Document 10436657
advertisement

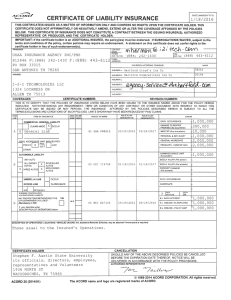
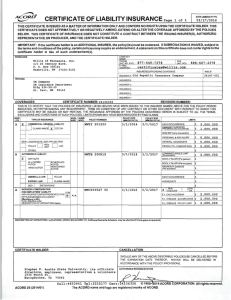
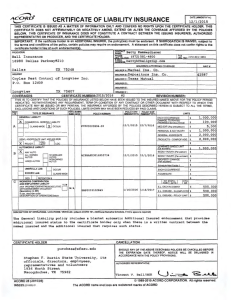
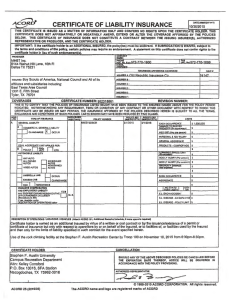
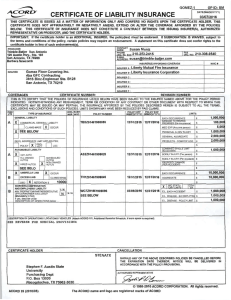
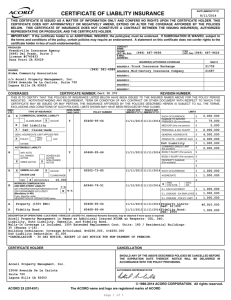
ACOffD~ DATE (MM/00/YYYY) CERTIFICATE OF LIABILITY INSURANCE I 12/8/2015 ~ THIS CERTIFICATE IS ISSUED AS A MATTER OF INFORMATION ONLY AND CONFERS NO RIGHTS UPON THE CERTIFICATE HOLDER. THIS CERTIFICATE DOES NOT AFFIRMATIVELY OR NEGATIVELY AMEND, EXTEND OR ALTER THE COVERAGE AFFORDED BY THE POLICIES BELOW. THIS CERTIFICATE OF INSURANCE DOES NOT CONSTITUTE A CONTRACT BETWEEN THE ISSUING INSURER(S), AUTHORIZED REPRESENTATIVE OR PRODUCER, AND THE CERTIFICATE HOLDER. IMPORTANT: If the certificate holder Is an ADDITIONAL INSURED, the policy(ies) must be endorsed. If SUBROGATION IS WAIVED, subject to the terms and conditions of the policy, certain policies may require an endorsement. A statement on this certificate does not confer rights to the certificate holder in lieu of such endorsement(s). CONTACT NAME : PRODUCER Watkins Insurance Group-Austin fA~gN:o 3834 Spicewood Springs Rd, St Austin TX 78759 Tiffany Arvie Eit•· I ff.~ 512-452-8877 >Jn• · 512-452-0999 JDM0AJ~ss:~ a~i e@watkinsinsurancegrou p . com INSURERISI AFFORDING COVERAGE NAIC # 10677 INSURER A : Cinci nnati Insurance Company INSURED JELC0-1 INSURER B : Jelco .. INSURER C : Jared Jellison PO Box IN SURER 0 : 151085 78715 INSURER E : Austin TX INSURER F : CERTIFICATE NUMBER· 1647805823 COVERAGES REVISION NUMBER· THIS IS TO CERTIFY THAT THE POLICIES OF INSURANCE LISTED BELOW HAVE BEEN ISSUED TO THE INSURED NAMED ABOVE FOR THE POLICY PERIOD INDICATED. NOTVVITHSTANDING ANY REQUIREMENT, TERM OR CONDITION OF ANY CONTRACT OR OTHER DOCUMENT \l\llTH RESPECT TO VVHICH THIS CERTIFICATE MAY BE ISSUED OR MAY PERTAIN , THE INSURANCE AFFORDED BY THE POLICIES DESCRIBED HEREIN IS SUBJECT TO ALL THE TERMS , EXCLUSIONS AND CONDITIO NS OF SUCH POLICIES. LIMITS SHOWN MAY HAVE BEEN REDUCED BY PAID CLAIMS . INSR LTR A "UUL TYPE OF INSU RANCE x r-- INSO "UB" wvo D CLAIMS-MADE POLICY EFF POLICY EXP IMM/00/YYYYI IMM/00/YYYYI POLICY NUMBER EPP 0171044 COMMERCIAL GENERAL LIABILITY w 12/5/2015 12/5/2016 OCCUR r-r-GEN'L AGGREGATE LIMIT APPLIES PER: Fl A POLICY 0 PROJECT D LOC 12/5/2015 EBA0171044 12/5/201 6 x f-- r-- A x ·- ALL OVVN ED AUTOS ~ t-- HIRED AUTOS t-- UMBRELLA LIAB EXCESS LIAB SCHEDULED AUTOS NON-OVVNED AUTOS MED EXP (An y one person) $10,000 PERSONAL & ADV INJURY $1 ,000,000 GENERAL AGGREGATE $2 ,000,000 PRODUCTS - COMP/OP AGG $2,000,000 $ 1,,vrvlBINt:U SINGLt: LIM\ 1 BODILY INJURY (Per person) s1 ,ooo .ooo $ BODILY INJURY (Per accident) $ r"vrio':' I Y utvV1A<.;t: (Per accid ent) $ I Ea accident! $ M 12/5/2015 EPP 0171044 OCCUR 12/5/2016 EACH OCCURRENCE AGGREGATE CLAIMS-MADE Ix I OED RETENTION $10,000 WORKERS COMPENSATION ANO EMPLOYERS' LIABILITY ANY PROPRIETOR/PARTNER/EXECUTIVE OFFICER/MEMBER EXCLUDED? (Mandatory In NH) YI N D N/A I PER I I OTH STATUTE ER Se.e ~~ o/~3/t 7 ~m::~~~fi~ '01oPERATIONS below A A $1 ,000,000 $300,000 OTHER: AUTOMOBILE LIABILITY r-ANY AUTO ,_ LIMITS EACH OCCURRENCE 0AM1'1.