The Impacts of the Affordable Care Act: How Reasonable
Are the Projections?
The MIT Faculty has made this article openly available. Please share
how this access benefits you. Your story matters.
Citation
Gruber, Jonathan. "THE IMPACTS OF THE AFFORDABLE
CARE ACT: HOW REASONABLE ARE THE PROJECTIONS?"
Working paper series (National Bureau of Economic Research),
working paper 17168. National Bureau of Economic Research,
(June 2011). 26 p.
As Published
http://www.nber.org/papers/w17168
Publisher
National Bureau of Economic Research
Version
Author's final manuscript
Accessed
Mon May 23 10:53:12 EDT 2016
Citable Link
http://hdl.handle.net/1721.1/72971
Terms of Use
Creative Commons Attribution-Noncommercial-Share Alike 3.0
Detailed Terms
http://creativecommons.org/licenses/by-nc-sa/3.0/
NBER WORKING PAPER SERIES
THE IMPACTS OF THE AFFORDABLE CARE ACT:
HOW REASONABLE ARE THE PROJECTIONS?
Jonathan Gruber
Working Paper 17168
http://www.nber.org/papers/w17168
NATIONAL BUREAU OF ECONOMIC RESEARCH
1050 Massachusetts Avenue
Cambridge, MA 02138
June 2011
Forthcoming as part of a Forum on Health Care Reform and the U.S. Budget, National Tax Journal.
Jonathan Gruber served as a paid advisor to the Romney Administration and Massachusetts Legislature
during the development of health care reform in Massachusetts, and has since been a member of the
Commonwealth Health Connector Board that oversees implementation of the law. He was also a paid
technical consultant to the Obama Adminstration during the development of the Affordable Care Act.
The views expressed herein are those of the author and do not necessarily reflect the views of the
National Bureau of Economic Research.
© 2011 by Jonathan Gruber. All rights reserved. Short sections of text, not to exceed two paragraphs,
may be quoted without explicit permission provided that full credit, including © notice, is given to
the source.
The Impacts of the Affordable Care Act: How Reasonable Are the Projections?
Jonathan Gruber
NBER Working Paper No. 17168
June 2011
JEL No. H3,I18
ABSTRACT
The Patient Protection and Affordable Care Act (ACA) is the most comprehensive reform of the U.S.
medical system in at least 45 years. The ACA transforms the non-group insurance market in the United
States, mandates that most residents have health insurance, significantly expands public insurance
and subsidizes private insurance coverage, raises revenues from a variety of new taxes, and reduces
and reorganizes spending under the nation’s largest health insurance plan, Medicare. Projecting the
impacts of such fundamental reform to the health care system is fraught with difficulty. But such projections
were required for the legislative process, and were delivered by the Congressional Budget Office (CBO).
This paper discusses the projected impact of the ACA in more detail, and describes the evidence that
sheds light upon the accuracy of the projections. It begins by reviewing in broad details the structure
of the ACA and then reviews evidence from a key case study that informs our understanding of the
ACA’s impacts: a comparable health reform that was carried out in Massachusetts four years earlier.
The paper discusses the key results from that earlier reform and what they might imply for the impacts
of the ACA. The paper ends with a discussion of the projected impact of the ACA and offers some
observations on those estimates.
Jonathan Gruber
MIT Department of Economics
E52-355
50 Memorial Drive
Cambridge, MA 02142-1347
and NBER
gruberj@mit.edu
I. INTRODUCTION
On March 23, 2010, President Obama signed into law the Patient Protection and
Affordable Care Act (ACA), the most comprehensive reform of the U.S. medical system in at
least 45 years. The ACA transforms the non-group insurance market in the United States,
mandates that most residents have health insurance, significantly expands public insurance and
subsidizes private insurance coverage, raises revenues from a variety of new taxes, and reduces
and reorganizes spending under the nation’s largest health insurance plan, Medicare. If fully
implemented, the ACA promises to lead to a dramatically different health care landscape for the
United States in the years to come.
Projecting the impacts of such fundamental reform to the health care system is fraught
with difficulty. But such projections were required for the legislative process, and were delivered
by the Congressional Budget Office (CBO). CBO projected that the ACA would increase health
insurance coverage by 32 million people and would raise federal government spending by almost
$1 trillion over the subsequent decade, but would raise revenues and reduce spending by even
more so that the bill overall reduced the federal budget deficit. These CBO projections were
central to the legislative debate over the ACA.
In this article, I discuss the projected impact of the ACA in more detail, and describe
evidence that sheds light upon the accuracy of the projections. I begin by reviewing in broad
detail the structure of the ACA. I then review the evidence from a key case study that informs
our understanding of the ACA’s impacts: a comparable health reform that was carried out in
Massachusetts four years earlier. I discuss the key results from that earlier reform and what they
2 might imply for the impacts of the ACA. Finally, I discuss the projections of the impact of the
ACA and offer some observations on those estimates.
II. THE AFFORDABLE CARE ACT
The ACA is an enormously detailed piece of legislation which touches on many aspects
of our health care system. I begin by providing a broad outline of the ACA’s key features to help
guide the discussion of the bill’s projected effects.
