8
ACORD
DATE (MMIOOIYVYYJ
I
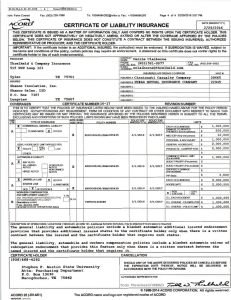
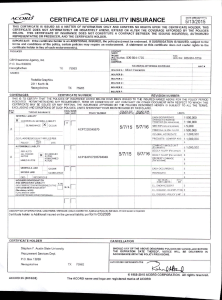
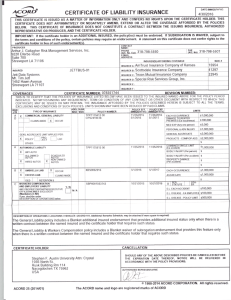
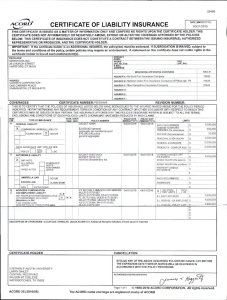
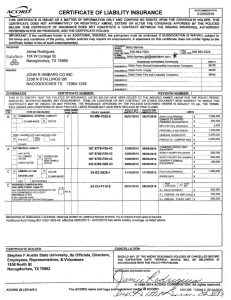
CERTIFICATE OF LIABILITY INSURANCE
~
03/01/2016
THIS CERTIACATE IS ISSUED AS A MAnER OF INFORMATION ONLY AND CONFERS NO RIGHTS UPON THE CERTIFICATE HOLDER. THIS
CERTIFICATE DOES NOT AFFIRMATIVELY OR NEGATIVELY AMEND, EXTEND OR ALTER THE COVERAGE AFFORDED BY THE POLICIES
BELOW. THIS CERTIFICATE OF INSURANCE DOES NOT CONSTITUTE A CONTRACT BETWEEN THE ISSUING INSURER(S), AUTHORIZED
REPRESENTATIVE OR PRODUCER, AND THE CERTIACATE HOLDER.
IMPORTANT: If the certificate holder Is an ADDITIONAL INSURED, the policy(ies) must be endorsed. If SUBROGATION IS WAIVED, subject to the
terms and conditions of the policy, certain policies may require an endorsement. A statement on this certificate does not confer rights to the
certificate holder in lieu of such endorsement(s).
PRODUCER
(:~J
Dave Kiley, State Farm Insurance
3608 Preston Rd., Suite 145
TX 75093
Plano,
1
E-MAIL
.~OORESS
:
~- r~~: No); 97~-985-88~ -~=
s haron @d avek1'Iey.f'le_t_ ________ _______
·--
Superior Kitchen Serv1ces LLC
DBA Aqua Tek
3309 US HIGHWAY 69 N
Lufkin, TX 75904
!~SURER A
I
INSURE~(S) AFFORDlNG CO_Y.ERAGE _
1-·
~ ---------.--- --- · -------- · -- - -
INSURED
~~~~cT Sharon
~; ~xt)· 9Z2~985~_8oo
: State
F~m
~~
LloyQl>_ _ ____ _____ - - - ·
_4ill.9_ _ _
=~:: ~~~~ I -~RD :
· - - - - - - - - - - --~~ --- -
- ---- --
-
- - ---
------
INSURER F :
CERTIFICATE NUMBER·
COVERAGES
REVISION NUMBER·
TH IS IS TO CERTIFY THAT TH E POLICIES OF INSURANCE LISTED BELOW HAVE BEEN ISSUED TO THE INSURED NAMED ABOVE FOR TH E POLICY PERIO D
INDICATED. NOTINITHSTANDING ANY REQUIR EMENT, TERM OR CONDITION OF ANY CONTRACT OR OTHER DOCUMEN T \IIIlTH RESPECT TO WHICH THIS
CERTIFICATE MAY BE ISSUED OR MAY PERTAIN , THE INSURANCE AFFORDED BY THE POLICIES DESCRIBED HEREIN IS SUBJECT TO ALL THE TERMS,
EXCLUSIONS AND CONDITIONS OF SUCH POLICIES. LIMITS SHOWN MAY HAVE BEEN REDUCED BY PAID CLAIMS.
INSR
L TR
- - mm:rsusw--·- - -- -- - - - - - rpOLICY EFf:- -porrcy EXP
,.,._., I vivo
POLICY NUMBER
I (MMIDOivYYYI
!WNDDrivYvJ
TYPE OF INSURANCE
A I GENERAL LIABILITY
r
ryll y '
1-Xl
L...:..J '---'
~_2M M ERCIAL GENERAL: LIABILITY
93-C D-F041-3 l
10/28/2015
n
cJ
jfg
~ ANY
Rj
AUTO
F-
~b~g~ED
r
UMBRELLA UAB
.
I
HIREOAUTOS
EXCESS LIAB
I
~
LOC
D
.. ~---2,?00,000
PRODUCTS - COMPIOPAGG
- - - -- - - --
:
03/16/201 6 ' 09/16/2016 ~~~~~.tNGLE
183 5256-C16-43A
SCHEDULED
'--
r- ~~~v.NED
X
GENE~~L AGGR~GATE
.
'
I IoccuR
$
- -- - - -
LIM I~-- _L_ ____ _
BODILY INJURY (Per person) -
s_______
500,0~-
500 000
EACH os;_s;u RRENC_e_ ____ _L__ ______
~_!'~----- ..!__ _ _ , _ __
I
s
OED
RETENTION $
WORKERS COMPENSATJON
AND EMPLOYERS' LIABILITY
y 1N
ANY PROPRIETOR/PARTNER/EXECUTIVE
OFFICE/MEMBER EXCLUDED?
· (Mandatory In NH)
- - - - - - -----
D
If yes, describe! ~~PERATIONS below
2,000 ,000
r~~=~=---~~~
)
_[]_cLAIMS-~~
I
_
$
BODILY INJURY (Per acd<lenl)' $
AUTOS
5,000
$
. .£___~~~~
_£>ERSONA;L & ADV INJURY
i
! AUTOf.IOBILE LIABILITY
B
L$ ~
1,000,000
1 ,,iliJ;I;!;~O"fiD!r~~ ,----_E_flEMISES (!;a occurr!'!E!)__ _$-- ~~-~
~~0 EXP (~y one pe~son)
- -- - - -. - - - ,
- - - - - -- 1- GEN'L AGGREGATE LIMIT APPLIES PER:
,->.<J POLICY
LIMITS
10/28/2016 ~CH OCCURRENCE
CLAIMS-MADE [){] OCCUR
__ -
·- --·
~- L. EACH ~T-~_
<_$_ _ , _ _ __
E.L. DISEASE· EA EMPLOY
~:-DISEASE - POUCY -~IMIT
l
_
$
5- - -· - - ---
OESCRIPTlON OF OPERATIONS I LOCATIONS I VEHICLES (Attach ACORD 101, Addllional Remarl<s Schedule, if mo..., space Is required)
CERTIFICATE HOLDER
Stephen F. Austin State University, its officials, directors,
employees, representatives and Volunteers
1936 North St.
Nacogdoches, TX 75962
ACORD 25 (2010/05)
CANCELLATION
SHOULD ANY OF THE ABOVE DESCRIBED POLICIES BE CANCELLED BEFORE
THE EXPIRATION DATE THEREOF, NOTICE WILL BE DELIVERED IN
CCORDANCE WIT
HE POLICY PROVISIONS.
 0
0