>t: TO Kt:N I t:U PREMIS ES IEa occurrence\ E.L. EACH ACCIDENT Property Equipment Fltr 12/5/2015 12/5/2015 12/5/2016 12/5/2016 $2 ,000,000 s $ E.L. DISEASE · EA EMPLOYEE $ E.L. DISEASE - POLICY LIMIT EPP 0171044 EPP 0171044 $2 ,000,000 BPP Limit Limit Equipment Ded $ $127 ,000 $31,900 $500 DESCRIPTION OF OPERATIONS I LOCATIONS I VEHICLES (ACORD 101, Addltlonal Remarl<I Schedule, may be attached If more apace la required) SUBJECT TO POLICY TERMS AND CONDITIONS . CANCELLATION CERTIFICATE HOLDER Stephen F. Austin P .O . Box 13030 Nacogdoches TX I State University 75962 SHOULD ANY OF THE ABO VE DESCRIBED POLICIES BE CANCELLED BEFORE THE EXPIRATION DATE THEREOF, NOTICE WILL BE DELIVERED IN ACCORDANCE WITH THE POLICY PROVISIONS. AU THORIZED REPRESENTATIVE )ur. :l!rL © 1988-2014 ACORD CORPORATION. All rights reserved. ACORD 25 (2014/01) The ACORD name and logo are registered marks of ACORD JELLINC-01 MJENKINS DATE (MM/DD/YYYY) CERTIFICATE OF LIABILITY INSURANCE 2/18/2016 THIS CERTIFICATE IS ISSUED AS A MATIER OF INFORMATION ONLY AND CONFERS NO RIGHTS UPON THE CERTIFICATE HOLDER. THIS CERTIFICATE DOES NOT AFFIRMATIVELY OR NEGATIVELY AMEND, EXTEND OR ALTER THE COVERAGE AFFORDED BY THE POLICIES BELOW. THIS CERTIFICATE OF INSURANCE DOES NOT CONSTITUTE A CONTRACT BETWEEN THE ISSUING INSURER($), AUTHORIZED REPRESENTATIVE OR PRODUCER, AND THE CERTIFICATE HOLDER. IMPORTANT: If the certificate holder is an ADDITIONAL INSURED, the policy(ies) must be endorsed. If SUBROGATION IS WAIVED, subject to the terms and conditions of the policy, certain policies may require an endorsement. A statement on this certificate does not confer rights to the certificate holder in lieu of such endorsement(s). CONTACT NAME: PRODUCER Cravens Warren Insurance Agency, Inc. 10011 W. Gulf Bank Rd. Houston, TX 77040 E-MAIL ADDRESS : NAIC # INSURER S AFFORDING COVERAGE INSURER A : Texas INSURED :JeJCO G&A Outsourcing, Inc. dba G&A Partners INSURER B : 4801 Woodway Drive, Suite #210 Houston, TX 77056 INSURER D : 22945 Mutual Insurance Com pan INSURERC : INSURER E : INSURER F : COVERAGES CERTIFICATE NUMBER: REVISION NUMBER: THIS IS TO CERTIFY THAT THE POLICIES OF INSURANCE LISTED BELOW HAVE BEEN ISSUED TO THE INSURED NAMED ABOVE FOR THE POLICY PERIOD INDICATED. NOTWITH STANDING ANY REQUIREMENT, TERM OR CONDITION OF AN Y CONTRACT OR OTHER DOCUMENT V\/ITH RESPECT TO WHICH THIS CERTIFICATE MAY BE ISSUED OR MAY PERTAIN, THE INSURANCE AFFORDED BY THE POLICIES DESCRIBED HEREIN IS