A. Background: U.S. Health Care
The United States spends 17 percent of its gross domestic product (GDP) on health care,
by far the most of any nation in the world. Moreover, the rate of health care spending is rapidly
outstripping the rate of growth of our economy, so that by 2080 health care spending is projected
to account for 40 percent of the U.S. economy (CBO, 2010a).
Despite this high level of spending, there remain enormous disparities in access to health
care in our nation. For example, the infant mortality rate for whites in the United States is 0.57
percent, while for blacks it is more than twice as high, at 1.35 percent.1 Many of these disparities
can be attributed to the fact that the United States is the only major industrialized nation without
universal access to health care. Almost one in five of the non-elderly, 50 million Americans,
have no health insurance coverage. The distribution of insurance coverage is shown in Table 1
(which is based on Fronstin, 2010).
The primary source of insurance coverage in the United States is employer-sponsored
insurance (ESI), which covers the majority of non-elderly Americans in the United States. This is
due to both the risk pooling provided by the workplace setting and the large tax subsidy provided
1
The Henry J. Kaiser Family Foundation, “Infant Mortality Rate (Deaths per 1,000 Live Births)
by Race/Ethnicity, Linked Files, 2004–2006,”
http://www.statehealthfacts.org/comparetable.jsp?cat=2&ind=48.
3 to ESI. As discussed in more detail in Gruber (2011b), the federal government forgoes roughly
$250 billion per year by excluding compensation in the form of health insurance from income
and payroll taxation. Since health insurance provided through employers is purchased with pretax dollars while insurance provided outside the employment setting is bought with post-tax
dollars, there is a strong incentive for insurance to be provided in the employment setting.
There are also two major sources of public insurance coverage. The Medicare program is
a universal insurance program for the elderly in the United States, while the Medicaid program
provides coverage for many of the poor, with a particular focus on low income children. As a
result, most uninsured are not the poorest Americans, but the “working poor” — those whose
income and age leaves them ineligible for public insurance coverage and who are not offered
insurance through their places of employment.
The only avenue available to such individuals is the non-group insurance market. In most
states, however, this market discriminates against the sick. Non-group insurance often features
“pre-existing conditions exclusions” that exclude from coverage any spending on illnesses that
were present at the time of insurance purchase. Moreover, non-group insurance availability can
be limited and prices very high for those who become ill. In a dynamic sense, this market does
not provide real insurance protection against illness. As a result, those outside of the employer
and public insurance systems face significant financial risk from illness.
B. Broad Outline of the Affordable Care Act
The core of the ACA is a “three-legged stool” designed to fix the broken non-employer
insurance market in the United States and expand health insurance coverage as a result. The first
leg of the stool includes reforms to the non-group insurance market. These include outlawing
exclusions for pre-existing conditions and other discriminatory practices, guaranteeing access to
4 non-group insurance, and imposing limits on the ability of insurers to charge differential prices
by health status — prices for a given product can only vary by age (subject to a 3:1 limit) and
smoking status (subject to a 1.5:1 limit). In addition, minimum standards are set for insurance in
the non-group and small group markets, including a list of “essential benefits” that must be
included in an insurance package and a minimum “actuarial value” (the share of total spending
on the essential benefits package that is covered, on average for a typical population, by
insurance) of 60 percent.
While these reforms are viewed by most as long overdue, most experts argued that they
cannot survive in a vacuum. In particular, if individuals are guaranteed insurance access at prices
that are independent of health status, then many may “free ride” by remaining uninsured until
they are sick and then buying insurance at average prices. Under these circumstances, insurers
will have to charge high prices to all to account for the fact that the pool buying insurance is
sicker than average. The resulting adverse selection cycle leads to high prices and a failed
insurance market. Indeed, this point is not just a theoretical curiosity. In the 1990s, five states
tried to reform their non-group insurance markets in such a manner, and by 2006 these were five
of the most expensive states in the nation in which to purchase non-group insurance (Gruber,
2011a).
The second leg of the stool is therefore a requirement that individuals purchase insurance,
or an individual mandate. More specifically, most individuals in the United States are required to
have coverage or to pay a penalty, which ultimately (by 2016) amounts to the larger of 2.5
percent of income or $695.
The problem with an individual mandate, however, is that it may be impossible to enforce
— as well as inadvisable to enforce — if insurance is not affordable. This motivates the third leg
5 of the stool: government subsidies to make insurance affordable for lower income families.
Under the ACA, these subsidies come in two forms. The first is an expansion of the Medicaid
program to all individuals with incomes below 133 percent of the poverty line (which is $10,830
for individuals and $22,050 for a family of four). The second is tax credits to offset the cost of
private non-group insurance. These tax credits are designed to cap the share of income that
individuals have to spend to get insurance, beginning with a cap at 3 percent of income at 133
percent of the poverty level and rising to a cap of 9.5 percent of income at 300 percent of the
poverty level (and remaining at 9.5 percent until 400 percent of the poverty level). In addition, if
individuals have incomes below the threshold for income tax filing, or if the cheapest health
insurance option available to them costs more than 8 percent of their income, they are exempt
from the mandate penalty.
