Liability Insurance Certificate for GE Healthcare
advertisement

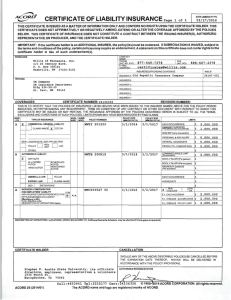
DATE (MM/DD/YYYY) CERTIFICATE OF LIABILITY INSURANCE 2/16/2016 THIS CERTIFICATE IS ISSUED AS A MATTER OF INFORMATION ONLY AND CONFERS NO RIGHTS UPON THE CERTIFICATE HOLDER. THIS CERTIFICATE DOES NOT AFFIRMATIVELY OR NEGATIVELY AMEND, EXTEND OR ALTER THE COVERAGE AFFORDED BY THE POLICIES BELOW. THIS CERTIFICATE OF INSURANCE DOES NOT CONSTITUTE A CONTRACT BETWEEN THE ISSUING INSURER(S), AUTHORIZED REPRESENTATIVE OR PRODUCER, AND THE CERTIFICATE HOLDER. IMPORTANT: If the certificate holder is an ADDITIONAL INSURED, the policy(ies) must be endorsed . If SUBROGATION IS WAIVED, subject to the terms and conditions of the policy, certain policies may require an endorsement. A statement on this certificate does not confer rights to the certificate holder in lieu of such endorsement(s). PRODUCER Tracy Darrin FAX Electric Insurance Company A/C No : 75 Sam Fonzo Drive Beverly, MA 01915-1000 INSURER S AFFORDING COVERAGE NAIC# 21261 INSURER A : Electric Insurance Com an • INSURED INSURER B : • A.M . Best: "A" FSC X as of 8/1 2/1 4 GE Healthcare Bio-Sciences Corp . 100 Results Way Marlborough , MA 01752 United States INSURER C: INSURER D: INSURER E: INSURER F: COVERAGES CERTIFICATE NUMBER: 176838 REVISION NUMBER: THIS IS TO CERTIFY THAT THE POLICIES OF INSURANCE LISTED BELOW HAVE BEEN ISSUED TO THE INSURED NAMED ABOVE FOR THE POLICY PERIOD INDICATED. NOTWITHSTANDING ANY REQUIRE MENT, TERM OR CONDITION OF ANY CONTRACT OR OTHER DOCUMENT WITH RESPECT TO WHICH THIS CERTIFICATE MAY BE ISSUED OR MAY PERTAIN, THE INSURANCE AFFORDED BY THE POLICIES DESCRIBED HEREIN IS SUBJECT TO ALL THE TERMS, EXCLUSIONS AND CONDITIONS OF SUCH POLICIES. LIMITS SHOWN MAY HAVE BEEN REDU CED BY PAID CLAIMS. ADDL SUBR POLICY EFF POLICY EXP INSR TYPE OF INSURANCE LIMITS 1 1.,~n wvn POLICY NUMBER IMM/DDIYYYYI IMM/DDIYYYYI LTR EACH OCCURRENCE x COMMERCIAL GENERAL LIABILITY $ $2 500 000 DAMl\l.>t: TO REN I t:U ~ CLAIMS-MADE OCCUR $ $50,000 PREMISES IEa occurrence\ MED EXP (Any one person) $ $10,000 ~ Ii] - A x ~ fl x GL 16-1 1/1/2016 1/1/2017 GEN'L AGGREGATE LIMIT APPLIES PER: POLICY D PROJECT D LOC OTHER: AUTOMOBILE LIABILITY A - A x ANY AUTO ALL OWNED AUTOS HIRED AUTOS UMBRELLA LIAB EXCESS LIAB $ $2 500 000 $5,000,000 PRODUCTS - COMP/OP AGG $ Included in Gen Agg . COMBINED SINGLE LIMIT !Ea accidenll BODILY INJURY (Per person) - SCHEDULED AUTOS NON-OWNED AUTOS F-4 x x ML 16-2 1/1/2016 1/1/2017 BODILY INJURY (Per accidenl) PROPERTY DAMAGE !Per accident) $ $2 ,500,000 $ $ $ s OCCUR CLAIMS-MADE x x XS 16-1 1/1/2016 1/1/2017 I I A $ GENERAL AGGREGATE $ ~ x - PERSONAL & ADV INJURY RETENTION $ OED WORKERS COMPENSATION AND EMPLOYERS' LIABILITY ANYPROPRIETORIPARTNERIEXECUTIVE OFFICER/MEMBER EXCLUDED? (Mandatory in NH) EACH OCCURRENCE $ $2,500 ,000 AGGREGATE $ $5 000 000 x I ~f:TUTE I YIN [El NIA x WC 16-1 1/1/2016 1/1/2017 ~~~~~;;;.fr~~ ~nFdOPERATIONS below I OTHER E.L. EACH ACCIDENT $ $ $2 500 000 E.L. DISEASE - EA EMPLOYEE $ $2 500 000 E.L. DISEASE · POLICY LIMIT $ $5 000 000 DESCRIPTION OF OPERATIONS I LOCATIONS I VEHICLES (ACORD 101 , Additional Remarl<s Schedule, may be attached If more space Is required) Should any of the above referenced policies be cancelled befo re the expiration date thereof, the issuing insurer will endeavor to mail 30 days prior written notice to the certificate hold er, however failure to do so shall not impose any obligation or liability of any kind upon the Insurer affording coverage , or its agents or representatives. Subject to the insurance policy terms and conditions , the above referenced insurances shall contain a waiver of subrogation , but only to the extent required by the underlying written contract with the Named Insured that is in place prior to an "occurrence" giving rise to a loss . CERTIFICATE HOLDER Stephen F. Austin State University P.O. Box 13030, SFA Station Nacogdoches , TX 75962 United States CANCELLATI ON SHOULD ANY OF THE ABOVE DESCRIBED POLICIES BE CANCELLED BEFORE THE EXPIRATION DATE THEREOF, NOTICE WILL BE DELIVERED IN ACCORDANCE WITH THE POLICY PROVISIONS. AUTHORIZED REPRESENTATIVE © 1988-2014 ACORD CORPORATION. All rights reserved . ACORD 25 (2014/01) The ACORD name and logo are registe red marks of ACORD ADDITIONAL REMARKS SCH EDULE NAMED INSURED AGENCY GE Healthcare Bio-Sciences Corp. 100 Results Way Marlborough , MA 01752 United States Electric Insurance Company 75 Sam Fonzo Drive Beverly, MA 01915-1000 EFFECTIVE DATE: 1/1/2016 ADDITIONAL REM ARKS TH IS ADDITIO NAL REMARKS FORM IS A SCHEDULE TO ACORD FORM , FORM NUMBER: 25 FORM TITLE: Certificate of Liability Insurance GL Coverages: a. Premises-Operations b. Products/Completed Operations c. xcu d. Blanket Contractual Liability e. Personal and Advertising Injury Limit f. Independent Contractors g. Separation of Insureds I Cross Liabi lity h. Sudden and Accidental Pollution Liab ility Auto Coverages: a. Symbol 1 - All Vehicles Excess Liability: a. Following Form WC Coverages: a. USL&H b. Jones Act I Maritime Liability c. Outer Continental Shelf Lands Act d. The Workers Compensation policy provides coverage in all states where the insured has operations, except for monopolistic states (ND, WY, PR, USVI) and states where the insured qualifies for self-insured status (OH, WA) ACORD 101 (2008/01) © 2008 ACORD CORPORATION. All right s reserved . The ACORD name and logo are registered marks of ACORD