replacement. J Bone Joint Surg Am. 1998;80:163–173. 3 Fortin PR, Penrod JR, Clarke AE, et al. Timing of total joint replacement affects clinical outcomes among patients with osteoarthritis of the hip or knee. Arthritis Rheum. 2002;46:3327–3330. 4 Lingard EA, Katz JN, Wright EA, Sledge CB. Predicting the outcome of total knee arthroplasty. J Bone Joint Surg Am. 2004; 86:2179 –2186. 5 Mizner RL, Petterson SC, Stevens JE, et al. Preoperative quadriceps strength predicts functional ability one year after total knee arthroplasty. J Rheumatol. 2005;32:1533– 1539. 6 Jones CA, Voaklander DC, Suarez-Alma ME. Determinants of function after total knee arthroplasty. Phys Ther. 2003;83: 696 –706. 7 Parent E, Moffet H. Preoperative predictors of locomotor ability two months after total knee arthroplasty for severe osteoarthritis. Arthritis Rheum. 2003;49:36 –50. 8 Kreder HJ, Grosso P, Williams JI, et al. Provider volume and other predictors of outcome after total knee arthroplasty: a population study in Ontario. Can J Surg. 2003; 46:15–22. 9 Vincent HK, Vincent KR. Obesity and inpatient rehabilitation outcomes following knee arthroplasty: a multicenter study. Obesity (Silver Spring). 2008;16:130 – 136. 10 van den Akker-Scheek I, Stevens M, Groothoff JW, et al. Preoperative or postoperative self-efficacy: which is a better predictor of outcome after total hip or knee arthroplasty? Patient Educ Couns. 2007;66:92–99. 11 Silva M, Shepherd EF, Jackson WO, et al. Knee strength after total knee arthroplasty. J Arthroplasty. 2003;18:605– 611. 12 Cibere J, Bellamy N, Thorne A, et al. Reliability of the knee examination in osteoarthritis: effect of standardization. Arthritis Rheum. 2004;50:458 – 468. 13 Maly MR, Costigan PA, Olney SJ. Contribution of psychosocial and mechanical variables to physical performance measures in knee osteoarthritis. Phys Ther. 2005;85: 1318 –1328. 14 Ouellet D, Moffet H. Locomotor deficits before and two months after knee arthroplasty. Arthritis Rheum. 2002;47:484 – 493. 15 Kennedy DM, Stratford PW, Wessel J, et al. Assessing stability and change of four performance measures: a longitudinal study evaluating outcome following total hip and knee arthroplasty. BMC Musculoskelet Disord. 2005;6:3. 16 Podsiadlo D, Richardson S. The Timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39:142–148. 17 Yoshida Y, Mizner RL, Ramsey DK, SnyderMackler L. Examining outcomes from total knee arthroplasty and the relationship between quadriceps strength and knee function over time. Clin Biomech. 2008;23: 320 –328. 18 Irrgang JJ, Snyder-Mackler L, Wainner RS, et al. Development of a patient-reported measure of function of the knee. J Bone Joint Surg Am. 1998;80:1132–1145. 19 Marx RG, Jones EC, Allen AA, et al. Reliability, validity, and responsiveness of four knee outcome scales for athletic patients. J Bone Joint Surg Am. 2001;83:1459 – 1469. 20 National Institutes of Health. NIH Consensus Statement on total knee replacement. NIH Consens State Sci Statements. 2003; 20:1–34. 21 Fitzgerald JD, Orav EJ, Lee TH, et al. Patient quality of life during the 12 months following joint replacement surgery. Arthritis Rheum. 2004;51:100 –109. 22 Ritter MA, Wing JT, Berend ME, et al. The clinical effect of gender on outcome of total knee arthroplasty. J Arthroplasty. 2008;23:331–336. 23 Hidding A, van Santen M, De Klerk E, et al. Comparison between self-report measures and clinical observations of functional disability in ankylosing spondylitis, rheumatoid arthritis and fibromyalgia. J Rheumatol. 1994;21:818 – 823. 24 Wittink H, Rogers W, Sukiennik A, Carr DB. Physical functioning: self-report and performance measures are related but distinct. Spine. 2003;28:2407–2413. Volume 90 Number 1 Physical Therapy f 51 Early Measures After Unilateral Total Knee Arthroplasty 25 Al-Abdulwahab SS. The effects of aging on muscle strength and functional ability of healthy Saudi Arabian males. Ann Saudi Med. 1999;19:211–215. 26 Menz HB, Lord SR, Fitzpatrick RC. Agerelated differences in walking stability. Age Ageing. 2003;32:137–142. 27 Gandhi R, de Beer J, Leone J, et al. Predictive risk factors for stiff knees in total knee arthroplasty. J Arthroplasty. 2006;21: 46 –52. 28 Fortin PR, Clarke AE, Joseph L, et al. Outcomes of total hip and knee replacement: preoperative functional status predicts outcomes at six months after surgery. Arthritis Rheum. 