The ACA primarily finances these subsidies through six sources (with their associated
share of financing): (1) a reduction in reimbursements to private “Medicare Advantage”
programs that provide an alternative to the government Medicare program for seniors (14%); (2)
reductions in Medicare reimbursement, primarily through a reduction of the inflation adjustment
provided to hospitals each year for their reimbursements under Medicare (33%); (3) an increase
in the Medicare payroll tax by 0.9 percent, and the extension of that tax to capital income, for
singles with incomes of more than $200,000 per year and families with incomes of more than
$250,000 per year (21%); (4) new excise taxes on several of the sectors that are likely to benefit
from the expanded coverage of medical spending in the United States, including insurers,
pharmaceutical companies, and medical device manufacturers (11%); (5) the “Cadillac tax,” a
non-deductible 40 percent excise tax on insurance products that cost more than $10,200 for an
individual or $27,500 for a family in 2018, with those limits indexed each year to the consumer
6 price index (3%); and other revenue sources such as penalty payments by individuals and
employers, and taxes on the higher wages that result from reduced employer spending on
insurance (21%).
The ACA also includes a number of provisions to address the problem of rapidly rising
health costs in the United States. The first is the Cadillac tax, which should reduce the incidence
of very generous health insurance plans and thereby excessive demand for health care. The
second is new health insurance “exchanges,” state-organized marketplaces where non-group and
small group insurers must compete in a transparent marketplace that is designed to maximize
competition and lower premiums. The third is the Independent Payment Advisory Board, which
is charged with re-designing reimbursement of providers under Medicare to lower costs and
ensure quality; this board’s recommendations are subject to an up or down vote by Congress.
The fourth is a new research institute — with sizeable funding — to study the comparative
effectiveness of medical treatments, in an effort to understand which treatments are most cost
effective. Finally, there are many pilot programs examining alternative organizations and
reimbursement structures for medical providers in an attempt to finds ways to undo the
pernicious incentives of our retrospective “fee-for-service” medical reimbursement system.
There are dozens of other provisions in the ACA that are not reviewed here as well, on topics
ranging from incentives for improving the quality of health care, to a new social insurance
program for long-term care, to incentives to increase primary care provision, and so on.
III. THE MASSACHUSETTS CASE STUDY
Projecting the impacts of a fundamental reform such as that described above is an
enormous challenge. The effects of the ACA will depend on dozens of behavioral responses by
firms and individuals (as well as state governments). There are several decades of empirical
7 research in health economics that can help inform our understanding of these behavioral
responses; Gruber (2002) provides a review of some of that evidence. But this past evidence is
by necessity based on changes to the existing health insurance environment, and may not be fully
indicative of the impacts of a fundamental change in the environment as sweeping as ACA.
A. The Massachusetts Experiment
Fortunately, our understanding of the impacts of the ACA can be further informed by the
experience of Massachusetts. In April 2006, Massachusetts passed a health reform that was
based on the same “three-legged stool” as the ACA, and in many ways inspired the federal
program. Massachusetts was one of the five states that had already reformed its non-group
markets in the 1990s and, as a result, had a small and expensive non-group market. Part of the
goal of reform in the state was to fix that market, while covering the majority of the roughly
600,000 uninsured residents of the state.
The key aspects of reform in Massachusetts were to supplement the existing reforms of
the non-group market with the introduction of an individual mandate to purchase insurance and
the creation of a new program, Commonwealth Care, which provides heavily subsidized
insurance for those below 300 percent of the poverty line. In addition, a new marketplace for
non-group insurance, the Connector, was created to facilitate purchase for those who did not
have access to employer-sponsored insurance.2 The Massachusetts reform did not include much
of what is incorporated into the ACA, in particular the revenue sources — reform in
Massachusetts was financed jointly by the federal government and by an existing tax that
financed care for the uninsured — and the efforts at cost control discussed above. But it does
2
For more information on the Connector and Massachusetts health reform in general, see
www.mahealthconnector.org.
8 provide an excellent case study of the three-legged stool approach to covering the uninsured and
fixing the non-group market.
B. Results
The results of the Massachusetts reform have been encouraging along a number of
dimensions.3 First, there has been a dramatic expansion of health insurance coverage in the state.
The data vary across sources, with state-level data from the Current Population Survey (CPS)
showing a 60 percent decline in the uninsured since 2006 — over a period of time where the
share of the national population without insurance was rising by 6 percent — and data collected
by the state’s Division of Health Care Finance and Policy showing a decline of 70 percent.4
Either number indicates a sizeable reduction in the number of uninsured, with Massachusetts
having by far the lowest uninsurance rate in the nation.
A major concern with such a large expansion in access to care is that it will cause
congestion on the supply side of the market. Indeed, many have argued that we have a chronic
shortage of primary care physicians in the United States and that expanding coverage will only
worsen that shortage. This has not been the case in Massachusetts, however. A recent study by
the Massachusetts Medical Society found that average wait times for both family and internal
medicine were basically flat in the period since the law passed (Massachusetts Medical Society,
2011).