SUBJECT TO ALL THE TERMS, EXCLUSIONS AND CONDITIONS OF SUCH POLICIES. LIMITS SHOWN MAY HAVE BEEN REDUCED BY PAID CLAIMS. INSR LTR 5UDM INSD WVD l "UUL TYPE OF INSURANCE -D - POLICY NUMBER POLICY EFF POLICY EXP IMM/DD/YYYYI IMM/DD/YYYYI COMMERCIAL GENERAL LIABILITY I- CLAIMS-MADE D OCCUR I- Fl GEN'L AGGREGATE LIMIT APPLIES PER: POLI CY D PRO JECT Loc O LIMITS EACH OCCURRENCE DAMAGE TO REN 1 t: u PREMISES !Ea occurrence) $ MED EXP (Any one person) $ PERSONAL & ADV INJ URY $ GENERALAGGREGATE $ PRODUCTS - COMP/O P AGG $ $ OTHER: - YE~~~~~~tlSINGLE AUTOMOBILE LIABILITY I- AN Y AUTO ALL OWNED AUTOS HIRED AUTOS UMBRELLA LIAB EXCESS LIAB LIMIT BODILY INJURY (Per person) ~ I- - SCHEDU LED AUTO S NON-OWN ED AUTOS PROPERTY DAMAGE ! Per accident! $ H $ $ OCCUR EACH OCCURRENC E CLAIMS-MADE AGGREGATE RETENTION $ OED WORKERS COMPENSATION AND EMPLOYERS' LIABILITY ANY PROPRI ETOR/PARTNER/EXECUTIVE OFFICER/M EMBER EXCLUDED? (Mandatory in NH ) $ BODILY INJURY (Per accident) $ I I A $ x I ~f~TUTE I I OTHER Y/N D N/A TSF0001076234 02/23/2016 02/23/2017 g~~~~rtfi8~ O~OPERATIONS below $ $ $ $ 1,000,000 E.L. DISEASE - EA EMPLOYEE $ 1,000,000 E.L. DISEASE - POLICY LIMIT 1,000,000 E.L. EACH ACCIDENT $ DESCRIPTION OF OPERATIONS I LOCATIONS I VEHICLES (ACORD 101 , Additional Remarks Schedule, may be attached If more space ls required) Form WC 42 03 11 , Texas Professional Employer Organization (PEO) Endorsement, extends coverage to the covered employees of Jellison, Inc. dba Jelco, the client of the Named Insured. CANCELLATION CERTIFICATE HOLDER SHOULD ANY OF THE ABOVE DESCRIBED POLICIES BE CANCELLED BEFORE THE EXPIRATION DATE THEREOF, NOTICE WILL BE DELIVERED IN ACCORDANCE WITH THE POLICY PROVISIONS. Stephen F. Austin State University , its officials, directors, employees, representatives and volunte 1936 North Street 1Nacoadoches TX 75962 AUTHORIZED REPRESENTATIVE ~!M~ © 1988-2014 ACORD CORPORATION. All rights reserved . ACORD 25 (2014/01) The ACORD name and logo are registered marks of ACORD 1exasMuruaI® WORKERS COMPENSATION AND EMPLOYERS LIABILITY INSU RANCE POLICY Insurance Company WC 42 03 11 TEXAS PROFESSIONAL EMPLOYER ORGANIZATION (PEO) ENDORSEMENT This endorsement provides coverage for the covered employees of the client shown in the Schedule below. This endorsement applies only if attached to a policy issued in your name as the primary insured , and only with respect to your client's and your covered employees under a professional employer services agreement between you and your client shown in the Schedule below. Certain words and phrases in this endorsement are defined as follows : Client means any person who enters into a professional employer services ag reement with a PEO. Coemployment relationship means a contractual relationship between a client and a PEO that involves the sharing