1999;42:1722–1728. 29 Mizner RL, Petterson SC, Snyder-Mackler L. Quadriceps strength and the time course of functional recovery after total knee arthroplasty. J Orthop Sports Phys Ther. 2005;35:424 – 436. 30 Liikavainio T, Lyytinen T, Tyrvainen E, et al. Physical function and properties of quadriceps femoris muscle in men with knee osteoarthritis. Arch Phys Med Rehabil. 2008;89:2185–2194. 52 f Physical Therapy Volume 90 31 McAlindon TE, Cooper C, Kirwan JR, Dieppe PA. Determinants of disability in osteoarthritis of the knee. Ann Rheum Dis. 1993;52:258 –262. 32 Slemenda C, Brandt KD, Heilman DK, et al. Quadriceps weakness and osteoarthritis of the knee. Ann Intern Med. 1997; 127:97–104. 33 Ritter MA, Carr KD, Keating EM, Faris PM. Long-term outcomes of contralateral knees after unilateral total knee arthroplasty for osteoarthritis. J Arthroplasty. 1994;9:347–349. 34 Farquhar S, Snyder-Mackler L. The Chitranjan Ranawat Award: the nonoperated knee predicts function 3 years after unilateral total knee arthroplasty [published online ahead of print May 27, 2009]. Clin Orthop Relat Res. doi:10.1007/s11999-0090892-9. 35 Taaffe DR, Duret C, Wheeler S, Marcus R. Once-weekly resistance exercise improves muscle strength and neuromuscular performance in older adults. J Am Geriatr Soc. 1999;47:1208 –1214. 36 Nichols JF, Hitzelberger LM, Sherman J, Patterson P. Effects of resistance training on muscular strength and functional abilities of community-dwelling older adults. J Aging Phys Act. 1995;3:238 –250. Number 1 37 Tanaka T, Kariya Y, Hoshino Y. Histochemical study on the changes in muscle fibers in relation to the effects of aging on recovery from muscular atrophy caused by disuse in rats. J Orthop Sci. 2004;9: 76 – 85. 38 Donovan J, Dingwall I, McChesney S. Weight change 1 year following total knee or hip arthroplasty. ANZ J Surg. 2006;76: 222–225. 39 Petterson SC, Raisis L, Bodenstab A, Snyder-Mackler L. Disease-specific gender differences among total knee arthroplasty candidates. J Bone Joint Surg Am. 2007; 89:2327–2333. 40 Benjamin J, Johnson R, Porter S. Knee scores change with length of follow-up after total knee arthroplasty. J Arthroplasty. 2003;18:867– 871. 41 Creamer P, Lethbridge-Cejku M, Hochberg MC. Factors associated with functional impairment in symptomatic knee osteoarthritis. Rheumatology (Oxford). 2000;39: 490 – 496. January 2010 Early Measures After Unilateral Total Knee Arthroplasty Appendix. Physical Therapy Treatment Regimen–Aggressive Strengthening Protocol All exercises were incorporated into treatment in the clinic and were advanced as described below. Direct physical therapist guidance and assistance were provided for all exercises until participants became self-sufficient and completed the exercises with proper form. Participants also performed stretching and strengthening exercises at home on days on which they did not receive physical therapy in the clinic. I. Warm-up exercise a. Five to 10 minutes of riding an exercise bicycle II. Range of motion (for participants with less than 120 degrees of knee flexion or with knee flexion contracture) a. Patellar mobilization (if indicated) 1. Three sets of 10 repetitions with knee in full extension 2. Active superior patellar glides b. Incision mobility 1. Soft-tissue mobilization of the entire length of the incision 2. Greater emphasis on the distal third c. Knee extension stretch 1. Manual overpressure on the knee d. Standing knee flexion stretch 1. The participant stands at the bottom of a flight of stairs with the foot of the operated side placed on the third step. While holding the rail, the participant leans forward, sits down to bend the knee to the end range, and holds the position for 30 seconds. The participant repeats the exercise 3 times. 2. Supine active assisted wall slides e. Manual stretching of hamstring muscle, quadriceps muscle, gastrocnemius muscle, and joint capsule as needed III. Strengthening a. Weight should be 70% of participant’s 1-repetition maximum b. Three sets of 8 repetitions for all exercises c. One to 2 minutes of rest between sets d. Exercises are advanced when the participant can complete the exercises and maintain control through 3 sets of 8 repetitions e. Exercises (initial) 1. Straight leg raises (without quadriceps muscle lag) ● The participant lies supine with the hip and knee on the nonoperated side flexed and the foot placed flat on an exercise table. The participant first isometrically contracts the quadriceps muscle and then lifts the leg to about 45 degrees of hip flexion while keeping the knee extended. The participant lowers the leg slowly to the starting position. 