Moreover, this expansion in insurance coverage has been associated with a rise in access
to care. The share of the population with a usual source of care, the share with a doctor’s visit in
3
This section draws heavily on and updates Gruber (2011a).
The former figure comes from data tabulations from the U.S. Census Bureau, Current
Population Survey, www.census.gov; the latter figure comes from the state’s Division of Health
Care Finance and Policy, Health Care in Massachusetts: Key Indicators,
http://www.mass.gov/Eeohhs2/docs/dhcfp/r/pubs/10/key_indicators_november_2010.pdf.
4
9 the last 12 months, the share receiving preventive care, and the share receiving dental care all
rose significantly from the fall of 2006 to the fall of 2008 (Long and Masi, 2009). Miller (2011)
finds a modest reduction in the rate of utilization of emergency care in the state, while the
Division of Health Care Finance and Policy (2009) reports a 40% decline in uncompensated care
in the first year after reform
Second, rather than a crowd-out of private insurance through the expansion of a publicly
funded entitlement, there has been a “crowd-in” through a rapidly rising rate of employer-insured
individuals. According to estimates from the Current Population Survey, the share of the
Massachusetts population with employer-sponsored insurance rose by 0.6 percent from 2006–
2009, while over the same period the share of the national population with employer-sponsored
insurance fell by 4 percent. Some of this “crowd-in” is due to increased enrollment in employersponsored insurance by those endeavoring to meet the requirements of the mandate, but some
has actually been through higher rates of employer insurance offering. The rate of employerprovided insurance offering in Massachusetts rose from 70 percent in 2005 to 76 percent in 2009,
while it remained flat at 60 percent nationally (Massachusetts Division of Health Care Financing
and Policy, 2010). There is no obvious explanation for this increase in employer offering as the
law introduces incentives for employers to drop insurance (by covering their low income
employees outside the employer setting) and does little to penalize those firms that do drop
coverage. The best potential explanation for this result is that there was a non-market impact of
the mandate on employer behavior, with employees demanding coverage to meet the mandate
and employers increasing coverage to meet the demand.
Fourth, the mandate implementation has been very smooth. Over 98 percent of tax filers
required to file health insurance information with their tax returns have complied with the filing
10 requirement. Out of the at least 500,000 individuals who were uninsured before reform, only
53,000 ended up being assessed penalties for not having insurance in 2008 (the remainder either
having gained insurance or were exempt from penalties) (Massachusetts Department of Revenue,
2009). Only 2,500 of those individuals filed and followed through on appeals of their penalty;
the penalty was waived in about three quarters of the cases.5
Fifth, the costs of administering health reform have been quite low. The Connector was
given only $25 million in seed funding, and its net worth remains at $20 million. The ongoing
administrative costs are funded by an insurance charge of only 3 percent, which is very small
compared to the typical loads found in the non-group and small group markets.6
Sixth, the reform has generally been popular. Sixty-nine percent of state residents
supported reform in 2006, and that number has remained essentially unchanged, with 67%
support in 2009 (Long and Stockley, 2009).
Seventh, premiums have fallen dramatically in the non-group market. According to
America’s Health Insurance Plans (2007, 2009), from 2006–2009 non-group premiums rose by
14 percent nationally; over that same period, they fell by 40 percent in Massachusetts. Some of
that decline was due to a redution in the level of non-group benefits, but this is a sizeable decline
in any case.
Eighth, there has been no meaningful impact on employer-sponsored insurance
premiums. Cogan, Hubbard, and Kessler (2010) argue that group premiums rose in
Massachusetts from 2006–2008. Using state-level data from the Medical Expenditure Panel
Insurance Component, they show that over this period single group premiums rose by 8.7 percent
in Massachusetts, but only 6.5 percent nationally, for a 2.2 percent excess growth rate in
5
6
This figure is based on private communication with Connector staff.
This figure is based on private communication with Connector staff.
11 Massachusetts; for families, premiums grew by 12.2 percent in Massachusetts but only 8.1
percent nationally, for a 4.1 percent excess growth rate.
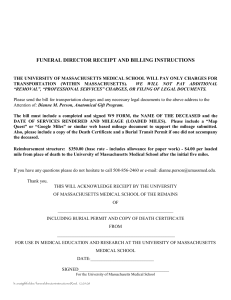
But these tabulations are very imprecise due to the very noisy nature of premium
movements over time at the state level. Over the 2006–2008 period, the standard deviation of the
state premium change was 4.6 percent for single premiums and 5.3 percent for family premiums.
