Document 10436755
advertisement

/""l
ACORD®
OAlE(MM~
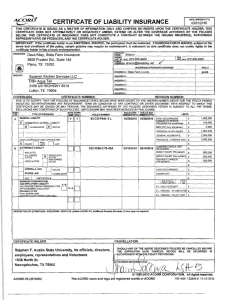
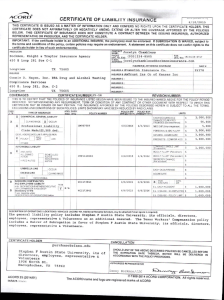
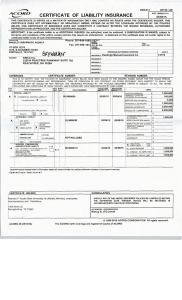
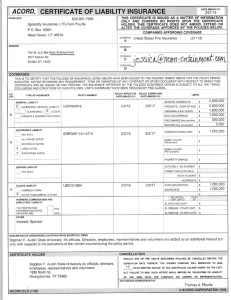
CERTIFICATE OF LIABILITY INSURANCE
02/09/2016
THIS CERTIFICATE IS ISSUED AS A MATTER OF INFORMATION ONLY AND CONFERS NO RIGHTS UPON THE CERTIFICATE HOLDER. 'THIS
CERTIFICATE DOES NOT AFFIRMATIVELY OR NEGATIVELY AMEND, EXTEND OR ALTER THE COVERAGE AFFORDED BY THE POLICIES
BELOW. THIS CERTIFICATE OF INSURANCE DOES NOT CONSTITUTE A CONTRACT BETWEEN THE ISSUING INSURER(S), AUTHORIZED
REPRESENTATIVE OR PRODUCER, AND .THE CERTIFICATE HOLDER.
IMPORTANT: H the cenlflcate holder Is an ADDITIONAL INSURED, the pollcy(ies) must be endorsed. If SUBROGATION IS WAIVED, subject to
the tenns and conditions of the policy, certain policies may require an endorsement A statement on this certificate does not confer rights to the
certificate holder In lleu of such endorsement(s •
PRODUCER
TWFG - Steve Eitelman
Ffk No ; (903) 660-2103
P.O. Box 1137
NAICI
Hallsville
TX 75650
INSURED
INSURER& :
VISUAL TECHNIQUES
INSURERC :
2200 JAHAN TRAIL
INSU~RD :
INSURERE :
TX
LONGVIEW
COVERAGES
75604
INSURERF ·
CERTIFICATE NUMBER:
REVISION NUMBER:
THIS IS TO CERTIFY THAT THE POLICIES OF INSURANCE LISTED BELOW HAVE BEEN ISSUED TO THE INSURED NAMED ABOVE FOR THE POLICY PERIOD
INDICATED. NOTWITHSTANDING ANY REQUIREMENT, TERM OR CONDITION OF A~ CONTRACT OR OTHER DOCUMENT WITH RESPECT TO WHICH THIS
CERTIFICATE MAY BE ISSUED OR MAY PERTAIN, THE INSURANCE AFFORDED BY THE POLICIES DESCRIBED HEREIN IS SUBJECT TO ALL THE TERMS,
EXCLUSIONS AND CONDITIONS OF SUCH POLICIES. LIM ITS SHOWN MAY HAVE BEEN REDUCED BY PAID CLAIMS.
INSR
LTR
TYPE OF INSURANCE
x
...__
A
-
COMMERCIAL GENERAL UABILilY
D
=i
""""
CLAIMS-MADE
0
..···-
POLICY NUMBER
· .~s~gv~ (=~
OCCUR
06/0112015
06/01/2016
POLICY DPRO·
JECT
D
LOC
-x
r-
s
s
ANYAlfTO
ALLOWNEO
AlJTOS
HIREOAUTOS
1,000,000
50,000
5,000
GENERAL AGGREGATE
s 2,000,000
s 2,000,000
PRODUCTS · COMP/OP AGG
s
PERSONAL &ADV INJURY
2,000,000
$
OTHER:
AUTOMOBILE LIABILllY
A
$
g~~~~~<?"';!""'cu
MED EXP (Any one D«>On)
BOP 3551673
GEN'!. AGGREGATE LIMIT APPLIES PER:
-
LIMITS
EACH OCCURRENCE
X
X
-
~6~LEO
BA 1057243
Oe/1212015
06/1212016
;;,~"""'" :siNGLE Ur.II I
$ 1,000,000
BODILY INJURY (Per person)
s
BOOllY INJURY (Per acclc!enQ $
f.,R_~.;::,,~AMAGE
NON-OWNED
AlJTOS
$
$
UMBRELLA LIAB
f--
EXCESSLIAB
EACH OCCURRENCE
HOCCUR
CLAIMS.MADE
AGGREGATE
I I
RETENTION $
CEO
WORKERS COMPENSATION
AND !MPLOYERS' LIABILITY
ANV PROPRIETOR/PARTNER/EXECUTIVE
OFFICERR.ICMBER EXCLUDED?