of employment responsibilities with, or allocation of employment responsibilities to , covered employees in accordance with the professional employer services agreement and Texas Labor Code , Chapter 91. Professional Employer Organization (PEO) means a business entity that offers professional employer services. Covered employee means an individual having a coemployment relationship with a PEO. Direct employee means an individual who is employed by a PEO or a cl ient and does not have a coemployment relationsh ip with a PEO . Professional Employer Services Agreement means a contract between a PEO and a client that includes details of the coemployment relationsh ip. Part One (Workers Compensation Insurance) and Part Two (Employers Liability Insurance) apply to the covered employees of the client shown in the Schedule below. Under Part One , we wi ll reimburse you for the benefits required by the workers compensation law if we are not permitted to pay the benefits directly to the persons entitled to them . Under Part Two , the limits of our liability apply jointly to you and the client. Our duty is to provide a single defense for you and the client on a claim, proceeding , or suit for damages payable under this insurance . The coverage afforded by this endorsement is not intended to satisfy the client's duty to secure its obligations under the workers compensation law fo r its direct employees. If th is policy is cancelled , we will send notice of such cancellation to you . You must notify each cl ient by certified mail within three days of rece ipt of such notice . Premium will be charged for covered employees of the client shown in the Schedule below. To satisfy your obligations under Part Five (Premium) , C.2, you must maintain and furnish to us a complete payroll record by cl ient for these covered employees. Part Fou r (Your Duties If Injury Occurs) applies to you and to the client. The client will recognize our right to defend under Parts One and Two and our right to inspect under Part Six (Conditions) . WC420311 (ED . 7-15) 1 of 2 INSURED'S COPY Schedule Name of Client: Address: See attached Extension of Information Page, Locations - Client, for list of clients. 2 of 2 This endorsement changes the policy to which it is attached effective on the inception date of the policy unless a different date is indicated below. (The following "attaching clause" need be completed only when this endorsement is issued subsequent to preparation of the policy.) This endorsement, effective on at 12:01 A.M. standard time, forms a part of Policy No. TSF-0001076234 20160223 ofthe Texas Mutual Insurance Company Issued to G & A OUTSOURCING I NC OBA: G & A PARTNERS Endorsement No. Premium$ NCCI Carrier Code 29939 Authorized Representative WC420311 (ED. 7-15) INSURED 'S COPY BSBUHAY 2-16-2016