This implies that the changes documented by this article are not statistically meaningful in that
they are well below a one standard deviation change in premiums. To illustrate this point further,
consider Figure 1, which shows the change in single premiums from 2006–2008 by state,
graphed against the state rankings of premium change. Massachusetts is ranked 31st, which is
somewhat higher than the median, but clearly not distinguishable from states around it. The
change in premiums for Massachusetts, for example, is well below that of other neighboring
New England states such as Vermont (ranked 46) or New Hampshire (ranked 47).7
Finally, the costs of reform at full implementation have been very close to original
projections. Legislative staff in 2006 projected that the Commonwealth Care program would cost
$750 million when fully implemented. In FY 2009, the first full year of implementation, costs
were $800 million. The Massachusetts Taxpayers Foundation (2009) undertook a comprehensive
study of the net cost of reform, taking into account the costs of Commonwealth Care and Mass
Health expansions, as well as savings through uncompensated care and supplemental payments
to safety net hospitals. The study concluded that the net cost of reform in the state has been $707
million, roughly half of which is borne by the federal government. Given that the state has newly
insured about 300,000 individuals according to survey evidence, that is a cost to the state of only
$2,350 per newly insured. This is a very low cost per newly insured compared to earlier
7
Note that the change in uninsurance rate and non-group premiums are both highly significant
relative to other states over this time period.
12 estimates of the cost of alternative approaches to expanding insurance coverage (Gruber, 2008).
This largely reflects the fact that so much of the increase in insurance coverage has been through
private coverage.
IV. IMPLICATIONS FOR THE ACA
The projections of the impacts of the ACA from CBO (2010b) are summarized in Table
2. The top panel shows projected impacts on coverage. CBO projects that there will be a very
modest erosion of employer-sponsored insurance, with large increases in both public insurance
and non-group insurance, so that there is an overall reduction in the number of uninsured of 32
million people. They also project about $940 billion in new spending, offset with $1,080 billion
in spending reductions and revenue increases, for a first decade deficit reduction of about $140
billion. Moreover, in their discussion of the bill, CBO notes that they project the deficit reduction
to increase over time, and reach more than $1 trillion in the second decade.
A. Population Movements
Perhaps the most surprising aspect of the CBO estimates is the rather modest erosion of
employer-sponsored insurance that they project. But, in fact, this estimate is consistent with past
evidence as well as with the experience of Massachusetts.
This small erosion occurs for several reasons. First, more than half of employees covered
by health insurance are in firms with more than 100 employees, and past evidence suggests that
such firms are not price sensitive in their decisions to offer insurance (Gruber and Lettau, 2004).
Second, the subsidies under the ACA are not very generous above about 250 percent of
the poverty line, so that for most firms the majority of workers will not see substantially better
deals outside of the employment setting rather than inside. To illustrate this point, I draw on the
Gruber Microsimulation Model (GMSIM), a large-scale econometric simulation model that I
13 have developed over the past dozen years to model health care reforms. To the extent that CBO
has made details of their model public, in many ways the GMSIM mirrors the CBO approach to
modeling health reform.8
To model firm behavior in such microsimulation models, it is important to understand
that firms make decisions based on the firm-wide aggregate effects of a policy. To mimic this in
GMSIM, we construct “synthetic firms” that are meant to reflect the demographics of actual
firms. The core of this computation comes from U.S. Bureau of Labor Statistics (BLS) data
providing the earnings distribution of co-workers for individuals of any given earnings level, for
various firm sizes and regions of the country. Using these data, the model randomly selects
individuals in the same firm size/region/health insurance offering cell as a given CPS worker in
order to statistically replicate the earnings distribution that the BLS data would predict for that
worker. These workers then become the co-workers in a worker’s synthetic firm.
Using these synthetic firms, we can look at the composition of firms below 100
employees to assess the extent to which low-income workers are concentrated in such firms. In
fact, we find that only one-quarter of small firms have more than 10 percent of their employees
in families with incomes of less than 133 percent of the poverty line, and virtually none have
more than 50 percent of their employees with incomes less than that amount. Only 21 percent of
firms have more than 10 percent of their employees in families with incomes of 133–250 percent
of the poverty line, and once again virtually no firms have more than half of their employees
earning in that range.
Third, this modest effect may be offset if the Massachusetts experience, where the
individual mandate appears to have led more firms to offer insurance, is repeated at the national
8
A detailed appendix that describes GMSIM is available at MIT Department of Economics,
“Documentation for the Gruber Microsimulation Model,” http://econ-www.mit.edu/files/5939.
14 level. It is unclear how large this effect will be relative to the case of Massachusetts, as federal
subsidies to non-group insurance are much less generous, although they do extend to four times
(rather than three times) the poverty line.
Fourth, there is an offsetting increase in ESI enrollment due to the mandate. A large share
of the uninsured (perhaps one-quarter) are offered and eligible for ESI but do not enroll. These
individuals will now enroll in large numbers due to the mandate.
Finally, an additional offset will be any pressure on firms to offer insurance due to the
“free rider” penalty in the ACA. This section of the ACA charges firms of more than 50
employees a large $2,000–$3,000 charge if their employees receive subsidies on the health
insurance exchange.9 This provides a strong countervailing financial incentive to firms to offer
insurance. The Massachusetts reform featured a much more modest ($300) charge.
With only a modest reduction in ESI, and an enormous expansion of public and
subsidized private insurance, CBO (2010b) projects that 32 million uninsured will gain coverage
by 2019, relative to a pre-law baseline estimate of 55 million uninsured. This estimate of a 58
percent reduction in the uninsured is somewhat lower than the reduction in Massachusetts, but
this is partly because the ACA does not provide subsidies or public insurance to undocumented
immigrants, who make up almost one-quarter of the uninsured nationally but much less than that
in Massachusetts.