(Mandatory In NH)
•s
$
YIN
D
NIA
gr~~= ~~~ERATIONS baow
::Xe A++tihJ~
r'%
I ~¥frnTE I
12~
E.l. EACHACCIDEHT
s
E.L DISEASE - EA EMPLOYEE S
E.L DISEASE - POUCY UMrT
$
DESCRIPTION OF OPERATIONS I LOCATIONS I Vl!HICLES (ACORO 101, Additional Remarks 8<Jhedule, m1y b• allaehod If more space lo required)
CANCELLATION
CERTIFICATE HOLDER
SHOULD ANY OF THE ABOVE DES~RIBED POLICIES BE CANCELLED BEFORE
THE EXPIRATION DATE THEREOF, NOTICE WILL BE DELIVERED IN
ACCORDANCE WITH THE POLICY PROVISIONS.
Stephen F. Austin Slate University
Its officials, directors, employees, representatives and Volunteers.
1936 North St
Nacogdoches
TX
A;r;z;~ATWE
75962
1
© 1988-2014 ACORD CORPORATION. All rights reserved.
ACORD 25 {2014101)
The ACORD name and logo are registered marks of ACORD
ixasMurual
WORKERS' COMPENSATION ANO
00
EMPLOYERS LIABILITY INSURANCE POLICY
Insunncc Ccinpany .
6210 EHighway 290
Austin, Texas 78723-1098
ITEM1
INFORMATION PAGE
VISUAL TECHNIQUES INC
2200 JAHAN TRl:
LONGVIEW, TX 75604-2521
POLICY NUMBER
SBP-0001280906 20151231
INSURED
NAMEAND ·
ADDRESS
Federal Tax ID
OTHER WORKPLACES NOT SHOWN ABOVE:
see attached schedule of operation .
PROOUCER
42092
Bureau Number
Branch
Renewal of
Entity ;
Interim Adjustment
Group
NCCI ca·r rler Code
CLIFFORD STEPHEN .EI TELMAN
PO BOX 1137
. HALLSVILLE, .TX 75650-1137
ITEM 2
The Policy Period is from: 12-31-2015
ITEM3
A.
B.
{ To: 12-31-2016 /
75-1772311
DAL LAS
0001280905
CORPORAT I ON
29939
12:01 A.M. standard time at the lnsured's·malllng address
Workers' Compensation Insurance: Part <3°"'::;- • •• ooli"v .aJles to the Workers' Compensation Law of the
states listed here: TEXAS
. Employers Liability Insurance: Part Two of the policy applies to work In each state listed In Item 3A.
The Limits of.our Liability under Part Two are:
Bodily Injury by Accident
Bodily Injury by Disease
Bodily Injury by Disease
$
$
$
1 ,000 ,000
Each Accident
1 ,000 ,000
Each Employee
1 ,000 ,000
Polley Limit
C.
Other States Insurance: Part Three o! the policy applies to the states, If any, listed here: NONE
D.
This policy includes these endorsements and schedules:
See Schedule of Endorsements attached
ITEM 4
The premium for this policy will be determined by our manuals of Rules, Classifications, Rates and Rating Plans.
All information required below is subject to verification and change by audit.
:
TOTAL ESTIMATED STANDARD PREMIUM
:$
3,609.00
WAIVER OF SUBROGATION
,
INCREASED EMPLOYERS LIABILITY LIMITS
••
'
,
TOTAL PREMIUM SUBJECT TO MODIFICATIONS
PREMIUM MODIFIED TO REFLECT PREM INCENTIVE OF (
,85 )
.• 96 . )
PREMIUM MODIFIED TO REFLECT SCHEDULE RATING OF (
WORKERS' · COMP HEAL TH CARE NETWORK DISCOUNT ( '
• 12
)
DEDUCTIBLE PREM I UM • •
,
,
ADM·IRALTY/FELA OR L & HW
,
PREMIUM DISCOUNT, IF APPLICABLE (
EXPENSE CONSTANT CHARGE
, • •
.
TOTAL ESTIMATED ANNUAL PREMIUM
MINIMUM PREMIUM
260.00
DEPOSIT PREMiUM
2 , 849.00
Issue Date:
:
:$
Countersigned by .
120.00-
368.00-
.oo
.oo
.oo
150 . 00
2,849.00
(lvL.J2. .,.,.CJ
A-..~
~ ..... •
1-07-201.6
f.ncludes copyright materiarofthe National Counctl on Compfi!nsation Insurance, Inc. used with Its permission
©Copyright 2015 National Councll of Compensation lnsurace, Inc. All rights reserved.
WC000001B (ED . 1-1-2015)
.00
160.00
3,759.00
564.00-
.
. ..
..
..
..