2. Hip abduction (side-lying position) ● The participant is in the side-lying position on the nonoperated side. The participant flexes the bottom leg for balance and then lifts the top leg until 45 degrees of hip abduction is reached. The participant lowers the abducted leg slowly to the starting position. The participant should not externally rotate the hip during abduction. 3. Standing terminal knee extension with resistance band ● The participant stands with a rubber band resisting knee extension. The participant flexes the knee to 45 degrees and straightens the leg against the resistance to full extension. 4. Lateral step-ups ● The exercise begins with a 5.08-cm (2-in) block and advances to a 10.16-cm (4-in) block and then a 15.24-cm (6-in) block. The participant should step to the side with slow, controlled movements during ascent and descent. 5. Hamstring muscle curls ● Standing with hands on a table or counter for support, the participant flexes the knee maximally. (Continued) January 2010 Volume 90 Number 1 Physical Therapy f 53 Early Measures After Unilateral Total Knee Arthroplasty Appendix. Continued f. Exercises (additional) 1. Seated knee extension (90°–0°) ● The participant sits on a knee exercise machine with the knee bent to 90 degrees and the tibial pad placed at a 2-finger width proximal to the lateral malleolus. The participant extends the knee to full extension and then slowly lowers it to the starting position. 2. Terminal knee extension (45°–0°) ● With the participant in the long sitting position, a bolster is placed under the operated knee to keep it in a flexed position (45°). The participant extends the knee to full extension and then slowly lowers it to the starting position. 3. Heel-raises ● In the standing position, the participant raises the heel as far as possible and then slowly lowers it to the starting position. Bilateral heel-raises are used if the participant is unable to perform 15 repetitions of the unilateral heel-raise. Unilateral heel-raises are used if the participant is able to perform more than 15 repetitions of the unilateral heel-raise. A weighted backpack is used to increase the challenge once the participant is able to perform 3 sets of 10 repetitions of unilateral heel-raises. 4. Wall slides ● Standing with the back against the wall, the participant flexes the hips and knees, slides the back down until reaching 45 degrees of knee flexion, and then slides the back up to return to the starting position. The exercise is advanced by increasing the degree of knee flexion up to 90 degrees. 5. Front lunges ● Standing with hands on hips, the participant puts the involved leg forward and lunges until the forward knee reaches 45 to 90 degrees, depending on the level of progression. IV. Quadriceps femoris neuromuscular electrical stimulation a. The participant is seated on a Kin-Com dynamometer with the involved knee flexed to 60 degrees, and a portable stimulator (Empi 300pv)a is used for stimulation. The participant performs 1 submaximal warm-up and then 2 maximum voluntary isometric contractions (MVICs). The average of the 2 MVICs is considered to be the participant’s daily MVIC. b. Parameters 1. On time: 12 seconds; off time: 50 seconds 2. Symmetrical waveform at 50 pulses per second 3. Two-second ramp time 4. Pulse width of 400 microseconds 5. Amplitude to maximum tolerable (at least 30% of the MVIC) c. Ten contractions per session d. Three sessions per week until the quadriceps muscle MVIC is 80% of that of the uninvolved limb V. Management of pain and swelling a. Ice and elevation after exercises b. Compression as needed VI. Functional retraining a. Gait training with emphasis on heel-strike and push-off at toe-off and on normal knee joint excursions b. Stair ascending and descending 1. Step-over-step pattern 2. Training should be performed when the unilateral stance is steady and not painful a Empi, 599 Cardigan Rd, St Paul, MN 55126-4099. 54 f Physical Therapy Volume 90 Number 1 January 2010