B. Premium Impacts
9
In particular, if any employee joins the exchange and receives tax credits and the firm does not
offer insurance, the firm must pay $2,000 per employee (minus a 30 employee “exemption”). If
the firm offers insurance, but an employee still ends up getting tax credits in the exchange
(which can happen if the employee’s insurance contribution exceeds 9.5 percent of their
income), then the firm owes $3,000 per employee who gets tax credits.
15 CBO (2009) provided estimates of the impact of the ACA on health insurance premiums
in the non-group and employer markets. For the non-group market, CBO compares premiums in
the state-based health insurance exchanges to premiums that would exist in the non-group market
absent reform, which they compute by projecting current non-group premiums forward. Their
headline estimate is that exchange premiums will be 10–13 percent higher, on average, with
reform than in the non-group market absent reform — although for any family below 400
percent of poverty this cost could be partially offset by tax credits. As they discuss, however, this
result reflects the net impact of three effects. First, premiums will drop 7–10 percent due to an
improved health mix in that market (due to the mandate). Second, premiums will drop another 7–
10 percent due to lower prices arising from enhanced competition and other factors in the nongroup market. Finally, premiums would rise by 27–30 percent due to individuals buying more
generous policies in the exchange than they do in today’s non-group market.
Therefore, CBO estimates imply that for a given level of policy generosity in the
exchange, premiums would actually fall by 14–20 percent. This is consistent with the findings of
declines in non-group premium in Massachusetts. Thus, the overall rise occurs because
individuals buy more generous policies than the limited policies purchased in the non-group
market today. CBO (2009) does not discuss the key question of why these more generous
policies are purchased — that is, to what extent is this due to voluntary upgrades versus forced
“buying up” to meet the new minimum standards in this market? Given that the minimum
standards are fairly modest, however, it seems likely that most of the increase in plan quality
reflects voluntary upgrades.
The CBO estimates show essentially no change in group premiums: for small groups,
they estimate a range from a reduction of 2 percent to an increase of 1 percent; for large groups,
16 they estimate a range from a reduction of 3 percent to no effect. This is once again consistent
with the evidence from Massachusetts, which showed no significant impact on group premiums.
C. Budgetary Implications
CBO (2010b) estimates that the ACA subsidies and public insurance expansion will cost
$940 billion by 2019. In 2019, CBO estimates that the government will spend $214 billion to
cover 32 million people, or $6,690 per person. Deflating at 6 percent per year, health care
premium inflation to 2009 yields a cost of $3,730 per person. This is about 50 percent higher
than the cost of $2,350 per person newly covered in Massachusetts, which is plausible since
incomes are lower nationally than in Massachusetts. So once again CBO’s estimates are
consistent with — or perhaps a bit more conservative than — what was observed in
Massachusetts.
CBO also estimates that the revenue increases and spending cuts will exceed the new
level of spending, reducing the federal deficit by more than $100 billion in the first decade and
more than $1 trillion in the second decade. In the first decade alone this would be the most
fiscally responsible legislation passed by Congress since 1997.
Some have questioned the likelihood of this deficit reduction — claiming, for example,
that the numbers are “cooked” because some of the revenue raisers begin before 2014, whereas
the majority of spending doesn’t start until after 2014. But CBO estimates that the trend under
the law will actually be toward larger deficit reduction over time; indeed, the reduction in the
deficit is increasing in the last two years of the budget window. Thus, the cuts in spending and
increases in taxes are actually back-loaded — not front-loaded, as these critics imply.
Others have raised the possibility that the cuts that provide much of this financing will
never take place — and point to the experience with the physician-payment cuts required by the
17 Balanced Budget Act of 1997, which have been repeatedly delayed by Congress. As Van de
Water and Horney (2010) have highlighted, however, Congress has passed many Medicare cuts
over the past 20 years, and the physician-payment cut is the only one that has not taken effect.
That said, the fiscal responsibility promised by this legislation does depend on the ability of
future Congresses to hold to the reimbursement reductions and tax increases laid out in the ACA.
D. Health Care Costs
The best available projections of the impact of the ACA on the level and growth of health
care costs in the near term come from the Center for Medicaid and Medicare Services Office of
the Actuary (CMS). 10 With U.S. health care spending already accounting for 17 percent of GDP
and growing, there is also concern about policies that increase this spending. And, as the CMS
actuary points out, the ACA will increase national health care expenditures. At the peak of its
effect on spending in 2016, the law will increase health care expenditures by about 2 percent; by
2019, the ACA-related increase will be 1 percent, or 0.2 percent of GDP.
It is worth noting that these increases are quite small relative to the gains in coverage
under the new law. The CMS predicts that 34 million more people will be insured by 2019
(which is similar to the independent estimate of CBO) relative to a base of 254 million insured.
The agency also estimates that without this reform, health care costs would grow by 6.6 percent
per year between 2010–2019. So the ACA will be increasing the ranks of the insured by more
than 13 percent at a cost that is less than one sixth of one year’s growth in national health care
expenditures.
Alternatively, consider the fact that under this legislation, by 2019, the United States will
be spending $46 billion more on medical care than we do today. In 2010 dollars, this amount to
10
The discussion in this section draws on Gruber (2010).
18 only $800 per newly insured person, quite a low cost compared, for example, to the $5,050
average single premium for employer-sponsored insurance (Kaiser Family Foundation, 2010).
U.S. spending on health care is very high and a source of great concern, but it is the
growth rate of medical spending, not its level, that ultimately determines our country’s financial
well-being. If current trends persist, we will be spending an unsustainable 40 percent of our GDP
on health care by 2080, as the growth of health care costs continues to outstrip the growth rate of
the overall economy. In this environment, whether health care costs rise or fall by 1 percent or
even 5 percent is irrelevant — all we do is move the day of reckoning less than 1 year closer or
further away. Clearly, the key to the long-term viability of our health care system is to “bend the
cost curve.”
On this count, the CMS actuary’s news is (slightly) good: although the ACA will boost
medical spending somewhat, its incremental impact on spending will decrease over time (as
noted above, from 2 percent in 2016 to 1 percent in 2019). These declining estimates imply that
by the second decade the ACA will actually lower national health spending. This is due to
provisions such as the Cadillac tax, for which the definition of a high-cost plan is indexed to the
growth in overall prices in the economy, not the (projected to be higher) growth in health
insurance premiums. As a result, an increasing proportion of plans will be taxed, and more
people will shift into lower-cost insurance options in order to avoid paying the tax, lowering
national health expenditures.
19 V. CONCLUSION
The ACA is a transformative piece of legislation that, if fully implemented, will reshape
the U.S. health care system for decades to come. As such, it is very difficult to accurately predict
its impacts. In this article, I have reviewed the basis for the projections that do exist,
particularly based on the experience of Massachusetts with a similar program.
The real question is how far the ACA will go in slowing cost growth. Here, there is great
uncertainty—mostly because there is such uncertainty in general about how to control cost
growth in health care. There is no shortage of good ideas for ways of doing so, ranging from
reducing consumer demand for health care services, to reducing payments to health care
providers, to reorganizing the payment for and delivery of care, to promoting cost-effectiveness
standards in care delivery, to reducing pressure from the threat of medical malpractice claims.
There is, however, a shortage of evidence regarding which approaches will actually work—and
therefore no consensus on which path is best to follow.
In the face of such uncertainty, the ACA pursued the path of considering a range of
different approaches to controlling health care costs, from those that work on the demand side
(the Cadillac tax), to those that work on the supply side (innovative provider payment models),
and to those that promote the type of evidence-based medicine that is key to ensuring cost
effectiveness. Whether these policies by themselves can fully solve the long run health care cost
problem in the United States is doubtful. They may, however, provide a first step towards
controlling costs—and understanding what does and does not work to do so more broadly.
20 REFERENCES
America’s Health Insurance Plans, 2007. “Individual Health Insurance 2006–2007: A
Comprehensive Survey of Premiums, Availability and Benefits.” America’s Health Insurance
Plans, Washington, DC,
http://www.ahipresearch.org/pdfs/Individual_Market_Survey_December_2007.pdf.
America’s Health Insurance Plans, 2009. “Individual Health Insurance 2009: A Comprehensive
Survey of Premiums, Availability and Benefits.” America’s Health Insurance Plans, Washington,
DC, http://www.ahipresearch.org/pdfs/2009IndividualMarketSurveyFinalReport.pdf.
Cogan, John F., R. Glenn Hubbard, and Daniel Kessler, 2010. “The Effect of Massachusetts’
Health Reform on Employer-Sponsored Insurance Premiums.” Forum for Health Economics and
Policy 13 (2), Article 5.
Congressional Budget Office, 2009. “An Analysis of Health Insurance Premiums Under the
Patient Protection and Affordable Care Act.” Letter to the Honorable Evan Bayh (November 30).
Congressional Budget Office, Washington, DC, http://www.cbo.gov/doc.cfm?index=10781.
Congressional Budget Office, 2010a. The Long-Term Budget Outlook. Congressional Budget
Office, Washington, DC.
Congressional Budget Office, 2010b. “H.R. 4872, Reconciliation Act of 2010.” Letter to the
Honorable Nancy Pelosi (March 18). Congressional Budget Office, Washington, DC,
http://www.cbo.gov/ftpdocs/113xx/doc11355/hr4872.pdf.
Fronstin, Paul, 2010. “Sources of Health Insurance and Characteristics of the Uninsured:
Analysis of the March 2010 Current Population Survey.” Issue Brief No. 347. Employee
Benefits Research Institute, Washington, DC, http://www.ebri.org/pdf/briefspdf/EBRI_IB_092010_No347_Uninsured1.pdf.
Gruber, Jonathan, 2002. “Taxes and Health Insurance.” In Poterba, James M., (ed.), Tax Policy
and the Economy, Volume 16, 37–66. National Bureau of Economic Research, Cambridge, MA.
Gruber, Jonathan, 2008. “Covering the Uninsured in the United States.” Journal of Economic
Literature 46 (3), 571–606.
Gruber, Jonathan, 2010. “The Cost Implications of Health Care Reform.” New England Journal
of Medicine 362 (22), 2050–2051.
Gruber, Jonathan, 2011a. “Massachusetts Points the Way to Successful Health Care Reform.”
Journal of Policy Analysis and Management 30 (1), 184–192.
Gruber, Jonathan, 2011b. “The Tax Exclusion for Employer-Sponsored Health Insurance.”
21 National Tax Journal 64 (2), 511–530.
Gruber, Jonathan, and Micheal Lettau, 2004. “How Elastic Is The Firm’s Demand For
Health Insurance?” Journal of Public Economics 88 (7–8), 1273–1293.
Kaiser Family Foundation, 2010. “Employer Health Benefits: 2010.” Kaiser Family Foundation,
Menlo Park, CA, http://ehbs.kff.org/pdf/2010/8085.pdf.
Long, Sharon K., and Paul B. Masi, 2009. “Access and Affordability: An Update on Health
Reform in Massachusetts.” Health Affairs 28 (4), 578–587.
Long, Sharon K. and Karen Stockley, 2010. “Health Reform in Massachusetts: An Update As of
Fall 2009”. Urban Institute: June, 2010.
Massachusetts Department of Revenue, 2009. “Individual Mandate 2008 Preliminary Data
Analysis.” Massachusetts Department of Revenue, Boston MA,
http://www.mass.gov/Ador/docs/dor/News/PressReleases/2009/2008_Health_Care_Report.pdf.
Massachusetts Division of Health Care Finance and Policy, 2010. “Results from the 2009
Massachusetts Employer Survey.” Massachusetts Division of Health Care Financing and Policy,
Boston, MA, http://archives.lib.state.ma.us/bitstream/handle/2452/46958/ocn5495636292009.pdf?sequence=1.
Massachusetts Division of Health Care Finance and Policy, 2009. “Health Care In
Massachusetts: Key Indicators,” Massachusetts Division of Health Care Financing and Policy,
Boston, MA, http://www.mass.gov/Eeohhs2/docs/dhcfp/r/pubs/09/key_indicators_nov_09.pdf
Massachusetts Medical Society, 2011. 2011 Patient Access to Health Care Study, Massachusetts
Medical Society, Waltham, MA,
http://www.massmed.org/AM/Template.cfm?Section=Contacts_and_Directions&CONTENTID
=54336&TEMPLATE=/CM/ContentDisplay.cfm.
Massachusetts Taxpayers Foundation, 2009. “Massachusetts Health Reform: The Myth of
Uncontrolled Costs.” Massachusetts Taxpayers Foundation, Boston, MA, http://www.masstaxpayers.org/publications/health_care/20090501/massachusetts_health_reform
_the_myth_uncontrollable_costs.
Miller, Sarah, 2011. “The Effect of Insurance on Outpatient Emergency Room Visits: An
Analysis of the 2006 Massachusetts Health Reform.” Unpublished manuscript. University of
Illinois, Urbana-Champaign, IL.
U.S. Census Bureau, 2010. “Income, Poverty and Health Insurance Coverage in the United
States, 2009.” Current Population Report P60–238. U.S. Census Bureau, Washington, DC.
22 Van de Water, Paul N., and James R. Horney, 2010. “Health Reform Will Reduce the Deficit.”
Center on Budget and Policy Priorities, Washington, DC,
http://www.cbpp.org/cms/index.cfm?fa=view&id=3134.
23 Table 1
Sources of Health Insurance Coverage in the United States, 2009
Total Population
Private
Public
Employment-based
Direct purchase
Medicare
Medicaid
Uninsured
Source: Fronstin (2010).
People (millions)
304.3
Percentage of Population
100
194.5
169.7
27.2
93.2
43.4
47.8
50.6
63.9
55.8
8.9
30.6
14.3
15.7
16.7
24 Table 2
CBO Estimates of the Impact of the ACA
Uninsured
Employer
Non-group & other
Exchange
Medicaid
Coverage Provisions
Medicaid
Exchange Subsidies
Small Employer Tax
Credits
Gross Coverage Costs
Offsets
Spending Reductions
Revenue Increases
Gross Offsets
Population Effects in 2019 ($Million)
Baseline (No ACA)
54
162
30
0
35
Budget Effects ($Billion)
2019
Effect of the ACA
–32
–3
–5
24
16
2010–2019
97
113
4
434
464
40
214
938
–117
–108
–225
514
562
1076
Net Budgetary Impact
–15
–143
Notes: Subcomponents do not add to totals due to rounding and other small differences in
definitions.The difference between net budgetary impact and spending minus revenues is due to
these issues as well as other non-coverage provisions.
Source: CBO (2010b).
25 Figure 1
Percentage Change in Premiums against State Rank, 2006–2008
% Change in Premium, 2006-08
.166116
-.015421
1
31
Ranking by Premium Change
26 51